J O T JOURNALOF ORTHOPAEDIC TRAUMA www.jorthotrauma.com OFFICIAL JOURNAL OF Orthopaedic Trauma Association Belgian Orthopaedic Trauma Association Canadian Orthopaedic Trauma Society Foundation for Orthopedic Trauma International Society for Fracture Repair The Japanese Society for Fracture Repair Special Case Report Series CASE REPORTS
Transcript
JOT
JOURNALOF ORTHOPAEDIC
TRAUMA
www.jorthotrauma.com
OFFICIAL JOURNAL OF
Orthopaedic Trauma Association
Belgian Orthopaedic Trauma Association
Canadian Orthopaedic Trauma Society
Foundation for Orthopedic Trauma
International Society for Fracture Repair
The Japanese Society for Fracture Repair
Special Case Report Series
CASE REPORTS
Fixator-Assisted Femoral Lengthening After IntramedullaryExchange Nailing for Subtrochanteric Nonunion
Frank A. Liporace, MD and Richard S. Yoon, MD
Summary: Nonunions in the femur can be a severely debilitatingcondition. When a nonunion results in significant shortening andleg length discrepancy, simple activities of daily living becomeextremely difficult and painful tasks. Here, we present a 36-year-oldman who presented 3 years after a motor vehicle accident,complaining of severe left thigh pain and a short left lowerextremity. Initially treated in Egypt with an intramedullary nail(IMN) and distal screws, workup revealed an aseptic subtrochan-teric femoral nonunion with a leg length discrepancy of approxi-mately 6.5 cm. The patient subsequently underwent exchange nailwith rail fixator placement and was lengthened over the nail. Afterachieving adequate length, the patient underwent a secondexchange nail, which was complicated by IMN instability. Becauseof the IMN instability, the patient underwent a third exchange nailwith blocking screws and finally healed. On final follow-up, thepatient was pain free and no longer felt the leg length discrepancy,with an overall discrepancy of approximately 1.5 cm.
INTRODUCTIONWith contemporary fixation options, subtrochanteric nonunions of
the femur are a rare occurrence.1,2 However, when they do occur,exchange nailing is often a popular and well-received first option.3–6
Although a systematic approach to treating an isolated aseptic nonunionmay offer a reliable road to healing, coupling nonunion with concom-itant leg length discrepancy exponentially increases the overall diffi-culty of the treatment regimen.
Here, we present a 36-year-old man presenting with bothsubtrochanteric femoral nonunion and concurrent leg lengthdiscrepancy. We outline our workup, our treatment regimen,rationale, and tips to avoid specific pitfalls encountered duringthe case. Informed consent was obtained from the patient.
CASE PRESENTATIONOur patient is a 36-year-old man who presented to our office
complaining of debilitating left thigh pain and a short left lowerextremity.He is ahealthy,nondiabetic, nonsmokerwithout a significantmedical history. Three years before presentation, he suffered a closedleft subtrochanteric femur fracture after a high-energy motor vehicleaccident. The patient was treated in Egypt with 20 cm laterally basedopen reduction and intramedullary nail (IMN) placement.
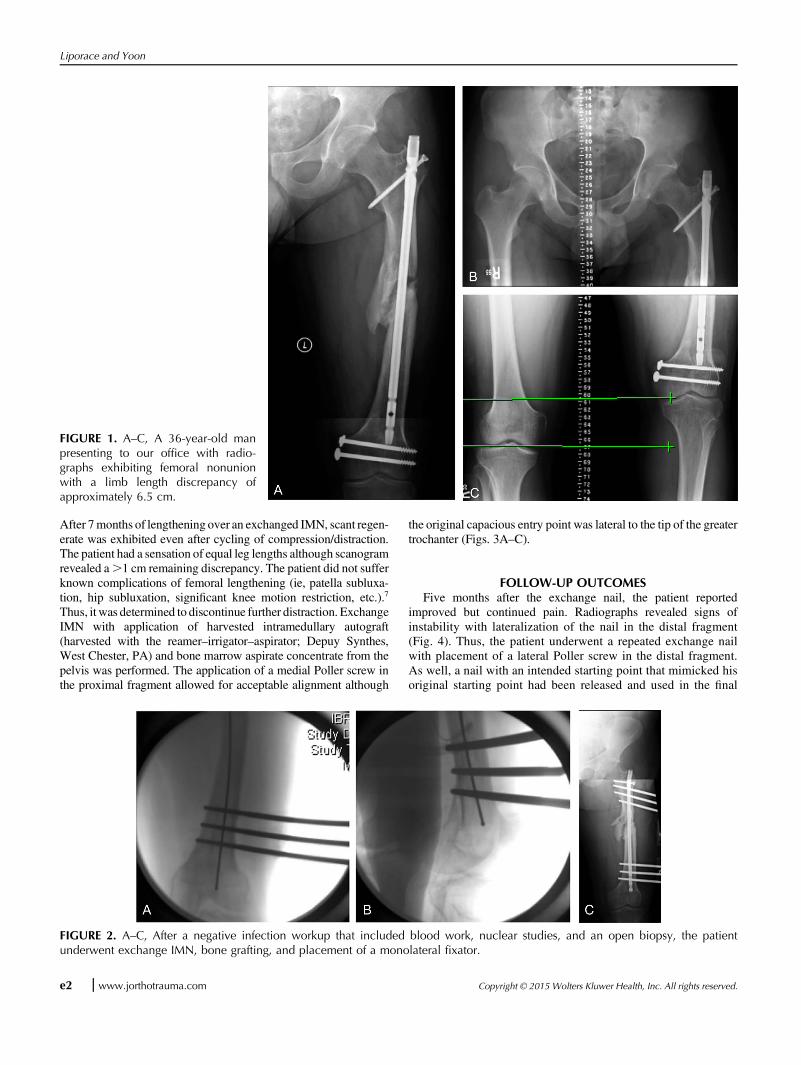
On initial presentation to our office, the patient was afebrile withstable vitals. In a wheel chair, the patient was able to ambulate shortdistances with a large shoe lift under the left lower extremity. Physicalexamination was notable for a large, nonerythematous, dry, healedwound over the left lateral thigh measuring approximately 20 cm inlength. The patient reported pain. Radiographs revealed a subtrochan-teric femoral nonunion and a left femur that was approximately 6.5 cmshorter than the contralateral side (Figs. 1A–C).
DIAGNOSTIC FOCUS—SURGICAL MANAGEMENTInfection workup, including ESR, CRP, WBC, and nuclear
studies, as well as a nonunion site biopsy, was negative. The goalswere limb lengthening, promoting healing, and alleviating insta-bility/pain. Initially, a narrow diameter IMN was placed with amonolateral external fixator to allow for distraction (Figs. 2A–C).
Accepted for publication February 20, 2015.
From the Division of Orthopaedic Trauma, Department of OrthopaedicSurgery, NYU Hospital for Joint Diseases, New York, NY.
F. A. Liporace has received royalties for lower extremity intramedullarynails from Biomet, Inc, Warsaw, IN. R. S. Yoon reports no conflict ofinterest.
Reprints: Frank A. Liporace, MD, Division of Orthopaedic Trauma, Depart-ment of Orthopaedic Surgery, NYU Hospital for Joint Diseases, 301 E 17thSt, Suite 1402, New York, NY 10003 (e-mail: [email protected]).
The views and opinions expressed in this case report are those of theauthors and do not necessarily reflect the views of the editors of Journalof Orthopaedic Trauma or Biomet.
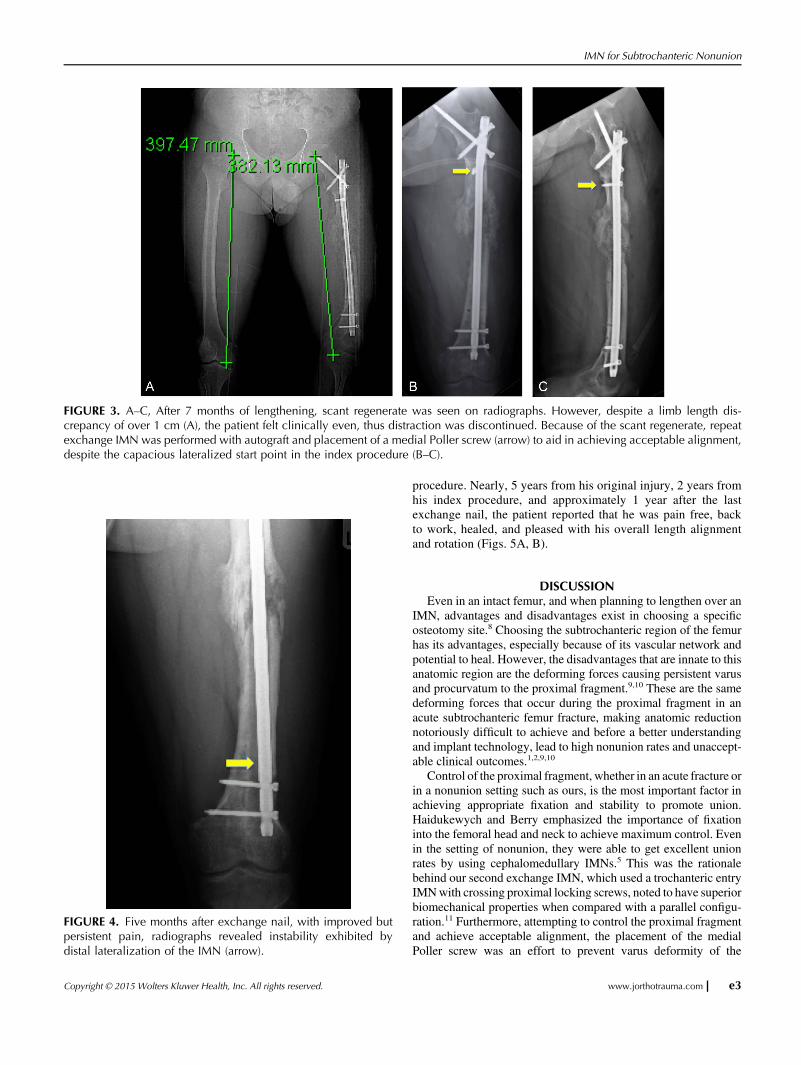
After 7months of lengthening over an exchanged IMN, scant regen-erate was exhibited even after cycling of compression/distraction.The patient had a sensation of equal leg lengths although scanogramrevealed a.1 cm remaining discrepancy. The patient did not sufferknown complications of femoral lengthening (ie, patella subluxa-tion, hip subluxation, significant knee motion restriction, etc.).7
Thus, it was determined to discontinue further distraction. ExchangeIMN with application of harvested intramedullary autograft(harvested with the reamer–irrigator–aspirator; Depuy Synthes,West Chester, PA) and bone marrow aspirate concentrate from thepelvis was performed. The application of a medial Poller screw inthe proximal fragment allowed for acceptable alignment although
the original capacious entry point was lateral to the tip of the greatertrochanter (Figs. 3A–C).
FOLLOW-UP OUTCOMESFive months after the exchange nail, the patient reported
improved but continued pain. Radiographs revealed signs ofinstability with lateralization of the nail in the distal fragment(Fig. 4). Thus, the patient underwent a repeated exchange nailwith placement of a lateral Poller screw in the distal fragment.As well, a nail with an intended starting point that mimicked hisoriginal starting point had been released and used in the final
FIGURE 1. A–C, A 36-year-old manpresenting to our office with radio-graphs exhibiting femoral nonunionwith a limb length discrepancy ofapproximately 6.5 cm.
FIGURE 2. A–C, After a negative infection workup that included blood work, nuclear studies, and an open biopsy, the patientunderwent exchange IMN, bone grafting, and placement of a monolateral fixator.
procedure. Nearly, 5 years from his original injury, 2 years fromhis index procedure, and approximately 1 year after the lastexchange nail, the patient reported that he was pain free, backto work, healed, and pleased with his overall length alignmentand rotation (Figs. 5A, B).
DISCUSSIONEven in an intact femur, and when planning to lengthen over an
IMN, advantages and disadvantages exist in choosing a specificosteotomy site.8 Choosing the subtrochanteric region of the femurhas its advantages, especially because of its vascular network andpotential to heal. However, the disadvantages that are innate to thisanatomic region are the deforming forces causing persistent varusand procurvatum to the proximal fragment.9,10 These are the samedeforming forces that occur during the proximal fragment in anacute subtrochanteric femur fracture, making anatomic reductionnotoriously difficult to achieve and before a better understandingand implant technology, lead to high nonunion rates and unaccept-able clinical outcomes.1,2,9,10
Control of the proximal fragment, whether in an acute fracture orin a nonunion setting such as ours, is the most important factor inachieving appropriate fixation and stability to promote union.Haidukewych and Berry emphasized the importance of fixationinto the femoral head and neck to achieve maximum control. Evenin the setting of nonunion, they were able to get excellent unionrates by using cephalomedullary IMNs.5 This was the rationalebehind our second exchange IMN, which used a trochanteric entryIMNwith crossing proximal locking screws, noted to have superiorbiomechanical properties when compared with a parallel configu-ration.11 Furthermore, attempting to control the proximal fragmentand achieve acceptable alignment, the placement of the medialPoller screw was an effort to prevent varus deformity of the
FIGURE 3. A–C, After 7 months of lengthening, scant regenerate was seen on radiographs. However, despite a limb length dis-crepancy of over 1 cm (A), the patient felt clinically even, thus distraction was discontinued. Because of the scant regenerate, repeatexchange IMN was performed with autograft and placement of a medial Poller screw (arrow) to aid in achieving acceptable alignment,despite the capacious lateralized start point in the index procedure (B–C).
FIGURE 4. Five months after exchange nail, with improved butpersistent pain, radiographs revealed instability exhibited bydistal lateralization of the IMN (arrow).
proximal fragment and counteract the large lateral start point usedin the index procedure.
However, an unbalanced construct was created with too rigidfixation proximally and relatively weaker distal fragmentfixation. By ignoring the distal fragment and not accountingfor an overpowering proximal valgus force, lateralization of theIMN occurred distally. Furthermore, with a slightly medial startpoint for the trochanteric entry nail, inherent valgus was builtinto this construct. Thus, on revision and the final exchangenail, a more balanced construct was placed with a proximalparallel screw configuration (enough to prevent varus cutout)coupled with distal locking screws and a lateral Poller screw toprevent recurrent valgus deformity. The final nail was alsoa lateral trochanteric entry nail, which by design avoids varusdeformity (for our case using the original start point), but forthis case, also avoided undesired valgus, which caused priorinstability.
CONCLUSIONSApplying the basic principles of both nonunion repair and
lengthening concurrently can lead to a good clinical result. However,one must take into account the importance of achieving proximalfixation into the head neck junction to counteract the deforming forcesinherent to the subtrochanteric region but without ignoring the distalfragment. One should be cognizant of the nail type, the starting point,and the subsequent deformity that canbe caused by each. Poller screwsplaced medial to the nail proximally and lateral to the nail distally canalso aid in avoiding instability and maintaining proper alignment.Finally, clinical success is achieved not only by evaluating radio-graphic evidence of healing but more importantly with the patient’sshared decision making, which in this case, led to clinical successdespite a residual 1.5 cm discrepancy.
REFERENCES1. Afsari A, Liporace F, Lindvall E, et al. Clamp-assisted reduction of highsubtrochanteric fractures of the femur. J Bone Joint Surg Am. 2009;91:1913–1918.
2. Wiss DA, Brien WW. Subtrochanteric fractures of the femur. Results oftreatment by interlocking nailing. Clin Orthop Relat Res. 1992:231–236.
3. Furlong AJ, Giannoudis PV, DeBoer P, et al. Exchange nailing for femoralshaft aseptic non-union. Injury. 1999;30:245–249.
4. Gao KD, Huang JH, Li F, et al. Treatment of aseptic diaphyseal nonunionof the lower extremities with exchange intramedullary nailing and block-ing screws without open bone graft. Orthop Surg. 2009;1:264–268.
5. Haidukewych GJ, Berry DJ. Nonunion of fractures of the subtrochantericregion of the femur. Clin Orthop Relat Res. 2004:185–188.
6. Swanson EA, Garrard EC, Bernstein DT, et al. The results of a systematicapproach to exchange nailing for the treatment of aseptic femoral nonun-ions. J Orthop Trauma. 2015;29:21–27.
7. Song HR, Oh CW, Mattoo R, et al. Femoral lengthening over an intra-medullary nail using the external fixator: risk of infection and knee prob-lems in 22 patients with a follow-up of 2 years or more. Acta Orthop.2005;76:245–252.
8. Nayagam S. Femoral lengthening with a rail external fixator: tips andtricks. Strateg Trauma Limb Reconstr. 2010;5:137–144.
9. Kraemer WJ, Hearn TC, Powell JN, et al. Fixation of segmental subtro-chanteric fractures. A biomechanical study. Clin Orthop Relat Res. 1996:71–79.
10. Sims SH. Subtrochanteric femur fractures. Orthop Clin North Am. 2002;33:113–126, viii.
11. Grisell M, Moed BR, Bledsoe JG. A biomechanical comparison of tro-chanteric nail proximal screw configurations in a subtrochanteric fracturemodel. J Orthop Trauma. 2010;24:359–363.
FIGURE 5. A–B, Repeat exchange nailing useda newer IMN design that took advantage of theoriginal lateralized start point used at the index sur-gery. Cephalomedullary fixation with a distallyplaced lateral Poller screw (arrow) aided in main-taining alignment and appropriate stability until finalfollow-up (A–B).
Read the rest of the JOT Case Reports online on www.jorthotrauma.com. It’s theGrandRounds series from the Journalof Orthopaedic Trauma, the official journal of the OrthopaedicTrauma Association.