55
Joint Commission Blood Management Performance Measures Mark T. Lucas, MPS, CCP Joint Commission Technical Advisory Panel Blood Management Performance Measures Project
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | moriah-huling |
| View: | 215 times |
| Download: | 1 times |
Joint Commission Blood Management Performance
Measures
Mark T. Lucas, MPS, CCPJoint Commission Technical Advisory
Panel Blood Management Performance
Measures Project

The Joint Commission• "To continuously improve health care for the public, in
collaboration with other stakeholders, by evaluating health care organizations and inspiring them to excel in providing safe and effective care of the highest quality and value“
• The Joint Commission accredits over 19,000 health care organizations and programs in the United States.
• 400+ programs internationally.
• Centers for Medicare Services recognize Joint Commission accreditation as a condition of licensure and the receipt of Medicaid and Medicare reimbursement.
History of The Joint Commission
• 1951 – ACP, AHA, AMA, CMA join with ACS to create the Joint Commission, an independent, not-for-profit organization whose primary purpose is to provide voluntary accreditation of hospitals on minimum standards for patient safety and efficacy of treatment.
• 1953 - JC published Standards for Hospital Accreditation
• 1965 – Congress passes the Social Security Amendments, stating that hospitals who meet JC standards can participate in Medicare and Medicaid programs.
History of The Joint Commission
• 1995 – Federal Government recognizes Joint Commission laboratory accreditation services as meeting CLIA 1988 requirements.
• 1997 – JC introduces ORYX to integrate outcomes and performance measures into accreditation.
• 2003 National Patient Safety Goals are instituted.
• 2005 – JC goes global. WHO recognition.
History of The Joint Commission
• 2007 – JC launches VAD Certification Program for destination therapy
• 2007 JC says “Hospitals go smoke free”
• 2007 Blood Management becomes important as a means of reducing unnecessary transfusions and costs
JC is coming!!!!!
The Joint Commission
Standardized performance measures NQF endorsed Inpatient hospital care Required for accreditation since 2002 Shared with Centers for Medicare & Medicaid
Services (mostly) Currently 10 sets More in development
Performance Measures
Indicators, statistics, or metrics that are used to gauge the performance of an activity, process, or operating entity.
Performance measures are also the reference markers used to measure whether a goal is being achieved
• Patient decision-making based on data and scientific evidence.
• The results demonstrate improvements in health care quality and patient safety.
12
Joint Commission Standards• Standards address the organization’s
level of performance in key functional areas
• Standards set forth performance expectations for activities that affect the safety and quality of patient care
• The Joint Commission develops its standards in consultation with health care experts, providers, measurement experts, purchasers, and consumers
13
Transfusions in the United States
1. 80,000 transfusion decisions occur each day
2. U.S. txfs 44% more blood than Europe and Canada
3. Variability in txfsn practice, inadequate training in txfsn medicine, no standards for tx.
4. Rising costs of healthcare, blood products
5. New evidence for safety of blood txfsn
6. Importance and utility of blood management to reduce cost and promote effective use of resources

Joint CommissionAll the variability in transfusion practices
shows "there is both excessive and inappropriate use of blood transfusions in the U.S.," advisers to Health and Human Services Secretary Kathleen Sebelius concluded earlier this month. "Improvements in rational use of blood have lagged."
Stakeholder Panel Meeting -
February 5, 2007
• Stakeholders Meeting at Joint Commission in Chicago
• Feasibility and utility of developing a set of blood management performance measures
• Unrestricted educational grant from Bayer Healthcare Pharmaceuticals
Objectives: 1. Investigate the current state of blood management
practices 2. Review evidence-based studies, clinical guidelines and
performance measures for use in improving blood management practices
3. Establish the need and desire for standardized performance measures focused on blood management

Stakeholder Organizations
• National Partnership for Women and Families• Society of Thoracic Surgeons• Cleveland Clinic• Department of Health and Human Services• American Academy of Orthopaedic Surgeons• American Association of Blood Banks• Food and Drug Administration• American College of Surgeons• American Society of Hematology• American Society of Anesthesiology• National Heart, Lung and Blood Institute• American Nurses Association• Society for Critical Care Medicine• American Red Cross• Society for the Advancement of Blood Management• Office of Blood Research and Review
17
Technical Advisory Panel
•David J. Ballard, MD, MSPH, PhD, FACP, Co-chair•Neil Bangs, MS, MT (ASCP) SBB•Richard J. Benjamin, MD, PhD, FRCPath, MS•Laurence Bilfield, MD•Victor A. Ferraris, MD, PhD•John Freedman, MD, FPCPC•Jonathan C. Goldsmith, MD •Lawrence Tim Goodnough, MD•Penny S. Gozia, MD, MBA•Jerry Holmberg, PhD, MT (ASCP), SBB
•Jonathan H. Waters, MD, Co-chair•Harvey Klein, MD•Mark T. Lucas, MPS, RCS, CCP•Vijay K. Maker, MD, FACCS •John (Jeffrey) McCullough, MD•Aryeh Shander, MD, FCCM, FCCP•Bruce D. Spiess, MD, FAHA•Lynne, Uhl, MD•Jeffrey Wagner, BSN, RN•Rosalyn Yomatovian, MD
The Gathering

Panel Discussion
PBM Development
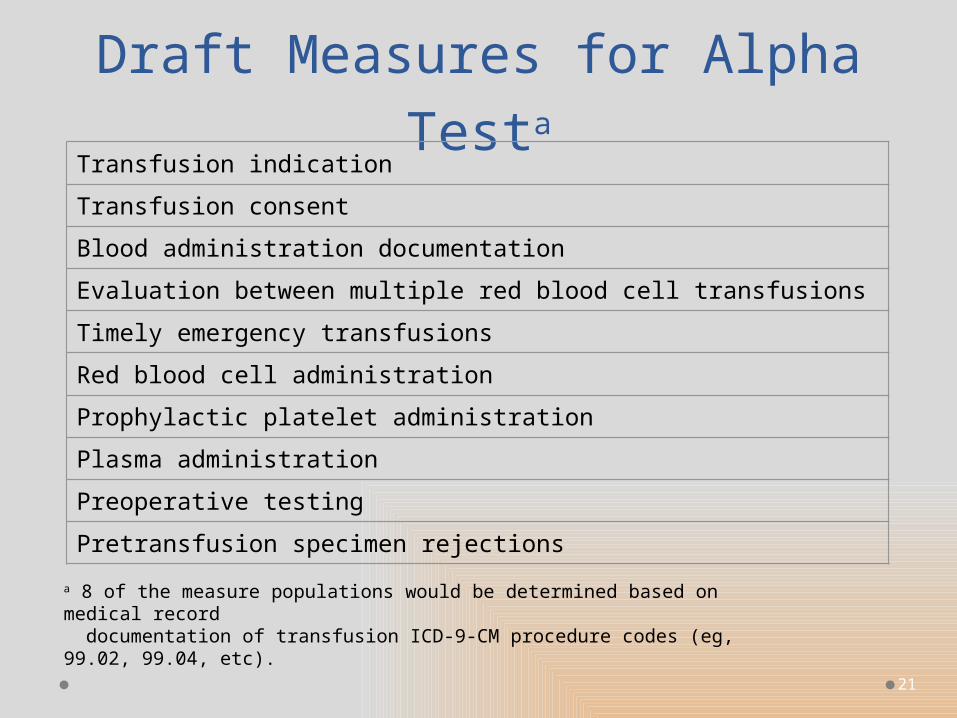
Over 68 candidate measures considered by technical advisory panel (TAP)
19 measures selected for public comment10 measures underwent alpha testing7 measures selected for pilot testing
21
Draft Measures for Alpha Testa
Transfusion indication
Transfusion consent
Blood administration documentation
Evaluation between multiple red blood cell transfusions
Timely emergency transfusions
Red blood cell administration
Prophylactic platelet administration
Plasma administration
Preoperative testing
Pretransfusion specimen rejections
a 8 of the measure populations would be determined based on medical record documentation of transfusion ICD-9-CM procedure codes (eg, 99.02, 99.04, etc).
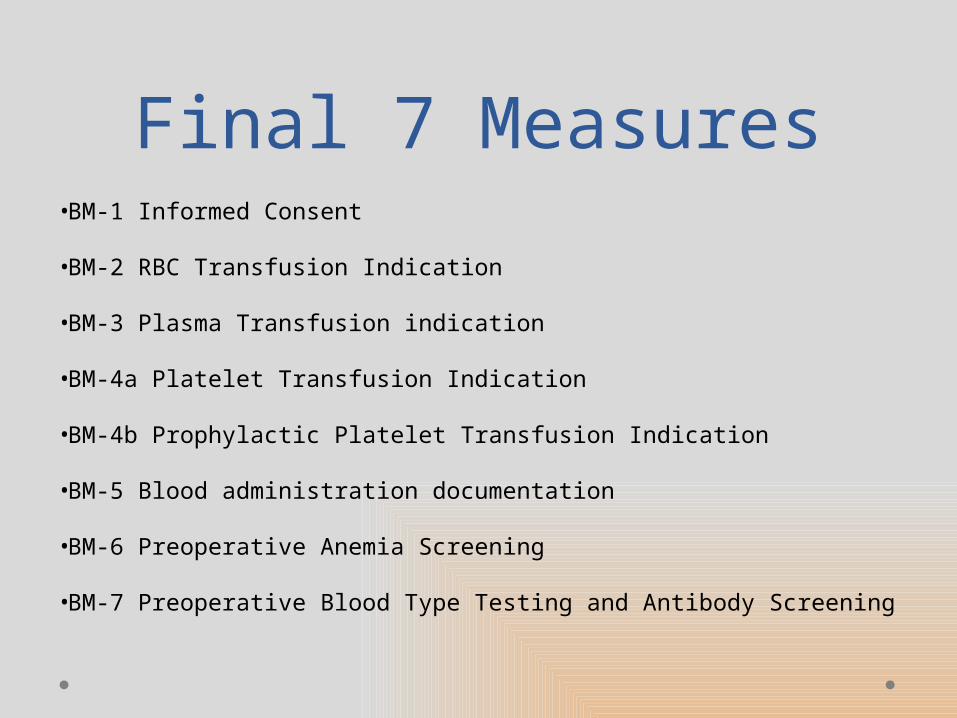
Final 7 Measures•BM-1 Informed Consent
•BM-2 RBC Transfusion Indication
•BM-3 Plasma Transfusion indication
•BM-4a Platelet Transfusion Indication
•BM-4b Prophylactic Platelet Transfusion Indication
•BM-5 Blood administration documentation
•BM-6 Preoperative Anemia Screening
•BM-7 Preoperative Blood Type Testing and Antibody Screening

Transfusion Consent
• Numerator: Patients with a signed consent who received information about the risks, benefits and alternatives prior to the initial blood transfusion or the initial transfusion was deemed a medical emergency
• Denominator: Patients of all ages who received red blood cell, plasma or platelet transfusions
23
Transfusion Consent Rationale
• The rate of transfusion consent in the US is unknown• Studies in other countries showed there is poor
documentation and room for improvement • Involving patients in healthcare decisions is a
national priority
24
Transfusion Consent Data Elements
• Transfusion Consent
• Information Addressed Risks, Benefits and Alternatives to transfusion
25
26
Transfusion Alternatives
• Preoperative Periodo Erythropoietino Androgenso Iron, folate, B12
supplements• Avoidance of anticoagulant drugs
o NSAIDSo Herbal supplementso Antiplatelet drugso Heparin/warfarin
• Intraoperative Periodo Normovolemic hemodilutiono Cell salvage
• Adjuncts o Point of care testingo Microsampling
• Drug therapyo desmopressino ε-aminocaproic acido recombinant factor VIIa
• Deliberate hypotension• Maintenance of normothermia• Avoidance of normal saline• Appropriate positioning
• Postoperative Periodo Washed or unwashed cell
salvageo Erythropoietin/Irono Hyperbaric oxygen therapyo Minimize phlebotomy
27
RBC Transfusion Indication
N:Number of RBC transfusion units with pre-transfusion hemoglobin or hematocrit and clinical indication documented
D:Number of red blood cell transfusion units evaluated
RBC Indication Rationale
• The rate of RBC transfusions in US hospitals is unknown
• Promotes a standardized process of:o checking a lab result prior to each transfusiono documentation of a reason why blood was
transfused• Information about total blood use could be used to
determine benchmarks by diagnoses or procedure
28
RBC Data Elements
• Clinical Indication for RBCs• Pre-transfusion Hemoglobin/hematocrit Result• RBC ID
• Trauma patients excluded• RBC unit exclusions
29
30
Plasma Transfusion Indication
N:Number of plasma transfusion units with pre-transfusion laboratory value AND clinical indication documented
D:Number of plasma units evaluated
Trauma patients excluded
Plasma Rationale
• The rate of plasma transfused in the US hospitals is unknown
• Promotes a standardized process of:o checking a lab result prior to transfusiono documentation of a reason why blood was
transfused• STS recommends transfusion based on
bleeding and preferably guided by POC tests (Grade C, Class IIa)
31
Plasma Data Elements
• Clinical Indication for Plasma
• Pre-transfusion Laboratory Testing
• Plasma ID
32
33
Platelet Transfusion Indication
N:Number of platelet transfusion units with pre-transfusion platelet testing AND clinical indication documented
D:Number of platelet units evaluated
Trauma patients excluded
Platelet Rationale
• The rate of platelets transfused in the US hospitals is unknown
• Transfusion of platelets associated with adverse events
• Promotes a standardized process of:o checking a lab result prior to transfusiono documentation of a reason why platelets
were transfused
34
Platelet Data Elements
• Platelet Clinical Indication
• Pre-transfusion Platelet Testing
• Platelet ID
35
36
Blood Administration Documentation
N:Number of transfusion units (bags) or doses with documentation for all of the following: o patient identification and transfusion order (or Blood
ID) confirmed prior to the initiation of transfusiono date and time of transfusion o blood pressure, (pulse) and temperature recorded
pre, during and post transfusion
D:Number of red blood cells, plasma and platelet units or doses evaluated
Blood Administration Rationale
• Majority of blood is transfused in hospitals• Numerous errors are associated with
incorrect Patient ID• The transfusion process is very complex and
has been identified as a high-risk area for error
• Standardizing the process will enable reliable tracking of potential adverse events nationally
37
Administration Data Elements
• Patient ID Verification • Transfusion Order• Transfusion Start Date• Transfusion Start Time• Vital Sign Monitoring• Blood ID Number
Note: Patients with trauma codes or RBC unit exclusions are not in this measure
38
39
Preoperative Anemia Screening
N:Patients with preoperative anemia screening 14 - 45 days before Anesthesia Start Date
D:Selected elective surgical patients
Cardiac patients removed

Anemia Screening Rationale
• Preoperative anemia is associated with increased morbidity and mortality
• A national audit found that 35% of patients scheduled for joint replacement therapy had a hgb <13 at preadmission testing
• Formal protocols for early detection, evaluation and management of high-blood loss surgeries has been identified as an unmet need
40
Anemia Screening Data Elements
• Preoperative Anemia Screening Result Date
• Reasons for No Preoperative Anemia Screening
• Point of Origin for Admission or Visit
41

42
Preoperative Blood Type Screening
N:Patients with preoperative type and screen or type and crossmatch completed prior to Surgery Start Time Anesthesia Start Time
D:Selected elective surgical patients
Blood Type Testing Rationale
• This measure is supported by the Joint Commission National Patient Safety Goal
• Patient safety is a national priority
• This issue affects the majority of hospitals and other high-blood use procedures
43
Blood Type Testing Data Elements
• Preoperative Blood Type Testing
• Blood Type Testing Ordered
44
Lessons learned…• Measuring blood transfusions and associated
processes would enable hospitals to identify areas for improvement
• Optimizing a patient’s hemoglobin level before surgery may result in less blood use during and after surgery
• Checking to make sure blood is available before surgery (if ordered) is in the patient’s and hospital’s best interest
45
Lessons learned…• These are general measures that collect data on
all patients that can be further analyzed by diagnoses and/or procedure code, age group or appropriateness as studies become available
• There is a lack of literature regarding “gaps in care” that these measures address
• The lack of national guidelines for blood – impacts the ability to standardize clinical indications
46
Lessons learned…• The abstraction burden for these measures using
paper-based records is
• Complete data on all transfusions could be collected by eMeasures with minimal effort and provide comprehensive data on product usage and benchmarking
• Some of the measures are similar to the measures collected in Australia
47
Final Lessons Learned…
• Use of these measures could be used in conjunction with the hemovigilance measures on transfusion related events
• If the rate of blood transfusions in hospitals is unknown, how will outcomes be monitored?
48

Next Steps
• Measures have been placed in The Joint Commission’s Library of Other Measures for use by anyone interested
• Encourage use of the PBM measures at the local level
• Funding pending for retooling the specifications for retrieval from the electronic medical record
49

PBM Data Collection
PBM Data Collection
National Quality Foundation
• NQF established a set of national voluntary consensus standards for measuring the quality of hospital care. These measures will permit consumers, providers, purchasers, and quality improvement professionals to evaluate and compare the quality of care in general acute care hospitals across the nation using a standard set of measures. The majority of the Joint Commission’s measures are endorsed by NQF and are denoted on the measure information forms.
• Final 7 measures were recommended by the TAP in November 2010 and submitted to the National Quality Forum (NQF) for consideration of endorsement in December 2010
• Not endorsed for use at the national level.
• Final measure specifications were posted in the Joint Commission Library of Other Measures in 2011. Measures that reside in the library are not collected, but are fully specified and available at the local level.
Implementation Guide for The Joint
Commission Patient Blood Management
Performance Measures
• 180 page document• How to use and implement the measures• Measure interpretation, rationale,
responsible parties• ICD-9 relationship to measures• Data collection, documentation• Patient base• Algorithms for implementation• References, definitions, ICD-9 codes
What Does This All Mean for
Perfusion
• Participating Hospitals will collect data on transfusion for appropriateness and cost effectiveness to compare with national standards
• New informed consent will mandate the explanation of transfusion alternatives, bringing about physician and patient knowledge and awareness of blood management
• Documentation and lab testing will be required, may increase costs
• Adoption of blood management will decrease costs and preserve resources
• Other agencies, CMS (?), may get on board

Duh!!! Blood Management

















