1
Characterization of rough and smooth morphotypes of Mycobacterium 1
abscessus isolated from clinical specimens 2
3
4
5
Kai Rüger#, Annegret Hampel#, Sandra Billig, Nadine Rücker, Sebastian Suerbaum, and 6
Franz-Christoph Bange* 7
8
9
10
11
12
From the Department of Medical Microbiology and Hospital Epidemiology, Hannover Medical 13
School, Carl-Neuberg-Strasse 1, 30625 Hannover, Germany 14
15
16
# contributed equally 17
18
* Corresponding author. Department of Medical Microbiology and Hospital Epidemiology, 19
Medical School Hannover, Carl-Neuberg-Strasse 1, 30625 Hannover, Germany; phone: 20
++49-511-532-4359; fax: ++49-511-532-4366; e-mail: [email protected] 21
22
23
24
JCM Accepts, published online ahead of print on 6 November 2013J. Clin. Microbiol. doi:10.1128/JCM.01249-13Copyright © 2013, American Society for Microbiology. All Rights Reserved.
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
2
Abstract 25
26
Mycobacterium abscessus, which consists of the two subspecies abscessus and bolletii, can 27
produce rough or smooth colony morphologies. Here we analyzed 50 M. abscessus isolates 28
cultured from the respiratory specimens of 34 patients, 28 (82%) of whom had cystic fibrosis 29
(CF), with respect to their colony morphology and antibiotic susceptibility. The overall 30
proportion of occurrence of either morphotype was similar, with 50% of patients showing a 31
rough and 38% showing a smooth morphotype. 12% of patients showed both morphotypes 32
simultaneously. At a subspecies level, the proportion of rough and smooth morphotypes 33
differed substantially. 88% of rough morphotypes belonged to M. abscessus subspecies 34
abscessus, and 85% of smooth morphotypes belonged M. abscessus subspecies bolletii. 35
Inducible clarithromycin resistance due to the Erm(41) methylase, as well as high level 36
resistance against clarithromycin due to mutations within the rrl gene occurred independently 37
of the morphotype. MIC50 of amikacin and cefoxitin were identical for both morphotypes, 38
whereas MIC50 of tigecycline was 0.25 µg / mL for the rough morphotype, and 2.0 µg / mL for 39
the smooth morphotype. Our results show that the smooth morphotype was more dominating 40
in respiratory specimens from CF patients than previously thought. With respect to 41
resistance, colony morphology did not affect susceptibility of Mycobacterium abscessus to 42
the first line antibiotics clarithromycin, amikacin and cefoxitin. 43
44
45
46
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
3
Introduction 47
48
The genus Mycobacterium (M.) contains more than 100 different species which 49
belong either to the Mycobacterium tuberculosis complex or to the large group of non-50
tuberculous mycobacteria (NTMs). M. abscessus is an NTM, and clinical studies have begun 51
to shed light on its epidemiology. M. abscessus is involved in soft tissue infections, and a 52
dominant respiratory pathogen in patients with cystic fibrosis (CF). It is the second most 53
common NTM isolated from CF patients in the United States, and the most common NTM 54
isolated from CF patients in Europe (1-6). Fatal infections with M. abscessus have been 55
reported, especially after lung transplantation (7). M. abscessus was subdivided in type I and 56
type II, which, together with Mycobacterium chelonae, share an identical 16S rRNA gene, but 57
show differences within the hsp65 gene (8, 9). Based on multilocus sequence analysis of 58
hsp65, rpoB, secA and the 16S-23S internal transcribed spacer (ITS) region, the M. 59
abscessus was further subdivided into three species, M. abscessus (sensu stricto), M. 60
bolletii, and M. massiliense (10, 11). Recently, it has been proposed to unite M. bolletii and 61
M. massiliense as M. abscessus subspecies bolletii (the former type II) and separate it from 62
M. abscessus subspecies abscessus (the former type I) (12). 63
M. abscessus colonies on agar plates grow with either a rough or a smooth 64
morphology (13, 14). M. abscessus can show cord formation when visualized microscopically 65
(15). Production of a glycopeptidolipid (GPL) masks the cord forming structures of the 66
mycobacterial cell wall. Macroscopically, cord forming M. abscessus grow with the rough 67
morphotype, and non-cord forming, GPL-producing M. abscessus grow with the smooth 68
morphotype (14). The presence of GPL is associated with lesser virulence. A rough clinical 69
isolate persisted in the lungs of experimentally infected mice and disseminated into the 70
spleen, whereas a smooth isolate was cleared from the lungs within three weeks (16). An 71
isogenic mutant of M. abscessus that lacked GPL production lost biofilm formation, but 72
gained the ability to replicate inside macrophages, stimulate Toll-like receptor 2, and induce 73
cytokine production (17, 18). It has also been suggested that the rough morphotype is more 74
virulent in humans (19). 75
In a previous study looking at the epidemiology of M. abscessus, 12 rough but only 1 76
smooth morphotype was isolated from the respiratory tract of CF-patients (13). At present, it 77
is not known whether clinical isolates of smooth and rough morphotypes of M. abscessus 78
differ in the antimicrobial susceptibility. Macrolides such as clarithromycin are first line 79
antibiotics for treatment of pulmonary disease caused by M. abscessus subspecies bolletii. 80
Due to the presence of the inducible methylase Erm(41) which confers macrolide resistance 81
in M. abscessus subspecies abscessus, response rates to clarithromycin are lower for this 82
subspecies (20-22). Amikacin and cefoxitin are the two other first line antibiotics for the 83
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
4
treatment of M. abscessus (23). M. abscessus are generally resistant to fluoroquinolones, 84
doxycycline and minocycline. A newer tetracycline, tigecycline, has shown in vitro activity 85
against M. abscessus (24, 25), but its role in treatment of disease has yet to be established. 86
In this study, we compared the proportion of the occurrence of rough and smooth 87
morphotypes of M. abscessus isolated from the respiratory tract of 34 patients, 28 of whom 88
had cystic fibrosis, and analyzed the susceptibility patterns to clarithromycin, amikacin, 89
cefoxitin and tigecycline of the two morphotypes. 90
91
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
5
Materials and Methods 92
93
Strains and Cultures. We searched the Laboratory Information System of the 94
Department of Medical Microbiology and Hospital Epidemiology of the Hannover Medical 95
School for patients from whose respiratory tract M. abscessus was cultured between 01/2000 96
and 12/2011. Isolates were then recultured from frozen stocks on 7H11-agar at 37°C for 7 97
days, and colony morphology was determined. From patients with more than one isolate, the 98
last available isolate was included in this study, when cultured at least one year after the first 99
isolate, and was termed “second“ isolate. Colonies from plates were used directly for 100
inoculation of RAPMYCO Sensititre® 96 well plates (susceptibility testing), and for pulse field 101
gel electrophoresis. For all DNA-sequencing procedures, colonies were subcultured in 7H9 102
liquid medium, and genomic DNA was extracted. 103
Isolation and identification of M. abscessus from patient samples. All specimens 104
were processed in the MGIT culture system (Becton Dickenson). In our laboratory, cultures 105
that grow acid fast bacilli are initially subjected to 16S rRNA gene sequencing. Those 106
identified as M. chelonae / M. abscessus complex are subsequently analyzed by a Light-107
Cycler targeting the hsp65 gene that allows differentiation of M. chelonae, M. abscessus 108
subspecies abscessus (type I) and M. abscessus subspecies bolletii (type II) as described 109
previously (9). 110
Phenotypic resistance. 50 isolates of M. abscessus from 34 patients were tested. 111
30 first isolates from 30 patients that had only one of the two morphotypes, 8 first isolates 112
form 4 patients with had a rough and smooth morphotypes simultaneously, and 12 second 113
isolates. Overall we tested 29 rough and 21 smooth isolates. Phenotypic resistance was 114
tested with RAPMYCO Sensititre® 96 well plates (TREK DIAGNOSTIC SYSTEMS), as 115
recommended by the manufacturer. Briefly, bacterial colonies were harvested, and diluted in 116
water to a McFarland standard 0.5. 50 µL of the solution were transferred into cation-117
adjusted Mueller-Hinton-Broth, and finally 100 µL of the bacteria / Mueller-Hinton-Broth 118
suspension was transferred into each well of the RAPMYCO Sensititre® 96 well plates. 119
Plates were incubated at 30°C, and manually assessed on day 5 and 14. For quality control 120
we used Staphylococcus aureus ATCC 29213. 121
Genotypic analysis of erm(41), rrl, and rrs. PCR was done with a T Professional-122
Cycler (Biometra) using Taq-Polymerase (New England Biolabs) in a 25 µL assay. The 123
erm(41) gene was amplified with forward primer erm41KRforward_#615 124
(5’_AAGATGCACACCGTGCAGATG_3’) and reverse primer erm41KRreverse_#616 125
(5’_ACATCGCTGTCCACGATGAAAG_3’) at 65°C annealing temperature resulting in a 126
934 bp or 658 bp fragment. Fragment size was analyzed on an agarose gel. Subsequent 127
sequencing was done using the forward primer. The rrl gene was amplified with forward 128
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
6
primer # 18 (5’_AGTCGGGACCTAAGGCGAG_3’) and reverse primer # 21 129
(5’_TTCCCGCTTAGATGCTTTCAG_3’) as published by Meier et al. with an annealing 130
temperature of 62°C resulting in a 1525 bp fragment. Subsequent sequencing was done 131
using the primer # 19 (5’_GTAGCGAAATTCCTTGTCGG_3’) (26). The rrs gene was 132
amplified using forward primer # 283 (5’_GAGTTTGATCCTGGCTCAGGA_3’) and reverse 133
primer # 261 (5’_AAGGAGGTGATCCAGCCGCA_3’) as published by Prammananan et al. 134
with an annealing temperature of 65°C resulting in a fragment of 1507 bp. Subsequent 135
sequencing was done using the primer # 289 (5’_AAGTCGGGAGTCGCTAGTAAT_3’) (27). 136
Amplification of erm(41), rrl and rrs was done in 35 cycles with 30 seconds of denaturation at 137
96°C, and 60 seconds of elongation at 68°C, including a final elongation step for 5 min. 138
Pulsed Field Gel Electrophoresis. Bacterial colonies were harvested from 7H11 139
agar, dissolved in 5 mL 7H9, and cultured for 72 hours and 37°C. 400 µL of lysis solution 140
containing 0.2 M glycine, 60 µg / mL D-cycloserine, 20 mM lithium chloride, 200 mg/mL 141
lysozyme and 5 mM EDTA was added and incubated for 16 h and 37°C. Cells were 142
harvested by centrifugation at 3000 x g for 15 min resuspended in TS-buffer (50 mM Tris, 143
0.5 M sucrose, pH 7.6) and aliquots of 250 µL were frozen at -20°C. The aliquots were 144
thawed at room temperature and heated to 75°C for 20 min. 200 µL of lysed cells were 145
casted into a gel block using 2% low-melting-point agarose. Cell lysis was performed by 146
adding lysostaphin for 15 min at room temperature, and lysozyme over night at 37°C, 147
proteinase K and SDS for 20 h at 55°C (13). For DNA digestion we used XbaI. Digestion was 148
performed for approximately 18 h at 37°C. Our protocol consisted of initial time 3 s, final time 149
12 s, runtime 20 h, temperature 14°C, voltage 200 V, agarose concentration 1%, buffer 150
0,5xTBE. Staining was done with ethidium bromide. 151
DNA Sequencing of msp1. Analysis of msp1 was done as decribed (28). Briefly, the 152
5’ part of the msp1 gene containing a potential CG insertion was amplified. 5 µl of the purified 153
chromosomal DNA of both morphotypes from the patients P2, P17, P31 and P37 were added 154
as a template to a reaction mix containing 20 mM Tris-HCl (pH 8), 50 mM KCl, 1.5 mM 155
MgCl2, 250 µM dNTPs, 10 pmol of primers # 767 (5’ AAAAGGCGACGGATATTCAA 3’) and 156
# 768 (5’ GAGTATCGGCGAATCCGTAA 3’) and 2.5 U Taq-DNA polymerase (Invitrogen, life 157
technologies). 35 PCR cylces were performed using the following conditions: 95°C for one 158
minute, 52°C for 30 seconds and 68°C for one minute. The purified PCR fragments had a 159
length of about 450 bp and their nucleotide sequence was analysed by using the ABI PRISM 160
BigDye Terminator Cycle Sequencing v1.1 Ready Reaction Kit (Applied Biosystems, Austin, 161
USA) and the # 767 primer. 162
Stability testing of the morphotypes. The original samples of the patients P2, P17, 163
P31 and P37 were plated on 7H11 agar plates and single colonies presenting the smooth 164
and rough morphotype were isolated and subcultured as next generation on 7H11 agar 165
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
7
plates. The subculture of each morphotype was repeated for 12 generations. In addition, 166
frozen stocks of the stabilized morphotypes from patients P2, P17, P31 and P37 were 167
thawed and plated on 7H11 agar plates. The stocks were afterwards refrozen at -20°C. The 168
procedure was repeated for 12 cycles and the morphotypes were checked for stability. 169
170
171
172 173
174
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
8
Results 175
176
Detection of rough and smooth morphotypes in clinical specimens. Figure 1 177
shows appearance of rough and smooth morphotypes of M. abscessus. When we re-cultured 178
frozen stocks from 34 patients, 28 of whom had CF, 30 patients had either the rough or 179
smooth morphotype. Of these, 17 (50%) had a rough morphotype, and 13 (38.2%) had a 180
smooth morphotype. In the 28 CF-patients, 14 (50%) showed a rough morphotype, and 13 181
(46.4%) a smooth morphotype. In four patients (P2, P17, P31, P37), the cultures form the 182
frozen stocks produced rough and smooth colonies simultaneously (Figure 2). From each 183
patient we took a smooth and a rough colony and generated 12 sequential subcultures on 184
7H11 agar plates. Rough and smooth morphotypes from two patients (P2 and P17) were 185
stable on the first subculture, from one patient (P37) on the second subculture, and from one 186
patient (P31) on the eighth subculture. Using pulse field gel electrophoresis, we found that 187
rough and smooth morphotypes were indistinguishable in each of the four patients (Figure 2). 188
We submitted a stable rough and smooth subculture from each of the four patients to 12 189
subsequent freeze/thaw cycles and found that colony morphology did not change. The 190
majority of rough morphotypes belonged to M. abscessus subspecies abscessus, the 191
majority of smooth morphotypes belonged to M. abscessus subspecies bolletii (Table 1). 192
From 12 of the 34 patients a second isolate was available. The range of time laps between 193
first and second isolate was 1.3 to 9.4 years. Morphology of the first and the second isolate 194
was identical in 11 patients. One patient showed both morphotypes in his first specimen. The 195
second specimen showed only the rough morphotype. Pulse field gel electrophoresis 196
revealed clonal identity between first and second isolate for each of the 12 patients. 197
In a recent publication, the genomes and transcriptomes of smooth and rough 198
variants of three M. abscessus strains, two laboratory strains and one clinical strain from a 199
patient with cystic fibrosis, were compared (28). The switch from a smooth to a rough 200
morphotype of M. abscessus was associated with the down regulation of the msp1-msp2-201
gap operon in all three rough variants. This operon encodes two non-ribosomal peptide 202
synthases and a glycopetide transport gene. The genome of one rough variant revealed a 203
CG insertion within the 5’ part of the msp1, which caused a frame shift, leading to 204
transcriptional arrest of the msp1-msp2-gap operon (28). We compared the 5’ part of msp1 205
from the 4 rough and 4 smooth strains that we obtained from the four patients with the mixed 206
morphotype (P2, P17, P31, P37, see also figure 2). None of the rough strains carried the CG 207
insertion in the 5’ part of msp1, indicating that at least in these 4 isogenic smooth / rough 208
pairs the morphotypic switch was not caused by the CG insertion within the msp1 gene. 209
MICs of clarithromycin in smooth and rough morphotypes. We tested 50 isolates 210
from 34 patients, 29 rough and 21 smooth isolates. A suspension of bacteria grown on agar 211
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
9
plates was inoculated in 96-wells, and MICs for clarithromycin were read on day 5 and 14. 212
Rough and smooth isolates had a MIC50 of 0.5 µg / mL on day 5. By day 14, the rough 213
isolates had an MIC50 of >16 µg / mL, whereas smooth isolates had an MIC50 of 1 µg / mL, 214
indicating the presence of an inducible clarithromycin resistance in rough isolates. 215
Stratification of rough and smooth morphotypes to the level of subspecies showed that the 216
inducible clarithromycin resistance occurred more frequently in M. abscessus subspecies 217
abscessus than in M. abscessus subspecies bolleti. By day 14 both rough and smooth 218
morphotypes of M. abscessus subspecies abscessus had an MIC50 of >16 µg / mL, whereas 219
rough morphotypes of M. abscessus subspecies bolletii had an MIC50 of 2 µg / mL, and 220
smooth morphotypes had an MIC50 of 1 µg / mL. Non-inducible, high-level resistance to 221
clarithromycin, which was defined as an MIC >16 µg / mL on day 5, was detected in 9 of 50 222
isolates, 5 with a rough and 4 with a smooth morphotype.. In all 50 isolates we sequenced 223
the gene erm(41), which encodes a methylase that mediates inducible clarithromycin 224
resistance in M. abscessus (20). 69% of rough isolates and 19% of smooth isolates had the 225
wild type allele (Table 3). 31% of rough morphotypes, and 81% of smooth morphotypes had 226
either a 276 bp deletion or a single nucleotide polymorphism at position 28 (TsC) of the 227
erm(41) (Table 3). Both mutations lead to the loss of the inducible clarithromycin resistance 228
(20, 21). 229
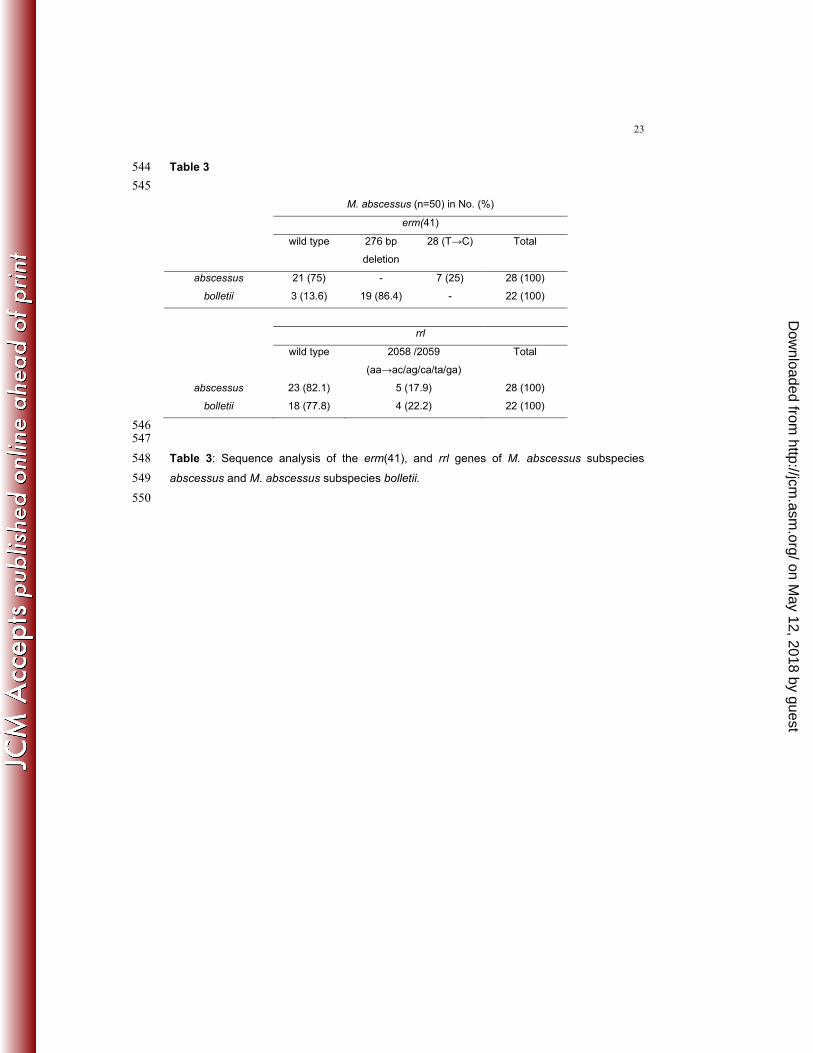
Bastian and colleagues showed that within the erm(41) gene the TsC mutation 230
occurs only in M. abscessus subspecies abscessus, and the 276 bp deletion occurs only in 231
M. abscessus subspecies bolletii (21). They also found that 77% M. abscessus subspecies 232
abscessus and 41% of M. abscessus subspecies bolletii had the wild type erm(41). Thus we 233
stratified the genotypic analysis of the erm(41) of the 50 clinical isolates from this study 234
according to two subspecies of M. abscessus. 75 % of M. abscessus subspecies abscessus 235
and 13.6 % of M. abscessus subspecies bolletii carried the wild type erm(41) (Table 4). The 236
276 bp deletion was exclusively present in M. absecssus subspecies bolletii, whereas the 237
TsC was exclusively present in M. abscessus subspecies abscessus (Table 4). 238
Mutations at position 2058 and 2059 of the rrl gene, which causes high-level 239
resistance to clarithromycin (29), were present in all 9 strains with MIC >16 µg / mL on day 5. 240
(Table 3). Of these 9 isolates four (P2, P3, P6, and P14) were second isolates, three of 241
which (P2, P3, and P14) had a corresponding first isolate without high-level clarithromycin 242
resistance (Table 5) suggesting development of high level resistance against clarithromycin 243
in vivo. Interestingly, 2 of the 9 strains with high level resistance had a functional erm(41), 244
showing the presence of both inducible and high level resistance against clarithromycin. 245
MICs of amikacin in smooth and rough morphotypes. In M. abscessus MIC50 of 246
amikacin was 16 µg / mL and did not vary between rough and smooth morphotypes. Of 50 247
isolates, 8 showed high level resistance against amikacin, as defined by a MIC ≥ 64 µg / mL, 248
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
10
4 with a rough morphotype and 4 with a smooth morphotype. Of the 8 isolates, 4 (P2, P3, P4, 249
and P6) were second isolates, three of which (P2, P3, and P4) had a corresponding first 250
isolate without high-level aminoglycoside resistance (Table 4), suggesting development of 251
high level resistance against aminoglycoside in vivo. 7 strains with a MIC ≥ 64 µg / mL had a 252
single nucleotide polymorphism at position 1408 (AsG) of the rrs gene, which had been 253
shown to mediate high-level aminoglycoside resistance in M. abscessus (27). 254
MICs of cefoxitin, doxycycline, minocycline, and tigecycline. Besides 255
clarithromycin and amikacin, cefoxitin is frequently used for treatment of M. abscessus 256
infection. For cefoxitin we found a MIC50 of 64 µg / mL and a MIC90 of 128 µg / mL that did 257
not vary between rough and smooth morphotypes of M. abscessus. We also tested 258
tetracyclins such as doxycycline, minocycline, and tigecycline. Doxycycline and minocycline 259
had a MIC50 and MIC90 above 8µg / mL both in rough and in smooth morphotypes. In 260
contrast, MICs were lower for tigecycline and differed between rough, which had an MIC50 of 261
0.25 µg / mL and an MIC90 of 1 µg / mL, and smooth isolates which had an MIC50 of 2 µg / 262
mL, and an MIC90 > 4 µg / mL. 263
264
265
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
11
Discussion 266
267
In this study we investigated the prevalence and antibiotic susceptibility of rough and 268
smooth morphotypes in the respiratory specimens from 34 patients most of which had cystic 269
fibrosis. Even though isolates with rough morphotypes occurred more frequently than those 270
with smooth morphotypes (50% and 38%), our results show that in CF patients the rough 271
morphotype was less dominating in respiratory specimens than previously thought. 272
Proportions found in a study from Korea were 61% for rough and 28% for smooth 273
morphotypes (30). A study from Sweden found 12 rough but only 1 smooth isolate in the 274
respiratory tract of CF-patients (13). Looking at a subspecies level, in this present study the 275
proportion of smooth morphotypes were low (15%) in M. abscessus subspecies abscessus, 276
and high in M. abscessus subspecies bolletii (85%). This differs from the proportion found in 277
the Korea population, where the prevalence of smooth morphotypes were low in both 278
subspecies (27% and 28%) (30). Even though the population sizes studied so far are still 279
small, there appears to be no clear dominance of either morphotype in a given population or 280
between the two subspecies. Together, these findings suggest that the distribution M. 281
abscessus with rough and smooth colony morphology within the respiratory tract of affected 282
patients shows regional diversity, and that at least in CF patients it is not confined to one of 283
the two distinct subspecies of M. abscessus. 284
In rough and smooth morphotypes, we did not find a difference in MIC50 (= 16 µg / mL 285
for both morphotypes) for amikacin. In patients with cystic fibrosis, mucoid morphotypes of 286
Pseudomonas aeruginosa form biofilm and show resistance to a wide range of antibiotics 287
(31). Initially, it was thought that the extracelluar matrix (alginate) produced by mucoid strains 288
act as physical barrier to antibiotics. However, later it became evident that the broad range of 289
antibiotic resistances of Pseudomonas aeruginosa isolates in CF-patients is due to so called 290
hypermutators that assemble classic resistance mechanisms such as target mutations (32, 291
33). Nonetheless, treatment with alginate lysis of mucoid isolates of Pseudomonas 292
aeruginosa enhances susceptibility to tobramycin, indicating that at least for aminoglycoside 293
alginate acts as a physical barrier (34). Our study suggest, that glycopeptidolipid of M. 294
abscessus has no immediate effect on the antimicrobial action of amikacin. 295
Inducible clarithromycin resistance was higher in rough than in smooth morphotypes. 296
Loss of inducible clarithromycin resistance is caused by a deletion or a nucleotide 297
polymorphism within erm(41) (20, 21). The deletion is absent in M. abscessus subspecies 298
abscessus, and frequently present in M. abscessus subspecies bolletii (21). In this study, 299
88% of rough morphotypes belonged to M. abscessus subspecies abscessus, and 85% of 300
smooth morphotypes belonged to M. abscessus subspecies bolletii. Thus differences in the 301
proportion of inducible clarithromycin resistance between smooth and rough isolates are the 302
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
12
result of a higher proportion of M. abscessus subspecies abscessus among rough isolates, 303
and M. abscessus subspecies bolletii among smooth isolates, respectively. It is note worthy, 304
that we found 2 isolates which had a 23S rRNA mutation at position 2058/59 despite the 305
presence of the Erm methylase. Acquisition of high level clarithromycin resistance in the 306
presence of the Erm methylase has been demonstrated in vivo in a recent study, and it has 307
been suggested that a mutation at position 2058/59 of 23S rRNA provides an advantage that 308
is independent of a functional erm(41) gene (35). 309
In previous studies, of the tetracyclines, only tigecycline has been shown to be 310
effective against M. abscessus in vitro. Wallace and colleagues reported MICs of > 64 µg / 311
mL for minocycline and a MIC50 = 0.12 µg / mL for tigecycline (41). Another study reported a 312
MIC50 of 0.5 µg / mL for tigecycline, and an MIC50 of 32 µg / mL for doxycycline (25). Our 313
results suggest that for further evaluations of the efficacy of tigecycline for the treatment of 314
M. abscessus, the testing of the morphotype should be included. At present, we have no 315
mechanistic explanation as to why tigecycline shows higher MICs in smooth compared to 316
rough morphotypes. It is unclear whether glycopeptidolipids directly interfere with the drug. 317
In summary, we found no difference in susceptibility towards the two first-line 318
antibiotics amikacin and cefoxitin between rough and smooth morphotypes of Mycobacterium 319
abscessus that were isolated from CF patients. The higher rate of inducible resistance 320
against clarithromycin in rough morphotypes was due to a higher prevalence of 321
Mycobacterium abscessus subspecies abscessus in this group, which carries an inducible 322
methylase that mediates clarithromycin resistance. Therefore, with respect to the decisions 323
on antibiotic treatment, we see no immediate benefit in differentiating between the two 324
morphotypes by the clinical laboratory. Based on this and previous work, with respect to 325
diagnostics in the clinical microbiology, we would like to discuss the following. It might be 326
useful to further differentiate M. abscessus to obtain more information about differences in 327
epidemiology and virulence between the two subspecies. Differentiation can be achieved by 328
analysis of hsp65 gene polymorphism (8, 9). Subspecies differentiation could also serve as a 329
surrogate marker for inducible clarithromycin resistance. Yet it should be stressed, that in 330
strains isolated from CF-patients in this study, a subgroup of M. abscessus subspecies 331
bolletii (13.6%, see table 3) has a functional erm(41) and a subgroup of M. abscessus 332
subspecies abscessus lacks a functional erm(41) (25% study, table 3). Phenotypic testing for 333
antibiotic resistance might be useful for guiding antibiotic treatment. However, except for 334
clarithromycin resistance, the poor correlation between in-vitro drug susceptibility results and 335
clinical response to antibiotic treatment is of concern (36). The unambiguous detection of an 336
inducible clarithromycin resistance requires the sequencing of the erm(41) gene (21). The 337
proportion of strains with high level resistance against clarithromycin and amikacin was 338
between 10% and 20% in this study, thus partial sequencing of the 16S rRNA and 23S rRNA 339
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
13
to detect high level resistance against clarithromycin and amikacin should be considered and 340
based on the individual case. 341
342
343
344
345
Acknowledgments: 346
347
Funding: The work was supported by the Niedersächsische Verein zur Bekämpfung 348
der Tuberkulose, Lungen- und Bronchialerkrankungen, and by the International Research 349
Training Group 1273 funded by the German Research Foundation to SB. 350
351
352
Transparency declaration: None to declare 353
354
355
356
357
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
14
358
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
15
359
360
Reference List 361
362
363
364
365
366
1. Bange FC, Kirschner P, Bottger EC. 1999. Recovery of mycobacteria from patients 367
with cystic fibrosis. J. Clin. Microbiol. 37:3761-3763. 368
2. Bange FC, Brown BA, Smaczny C, Wallace Jr RJ, Bottger EC. 2001. Lack of 369
Transmission of Mycobacterium abscessus among Patients with Cystic Fibrosis 370
Attending a Single Clinic. Clin. Infect. Dis. 32:1648-1650. 371
3. Bange FC, Bottger EC. 2002. Improved decontamination method for recovering 372
mycobacteria from patients with cystic fibrosis. Eur. J. Clin. Microbiol. Infect. Dis. 373
21:546-548. 374
4. Olivier KN, Weber DJ, Wallace RJ, Jr., Faiz AR, Lee JH, Zhang Y, Brown-Elliot 375
BA, Handler A, Wilson RW, Schechter MS, Edwards LJ, Chakraborti S, Knowles 376
MR. 2003. Nontuberculous mycobacteria. I: multicenter prevalence study in cystic 377
fibrosis. Am. J. Respir. Crit Care Med. 167:828-834. 378
5. Giron RM, Maiz L, Barrio I, Martinez MT, Salcedo A, Prados C. 2008. 379
[Nontuberculous mycobacterial infection in patients with cystic fibrosis: a multicenter 380
prevalence study]. Arch. Bronconeumol. 44:679-684. 381
6. Roux AL, Catherinot E, Ripoll F, Soismier N, Macheras E, Ravilly S, Bellis G, 382
Vibet MA, Le Roux E, Lemonnier L, Gutierrez C, Vincent V, Fauroux B, Rottman 383
M, Guillemot D, Gaillard JL. 2009. Multicenter study of prevalence of nontuberculous 384
mycobacteria in patients with cystic fibrosis in france. J. Clin. Microbiol. 47:4124-4128. 385
7. Zaidi S, Elidemir O, Heinle JS, McKenzie ED, Schecter MG, Kaplan SL, Dishop 386
MK, Kearney DL, Mallory GB. 2009. Mycobacterium abscessus in cystic fibrosis lung 387
transplant recipients: report of 2 cases and risk for recurrence. Transpl. Infect. Dis. 388
11:243-248. 389
8. Devallois A, Goh KS, Rastogi N. 1997. Rapid identification of mycobacteria to species 390
level by PCR-restriction fragment length polymorphism analysis of the hsp65 gene and 391
proposition of an algorithm to differentiate 34 mycobacterial species. J. Clin. Microbiol. 392
35:2969-2973. 393
9. Sedlacek L, Rifai M, Feldmann K, Bange FC. 2004. LightCycler-based differentiation 394
of Mycobacterium abscessus and Mycobacterium chelonae. J. Clin. Microbiol. 42:3284-395
3287. 396
10. Adekambi T, Reynaud-Gaubert M, Greub G, Gevaudan MJ, La Scola B, Raoult D, 397
Drancourt M. 2004. Amoebal coculture of "Mycobacterium massiliense" sp. nov. from 398
the sputum of a patient with hemoptoic 399
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
16
pneumonia. J. Clin. Microbiol. 42:5493-5501. 400
11. Adekambi T, Berger P, Raoult D, Drancourt M. 2006. rpoB gene sequence-based 401
characterization of emerging non-tuberculous mycobacteria with descriptions of 402
Mycobacterium bolletii sp. nov., Mycobacterium phocaicum sp. nov. and 403
Mycobacterium aubagnense sp. nov. Int. J. Syst. Evol. Microbiol. 56:133-143. 404
12. Leao SC, Tortoli E, Euzeby JP, Garcia MJ. 2011. Proposal that Mycobacterium 405
massiliense and Mycobacterium bolletii be united and reclassified as Mycobacterium 406
abscessus subsp. bolletii comb. nov., designation of Mycobacterium abscessus subsp. 407
abscessus subsp. nov. and emended description of Mycobacterium abscessus. Int. J. 408
Syst. Evol. Microbiol. 61:2311-2313. 409
13. Jonsson BE, Gilljam M, Lindblad A, Ridell M, Wold AE, Welinder-Olsson C. 2007. 410
Molecular epidemiology of Mycobacterium abscessus, with focus on cystic fibrosis. J. 411
Clin. Microbiol. 45:1497-1504. 412
14. Howard ST, Rhoades E, Recht J, Pang X, Alsup A, Kolter R, Lyons CR, Byrd TF. 413
2006. Spontaneous reversion of Mycobacterium abscessus from a smooth to a rough 414
morphotype is associated with reduced expression of glycopeptidolipid and 415
reacquisition of an invasive phenotype. Microbiology 152:1581-1590. 416
15. Sanchez-Chardi A, Olivares F, Byrd TF, Julian E, Brambilla C, Luquin M. 2011. 417
Demonstration of cord formation by rough Mycobacterium abscessus variants: 418
implications for the clinical microbiology laboratory. J. Clin. Microbiol. 49:2293-2295. 419
16. Byrd TF, Lyons CR. 1999. Preliminary characterization of a Mycobacterium abscessus 420
mutant in human and murine models of infection. Infect. Immun. 67:4700-4707. 421
17. Nessar R, Reyrat JM, Davidson LB, Byrd TF. 2011. Deletion of the mmpL4b gene in 422
the Mycobacterium abscessus glycopeptidolipid biosynthetic pathway results in loss of 423
surface colonization capability, but enhanced ability to replicate in human macrophages 424
and stimulate their innate immune response. Microbiology 157:1187-1195. 425
18. Davidson LB, Nessar R, Kempaiah P, Perkins DJ, Byrd TF. 2011. Mycobacterium 426
abscessus glycopeptidolipid prevents respiratory epithelial TLR2 signaling as measured 427
by HbetaD2 gene expression and IL-8 release. PLoS. One. 6:e29148. 428
19. Catherinot E, Roux AL, Macheras E, Hubert D, Matmar M, Dannhoffer L, Chinet 429
T, Morand P, Poyart C, Heym B, Rottman M, Gaillard JL, Herrmann JL. 2009. 430
Acute respiratory failure involving an R variant of Mycobacterium abscessus. J. Clin. 431
Microbiol. 47:271-274. 432
20. Nash KA, Brown-Elliott BA, Wallace RJ, Jr. 2009. A novel gene, erm(41), confers 433
inducible macrolide resistance to clinical isolates of Mycobacterium abscessus but is 434
absent from Mycobacterium chelonae. Antimicrob. Agents Chemother. 53:1367-1376. 435
21. Bastian S, Veziris N, Roux AL, Brossier F, Gaillard JL, Jarlier V, Cambau E. 436
2011. Assessment of clarithromycin susceptibility in strains belonging to the 437
Mycobacterium abscessus group by erm(41) and rrl sequencing. Antimicrob. Agents 438
Chemother. 55:775-781. 439
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
17
22. Koh WJ, Jeon K, Lee NY, Kim BJ, Kook YH, Lee SH, Park YK, Kim CK, Shin SJ, 440
Huitt GA, Daley CL, Kwon OJ. 2011. Clinical significance of differentiation of 441
Mycobacterium massiliense from Mycobacterium abscessus. Am. J. Respir. Crit Care 442
Med. 183:405-410. 443
23. Brown-Elliott BA, Nash KA, Wallace RJ, Jr. 2012. Antimicrobial susceptibility 444
testing, drug resistance mechanisms, and therapy of infections with nontuberculous 445
mycobacteria. Clin. Microbiol. Rev. 25:545-582. 446
24. Wallace RJ, Jr., Brown-Elliott BA, Crist CJ, Mann L, Wilson RW. 2002. 447
Comparison of the in vitro activity of the glycylcycline tigecycline (formerly GAR-936) 448
with those of tetracycline, minocycline, and doxycycline against isolates of 449
nontuberculous mycobacteria. Antimicrob. Agents Chemother. 46:3164-3167. 450
25. Huang YC, Liu MF, Shen GH, Lin CF, Kao CC, Liu PY, Shi ZY. 2010. Clinical 451
outcome of Mycobacterium abscessus infection and antimicrobial susceptibility testing. 452
J. Microbiol. Immunol. Infect. 43:401-406. 453
26. Meier A, Kirschner P, Springer B, Steingrube VA, Brown BA, Wallace RJ, Jr., 454
Bottger EC. 1994. Identification of mutations in 23S rRNA gene of clarithromycin-455
resistant Mycobacterium intracellulare. Antimicrob. Agents Chemother. 38:381-384. 456
27. Prammananan T, Sander P, Brown BA, Frischkorn K, Onyi GO, Zhang Y, Bottger 457
EC, Wallace RJ, Jr. 1998. A single 16S ribosomal RNA substitution is responsible for 458
resistance to amikacin and other 2-deoxystreptamine aminoglycosides in 459
Mycobacterium abscessus and Mycobacterium chelonae. J. Infect. Dis. 177:1573-1581. 460
28. Pawlik A, Garnier G, Orgeur M, Tong P, Lohan A, Le Chevalier F, Sapriel G, 461
Roux AL, Conlon K, Honore N, Dillies MA, Ma L, Bouchier C, Coppee JY, 462
Gaillard JL, Gordon SV, Loftus B, Brosch R, Herrmann JL. 2013. Identification 463
and characterization of the genetic changes responsible for the characteristic smooth-to-464
rough morphotype alterations of clinically persistent Mycobacterium abscessus. Mol. 465
Microbiol. 466
29. Wallace RJ, Jr., Meier A, Brown BA, Zhang Y, Sander P, Onyi GO, Bottger EC. 467
1996. Genetic basis for clarithromycin resistance among isolates of Mycobacterium 468
chelonae and Mycobacterium abscessus. Antimicrob. Agents Chemother. 40:1676-1681. 469
30. Kim HY, Kook Y, Yun YJ, Park CG, Lee NY, Shim TS, Kim BJ, Kook YH. 2008. 470
Proportions of Mycobacterium massiliense and Mycobacterium bolletii strains among 471
Korean Mycobacterium chelonae-Mycobacterium abscessus group isolates. J. Clin. 472
Microbiol. 46:3384-3390. 473
31. Hoiby N, Bjarnsholt T, Givskov M, Molin S, Ciofu O. 2010. Antibiotic resistance of 474
bacterial biofilms. Int. J. Antimicrob. Agents 35:322-332. 475
32. Oliver A, Canton R, Campo P, Baquero F, Blazquez J. 2000. High frequency of 476
hypermutable Pseudomonas aeruginosa in cystic fibrosis lung infection. Science 477
288:1251-1254. 478
33. Oliver A, Mena A. 2010. Bacterial hypermutation in cystic fibrosis, not only for 479
antibiotic resistance. Clin. Microbiol. Infect. 16:798-808. 480
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
18
34. Alipour M, Suntres ZE, Omri A. 2009. Importance of DNase and alginate lyase for 481
enhancing free and liposome encapsulated aminoglycoside activity against 482
Pseudomonas aeruginosa. J. Antimicrob. Chemother. 64:317-325. 483
35. Maurer FP, Ruegger V, Ritter C, Bloemberg GV, Bottger EC. 2012. Acquisition of 484
clarithromycin resistance mutations in the 23S rRNA gene of Mycobacterium abscessus 485
in the presence of inducible erm(41). J. Antimicrob. Chemother. 67:2606-2611. 486
36. Leung JM, Olivier KN. 2013. Nontuberculous mycobacteria: the changing 487
epidemiology and treatment challenges in cystic fibrosis. Curr. Opin. Pulm. Med. 488
19:662-669. 489
490 491
492
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
19
Figure 1: Growth characteristics of rough and smooth phenotypes on 7H11 agar cultured at 493
37°C: a representative single rough (left) and smooth (right) colony 494
495 496 497 498 Figure 2: Colony morphology of the primary subculture and results of pulse field gel 499
electrophoresis of rough and smooth strains of the four patients (P2, P17, P31, P37) that 500
produced a mixed phenotype; subcultures from primary specimens that had been kept as 501
frozen stocks were recultured on 7H11 agar at 37°C and photos were taken; two patients 502
(P2+P17) had predominantly rough morphotypes and two patients (P31 + P37) had 503
predominantly smooth morphotypes; from each patient one smooth and one rough colony 504
was subcultured until the morphotype remained stable before genomic DNA was prepared, 505
XbaI digested, and separated by pulse field gel electrophoresis; the gel photo shows a 506
comparison of the smooth (s) and rough (r) morphotype from each of the four patients (P2, 507
P17, P31, P37); M = molecular marker; ATCC = M. abscessus ATCC 19977 type strain 508
509 510
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
20
511
512
513 Table 1: 514
515
first isolates from patients (n=34) with M. abscessus in No. (%)
subsp. abscessus subsp. bolletii total
rough 15 (88.2) 2 (11.8) 17 (100)
smooth 2 (15.4) 11 (84.6) 13 (100)
mixed 2 (50) 2 (50) 4 (100)
516
Table 1: Colony morphology of M. abscessus subspecies abscessus and M. abscessus 517
subspecies bolletii from 34 patients. Strains were cultured on 7H11 agar to evaluate culture 518
morphology; differentiation of subspecies was done by Light-Cycler based analysis of the 519
hsp65 gene. 520
521
522
523
524
525
526
527
528
529
530
531
532
533
534 535
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
21
536
537
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
22
Table 2: 538
539
M. abscessus (n=50) in No. (%)
erm(41)
colony morphology wild type 276 bp
deletion
28 (TsC) Total
rough 20 (69) 4 (13.7) 5 (17.3) 29 (100)
smooth 4 (19) 15 (71.4) 2 (9.6) 21 (100)
rrl
wild type 2058 /2059
(aasac/ag/ca/ta/ga)
Total
rough 24 (82.7) 5 (17.3) 29 (100)
smooth 17 (81) 4 (19) 21 (100)
540
Table 2: Sequence analysis of the erm(41) and rrl genes of 29 rough and 21 smooth 541
isolates. 542
543
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
23
Table 3 544
545
M. abscessus (n=50) in No. (%)
erm(41)
wild type 276 bp
deletion
28 (TsC) Total
abscessus 21 (75) - 7 (25) 28 (100)
bolletii 3 (13.6) 19 (86.4) - 22 (100)
rrl
wild type 2058 /2059
(aasac/ag/ca/ta/ga)
Total
abscessus 23 (82.1) 5 (17.9) 28 (100)
bolletii 18 (77.8) 4 (22.2) 22 (100)
546 547
Table 3: Sequence analysis of the erm(41), and rrl genes of M. abscessus subspecies 548
abscessus and M. abscessus subspecies bolletii. 549
550
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
24
Table 4 551
552
MIC (µg / mL) of first and last isolates
P2 (mixed) P3 (smooth) P4 (smooth) P6 (smooth) P14 (rough) first* second first second first second first second first second
clarithromycin 0.25 > 16 0.06 > 16 0.25 0.25 > 16 > 16 0.5 >16 amikacin 8 > 64 8 > 64 4 > 64 > 64 > 64 16 32
553 Table 4: MICs on day 5 of first and second isolates from 5 patients (P2, P3, P4, P6, P14) 554
using the microdilution method. The first specimen of patient 2 (P2) showed both 555
morphotypes, the second specimen of patient 2 showed only rough morphotypes. From the 556
first specimen MICs of the rough morphotype for clarithromycin and and amikacin are shown. 557
The MICs for the smooth morphotype were 0.5 µg / mL for calrithromycin and 16 µg / mL for 558
amikacin, respectively. 559
560
561
562
563
564
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
P2 P17
P31 P37
M M P2 M P17 M P31 M P37 M M
ATCC s r s r s r s r ATCC
on May 12, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
































![FALL SEMESTER SPRING SEMESTER · 2019-07-05 · 3 JCM 211: Jazz Composition [6] 3 JCM 212: Jazz Composition [6] 1 JCM 200: Large Jazz Ensemble [4] 2 JCM 225: Jazz Comp. & Arranging](https://static.documents.pub/doc/80x56/5e5bc8a6b05fc406b243fd16/fall-semester-spring-semester-2019-07-05-3-jcm-211-jazz-composition-6-3-jcm.jpg)