652 antenatal centre and the demand (45% at present, but increasing) for institutional confinement. The hospital unit, he thinks, should have its own antenatal centre and associated clinics round about; antenatal work should be carried out by trained obstetricians who could be called on for help by the midwives in the district. Other speakers, he noted, favoured a practitioner service, but he thought that any legislation should allow some latitude to different areas. Mr. Eardley Holland had proposed a scheme for a county area : his own scheme is more suited to an industrial area. It has given rise to con- siderable opposition, however, which though quiescent at present will no doubt be resumed at the end of the war. Mr. ARNOLD L. WALKER said that the chief function of a maternity hospital is to look after the healthy mother and child ; we are losing sight of this, and maternity is beginning to be regarded as another disease. Too much stress, he thinks, is laid on the value of the ancillary services in general hospitals. At voluntary hospitals the obstetricians form a committee ; in municipal hospitals one person is in control and he may be the superintend- ent, the medical officer of health, a whole-time medical officer, or a practising obstetrician. Almost all institu- tions make use of the best obstetric skill available. In Willesden a house has been built close to the hospital in which the obstetrician is required to reside but -he is subjected to no other restrictions on practice. His job is to see that the patients in the hospital are properly treated. Mr. Walker said he has held this post since 1930 and the division of responsibility has been satis- factory. Until 1940 a house-surgeon of his choosing used to be appointed, and it was easy to keep in close contact with all that went on. Since December, 1940, there has been no house-surgeon and he has had to under- take more work, but with a staff of competent midwives and some selected general practitioners who can be called in, it has not been difficult to carry on. Living so close to the hospital he can see a patient several times in a day or night and there is no temptation to hurry things or to interfere unnecessarily. He mentioned that some of the LCC consultants have to come several miles to the hospitals to which they are attached, which may not be satisfactory. In staffing maternity institutions he thinks it wise to plan for unification of control but devoutly hopes we shall not see a whole-time service. The danger of putting a single person in charge is that he lacks the criticism of his colleagues. The service, in his view, should be based on a well-trained body of midwives supported by a limited body of obstetricians. -Dr. W. ALLEN DALEY remarked that the patients will say whether the service is to be institutional or domicili- ary, and they are showing a growing preference for hospital care. In 1930 there were 10,000 institutional confinements in London ; in 1938 there were 21,000. There will always be some domiciliary midwifery. Midwives should have adequate training and refresher courses, and doctors too should be properly trained. No doubt they are better trained today than they were in the past but in London it is difficult to give them ade- quate experience owing to the small numbers of beds in the teaching laospitals. The LCC, he said, have placed their obstetric units at the disposal of the medical schools. They take the view that the general practitioner should be not only willing to undertake midwifery but com- petent to do it. The service should function as a whole, the domiciliary and antenatal services being associated with the hospital service. He agreed that obstetricians should live close to the hospitals at which they are to work. Administration should cement the partnership between voluntary and municipal agencies. Political control in this service is, he finds, a great driving force : there is no difficulty in getting people to expend public money on maternity care. Dr. G. DICK READ said he spoke from the periphery, and he did not look on obstetrics as rabbit breeding, or mothers as people to be shuffled here and there by municipalities. He thought the service should be run by central midwifery depots supplying their own ancillary services according to need. The obstetrician and the midwife, he said, are essentially physician-minded. In a hospital run by gynaecologists he had found that 9% of maternity cases were subjected to csesarean section and 43% to some sort of surgical interference. It is time, he feels, that obstetricians and gynaecologists were separ- ated ; and that what we need after the war is a ministry of reproduction. Dr. GERALDINE WINN EVERETT also spoke from the periphery, voicing the opinions of the doctors in her area. She favoured a general practitioner service. The patient and her doctor have a personal relationship, and in confinement a woman wants her own doctor who is familiar with her physical and mental make-up. In’any case the number of doctors needed makes it impossible to exclude the general practitioner. A list of doctors willing to undertake midwifery should be made out, on the understanding that those giving in their names are also willing to take extra training. There should be a central consultant in the area, giving help to all who apply for it, and local consultants who have 10 years postgraduate experience of obstetrics and of general practice, and a higher degree in obstetrics. Much of the present antenatal work is done by those who never deliver a case. Private patients engage their doctor ; midwives’ cases should go to a clinic and give the name of the doctor to whom they would like the medical-aid form sent. The clinic should be under the local consultant, and all abnormal cases should be seen in consultation with the patient’s own doctor. She would like to see more and better-equipped local hospitals. There is danger in taking an ill woman a long distance to hospital. The CHAIRMAN remarked that not all doctors at the periphery were competent to do obstetric practice, as Sir Alexander Macgregor had shown. Institutional treat- ment is increasing, and is showing mortality approach- ing the irreducible minimum. Domiciliary midwifery, he considers, will disappear in large towns, and it is therefore a waste of time to train a large number of young people who are never going to practise obstetrics. There should be only one head in a maternity hospital: he mentioned the master of the Rotunda as an outstand- ing example. He pointed out that anyone could become an obstetric specialist with constant practice and patience. The scheme proposed by Dame Louise he fourid to be almost identical with that suggested by Blair Bell and himself in 1931. He considers that peripheral difficulties would be more easily settled if there was a central directing body-not an advisory committee- at the Ministry of Health. Nobody, it seems, pays any attention to an advisory body. JOINT MEETING WITH THE MEDICAL SOCIETY FOR THE STUDY OF. VENEREAL DISEASES AT a joint meeting of the section of Physical Medicine of the Royal Society of Medicine and the Medical Society for the Study of Venereal Diseases held at the Royal Victoria Hospital, Netley, on May 16, a discussion on Gonococcal Arthritis and Rheumatism and their treatment by mechanically induced pyrexia was opened by Major G. D. KERSLEY, president of the section, who described the clinical findings and results of treatment in 50 consecutive cases of metastatic gonorrhoea. He said that, in general, rheumatism associated with gonococcal infection has three striking characteristics ; the variety of the manifestations, the variable duration of the period between time of infection and onset of symptoms, and the reaction to hyperpyrexia. The problem is to establish the diagnostic criteria by which a case of rheum a- tism may be regarded as gonococcal. In his series there was a patient with a history of attacks of rheumatism for years in whom this flared up with the onset of a gono- coccal urethritis. Is such rheumatism truly gonococcal or does the toxin of gonorrhoea act in the same way as the toxin of a non-specific infection in causing a flare-up of the pre-existing condition in a sensitive individual ? There were also 4 cases in which the onset of rheumatism coincided with a recurrence of urethral discharge in which gonococci were not found, at times ranging from 2 months to 21 years after an original attack of gonorrhoea. Was this attributable to latent gonococcal infection or to residual non-specific infection in the prostate ? Apart from such doubtful cases the clinical syndrome is very varied. The brunt of the attack commonly falls on fasciae, tendons, sheaths and ligaments, particularly the plantar fascia and the sheath of the tendo Achillis. Synovitis is common, sometimes progressing to arthritis, especially of the larger joints. The effusion may be
Transcript
652
antenatal centre and the demand (45% at present, butincreasing) for institutional confinement. The hospitalunit, he thinks, should have its own antenatal centre andassociated clinics round about; antenatal work shouldbe carried out by trained obstetricians who could becalled on for help by the midwives in the district. Otherspeakers, he noted, favoured a practitioner service, buthe thought that any legislation should allow some latitudeto different areas. Mr. Eardley Holland had proposeda scheme for a county area : his own scheme is moresuited to an industrial area. It has given rise to con-siderable opposition, however, which though quiescentat present will no doubt be resumed at the end of the war.Mr. ARNOLD L. WALKER said that the chief function
of a maternity hospital is to look after the healthy motherand child ; we are losing sight of this, and maternity isbeginning to be regarded as another disease. Too muchstress, he thinks, is laid on the value of the ancillaryservices in general hospitals. At voluntary hospitals theobstetricians form a committee ; in municipal hospitalsone person is in control and he may be the superintend-ent, the medical officer of health, a whole-time medicalofficer, or a practising obstetrician. Almost all institu-tions make use of the best obstetric skill available. InWillesden a house has been built close to the hospitalin which the obstetrician is required to reside but -he issubjected to no other restrictions on practice. His jobis to see that the patients in the hospital are properlytreated. Mr. Walker said he has held this post since1930 and the division of responsibility has been satis-factory. Until 1940 a house-surgeon of his choosingused to be appointed, and it was easy to keep in closecontact with all that went on. Since December, 1940,there has been no house-surgeon and he has had to under-take more work, but with a staff of competent midwivesand some selected general practitioners who can becalled in, it has not been difficult to carry on. Living soclose to the hospital he can see a patient several times ina day or night and there is no temptation to hurrythings or to interfere unnecessarily. He mentioned thatsome of the LCC consultants have to come several milesto the hospitals to which they are attached, which maynot be satisfactory. In staffing maternity institutionshe thinks it wise to plan for unification of control butdevoutly hopes we shall not see a whole-time service.The danger of putting a single person in charge is thathe lacks the criticism of his colleagues. The service, inhis view, should be based on a well-trained body ofmidwives supported by a limited body of obstetricians.
-Dr. W. ALLEN DALEY remarked that the patients willsay whether the service is to be institutional or domicili-ary, and they are showing a growing preference forhospital care. In 1930 there were 10,000 institutionalconfinements in London ; in 1938 there were 21,000.There will always be some domiciliary midwifery.Midwives should have adequate training and refreshercourses, and doctors too should be properly trained. Nodoubt they are better trained today than they were inthe past but in London it is difficult to give them ade-quate experience owing to the small numbers of beds inthe teaching laospitals. The LCC, he said, have placedtheir obstetric units at the disposal of the medical schools.They take the view that the general practitioner shouldbe not only willing to undertake midwifery but com-petent to do it. The service should function as a whole,the domiciliary and antenatal services being associatedwith the hospital service. He agreed that obstetriciansshould live close to the hospitals at which they are towork. Administration should cement the partnershipbetween voluntary and municipal agencies. Politicalcontrol in this service is, he finds, a great driving force :there is no difficulty in getting people to expend publicmoney on maternity care.
Dr. G. DICK READ said he spoke from the periphery,and he did not look on obstetrics as rabbit breeding, ormothers as people to be shuffled here and there bymunicipalities. He thought the service should be run bycentral midwifery depots supplying their own ancillaryservices according to need. The obstetrician andthe midwife, he said, are essentially physician-minded.In a hospital run by gynaecologists he had found that 9%of maternity cases were subjected to csesarean sectionand 43% to some sort of surgical interference. It is time,he feels, that obstetricians and gynaecologists were separ-
ated ; and that what we need after the war is a ministryof reproduction.
Dr. GERALDINE WINN EVERETT also spoke from theperiphery, voicing the opinions of the doctors in her area.She favoured a general practitioner service. The patientand her doctor have a personal relationship, and inconfinement a woman wants her own doctor who isfamiliar with her physical and mental make-up. In’anycase the number of doctors needed makes it impossibleto exclude the general practitioner. A list of doctorswilling to undertake midwifery should be made out, onthe understanding that those giving in their names arealso willing to take extra training. There should be acentral consultant in the area, giving help to all whoapply for it, and local consultants who have 10 yearspostgraduate experience of obstetrics and of generalpractice, and a higher degree in obstetrics. Much of thepresent antenatal work is done by those who never delivera case. Private patients engage their doctor ; midwives’cases should go to a clinic and give the name of thedoctor to whom they would like the medical-aid formsent. The clinic should be under the local consultant,and all abnormal cases should be seen in consultationwith the patient’s own doctor. She would like to seemore and better-equipped local hospitals. There isdanger in taking an ill woman a long distance to hospital.The CHAIRMAN remarked that not all doctors at the
periphery were competent to do obstetric practice, asSir Alexander Macgregor had shown. Institutional treat-ment is increasing, and is showing mortality approach-ing the irreducible minimum. Domiciliary midwifery,he considers, will disappear in large towns, and it istherefore a waste of time to train a large number ofyoung people who are never going to practise obstetrics.There should be only one head in a maternity hospital:he mentioned the master of the Rotunda as an outstand-ing example. He pointed out that anyone could becomean obstetric specialist with constant practice andpatience. The scheme proposed by Dame Louise he fouridto be almost identical with that suggested by Blair Belland himself in 1931. He considers that peripheraldifficulties would be more easily settled if there was acentral directing body-not an advisory committee-at the Ministry of Health. Nobody, it seems, pays anyattention to an advisory body.
JOINT MEETING WITH THE
MEDICAL SOCIETY FOR THE STUDY OF.VENEREAL DISEASES
AT a joint meeting of the section of Physical Medicineof the Royal Society of Medicine and the Medical Societyfor the Study of Venereal Diseases held at the RoyalVictoria Hospital, Netley, on May 16, a discussion on
Gonococcal Arthritis and Rheumatismand their treatment by mechanically induced pyrexia wasopened by Major G. D. KERSLEY, president of the section,who described the clinical findings and results of treatmentin 50 consecutive cases of metastatic gonorrhoea. He saidthat, in general, rheumatism associated with gonococcalinfection has three striking characteristics ; the varietyof the manifestations, the variable duration of the periodbetween time of infection and onset of symptoms, andthe reaction to hyperpyrexia. The problem is toestablish the diagnostic criteria by which a case of rheum a-tism may be regarded as gonococcal. In his series therewas a patient with a history of attacks of rheumatismfor years in whom this flared up with the onset of a gono-coccal urethritis. Is such rheumatism truly gonococcal ordoes the toxin of gonorrhoea act in the same way as thetoxin of a non-specific infection in causing a flare-upof the pre-existing condition in a sensitive individual ?There were also 4 cases in which the onset of rheumatismcoincided with a recurrence of urethral discharge in whichgonococci were not found, at times ranging from 2 monthsto 21 years after an original attack of gonorrhoea.Was this attributable to latent gonococcal infection orto residual non-specific infection in the prostate ?Apart from such doubtful cases the clinical syndrome isvery varied. The brunt of the attack commonly fallson fasciae, tendons, sheaths and ligaments, particularlythe plantar fascia and the sheath of the tendo Achillis.Synovitis is common, sometimes progressing to arthritis,especially of the larger joints. The effusion may be
653
considerable and wasting is well marked. The intensityof the pain varies from minor discomfort to acute painallowing no rest. In 3 cases keratodermia blenorrhagicawas present, and in two others calcaneal periostitiswas an obvious cause of symptoms. The time relation-ship between the first evidence of infection and the onsetof the first rheumatic symptoms was established in 40cases. In 3 they were simultaneous, in 27 the averagelapse of time was a little under 2 weeks, while in theremaining 10 the average time was 4 years. The kneesand ankles were predominantly affected and next infrequency the fascial structures, the latter being especiallyresistant to treatment. The sedimentationrate wasabove 25 mm. in the hour in the majority of cases.The white-cell count varied from 7000 to 17,000,averaging 10,000 per c.mm. In 37 cases the averageperiod of hospitalisation was 3-8 weeks, and of thesepatients 27 were discharged to duty cured, and 10,although improved, had to be invalided out of the Army.Major Kersley discussed various forms of treatment andconcluded that the treatment of choice is high pro-longed fever mechanically induced and maintained at106° F. to 107° F. for sessions of 6-10 hours. In the17 patients who received this treatment, undergoing8-hour sessions for an average of 3 to 4 treatments,symptoms were promptly relieved, sedimentation-ratesfell and the patients put on weight. Only 2 cases provedresistant to treatment. The results with sulphonamideswere disappointing and in no way confirmed someenthusiastic reports. Failing hyperthermy, proteinshock by the intravenous injection of TAB vaccine provedan effective remedy and good results were also obtainedby combining pelvic short-wave applications with localgalvanism. Some success was also obtained with ionisa-tion using saline. When the joint was very painful andswollen the anode was used as the active electrode in orderto obtain its analgesic effect on nerve-endings and to em-ploy any osmotic dispersal effect on the effusion. Whenthe condition was more chronic and there was periarticu-lar thickening the kathode was used as a counter irritant.
Lieut.-Colonel A. J. KING discussed methods for thediagnosis and elimination of causative foci of infection.His series of 61 cases included all such cases treatedduring a period in which the total admissions of patientsfor the treatment of urethritis were 2719, made up of1784 in whom the gonococcus was found and 935 inwhom the diagnosis was non-specific urethritis, givingan incidence of metastatic lesions of just over 2%.The cases were grouped according to the time relation-ship between genital infection and metastatic lesions.In 34 metastasis occurred in the course of the primaryurethral infection ; 4 had suffered a previous attack ofarthritis with urethritis and the joint infections recurred asthe result of a fresh attack or recrudescence of urethritis;and the third group consisted of 22 patients withsubacute or chronic metastasis associated with chronicprostatitis occurring months or years after the originalattack of urethritis. The obvious diagnostic sign wasurethral discharge and the gonococcus was present in21 cases. In 22 cases the gonococcus was not found.This did not rule out the diagnosis of ’gonorrhoea butmight on the other hand be evidence of poor tissue reac-tion against the gonococcus predisposing to metastasis.In such cases repeated smears and cultures may ultimatelyshow the gonococcus and even repeated negative testsare not conclusive, for the gonococcus may appear in thesecretions later, even while the patient is under treatment,or may be found in the genital tract of an infected partner.It may also be found later in cultures from the prostaticsecretion. In the remaining 18 cases there was nodetectable discharge or other sign of urethral infectionon examination during the day. Smears taken beforethe first morning specimen of urine had been passed andinspection of this specimen usually gave the clue to thesource of infection. This was held to be an extremelyimportant test in all cases of doubt. In reviewing otherdiagnostic signs Colonel King maintained that thepresence of more than an occasional leucocyte in theprostatic secretion is evidence of chronic prostatitis,a condition which is likely to persist throughout lifewhatever treatment is applied. The association ofchronic prostatitis and subacute or chronic metastasisis very common and in such cases the prostate usuallyfeels quite normal to the examining finger. He empha-
sised the diagnostic importance of cultures of the prostaticsecretion in subacute and chronic cases. This is a specia-lised technique requiring a high standard of care in thepreparation of a reinforced medium and in the use of adifferential stain for isolation of the gonococcal colonies.The complement-fixation test for gonorrhoea givesvaluable results in expert hands but few have masteredthe technique. The difficulty lies in the preparationof a reliable antigen. In 90 % of cases of acute gonococcalarthritis a positive result may be expected but the per-centage is much smaller in more chronic cases and in theconnective-tissue infections. In reviewing methods oftreatment Colonel King laid stress on the value ofposterior urethral irrigations. Prostatic massage is ofvalue only when there is evidence of
"
pocketing " ofpus in the prostate. The results with sulphonamidesin varying dosage have been unimpressive but goodresults have been obtained in early cases from protein-shock therapy by means of intravenous TAB vaccine.The best technique is the " divided dose " method in which25 million organisms are given intravenously, followed’by a similar dose after 4 hours when the temperaturehas begun to rise. Mechanically produced high pro-longed fever by means of the Kettering Hypertherm hasbeen used in 16 cases. Temperatures were maintained at106° F. to 107° F. for 8 hours in each session and treat-ments were repeated at intervals of 5-7 days if required.The largest number of sessions given in any one case was6. Earlier experience at the London Hospital in treatinga small series of recent acute cases of gonococcal arthritiswas most satisfactory ; there were no failures. Thepresent series was small and very variable as to type andduration of infection. No conclusions could be drawn,but with one exception, a case of severe plantar fasciitis,all were improved ; 8 patients had chronic conditionsof long standing in which complete cure was not to beexpected ; 2 were cured and 5 remained under treatmenthaving improved considerably. The treatment hasits dangers and skilful and experienced nursing is essen-tial. Approximately 160 patients have been treated, andone died from heat stroke.Major J. B. KING described some radiological aspects
of gonorrhoeal arthritis. He said that while there are noradiological changes which are entirely characteristic, thefindings in the acute phase are often sufficiently suggestivefor the possibility of a gonorrhceal cause to be suspected.There is often a very thin line of well-marked decalcifica-tion immediately under the articular surface. This isalso seen in other infective joint lesions, but in gonococcalarthritis the integrity of the actual articular surfaceis preserved to an unusual degree, unless the lesion isextremely acute or of long standing. The only bony,as distinct from joint, manifestations of gonorrhoeawhich can be considered in any way really typical arethose in the os calcis, where there is an irregular, denseposterior cortical hyperostosis, often with the formationof large spurs into the plantar fascia and insertion ofthe tendo Achillis.
Lieut.-Colonel T. E. OSMOND urged the importance oftechnique in cultivating the gonococcus. More positiveresults should be obtained with cultures than with smears,otherwise the technique of culture must be consideredfaulty. The gonococcus grows best in an atmospherein which the oxygen tension is lowered and the CO2tension increased. The surface of the medium should bemoist, and differential staining of gonococcal coloniesby means of the oxidase test requires experience. Heagreed that the complement-fixation test for gonorrhoeais much maligned ; with a good antigen the test should bepositive in 80-90 % of cases of gonococcal arthritis. Hebelieved that failures with the sulphonamides are due tothe fact that metastatic lesions are secondary to closedfoci of infection, in which the sulphonamides have beenshown to be ineffective. In long-standing cases he hadno doubt that secondary infection plays a large part inthe process.
Colonel L. W. HARRISON deplored the modern ten-dency to discount the value of drainage of the prostateby digital massage in these cases. Good results wereobtained with this treatment before modern methods wereintroduced, and he considered that it must retain itsplace. He agreed that lowered oxygen tension withincrease of CO2 is important for culture of the gonococcusand said that the question of a suitable medium is an
654
important one for future research. It has been statedthat the presence of starch in a culture medium is moreimportant than animal protein for the growth of thegonococcus. This is one of many questions which haveto be investigated. ,
Other speakers discussed the incidence and situationof the lesions of keratodermia blenorrhagica, the differen-tial diagnosis between metastatic gonorrhoea and chronicmeningococcal septicaemia, and the question of the opti-mum duration of sessions of high fever for the treatmentof metastatic gonorrhoea.
Reviews of BooksSeasonal lilfluence on Growth, Function and Inheritance
A. B. FITT, Ph.D., professor of education, Auckland. University College. Wellington: New Zealand Council
for Educational Research ; London : Humphrey Milford,Oxford University Press. Pp. 182. 10s. 6d.
’
THE accident of birth is beyond our control, and fewof us begrudge the other fellow his cleverness or othernatural advantages ; but generations unborn may echoTristram Shandy’s strictures upon his parents whenthey learn from Professor Fitt’s book that their height,strength and intelligence may be a bit below par becausethey were not conceived in the best months of the year-in this hemisphere approximately September to December.Indeed, it appears that nature urges us in the wrongdirection, for although babies conceived during thisperiod are less likely to die in the first month of life, thereare less of them than of the poorer quality conceivedin the March-May period. These, perhaps, are the moststartling conclusions from the painstaking statisticalwork recorded in this book, but of more practical import-ance is the evidence, rarely quite final but in sumirresistible, that human beings are at their best and moststable, physically, intellectually and morally, during the.autumn-winter period, and at their worst during thespring-summer months. In children, statistics have beenanalysed on height and weight increase, intelligencetests, illness and delinquency ; in adults on output ofwork, mortality and suicide. They have been takenboth from Professor Fitt’s own investigations and fromother sources, and although alternative explanationswould be found for many individual groups of data, theiragreement in trend is difficult to account for in any otherway than by the assumption of an inherent seasonalrhythm. Numerous minor and incomplete investigationsfit in with the general scheme. The fluctuations are notlarge, but he points out their implications for short-termmeasurements of rates of change in height, weight andintelligence ; for the timing of examinations and theorganisation of work ; for the study of crime and delin-quency ; and for the practice of medicine. The under-lying cause of the rhythm is discussed, and someingeni-ous parallels with hibernation advanced, the pituitaryand hypothalamus coming in for their inevitable share ofattention. The book is important as a pioneer work,and the investigation ought to be carefully repeated indifferent parts of the world. We may yet have much tolearn about the natural history of our own species.Handbook of Midwifery
’
(llth ed.) Sir COMYNS BERKELEY, M.D. Camb., F.R.C.P.,F.R.C.S., F.R.C.O.G. London : Cassell and Co. Pp. 622.8s. 6d.Tms well-illustrated book is written for pupil mid-
wives and medical students, a body of the profession thatthe author has spent a lifetime in teaching and examining.No single man is better qualified for this job than he andthis eleventh edition of a book that was born in 1906 andis still going strong is probably the best of its kind. Thearrangement ensures study of the physiological beforethe pathological, and stresses the normality of theaverage pregnancy and labour. One small but importantcriticism must be made. Sir Comyns gives directionsfor the guidance of the midwife if she is directed by thedoctor to continue the administration of chloroform andthese directions are wise and good. But it is stillquestioned by some whether chloroform should beadministered to a woman in labour, and more doubtfulstill whether it should be given by an unqualified person.The supervision a doctor conducting a difficult forcepsdelivery can give to the anaesthetic is necessarily perfunc-
tory, and there is no good evidence that the pregnantwoman takes chloroform better than anyone else. Her-liver may already be taxed by a mild toxaemia and insuch cases chloroform is a danger.’ Perhaps in subse-quent editions Sir Comyns will incorporate a smallsection on the alternative methods of anaesthesia avail-able for domicilin,rv use.
Functional PathologyLEOPOLD LicHTWirz, M.D., clinical professor of medicine,Columbia University. New York : Grune and Stratton.Pp. 567.THE mechanism of diseased function is not simple,
because the control of normal function is ill understoodand because structural changes in the body are notalways present to account for signs and symptoms.This is not a textbook but a personal interpretation,after thirty years of clinical and laboratory experience,of the manifestations of the main medical ailments.Endocrine disorders and rheumatism, for example, arefully described and allergy is given more attention thanmost English writers would give it. Some readers maydoubt whether it has been proved conclusively thatacute glomerular nephritis is an allergic disease or thatHenoch’s purpura is an example of anergy. The shortchapters which discuss body-water and the pathology ofintracellular oxidation are among the best. Not muchis said of treatment but the writer believes garlic usefulfor hypertension despite its disadvantages. ThroughoutProfessor Lichtwitz uses the informal, discursive andreminiscent tone of the clinic, and draws his illustrationsfrom a wide knowledge of history and a wealth of lesserknown sources of reference. The book has excellentphotographs, useful tables and charts and should fulfilthe author’s wish to stimulate discussion.
New InventionsAN IMPROVED LEUCOTOME
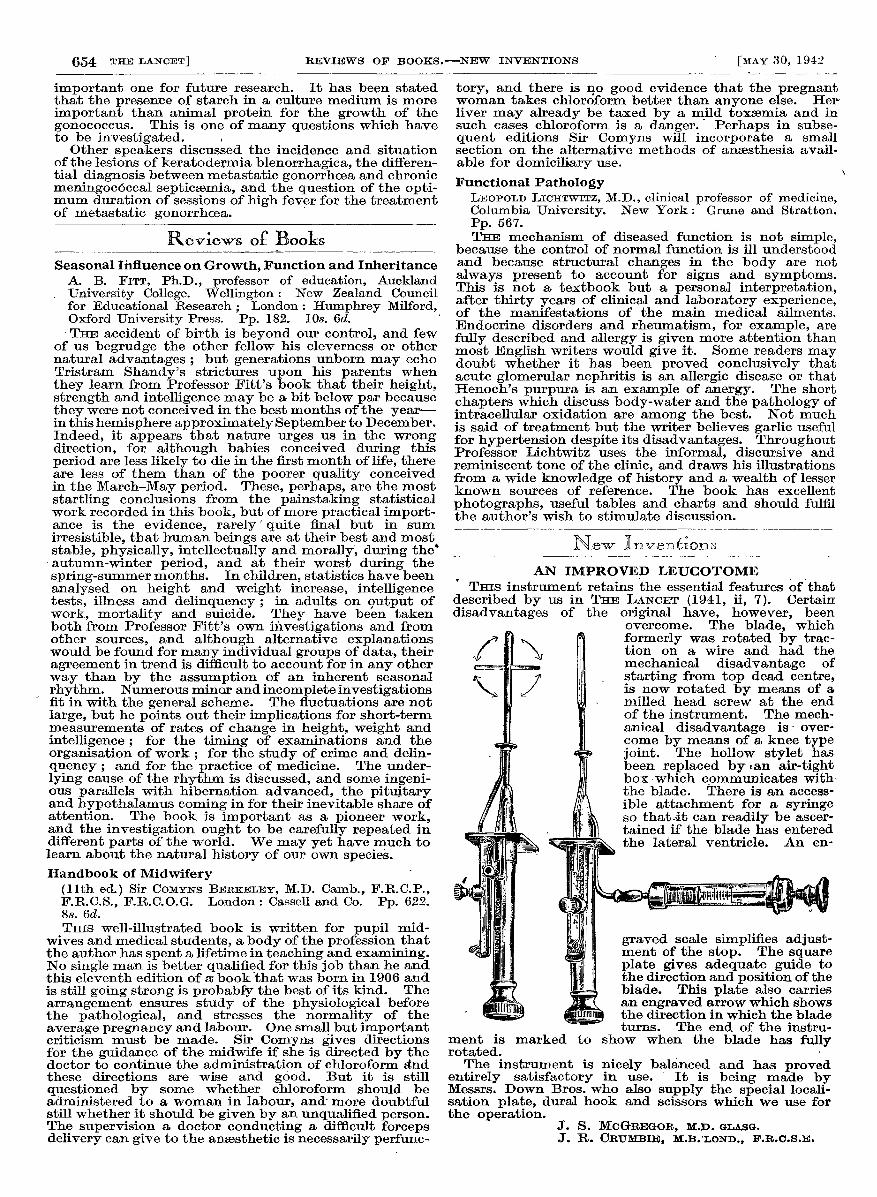
THIS instrument retains the essential features of thatdescribed by us in THE LANCET (1941, ii, 7). Certaindisadvantages of the original have, however, been
overcome. jme uiaue, Wniun
formerly was rotated by trac-/ ’Br i tion on a wire and had the,--, -. I mechanical disadvantage of
/ I! starting from top dead centre,, :: is now rotated by means of a
, . ! milled head screw at the endof the instrument. The mech-anical disadvantage is over-
j come by means of a knee type
If! joint. The hollow stylet hasM been replaced byan air-tightJ box which communicates with-
j the blade. There is an access-fjM m ible attachment for a syringem B so that.it can readily be ascer-
" fBM , )t) tained if the blade has entered
tF z - ! the lateral ventricle. An en-
B : H’ graved scale simplifies adjust-) g ment of the stop. The squarem at z plate gives adequate guide tojpL ’ the direction and position of theNT i&— blade. This plate also carries
, d JSEL an engraved arrow which shows<§j’! the direction in which the blade
turns. The end of the instru-ment is marked to show when the blade has fullyrotated.The instrument is nicely balanced and has proved
entirely satisfactory in use. It is being made byMessrs. Down Bros. who also supply the special locali-sation plate, dural hook and scissors which we use forthe operation.
J. S. MCGREGOR, M.D. GLASG.J. R. CRUMBIE, M.B. LOND., F.R.C.S.E.