James R. Gavin, III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Emory Health System Fairburn, Georgia Pamela R. Kushner, MD, MA, FAAFP Associate Clinical Professor of Family Medicine University of California College of Medicine Irvine, California Director, Osteoporosis Diagnostic Center Los Alamitos, California
Transcript
James R. Gavin, III, MD, PhD CEO and Chief Medical Officer
Healing Our Village, Inc. Emory Health System
Fairburn, Georgia
Pamela R. Kushner, MD, MA, FAAFP Associate Clinical Professor of Family Medicine
University of California College of Medicine Irvine, California
Director, Osteoporosis Diagnostic Center Los Alamitos, California
Session 2
Session 2: Benefit-to-Risk Ratios for Treatment of Type 2 Diabetes Learning Objectives
• Describe the benefits and potential risks of pharmacotherapeutic treatment options for patients with type 2 diabetes.
• Discuss the most recent clinical data and guidelines regarding antidiabetes medications for the treatment of type 2 diabetes.
Faculty James R. Gavin, III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Emory Health System Fairburn, Georgia
Clinical Professor of Medicine Emory University School of Medicine Atlanta, Georgia Dr James R. Gavin, III, is CEO and chief medical officer of Healing Our Village, Inc., in Fairburn, Georgia, and clinical professor of medicine at Emory University School of Medicine in Atlanta. He serves as a reserve officer in the US Public Health Service. Dr Gavin has authored or coauthored more than 200 articles and abstracts for such publications as Science, the Journal of Applied Physiology, and Diabetes. He has also authored 2 books: Healing Our Village: A Self-Care Guide for Diabetes Control (with L. Coleman) and Dr. Gavin’s Health Guide for African Americans (with S. Landrum). Dr Gavin is chairman of the Data Safety Monitoring Board for the VA Cooperative Diabetes Study and a member of several professional organizations, including the Institute of Medicine of the National Academy of Sciences, the American Diabetes Association, and the American Society of Clinical Investigation. Pamela R. Kushner, MD, MA, FAAFP Associate Clinical Professor of Family Medicine University of California College of Medicine Irvine, California
Director, Osteoporosis Diagnostic Center Los Alamitos, California Dr Pamela R. Kushner, a board-certified specialist in family medicine, is associate clinical professor of family medicine at the University of California, Irvine (UC-Irvine), School of Medicine. She serves as director of the Osteoporosis Diagnostic Center in Los Alamitos, California, and as an expert reviewer for the Medical Board of California. Dr Kushner earned her medical degree from the California College of Medicine at UC-Irvine, and completed a family medicine residency at Long Beach Memorial Medical Center in Long Beach, California. An active member of the American Academy of Family Physicians (AAFP) and the California Academy of Family Physicians (CAFP), Dr Kushner is the AAFP representative to the US Food and Drug Administration MedWatch Program and past president of both the Los Angeles and Long Beach chapters of CAFP. She was also the first woman president of the Long Beach (California) Medical Association. Dr Kushner has authored an article published in Stroke and has authored or coauthored several articles in other medical journals for health professionals. Faculty Financial Disclosure Statements The presenting faculty report the following: Dr Gavin is a consultant for Eli Lilly and Company; LifeScan, Inc.; Merck & Co. Inc.; and sanofi-aventis U.S.; and a speaker for Eli Lilly and Company and Novo Nordisk.
Session 2
Dr Kushner is a consultant for AstraZeneca Pharmaceuticals LP and GlaxoSmithKline; has received research grants from AstraZeneca Pharmaceuticals LP and Novartis Pharmaceuticals Corporation; is a speaker for AstraZeneca Pharmaceuticals LP; Forest Laboratories, Inc.; GlaxoSmithKline; and Pfizer Inc.; and serves as an advisor to AstraZeneca Pharmaceuticals LP and Eli Lilly and Company, the latter of which she is a shareholder. Education Partner Financial Disclosure Statement The content collaborators at ProCom report the following: Susan Etzi, MD, MPH, has no relationships to disclose. Drug List Generic Trade glipizide Glucotrol XL glyburide Diaβeta, Glynase, Micronase metformin Glucophage
Acronym ListAcronym Definition INS insulin MET metformin
Acronym Definition SU sulfonylurea TZD thiazolidinedione
Suggested Reading List
1. American Diabetes Association. Standards of medical care in diabetes—2007. Diabetes Care. 2007;30(suppl):S4-S41.
2. Amori R, Lau J, Pittas A. Efficacy and safety of incretin therapy in type 2 diabetes. JAMA. 2007;298:194-206. 3. Bhatt DL, Chew DP, Grines C, et al. Peroxisome proliferator-activated receptor gamma agonists for the
Prevention of Adverse events following percutaneous coronary Revascularization—results of the PPAR study. Am Heart J. 2007;154:137-143.
4. DREAM Investigators. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled trial. Lancet. 2006;368:1096-1105
5. Erdmann E, Dormandy J, Charbonnel B, et al; PROactive Investigators. The effect of pioglitazone on recurrent myocardial infarction in 2,445 patients with type 2 diabetes and previous myocardial infarction. J Am Coll Cardiol. 2007;49:1772-1780.
6. Home P, Jones NP, Pocock SJ, et al; the RECORD Study Group. Rosiglitazone RECORD study: glucose control outcomes at 18 months. Diabet Med. 2007;24:626-634.
7. Home PD, Pocock SJ, Beck-Nielsen H, et al; the RECORD Study Group. Rosiglitazone evaluated for cardiovascular outcomes—an interim analysis. N Engl J Med. 2007;357:28-38.
8. Kahn SE, Haffner SM, Heise MA, et al; the ADOPT Study Group. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006;355:2427-2443.
9. Lincoff AM, Wolski K, Nicholls SJ, et al. Pioglitazone and risk of cardiovascular events in patients with type 2 diabetes mellitus: a meta-analysis of randomized trials. JAMA. 2007;298:1180-1188.
10. Lipscombe LL, Gomes T, Leَvesque LE, et al. Thiazolidinediones and cardiovascular outcomes in older patients with diabetes. JAMA. 2007;298:2634-2643.
11. Nathan DM, Buse JB, Davidson MB, et al. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353:2643-2653.
12. Nissan SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007;356:2457-2471.
13. Rosenstock J, Brazg R, Andryuk PJ, et al; the Sitagliptin Study 019 Group. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin added to ongoing pioglitazone therapy in patients with type 2 diabetes: a 24-week, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Clin Ther. 2006;28:1556-1568.
14. Singh S, Loke YK, Furberg CD. Long-term risk of cardiovascular events with rosiglitazone. JAMA. 2007;298:1189-1195.
15. Singh S, Loke YK, Furberg CD. Thiazolidinediones and heart failure: a teleo-analysis. Diabetes Care. 2007;30:2148-2153.
Benefit to Risk Ratios for Treatment Benefit to Risk Ratios for Treatment of Type 2 Diabetesof Type 2 Diabetes
Pamela R. Kushner, MD, MA, FAAFPAssociate Clinical Professor, Family MedicineUniversity of California, Irvine College of MedicineIrvine, CaliforniaDirector, Osteoporosis Diagnostic CenterLos Alamitos, California
2
Case Case StudyStudy⎯⎯DavidDavid
• 9:00 AM appointment for a refill of antihistamines
• Routine questions reveal family history of type 2 diabetes
• Exam reveals elevated blood pressure (BP)
3
Case Case StudyStudy⎯⎯DavidDavid (cont(cont’’d)d)
• 38-year-old man
• Weight = 225 lb
• BMI = 32
• Waist circumference = 40 in
• BP = 140/90 mm Hg
• TG = 220 mg/dL
• LDL-C = 109 mg/dL
• HDL-C = 38 mg/dL
BMI=body mass index; TG=triglycerides; LDL-C=low-density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterolLaSalle J. Hospital Physician. 2005;41:37-46.
4
Case Case StudyStudy⎯⎯DavidDavid (cont(cont’’d)d)
• Family history– Mother diagnosed with type 2 diabetes
Based on the labs, family history, and diagnosis, what would your treatment plan include in addition to diet and exercise?
1. Antihypertensive2. Oral antidiabetic drug3. Statin4. All of the above
6
Treatment PlanTreatment Plan
• Diet and exercise
• Ramipril 10 mg
• Atorvastatin 10 mg
• MET=500 mg/bid
• Follow up in 4 weeks
MET=metformin
2
7
ARS Question #2 ARS Question #2 ??What is your first concern in treating a newly diagnosed patient with type 2 diabetes and hypertension?
1. High blood pressure2. A1C3. Fasting plasma glucose4. Lipids
8
Case StudyCase Study——33--Month FollowMonth Follow--Up VisitUp Visit
David returns for a follow-up visit in 3 months. He admits that he forgets to take his medication sometimes; however, he has been walking at lunch with a colleague.
Labs show:– FPG = 125 mg/dL– A1C = 6.3%– BP = 138/88 mm Hg
9
ARS Question #3ARS Question #3 ??What are the next steps for David’s treatment?
1. Strategies to encourage medication adherence
2. Weight loss and exercise program; increased physical activity
3. Change medications4. All of the above
1010
Benefits of Glycemic ControlBenefits of Glycemic Control
11
Risk of CVD Is Elevated Prior to Risk of CVD Is Elevated Prior to Diagnosis of Type 2 DiabetesDiagnosis of Type 2 Diabetes
CVD=cardiovascular diseaseHu F et al. Diabetes Care. 2002;25:1129-1134.
NondiabeticThroughout
Study
Rela
tive
Ris
k of
MI
or
Str
oke
1.00
≥15 y Before Diagnosis
2.40
10-14.9 y Before
Diagnosis
3.19
<10 y Before
Diagnosis
3.64
0.00
1.00
2.00
3.00
4.00
12
Glycemic Control and Risk of Glycemic Control and Risk of Development of HF in DiabetesDevelopment of HF in Diabetes
0
2
4
6
8
10
9 to <10 ≥108 to <97 to <8<7
4.5
5.86.3
8.39.2
P=.001
A1C (%)
HF
Hosp
italiz
atio
n a
nd/o
r D
eath
Rat
e/1,0
00 P
erso
n-Y
ear
s
Iribarren C et al. Circulation. 2001;103:2668-2673.
Age-Adjusted Incidence Rates
N=48,858
HF=heart failure
3
13
ARS Question #4ARS Question #4 ??Compared with patients who have A1C <7%, what is the risk of developing heart failure in patients with A1C ≥10%?
1. Increases by 20%2. Increases by 33%3. Increases by 50%4. More than doubles
14
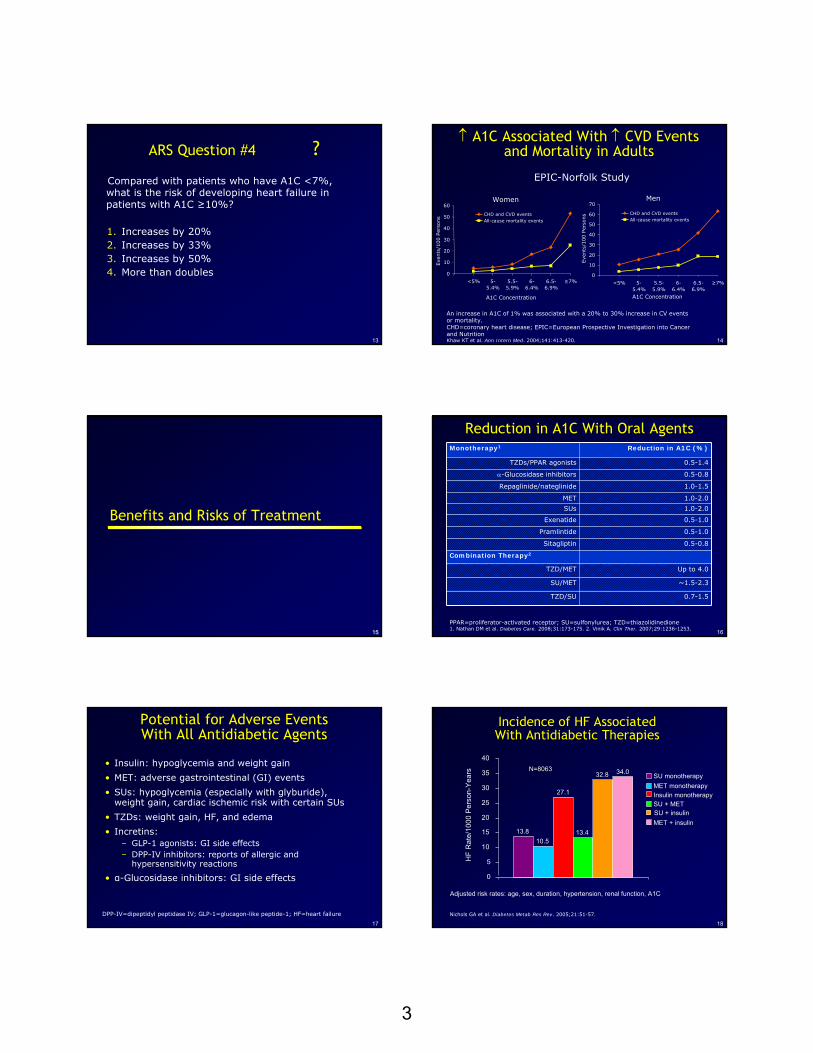
↑↑ A1C Associated With A1C Associated With ↑↑ CVD Events CVD Events and Mortality in Adultsand Mortality in Adults
An increase in A1C of 1% was associated with a 20% to 30% increase in CV events or mortality.CHD=coronary heart disease; EPIC=European Prospective Investigation into Cancer and NutritionKhaw KT et al. Ann Intern Med. 2004;141:413-420.
EPIC-Norfolk Study
Women
0
10
20
30
40
50
60
<5% 5-5.4%
5.5-5.9%
6-6.4%
6.5-6.9%
≥7%
A1C Concentration
Eve
nts
/100 P
erso
ns
CHD and CVD eventsAll-cause mortality events
Men
0
10
20
30
40
50
60
70
<5% 5-5.4%
5.5-5.9%
6-6.4%
6.5-6.9%
≥7%
A1C Concentration
Eve
nts
/100 P
erso
ns CHD and CVD events
All-cause mortality events
1515
Benefits and Risks of TreatmentBenefits and Risks of Treatment
16
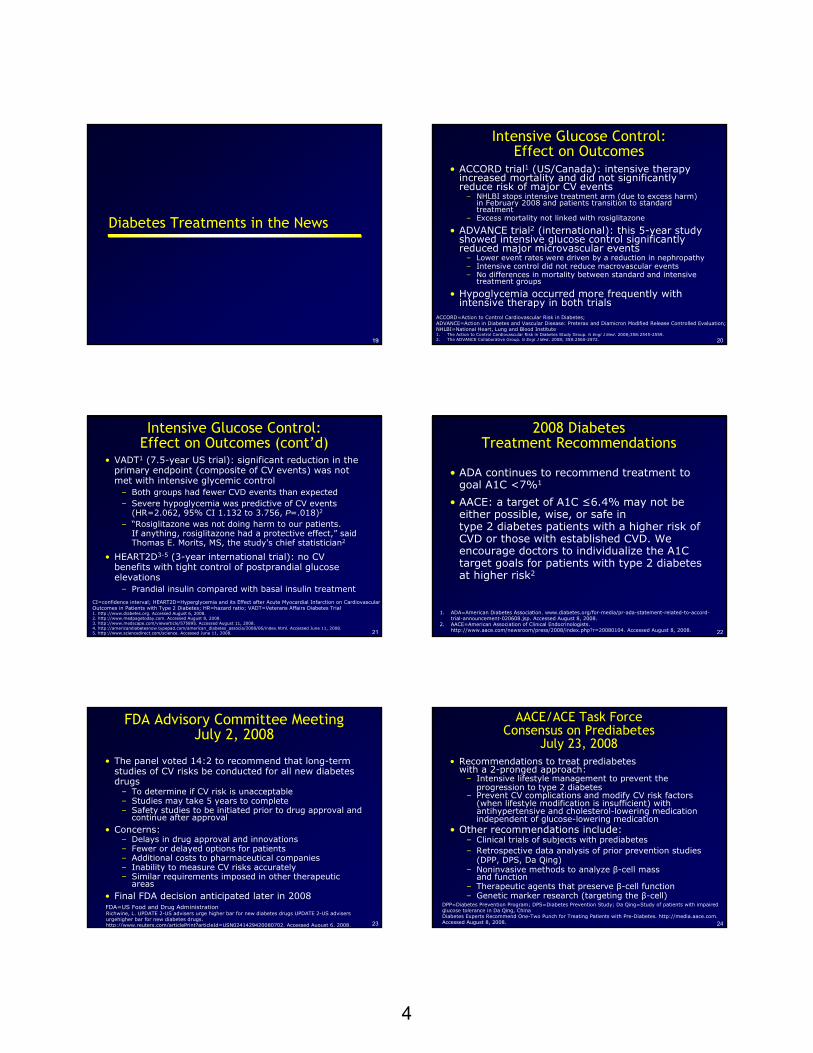
Reduction in A1C With Oral AgentsReduction in A1C With Oral Agents
Up to 4.0TZD/MET
~1.5-2.3SU/MET
0.7-1.5TZD/SU
Monotherapy1 Reduction in A1C (%)
TZDs/PPAR agonists 0.5-1.4
α-Glucosidase inhibitors 0.5-0.8
Repaglinide/nateglinide 1.0-1.5
MET 1.0-2.0
SUs 1.0-2.0
Exenatide 0.5-1.0
Pramlintide 0.5-1.0
Sitagliptin 0.5-0.8
Combination Therapy2
PPAR=proliferator-activated receptor; SU=sulfonylurea; TZD=thiazolidinedione1. Nathan DM et al. Diabetes Care. 2008;31:173-175. 2. Vinik A. Clin Ther. 2007;29:1236-1253.
17
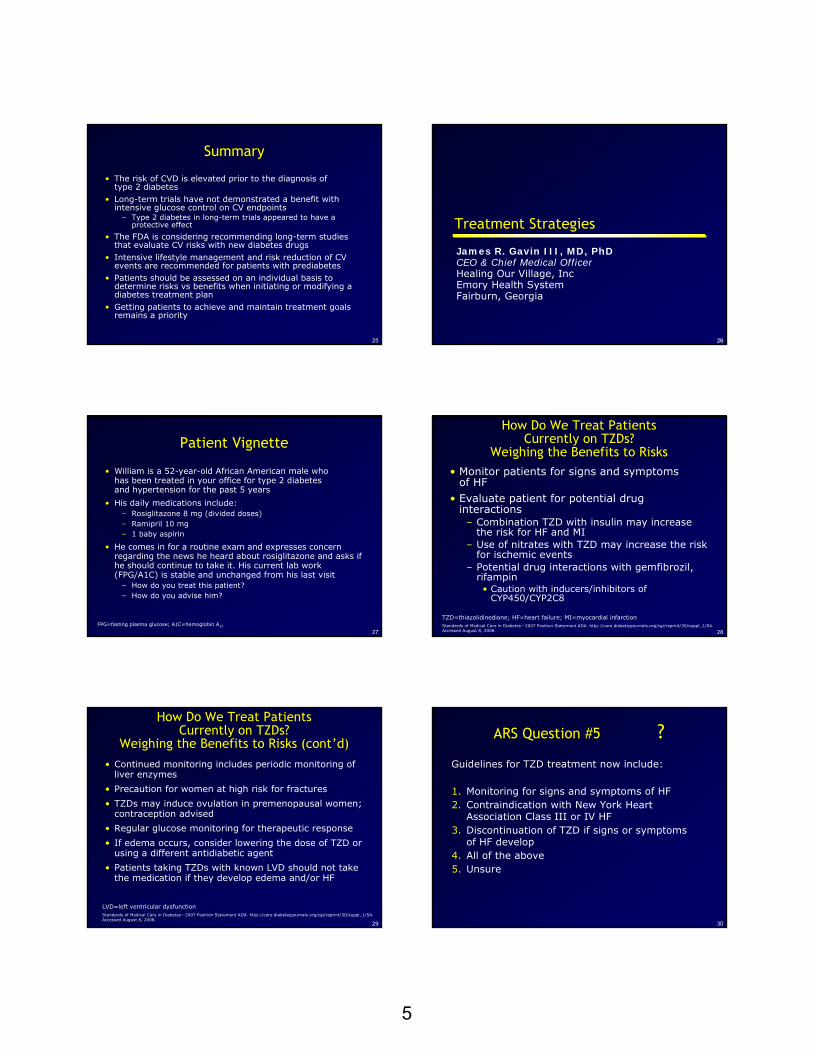
Potential for Adverse Events Potential for Adverse Events With All With All AntidiabeticAntidiabetic AgentsAgents
• Insulin: hypoglycemia and weight gain
• MET: adverse gastrointestinal (GI) events
• SUs: hypoglycemia (especially with glyburide), weight gain, cardiac ischemic risk with certain SUs
• TZDs: weight gain, HF, and edema
• Incretins: – GLP-1 agonists: GI side effects – DPP-IV inhibitors: reports of allergic and
Nichols GA et al. Diabetes Metab Res Rev. 2005;21:51-57.
13.810.5
27.1
13.4
32.8 34.0
0
5
10
15
20
25
30
35
40
SU monotherapyMET monotherapyInsulin monotherapySU + METSU + insulinMET + insulin
4
1919
Diabetes Treatments in the NewsDiabetes Treatments in the News
20
Intensive Glucose Control: Intensive Glucose Control: Effect on OutcomesEffect on Outcomes
• ACCORD trial1 (US/Canada): intensive therapy increased mortality and did not significantly reduce risk of major CV events
– NHLBI stops intensive treatment arm (due to excess harm) in February 2008 and patients transition to standard treatment
– Excess mortality not linked with rosiglitazone
• ADVANCE trial2 (international): this 5-year study showed intensive glucose control significantly reduced major microvascular events
– Lower event rates were driven by a reduction in nephropathy– Intensive control did not reduce macrovascular events– No differences in mortality between standard and intensive
treatment groups
• Hypoglycemia occurred more frequently with intensive therapy in both trials
ACCORD=Action to Control Cardiovascular Risk in Diabetes;ADVANCE=Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation; NHLBI=National Heart, Lung and Blood Institute1. The Action to Control Cardiovascular Risk in Diabetes Study Group. N Engl J Med. 2008;358:2545-2559. 2. The ADVANCE Collaborative Group. N Engl J Med. 2008; 358:2560-2572.
21
• VADT1 (7.5-year US trial): significant reduction in the primary endpoint (composite of CV events) was not met with intensive glycemic control
– Both groups had fewer CVD events than expected– Severe hypoglycemia was predictive of CV events
(HR=2.062, 95% CI 1.132 to 3.756, P=.018)2
– “Rosiglitazone was not doing harm to our patients. If anything, rosiglitazone had a protective effect,” said Thomas E. Morits, MS, the study's chief statistician2
• HEART2D3-5 (3-year international trial): no CV benefits with tight control of postprandial glucose elevations
– Prandial insulin compared with basal insulin treatmentCI=confidence interval; HEART2D=Hyperglycemia and its Effect after Acute Myocardial Infarction on CardiovascularOutcomes in Patients with Type 2 Diabetes; HR=hazard ratio; VADT=Veterans Affairs Diabetes Trial1. http://www.diabetes.org. Accessed August 6, 2008. 2. http://www.medpagetoday.com. Accessed August 8, 2008. 3. http://www.medscape.com/viewarticle/575895. Accessed August 11, 2008.4. http://americandiabetesnow.typepad.com/american_diabetes_associa/2008/06/index.html. Accessed June 11, 2008.5. http://www.sciencedirect.com/science. Accessed June 11, 2008.
Intensive Glucose Control: Intensive Glucose Control: Effect on Outcomes (contEffect on Outcomes (cont’’d)d)
• ADA continues to recommend treatment to goal A1C <7%1
• AACE: a target of A1C ≤6.4% may not be either possible, wise, or safe in type 2 diabetes patients with a higher risk of CVD or those with established CVD. We encourage doctors to individualize the A1C target goals for patients with type 2 diabetes at higher risk2
1. ADA=American Diabetes Association. www.diabetes.org/for-media/pr-ada-statement-related-to-accord-trial-announcement-020608.jsp. Accessed August 8, 2008.
2. AACE=American Association of Clinical Endocrinologists. http://www.aace.com/newsroom/press/2008/index.php?r=20080104. Accessed August 8, 2008.
23
FDA Advisory Committee Meeting FDA Advisory Committee Meeting July 2, 2008July 2, 2008
• The panel voted 14:2 to recommend that long-term studies of CV risks be conducted for all new diabetes drugs
– To determine if CV risk is unacceptable– Studies may take 5 years to complete– Safety studies to be initiated prior to drug approval and
continue after approval• Concerns:
– Delays in drug approval and innovations– Fewer or delayed options for patients – Additional costs to pharmaceutical companies– Inability to measure CV risks accurately– Similar requirements imposed in other therapeutic
areas• Final FDA decision anticipated later in 2008FDA=US Food and Drug AdministrationRichwine, L. UPDATE 2-US advisers urge higher bar for new diabetes drugs UPDATE 2-US advisers urgehigher bar for new diabetes drugs.http://www.reuters.com/articlePrint?articleId=USN0241429420080702. Accessed August 6, 2008. 24
AACE/ACE Task Force AACE/ACE Task Force Consensus on Consensus on PrediabetesPrediabetes
July 23, 2008July 23, 2008• Recommendations to treat prediabetes
with a 2-pronged approach:– Intensive lifestyle management to prevent the
progression to type 2 diabetes– Prevent CV complications and modify CV risk factors
(when lifestyle modification is insufficient) with antihypertensive and cholesterol-lowering medication independent of glucose-lowering medication
• Other recommendations include:– Clinical trials of subjects with prediabetes– Retrospective data analysis of prior prevention studies
(DPP, DPS, Da Qing)– Noninvasive methods to analyze β-cell mass
and function– Therapeutic agents that preserve β-cell function– Genetic marker research (targeting the β-cell)
DPP=Diabetes Prevention Program; DPS=Diabetes Prevention Study; Da Qing=Study of patients with impaired glucose tolerance in Da Qing, China Diabetes Experts Recommend One-Two Punch for Treating Patients with Pre-Diabetes. http://media.aace.com. Accessed August 8, 2008.
5
25
SummarySummary
• The risk of CVD is elevated prior to the diagnosis of type 2 diabetes
• Long-term trials have not demonstrated a benefit with intensive glucose control on CV endpoints
– Type 2 diabetes in long-term trials appeared to have a protective effect
• The FDA is considering recommending long-term studies that evaluate CV risks with new diabetes drugs
• Intensive lifestyle management and risk reduction of CV events are recommended for patients with prediabetes
• Patients should be assessed on an individual basis to determine risks vs benefits when initiating or modifying a diabetes treatment plan
• Getting patients to achieve and maintain treatment goals remains a priority
2626
Treatment Strategies Treatment Strategies
James R. Gavin III, MD, PhDCEO & Chief Medical OfficerHealing Our Village, IncEmory Health SystemFairburn, Georgia
27
Patient VignettePatient Vignette
• William is a 52-year-old African American male who has been treated in your office for type 2 diabetes and hypertension for the past 5 years
• He comes in for a routine exam and expresses concern regarding the news he heard about rosiglitazone and asks if he should continue to take it. His current lab work (FPG/A1C) is stable and unchanged from his last visit
– How do you treat this patient?– How do you advise him?
FPG=fasting plasma glucose; A1C=hemoglobin A1C
28
How Do We Treat Patients How Do We Treat Patients Currently on TZDs? Currently on TZDs?
Weighing the Benefits to RisksWeighing the Benefits to Risks• Monitor patients for signs and symptoms
of HF • Evaluate patient for potential drug
interactions– Combination TZD with insulin may increase
the risk for HF and MI– Use of nitrates with TZD may increase the risk
for ischemic events– Potential drug interactions with gemfibrozil,
rifampin• Caution with inducers/inhibitors of
CYP450/CYP2C8
TZD=thiazolidinedione; HF=heart failure; MI=myocardial infarctionStandards of Medical Care in Diabetes—2007 Position Statement ADA. http://care.diabetesjournals.org/cgi/reprint/30/suppl_1/S4. Accessed August 8, 2008.
29
How Do We Treat Patients How Do We Treat Patients Currently on TZDs?Currently on TZDs?
Weighing the Benefits to Risks (contWeighing the Benefits to Risks (cont’’d)d)• Continued monitoring includes periodic monitoring of
liver enzymes
• Precaution for women at high risk for fractures
• TZDs may induce ovulation in premenopausal women; contraception advised
• Regular glucose monitoring for therapeutic response
• If edema occurs, consider lowering the dose of TZD or using a different antidiabetic agent
• Patients taking TZDs with known LVD should not take the medication if they develop edema and/or HF
LVD=left ventricular dysfunctionStandards of Medical Care in Diabetes—2007 Position Statement ADA. http://care.diabetesjournals.org/cgi/reprint/30/suppl_1/S4.Accessed August 8, 2008.
30
ARS Question #5ARS Question #5 ??Guidelines for TZD treatment now include:
1. Monitoring for signs and symptoms of HF2. Contraindication with New York Heart
Association Class III or IV HF3. Discontinuation of TZD if signs or symptoms
of HF develop4. All of the above5. Unsure
6
3131
The Benefits of Combination TherapyThe Benefits of Combination Therapy
32
ARS Question #6ARS Question #6 ??TZDs can enhance glycemic control when used in combination with:
1. Sulfonylurea2. Metformin3. Sitagliptin4. All of the above
Benefit of Combination Benefit of Combination Therapy With TZDsTherapy With TZDs
-1.2-1
-0.8
-0.6
-0.4
-0.2
00.2
0.40.6
SU MET Insulin-1.4
Cha
nge
From
Bas
elin
e A
1C (%
)
34
A1C Change From Baseline: A1C Change From Baseline: PIO + MET vs GLIC + METPIO + MET vs GLIC + MET
LOCF. ITT population.
GLIC=gliclazide; ITT=intent-to-treat; LOCF=last observation carried forwardCharbonnel B et al. Diabetologia. 2005;48:1093-1104.
Cha
nge
From
Bas
elin
e A
1C (%
)
PIO + METGLIC + MET
0
-0.2
-0.4
-0.6
-0.8
-1
-1.2
-1.4
-1.6
0 10 20 30 40 50 60 70 80 90 100 110Weeks
35
ROSI/MET FixedROSI/MET Fixed--Dose Combination Effective Dose Combination Effective in Patients With Severe Hyperglycemiain Patients With Severe Hyperglycemia
190 drug-naïve patients initiated on 4 mg/1000 mg and titrated to maximum daily dose of 8 mg/2000 mg
44% of patients reached ADA goal <7% A1C (65/148)
3% incidence of edema (6/190)
Rosenstock J et al. Diabetes Obes Metab. 2006;8:643-649.
A1C
(%)
Baseline
ROSI + MET 8 mg/2000 mg
11.8%
7.8%
4% A1C reduction
FPG
( m
g/dL
)
BaselineROSI + MET
8 mg/2000 mg
305 mg/dL
166 mg/dL
139 mg/dL FPG reduction
-14
-12
-10
-8
-6
-4
-2
0
-350
-300
-250
-200
-150
-100
-50
0
36
ROSI + GLIM FixedROSI + GLIM Fixed--Dose Combination Dose Combination Effective in Newly Diagnosed PatientsEffective in Newly Diagnosed Patients
ITT population using LOCF method. *Compared with glimepiride (GLIM) and ROSI, P<.0001.Palmer JP et al. ADA Diabetes. 2006;55:541-P.
Perc
ent a
t Goa
l
A1C <7%
n=221 n=227 n=221 n=214
4946
72*75*
0
10
20
30
40
50
60
70
80
GLIM ROSI ROSI+GLIM4/4
ROSI+GLIM8/4
7
37
Effect of Sitagliptin + MET on A1C in Effect of Sitagliptin + MET on A1C in Patients With Type 2 Diabetes*Patients With Type 2 Diabetes*
Sitagliptin Improves Glycemic Control in Sitagliptin Improves Glycemic Control in Patients With Type 2 Diabetes Not Patients With Type 2 Diabetes Not
Controlled With PIOControlled With PIO
• Patients (N=353) with A1C between 7% and 10% were randomized (1:1) to addition of placebo or sitagliptin100 mg qd to ongoing PIO for 24 weeks
• Significant reductions in fasting serum proinsulin levels and the proinsulin/insulin ratio were observed with sitagliptin compared with placebo (P<.01 for both)
<.0014523Patients with
A1C <7% (%)
<.001–17.7—FPG (mg/dL)*
<.001–.70—Δ A1C (%)*
PSitagliptin +
PIOPlacebo +
PIO
*Values shown reflect subtraction of placebo.Rosenstock J et al. Clin Ther. 2006;28:1556-1568.
39
Effect of Effect of ExenatideExenatide + TZD on Body Weight + TZD on Body Weight in Patients With Type 2 Diabetesin Patients With Type 2 Diabetes
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
1.0
0 4 8 12 16
Weeks
Body
Wei
ght
Chan
ge
(kg)
Exenatide + TZD (n=121)
Placebo + TZD (n=110)
*P<.01; †P<.001.
CI=confidence interval
Zinman B et al. Ann Intern Med. 2007;146:477-485.
-1.51 kg (95% CI, -2.15 to -.88 kg; P<.001)
*
†† †
4040
Highlights of Clinical TrialsHighlights of Clinical Trials
41
DREAM Primary Outcome: DREAM Primary Outcome: Prevention of Type 2 Diabetes or DeathPrevention of Type 2 Diabetes or Death
DREAM=Diabetes Reduction Approaches with Ramipril and Rosiglitazone Medications; HR=hazard ratio
DREAM Investigators. Lancet. 2006;368:1096-1105.
0.0
0.1
0.2
0.3
0.4
0.5
0.6
Year
Cum
ulat
ive
Haz
ard
ROSI
Placebo
0 1 2 3 4
HR=0.40 (0.35-0.46); P<.0001
Number at RiskPlacebo 2634 2470 2150 1148 177ROSI 2635 2538 2414 1310 217
60%
42
ROSI Reduces the Development of Renal ROSI Reduces the Development of Renal Disease (DREAM Trial 2008)Disease (DREAM Trial 2008)
1.18 (0.88-1.57)§185 (48.7)193 (52.5)Microalbuminuriaregression to normal
The DREAM Trial Investigators. Diabetes Care. 2008;31:1007-1014.
8
43
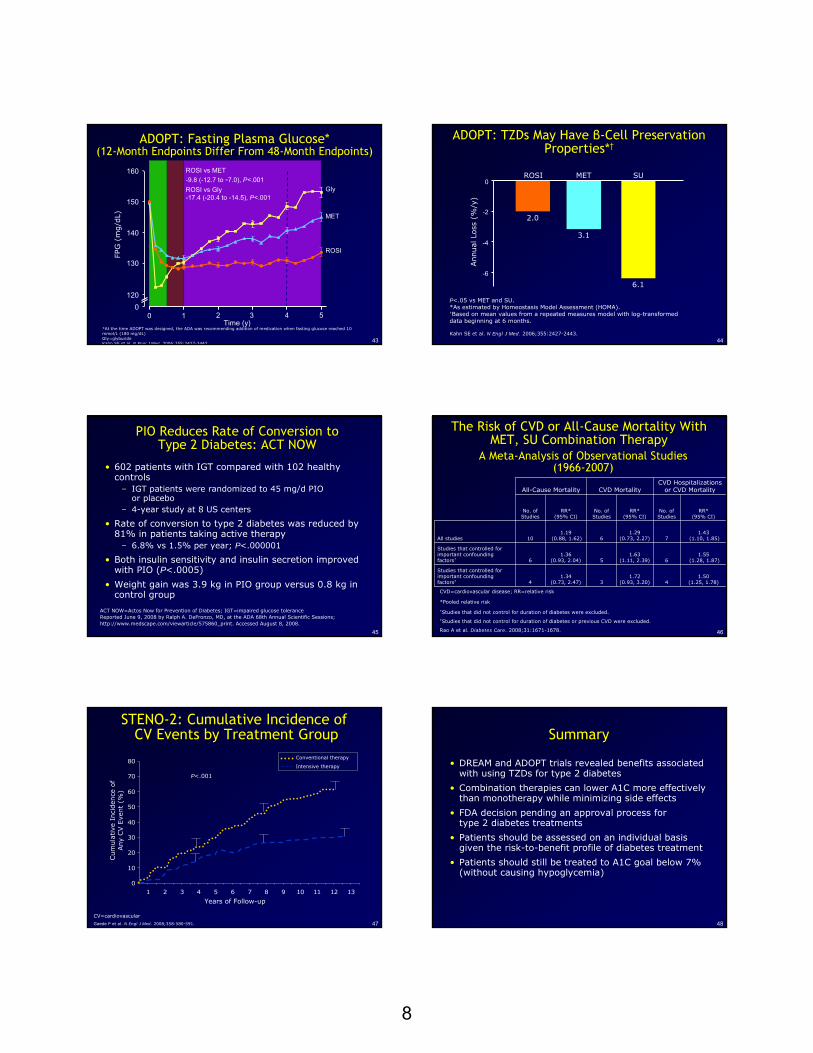
ADOPT: Fasting Plasma Glucose*ADOPT: Fasting Plasma Glucose*(12(12--Month Endpoints Differ From 48Month Endpoints Differ From 48--Month Endpoints)Month Endpoints)
Gly
MET
ROSI
ROSI vs MET-9.8 (-12.7 to -7.0), P<.001ROSI vs Gly-17.4 (-20.4 to -14.5), P<.001
FPG
(m
g/d
L)
0120
160
140
130
150
0 1 2 3 4 5Time (y)
*At the time ADOPT was designed, the ADA was recommending addition of medication when fasting glucose reached 10 mmol/L (180 mg/dL)Gly=glyburideKahn SE et al. N Engl J Med. 2006;355:2427-2443.
44
ADOPT: TZDs May Have ADOPT: TZDs May Have ββ--Cell Preservation Cell Preservation Properties*Properties*††
Annual Lo
ss (
%/y
)
-6
-4
-2
0ROSI SUMET
2.0
3.1
6.1
P<.05 vs MET and SU.*As estimated by Homeostasis Model Assessment (HOMA).†Based on mean values from a repeated measures model with log-transformed data beginning at 6 months.
Kahn SE et al. N Engl J Med. 2006;355:2427-2443.
45
PIO Reduces Rate of Conversion to PIO Reduces Rate of Conversion to Type 2 Diabetes: ACT NOWType 2 Diabetes: ACT NOW
• 602 patients with IGT compared with 102 healthy controls
– IGT patients were randomized to 45 mg/d PIO or placebo
– 4-year study at 8 US centers
• Rate of conversion to type 2 diabetes was reduced by 81% in patients taking active therapy
– 6.8% vs 1.5% per year; P<.000001
• Both insulin sensitivity and insulin secretion improved with PIO (P<.0005)
• Weight gain was 3.9 kg in PIO group versus 0.8 kg in control group
ACT NOW=Actos Now for Prevention of Diabetes; IGT=impaired glucose toleranceReported June 9, 2008 by Ralph A. DeFronzo, MD, at the ADA 68th Annual Scientific Sessions; http://www.medscape.com/viewarticle/575860_print. Accessed August 8, 2008.
46
The Risk of CVD or AllThe Risk of CVD or All--Cause Mortality With Cause Mortality With MET, SU Combination TherapyMET, SU Combination Therapy
A MetaA Meta--Analysis of Observational StudiesAnalysis of Observational Studies(1966(1966--2007)2007)
1.50 (1.25, 1.78)4
1.72 (0.93, 3.20)3
1.34 (0.73, 2.47)4
Studies that controlled for important confounding factors‡
1.55(1.28, 1.87)6
1.63 (1.11, 2.39)5
1.36 (0.93, 2.04)6
Studies that controlled for important confounding factors†
1.43(1.10, 1.85)7
1.29 (0.73, 2.27)6
1.19(0.88, 1.62)10All studies
RR* (95% CI)
No. of Studies
RR* (95% CI)
No. of Studies
RR* (95% CI)
No. of Studies
CVD Hospitalizations or CVD MortalityCVD MortalityAll-Cause Mortality
CVD=cardiovascular disease; RR=relative risk
*Pooled relative risk
†Studies that did not control for duration of diabetes were excluded.‡Studies that did not control for duration of diabetes or previous CVD were excluded.
Rao A et al. Diabetes Care. 2008;31:1671-1678.
47
STENOSTENO--2: Cumulative Incidence of2: Cumulative Incidence ofCV Events by Treatment GroupCV Events by Treatment Group
CV=cardiovascular
Gaede P et al. N Engl J Med. 2008;358:580-591.
0
10
20
30
40
50
60
70
80
1 2 3 4 5 6 7 8 9 10 11 12 13
P<.001
Cum
ula
tive
Inci
den
ce o
f Any
CV E
vent
(%)
Years of Follow-up
Conventional therapy
Intensive therapy
48
SummarySummary
• DREAM and ADOPT trials revealed benefits associated with using TZDs for type 2 diabetes
• Combination therapies can lower A1C more effectively than monotherapy while minimizing side effects
• FDA decision pending an approval process for type 2 diabetes treatments
• Patients should be assessed on an individual basis given the risk-to-benefit profile of diabetes treatment
• Patients should still be treated to A1C goal below 7% (without causing hypoglycemia)