64
Joint Commission on Accreditation of Healthcare Organizations 1 Medical Errors, Sentinel Events, and Accreditation Association of Anesthesia Program Directors October 28, 2000
| Date post: | 11-Jan-2016 |
| Category: |
Documents |
| Upload: | rudolph-simmons |
| View: | 217 times |
| Download: | 0 times |

Joint Commissionon Accreditation of Healthcare Organizations
1
Medical Errors,Sentinel Events, and
Accreditation
Association of Anesthesia Program Directors
October 28, 2000

Joint Commissionon Accreditation of Healthcare Organizations
2
“Mistakes are at the very base of human thought, embedded there, feeding the structure like root nodules. If we were not provided with the knack of being wrong, we could never get anything useful done.”
“We are built to make mistakes, coded for error … The capacity to leap across mountains of information and land lightly on the wrong side represents the highest of human endowments.”
Lewis Thomas, 1974

Joint Commissionon Accreditation of Healthcare Organizations
3
Accreditation is,at its core,
a risk reduction activity.

Joint Commissionon Accreditation of Healthcare Organizations
4
The Joint Commission’sSentinel Event Policy
Established in January 1996 with the following goals:
To have a positive impact in improving care
To focus attention on underlying causes and risk reduction
To increase the general knowledge about sentinel events, their causes and prevention
To maintain public confidence in the accreditation process

Joint Commissionon Accreditation of Healthcare Organizations
5
Sentinel Event
A sentinel event is an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof.
Serious injury specifically includes the loss of limb or function.
The phrase, "or the risk thereof" includes any process variation for which a recurrence would carry a significant chance of a serious adverse outcome.
Joint Commissionon Accreditation of Healthcare Organizations
6
To Err Is Human:Building a Safer Health System
44,000 – 98,000 patient deaths annually due to error
Goal: 50% reduction in errors over the next 5 years
Recommendations: National Center for Patient Safety within DHHS Mandatory reporting to state agencies Engage consumers, purchasers, accreditors,
regulators Effect a culture shift to make safety a top priority
Institute of Medicine Report, November 1999

Joint Commissionon Accreditation of Healthcare Organizations
7
Joint Commission Public Policy Position on Reporting & Managing Medical Errors
In order to measurably improve patient safety, the Joint Commission supports
Creation of an effective national reporting system
(mandatory or voluntary)
Conditioned on the following:1. Limited to well-defined “serious adverse events,” if mandatory
2. Standardized definition of a reportable medical error or event
3. Requirement for in-depth analysis of each error/event
4. Federal protection from disclosure of the resulting information
5. Requirement for action plan with follow-up
6. Sharing of event-related information with oversight bodies

Joint Commissionon Accreditation of Healthcare Organizations
8
Experience to Date
188 inpatient suicides126 events relating to medication errors119 operative/post op complications 88 events of surgery at the wrong site 51 deaths related to delay in treatment 49 patient falls (13 multi-story) 42 assault/rape/homicide 41 deaths of patients in restraints 32 deaths following elopement 22 transfusion-related events 22 Perinatal death/injury 18 infant abductions/wrong discharges 18 fires167 “other”
Of 983 sentinel events reviewed by the Accreditation Committee:

Joint Commissionon Accreditation of Healthcare Organizations
9
Total “Reviewed” Events by State
International3
PR: 13
3
56
29 8
68
2
5
6
9
2
6
4
31
7
5
14
31
9
10
13
9
8
14
55
32
11 30
9
20
8 17 22
62
16
24
258
34
62
7
15543
105
59
6
8
2
9

Joint Commissionon Accreditation of Healthcare Organizations
10
Sources of Sentinel Event Information

Joint Commissionon Accreditation of Healthcare Organizations
11
Settings of the Sentinel Events
0 200 400 600 800 1000 1200
Health care network
Clinical laboratory
Ambulatory care setting
Home care service
Emergency department
Long term care facility
Out-pt behavioral health
Psychiatric unit
Psychiatric hospital
General hospital
Total events

Joint Commissionon Accreditation of Healthcare Organizations
12
Root cause analysis …
. . . a process for identifying the basic or causal factors that underlie variation in performance, including the occurrence or possible occurrence of a sentinel event.

Joint Commissionon Accreditation of Healthcare Organizations
13
Classification of Root Causes
General classification based on Joint Commission standards
Patient care functions
Organization management functions
Joint Commissionon Accreditation of Healthcare Organizations
14
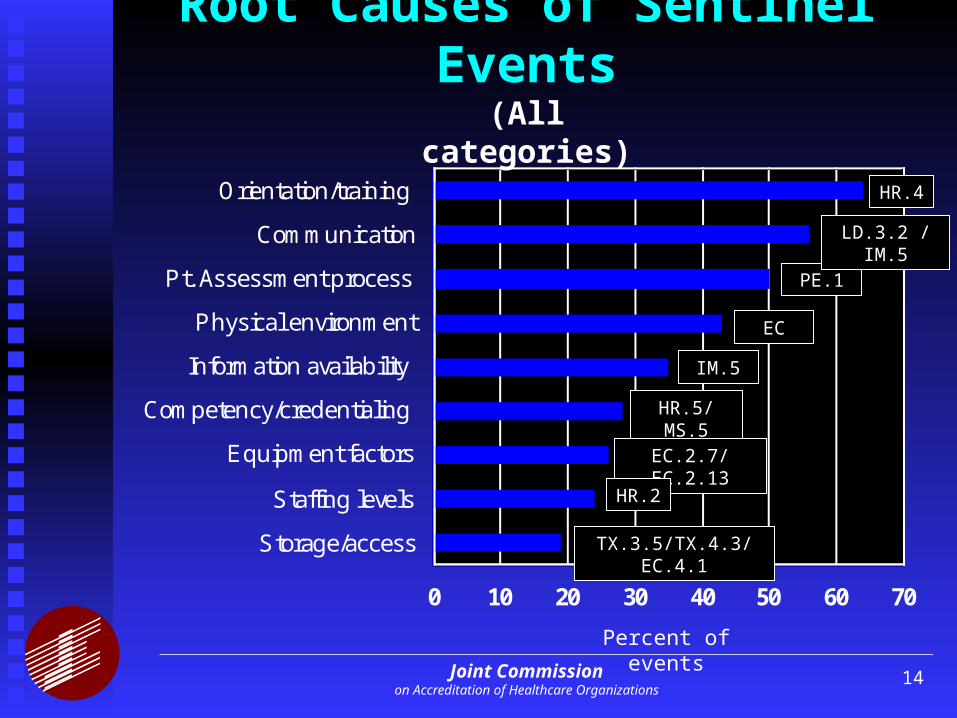
Root Causes of Sentinel Events
0 10 20 30 40 50 60 70
Storage/access
Staffing levels
Equipment factors
Competency/credentialing
Information availability
Physical environment
Pt. Assessment process
Communication
Orientation/training
(All categories)
Percent of events
HR.4
PE.1
EC
IM.5
HR.5/MS.5
EC.2.7/EC.2.13
HR.2
TX.3.5/TX.4.3/EC.4.1
LD.3.2 / IM.5

Joint Commissionon Accreditation of Healthcare Organizations
15
Root Causes of Medication Errors
0 10 20 30 40 50 60 70
Distraction
Labeling
Supervision
Competency/credentialing
Information availability
Storage/access
Communication
Orientation/training HR.4
TX.3.3/3.5
IM.5
HR.5/MS.5
MS.2.5
TX.3.5
EC.4.1
LD.3.2 / IM.5
Percent of events

Joint Commissionon Accreditation of Healthcare Organizations
16
Root Causes of Wrong Site Surgery
0 10 20 30 40 50 60 70 80
Competency / credentialing
Distraction
Info not available in OR
No verification process
No communication with pt
OR hierarchy
Verification Policy not followed
Incomplete pt assessment
OR team miscommunication IM.5
PE.1.8
TX.5.2/PF.1.10
IM.5
EC.4.1
HR.5 / MS.5
?
?
?
Percent of events

Joint Commissionon Accreditation of Healthcare Organizations
17
Strategies for Reducing the Riskof Wrong Site Surgery
0 10 20 30 40 50 60 70 80
Mark operative site
Require verbal team verification in OR
Develop verification checklist
Require surgeon to get informed consent
Require pre-op site verification by patient
Software enhancements
Revise competency assessment process
Monitor high-risk policy compliance
Revise equipment set-up procedures Percent of events

Joint Commissionon Accreditation of Healthcare Organizations
18
Suggestions from the Joint Commission to Reduce the Risk of Wrong-Site Surgery:
1. Involve patient and surgeon in pre-op identification and marking of operative site
2. Implement verbal verification process in O.R.
Other strategies that may be helpful: Personal involvement of the surgeon in
obtaining informed consent Ongoing monitoring of compliance with high-
risk procedures (e.g., site verification procedure)
Software enhancements to ensure consistent site identification and information availability

Joint Commissionon Accreditation of Healthcare Organizations
19
New PublicationWe are pleased to introduce the first issue of Sentinel Event Alert, a periodic publication dedicated to providing important information relating to the occurrence and management of sentinel events in Joint Commission-accredited health care organizations. Sentinel Event Alert, to be published when appropriate as suggested by trend data, will provide ongoing communication regarding the Joint Commission's Sentinel Event Policy and Procedures, and most importantly, information about sentinel event prevention. It is our expectation and belief that in sharing information about the occurrence of sentinel events, we can ultimately reduce the frequency of medical errors and other adverse events.
Medication Error Prevention -- Potassium ChlorideIn the two years since the Joint Commission enacted its Sentinel Event Policy, the Accreditation Committee of the Board of Commissioners has reviewed more than 200 sentinel events. The most common category of sentinel events was medication errors, and of those, the most frequently implicated drug was potassium chloride (KCl). The Joint Commission has reviewed 10 incidents of patient death resulting from misadministration of
SENTINEL EVENT ALERTA publication of the Joint Commission onAccreditation of Healthcare Organizations
Jo in t C om m issionon A ccred ita tion o f H ea lthcare O rgan iza tions
One Renaissance BoulevardOakbrook Terrace, IL 60181Phone: (630) 792-5800
Issue One2-27-98
"The w ay to p reven t trag ic dea ths from acc iden ta l in travenous in jection o f concen tra ted K C l is excruc ia ting ly s im p le - -o rgan iza tions m ust take it o ff the floo r s tock o f a ll un its . It is one o f the best exam ples I know o f a 'fo rc ing function ' -- a p rocedure tha t m akes a certa in type o f e rro r im possib le ." Luc ian L . Leape, M .D .

Joint Commissionon Accreditation of Healthcare Organizations
20
Sentinel Event Trends:All Reviewed Events
0
100
200
300
400
500
1995 1996 1997 1998 1999 2000

Joint Commissionon Accreditation of Healthcare Organizations
21
Sentinel Event Trends:Potassium Chloride Events
0
2
4
6
8
10
1995 1996 1997 1998 1999 2000
S. E. Alert # 1
February 1998

Joint Commissionon Accreditation of Healthcare Organizations
22
Sentinel Event Trends:Suicide Events (Percent of Total)
0
5
10
15
20
25
30
1995 1996 1997 1998 1999 2000
S. E. Alert # 7
November 1998

Joint Commissionon Accreditation of Healthcare Organizations
23
Sentinel Event Trends:Restraint Deaths (Percent of Total)
0
2
4
6
8
10
1995 1996 1997 1998 1999 2000
S. E. Alert # 8
November 1998

Joint Commissionon Accreditation of Healthcare Organizations
24
Sentinel Event Trends:Wrong-site Surgery (Percent of Total)
0
2
4
6
8
10
12
14
16
1995 1996 1997 1998 1999 2000
S. E. Alert # 6
August 1998

Joint Commissionon Accreditation of Healthcare Organizations
25
Proactive Risk Reduction
RCA is reactive; subject to “hindsight bias”
The sentinel event can have a “blinder” effectThe best RCAs look at all the risk points
Why wait for the sentinel event? Identify the high risk processes Conduct proactive risk assessment Redesign for safety

Joint Commissionon Accreditation of Healthcare Organizations
26
IOM Recommendation forEstablishment of Safety Programs
Health care organizations should establish patient safety programs with defined executive responsibility that
are clearly focused on patient safety, implement non-punitive systems for reporting and
analyzing medical errors, incorporate well-understood safety principles, and establish interdisciplinary team training for
providers of patient care which incorporates proven methods of team training.

Joint Commissionon Accreditation of Healthcare Organizations
27
Government’s Responseto the IOM Report
The President’s response
The QuIC Report
HCFA’s response New Condition of Participation establishing
requirement for Patient Safety Programs in hospitals
Joint Commissionon Accreditation of Healthcare Organizations
28
Standards Relatingto Sentinel Events
LD.4.3.4 Role of Leadership
PI.2 Design of new processes
PI.3.1.1 Data collection
PI.4.3 Root cause analysis
PI.4.4 Action plan

Joint Commissionon Accreditation of Healthcare Organizations
29
Proposed Revisions to Joint Commission Standards in Support of Error Reduction Programs in Health Care Organizations
Leadership
Performance Improvement
Information Management
Other functions

Joint Commissionon Accreditation of Healthcare Organizations
30
Proposed Standards Revisionsfor Error Reduction Programs
Leadership standards to emphasize safety
In response to actual occurrences
As a component of new design and redesign activities
As an ongoing proactive effort.
Joint Commissionon Accreditation of Healthcare Organizations
31
Proposed Standards Revisionsfor Error Reduction Programs
Performance Improvement standards to require
Proactive risk assessment and risk reduction
. . . Based on available risk-related information
Focused on high-risk activities selected by the organization.

Joint Commissionon Accreditation of Healthcare Organizations
32
Proposed Standards Revisionsfor Error Reduction Programs
Information Management standards to strengthen
Aggregation of safety-related information
Use of knowledge-based information on safety-related issues
Effective communication among participants in health care processes

Joint Commissionon Accreditation of Healthcare Organizations
33
Proposed Standards Revisionsfor Error Reduction Programs
Other standards-based functions, including
Patient Rights
Patient and Family Education
Continuum of Care
Environment of Care
Human Resource Management

Joint Commissionon Accreditation of Healthcare Organizations
34
Joint Commission Standards
Are designed to . . .
Focus on safety and quality of patient care
Represent consensus on state-of-the-art in expected organization performance
Whenever possible, be evidence-based
State objectives or principles, rather than specific mechanisms for meeting requirements
Be reasonable and achievable
Be surveyable

Joint Commissionon Accreditation of Healthcare Organizations
35
Standards Development Process
Ongoing field analysis and literature review Preliminary review by Professional & Technical
Advisory Committees (PTACs) Internal & external workgroups Qualified experts in the relevant fields Field evaluation of draft standards Further revision based on field evaluation Review by PTACs Approval by SSP Committee of the Board Ongoing field assessment (compliance monitoring)
Joint Commissionon Accreditation of Healthcare Organizations
36
Standards Relevant to Anesthesia Services
Patient rights Patient assessment Anesthesia care Medication use Leadership Performance improvement Human resources management Information management Medical staff

Joint Commissionon Accreditation of Healthcare Organizations
37
Sedation and Anesthesia Defined
1. Minimal sedation Cognitive function & coordination affected Respond normally to verbal commands CP function unaffected
2. Moderate sedation / analgesia (“conscious sedation”) Drug-induced depression of consciousness Purposeful response to verbal stimuli Adequate spontaneous ventilation Cardiovascular function maintained

Joint Commissionon Accreditation of Healthcare Organizations
38
Sedation and Anesthesia Defined
3. Deep sedation / analgesia Drug-induced depression of consciousness Cannot be easily aroused Purposeful response to painful stimuli Airway / ventilation may be impaired Cardiovascular function ususally maintained
4. Anesthesia General anesthesia Spinal anesthesia Major regional anesthesia

Joint Commissionon Accreditation of Healthcare Organizations
39
Standards Relevant to Anesthesia Services
Patient rights Patient assessment Anesthesia care Medication use Leadership Performance improvement Human resources management Information management Medical staff
Revised to apply to Moderate and Deep Sedation and Anesthesia
Effective January 2001

Joint Commissionon Accreditation of Healthcare Organizations
40
Patient Rights Informed consent
Clear explanation of proposed treatments Potential benefits and drawbacks Likelihood of success Alternatives, including non-treatment Possible results of alternatives or non-treatment Possible need for and risks of transfusion Identity/professional status of practitioners
These are process requirements, not documentation requirements

Joint Commissionon Accreditation of Healthcare Organizations
41
Patient Assessment
Pre-anesthesia assessment All moderate or deep sedation or anesthesia Assess risk & select form of sedation/anesthesia Determine patient is an appropriate candidate Qualified L.I.P. conducts or confirms Re-evaluate immediately pre-induction
Post-anesthesia assessment On admission to, during, & discharge from PACU Discharge by L.I.P. or approved criteria

Joint Commissionon Accreditation of Healthcare Organizations
42
Anesthesia Care
Sedation / anesthesia care is planned The need for blood / components is considered The plan is communicated among the care
providers
The patient’s physiologic status is monitored Heart & respiratory rate Oxygenation (continuous pulse oximetry) Adequacy of pulmonary ventilation BP at regular intervals ECG if known CV disease or dysrhythmias

Joint Commissionon Accreditation of Healthcare Organizations
43
Medication Use
Medications are appropriately controlled
Emergency medications are consistently available, controlled, and secure
Does not require anesthesia carts to be locked
Does not require constant attendance if
1. They are in a limited access area
2. No evidence of abuse, misuse, or diversion

Joint Commissionon Accreditation of Healthcare Organizations
44
Leadership
Uniform performance Consistency of process for sedation / anesthesia
procedures for comparable risk patients in different locations
Assessment Monitoring Recovery & discharge
Department directors’ responsibilities

Joint Commissionon Accreditation of Healthcare Organizations
45
Department Directors’ Responsibilities
All clinical activities within the department Integrate and coordinate Policies and procedures Recommend staffing levels Determine qualifications & competence of staff Surveillance of professional performance of L.I.P.s Involve department in performance improvement Maintain quality control programs Provide for orientation, continuing education Recommend space and other resources Participate in selecting outside vendors

Joint Commissionon Accreditation of Healthcare Organizations
46
Improving Organization Performance
Department vs. organization-wide requirements
Required measurement & analysis: Significant adverse events associated with
anesthesia use Outcomes of patients undergoing moderate and
deep sedation Outcomes related to resuscitation Patient perceptions of pain management Confirmed transfusion reactions Significant adverse drug reactions Significant medication errors All sentinel events
Joint Commissionon Accreditation of Healthcare Organizations
47
Information Management
Required documentation in the medical record: Informed consent, when req’d by the hospital Findings of patient assessments Clinical observations Response to care, including sedation / anesth. All medications administered Any adverse drug reactions Discharge from PACU
Compliance with discharge criteria Responsible L.I.P.

Joint Commissionon Accreditation of Healthcare Organizations
48
Human Resources Management
Sufficient numbers of qualified personnel (in addition to the L.I.P. performing the procedure) To evaluate the patient prior to sedation / anesth. To provide the sedation / anesthesia To perform the procedure To monitor the patient To recover and discharge the patient
Staffing plan Orientation & training Competency assessment

Joint Commissionon Accreditation of Healthcare Organizations
49
Medical Staff Credentialing
Qualified individuals provide sedation / anesthesia
Licensed independent practitioners (L.I.P.s)
Competent to
evaluate patients for sedation / anesthesia
administer drugs to predictably achieve desired level of sedation / anesthesia
monitor patients to maintain desired level
rescue patients who have slipped into next level of sedation / anesthesia
Joint Commissionon Accreditation of Healthcare Organizations
50
Survey Process Anesthetizing locations visits
Operating room Same-day surgery Endoscopy suites Interventional radiology / special procedures Dental clinics . . .
Scheduled visits Interact with direct care staff Evaluate compliance with relevant standards Observe patients in PACU Physical environment, equipment & utilities mgmt.

Joint Commissionon Accreditation of Healthcare Organizations
51
Survey Process
Patient Care Interview Builds on earlier survey activities Brings together representatives of staff concerned
with all aspects of patient care Assesses coordination of care Addresses unresolved issues
Medical Staff Leadership Interview Includes department directors Assesses MS role in hospital activities relating to
patient care and performance improvement

Joint Commissionon Accreditation of Healthcare Organizations
52
New Pain Assessment and Management Standards
Effective January 1, 2001

Joint Commissionon Accreditation of Healthcare Organizations
53
What Do They Address?
Right to have Pain assessed and managed Screening for and Assessment of Pain Care Education Continuum of Care Ongoing Organization Improvement

Joint Commissionon Accreditation of Healthcare Organizations
54
How Are They Surveyed?
Document Reviews Policy, Procedure, Practice Guidelines Minutes Open and Closed Patient Records
Observation and Interviews Staff Patients and Families

Joint Commissionon Accreditation of Healthcare Organizations
55
New Rights Standard
“All patients/individuals/residents/clients have a right to have their pain assessed and managed appropriately.”
Surveyors look for how you let recipients of care and services know . . .
Joint Commissionon Accreditation of Healthcare Organizations
56
New Assessment Standard
Standard and its Intent Surveyed
“All patients/individuals/residents/clients are assessed.”
All are Screened Those with Pain are Assessed and Re-
assessed

Joint Commissionon Accreditation of Healthcare Organizations
57
Fifth Vital Sign?
“Yes” - for patients with pain found at time of initial screening and/or for those who are likely to have pain (e.g., surgery, sickle cell crisis)
Joint Commission standards do not view pain assessments as fifth vital sign for all recipients of care or services

Joint Commissionon Accreditation of Healthcare Organizations
58
Addition to Care Standards
Introduction Added “Symptom Management” to
Introduction
Medication Use Added “Patient-controlled Analgesia” to
medication administration standard as well as “Epidural/Spinal and Other Interventions” (complementary/alternative)

Joint Commissionon Accreditation of Healthcare Organizations
59
Many Ways to Provide “Pain Care”
Ambulatory, Home, Hospital, and Long Term Care Formal Pain Programs, Departments or Services Pain management included in Care Paths, Care
Maps, Clinical Practice Guidelines (CPGs), formal Practice Parameters, Standards of Practice
Enforced Standardized Protocols or Policy Behavioral Health – Assessment Protocol or Policy,
Referral for individuals w/physical pain Other Innovative Ways Not Applicable for Health Care Networks, PPOs

Joint Commissionon Accreditation of Healthcare Organizations
60
New Education Standard
Patients/Individuals/Residents/Clients and their families are educated about pain and managing pain as part of treatment, when appropriate (PF.3.4)
Intent of PF.3.4 Understanding pain and the importance of
effective management Understanding cultural and belief system
barriers

Joint Commissionon Accreditation of Healthcare Organizations
61
New Continuum of Care Language
Addition to Intent of Discharge Planning standard (CC.6.1) Discharge planning focuses on meeting
patients’ health care needs after discharge. Discharge planning identifies patients’
continuing physical, emotional, symptom management (e.g., pain, nausea, or dyspnea), housekeeping, transportation, social, and other needs and arranges for services to meet them.

Joint Commissionon Accreditation of Healthcare Organizations
62
PI.3.1 Collect Data
To monitor the organization’s performance Leaders prioritize data collection based on mission
and scope of services provided Leaders consider for data collection . . . The
appropriateness and effectiveness of pain management
Leaders required to collect data about the needs, expectations, and satisfaction of individuals and organizations served

Joint Commissionon Accreditation of Healthcare Organizations
63
Scoring PI.3 Data Collection Surveyors will expect to see Evidence of data
collection on one or both topics
Outcomes of pain management (on consider list)
Results of Patient Perceptions related to management of pain (on mandatory list)

Joint Commissionon Accreditation of Healthcare Organizations
64
In Summary . . .
Patient’s Rights Issue Staff Competence Issue
Screening, Assessment, Reassessment Appropriate Guidelines for Management
Clinical Practice Guidelines Practice Parameters
Leadership Support, Policy/Procedure Quality Monitoring for Improved Processes and
Outcomes

















