161
JP Pretorius Principal Specialist Surgeon Dept of Surgery and Division of Intensive Care University of Pretoria & Pretoria Academic Hospital PROPHYLACTIC ANTIMICROBIAL THERAPY
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | darleen-corey-armstrong |
| View: | 222 times |
| Download: | 3 times |
JP Pretorius
Principal Specialist Surgeon
Dept of Surgery and Division of Intensive Care
University of Pretoria &
Pretoria Academic Hospital
PROPHYLACTIC ANTIMICROBIAL THERAPY

Outline – Red hot terminology• Classification of wounds• Why is there a need to “get it right first time”?
Early appropriate therapy• Source control• Definitions and terminology:
1) Surgery and antibiotic prophylaxis2) What is “collateral damage”3) Empiric therapy (educated 1st choice)4) Directed therapy (MCS results)5) De-escalation (adjusted choice)6) Stopping / Discontinuing therapy7) Community acquired infection8) Health Care Associated infection9) Nosocomial infection
• Changing trends in antibiotic resistance• Choices for empiric therapy• Choices for pathogen defined therapy (directed)• Doses / Duration / Pk / Pd / Efficient administration
INDEPENDENT PREDICTORS OF INFECTION
• Preoperative shock• Number of organs injured• Concomitant central nervous system
injury

Determinants of surgical wound infection
Microbial concentrationand virulence
Foreign material
Injury to wound tissuesResistance to
peri-operative AB’s
= Risk fo surgical wound infection
General/Local host immunity
Peri-operative antibiotics

Risk of Surgical Site Infectionand Degree of wound contamination
Altemeier classes 1 – 4:
Class 1: Clean surgery: 1 – 2% riskClass 2: Clean contaminated surgery: 5 – 15% risk
(elective colectomy or hysterectomy)
Class 3: Contaminated surgery: 15 – 30% risk (enterotomy with spillage)
Class 4: Dirty surgery: > 30% risk (established infection ie intra-abdominal abcess)
Simplistic but still valid!
Patient characteristics associated with increased risk for surgical site
infection
?

Patient characteristics associated with increased risk for surgical site
infection• Extremes of age• Diabetes / periopeative hyperglycaemia• Concurrent tobaco use• Remote infection at time of surgery• Obesity• Malnutrition• Low preoperative S-albumin• Concurrent steroid use• Prolonged preoperative stay• Prior site irradiation• Colonization with S aureus
Procedural factors associated with increased risk for surgical site
infections
?

Procedural factors associated with increased risk for surgical site
infections• No preoperative antiseptic showering• Shaving of site night prior to procedure• Use of razor for hair removal• Improper preop skin preparation• Improper antimicrobial prophylaxis• Delayed redosing of AB’s in prolonged cases• Inadequate OR ventilation• Increased OR traffic• Break in sterile technique and asepsis• Perioperative hypothermia / hypoxia• Poor surgical technique

Major Pathogens in Surgical Wound Infections
?
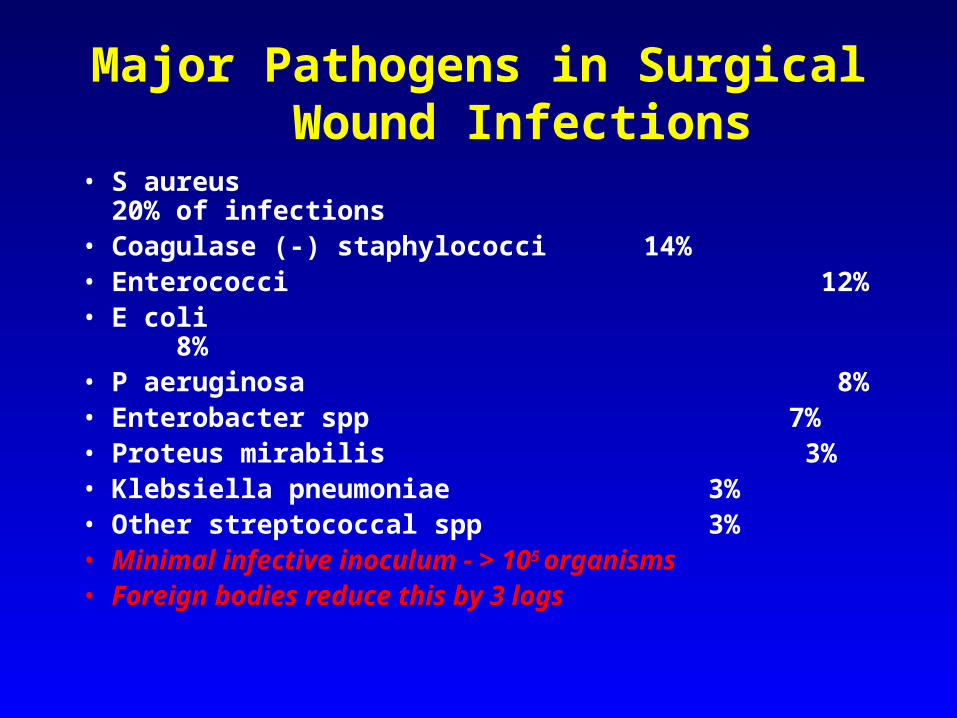
Major Pathogens in Surgical Wound Infections
• S aureus 20% of infections• Coagulase (-) staphylococci 14%• Enterococci 12%• E coli 8%• P aeruginosa 8%• Enterobacter spp 7%• Proteus mirabilis 3%• Klebsiella pneumoniae 3%• Other streptococcal spp 3%• Minimal infective inoculum - > 105 organisms• Foreign bodies reduce this by 3 logs
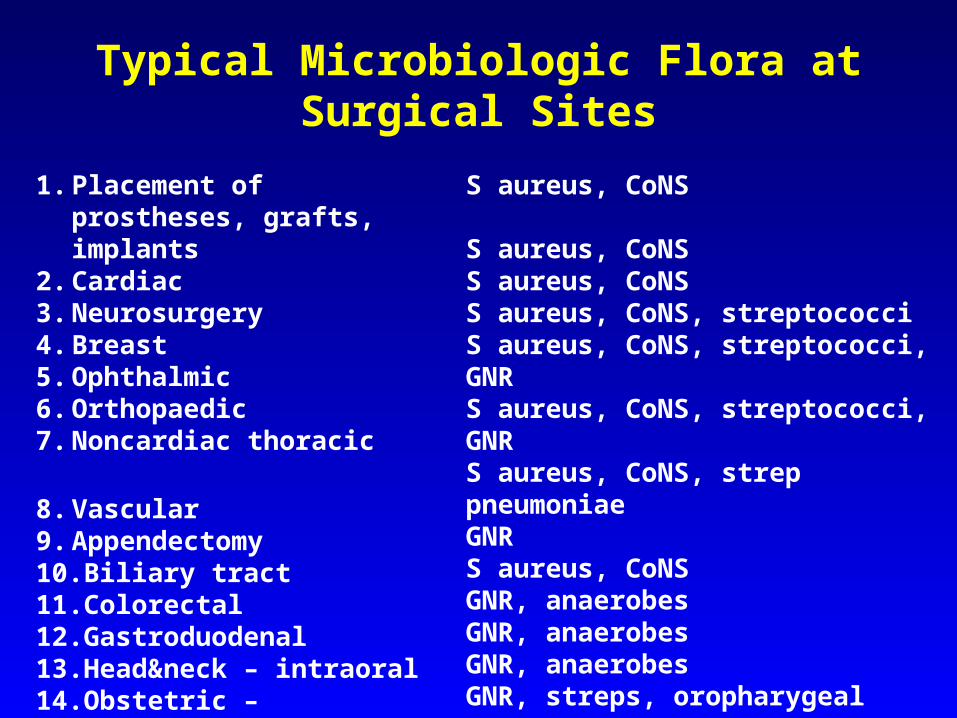
Typical Microbiologic Flora at Surgical Sites
S aureus, CoNS
S aureus, CoNSS aureus, CoNSS aureus, CoNS, streptococciS aureus, CoNS, streptococci, GNRS aureus, CoNS, streptococci, GNRS aureus, CoNS, strep pneumoniaeGNRS aureus, CoNSGNR, anaerobesGNR, anaerobesGNR, anaerobesGNR, streps, oropharygeal anaerS aureus, streps, oroph anaerGNR, enterococ, group B strepGNR
1. Placement of prostheses, grafts, implants
2. Cardiac3. Neurosurgery4. Breast5. Ophthalmic6. Orthopaedic7. Noncardiac thoracic
8. Vascular9. Appendectomy10.Biliary tract11.Colorectal12.Gastroduodenal13.Head&neck – intraoral14.Obstetric – Gyneacological15.Urologic

Antibiotic prophylaxis for longer than 24 hours not
only has no benefit, but is now recognized to be
detrimental
Unfortunately….. reducing prophylaxis to less than 24 hours has not become popular despite evidence that prolonged prophylaxis increases the risk of nosocomial bloodstream infections. It is imperative for surgeons to modify their practices.

Current recommendation for all elective surgical procedures
Single-dose prophylaxis with a first- or second generation cephalosporin - even in:
• Cardiac-• Vascular-• Orthopedic-• Neurosurgical procedures (where a 24 hour
regimen has been traditional)
EVEN:
a SINGLE dose of antibiotic administered appropriately, increases the risk of such nosocomial infections as: 1. Pneumonia2. Antibiotic associated colitis
AND: Intraoperative redosing is prudent if:1. the operation > 3hrs2. blood loss > 1.5L
* Once the incision is closed, parenteral antibiotics no longer have an impact on the risk of infection!* Prolonged prophylaxis sets the stage for emergence of resistant organisms
According to reports from the Centers for Disease Control:Antibiotic prophylaxis may be administered
appropriately based on the patients RISK FACTORS:
• Abdominal procedure
• Any operation > 2 hrs
• Contaminated or dirty field
• > 3 comorbid medical illnesses
Stratification done by:
• Number of risk factors present
• Degree of wound contamination
The incidence of wound infection increased significantly as the
number of risk factors increased:
• 1 risk factor + dirty wound = 7% wound infection rate
• 4 risk factors + the same dirty wound = 27% wound infection rate

Published Guidelines for Antibiotic Prophylaxis in Surgical patients:
• Single dose prophylaxis• 1st Generation Cephalosporin (Cefazolin) for most
procedures (Workhorse)• Multiple dosing with Cefazolin:
48 hrs in cardiac cases24 hrs in vascular cases
• The AB chosen, must cover the spectrum of expected organisms. eg Single dose 2nd generation cephalosporin for abdominal trauma, appendectomy, colorectal procedures
• Anti-MRSA drugs used only for prophylaxis on documented incidence of surgical site infections in your hospital (Condon threshold MRSA > 20% )
RECENTLY:
The Medical Letter on Drugs and Therapeutics
recommended that multiple doses may be inappropriate for
ANY surgical prophylaxis!!!!
eg: Prophylaxis of Endocarditis
The “ less is more “ trend – reflected by the AHA recommendations:
1. Most cases of endocarditis are not attributable to an invasive procedure
2. Cardiac conditions are stratified in relation to endocarditis risk as high / moderate /negligible
3. Overall fewer procedures require prophylaxis
4. When using prophylaxis, prescribe fewer antibiotics and for shorter terms

Timing of prophylaxis• Burke 1961: the surgical wound is best protected
when antibiotics are administered before the incision is made.
• Classen 1992: 30 yrs later timelines for administration - still a major problem!!!!
• New York State’s peer-review programme 1996:
* only 86% received AB’s although indicated
* 44 different AB’s used for 2256 patients• Nichols 1972: some standardization for colon
preparation pre-op: oral neomycin, erythromycin or metronidazole
• < 2/3 received either oral or timely parenteral AB before elective colon surgery
Timing continued -
• Liberal definition of “TIMELY” = 2 hrs up to the time of the skin incision
• NY State study: only 61% received timely AB prophylaxis
• In 26% AB’s were administered prematurely• Adequate tissue concentrations of AB’s at time of
skin incision – 46% of aortic surgery patients
- 73% of colectomy patients
- 60% of hip surgery patients
Penicillin Allergy• Serious penicillin allergy is less common than
medical records portray• Uncritical history taking, labels patients who are
not penicillin allergic• Epidemiologic studies show incidence of 7/1000
of general population (anaphylactic allergy to penicillin)
• First reaction is worst• Cross-reactivity between ceph and pen allergy is
only about 5%. Thus can give ceph, provided it is not an anaphylactoid reaction
• Childhood pen allergies can be outgrown• Critically ill patients may be anergic and unable
to react
Hospital Infection Control Practices Advisory Committee
Recommendations for Surgical Antimicrobial prophylaxis
• Administer AB only when indicated; select based on published recommendations for a specific operation. Assure efficacy against most common pathogens
• Administer AB intravenously, timed to ensure bactericidal serum and tissue concentrations when the incision is made
• Maintain therapeutic concentrations during operation and, at most, a few hours after closure
• Elective colorectal operations: mechanical preparation with enemas, cathartic agents, non-absorbable oral AB’s the day before surgery in addition to timely IV antimicrobial drugs.
• High risk caesarean section patients, administer IV AB’s immediately after cord is clamped

The keys to rational antibiotic prophylaxis in surgical patients include:
1. Timely and accurate diagnosis2. Rapid and definitive therapy3. Astute differentiation of infection from contamination and sterile inflammation

Definitions as an aid to planning prophylaxis
• Contamination: presence of pathogenic microorganisms on normally sterile tissue without an inflammatory response – requires only a single dose off antibiotic for prophylaxis
• Infection: invasion of a pathogenic microorganism into normally sterile tissue with a local inflammatory host response – necessitates therapeutic antibiotics
Antibiotics are NOT APPROPRIATE for sterile inflammation due to a noninfectious trigger, such as severe tissue injury

Thank you !
Example: Endocarditis Prophylaxis
• Negligible – mitral valve prolapse with midsystolic click, no regurgitation, no thickened leaflets
- implanted non-valve devices (pacemakers and defibrillators)
• Moderate – single dose ampicillin• High – ampicillin with gentamycin
Avoid broad-spectrum agents eg 3rd generation Cephalosporins!!!!!!

Example: Endocarditis ProphylaxisGastrointestinal and Genitourinary procedures:
• Moderate risk: single oral dose of amoxicillin or IV ampicillin
• High risk: an aminopenicillin with gentamycin 30 minutes before surgery
+
another dose of ampicillin alone 6 hrs thereafter
AIM: maximal coverage against enterococci, the major pathogens in endocarditis folowing GI/GU surgery.
Optimising Antibiotic Treatment in Serious
Infections

1. Intra-abdominal InfectionTHE PROBLEM
• Important cause of ICU morbidity and mortality.
• ICU admission for IAI – 30% succumb.
• Tertiary peritonitis >50% mortality.
• Association between progressive organ dysfunction and occult intraperitoneal infection.
Marshall JC CCM 2003

2. Intra-abdominal Infection.THE PERITONEAL CAVITY
• Normally <100ml of fluid, with scattered macrophages and lymphocytes.
• Diaphragmatic movement / contraction generates negative pressures.
• Peritoneal fluid moves upward towards specialized fenestrae in diaphragmatic peritoneum, draining into the lymphatic system.
• Vigorous inflammatory response increased vascular permeability protein-rich exudate cytokines and chemokines influx of monocytes and neutrophils

3. Intra-abdominal Infection
THE INFLAMMATORY RESPONSE
• Tissue factor expression of peritoneal macrophages.• Coagulation cascade is activated.• Accelerated generation of fibrin.• Fibrin polymerizes to form adhesions and capsules of
abscesses.• Rich somatic nerve supply – thus severe pain.• Pain localises to area of maximal inflammation.• Normal innate immune response is rapid and effective a) Neutrophil phagocytosis is impaired by
complicated peritonitis. b) Fibrin deposition can impede microbial clearance.
4. Intra-abdominal InfectionPATHOGENESIS
• Disruption of adjacent GIT• Spillage of complex indigenous flora.• Stomach and Duodenum Sterile Sparse gm-positive organisms, lactobacilli and occasionally Candida.• Proximal small bowel. Gm-negative organisms• Distal small bowel and colon Anaerobes Importance in stable patterns of intestinal
colonization. (Colonization resistance)• CANDIDA…….???

5. Intra-abdominal InfectionPATHOGENESIS cont.
• In the critically ill normal colonization resistance is disrupted over time.
• Due to anti-anaerobic antibiotics• Leads to colonization by Candida and vancomycin-
resistant Enterococci.• Explains the typical flora of tertiary peritonitis.• Enterococci more often in post op peritonitis• Nasal MRSA colonization risk factor for MRSA
peritonitis.
6. Intra-abdominal Infection
PATHOGENESIS: SUMMARY.
• Acute loss of integrity of gut wall – acute spillage with generalized peritonitis.
• Slow leakage of gut content – inflammatory response with abscess formation.
• After both – vigorous systemic response leading to acute organ system dysfunction.

Dupont (n=264)
Roehborn (n=110)
Gram Positive Cocci Staphylococcus spp Streptococcus spp Enterococcus spp
Gram Negative Bacilli Escherichia coli Klebsiella spp Enterobacter spp Pseudomonas spp
Bacteroides spp Miscellaneous
2
11 11
35 6 4 2 9
19
2
15 5
38 7 4 2
11 15
Dupont H. Antimicrob Agents Chemother 2000;44:2028-33Roehrborn A. Clin Infect Dis 2001;33:1513-9
Proportions of Bacterial Isolates (%)in Community-acquired Peritonitis
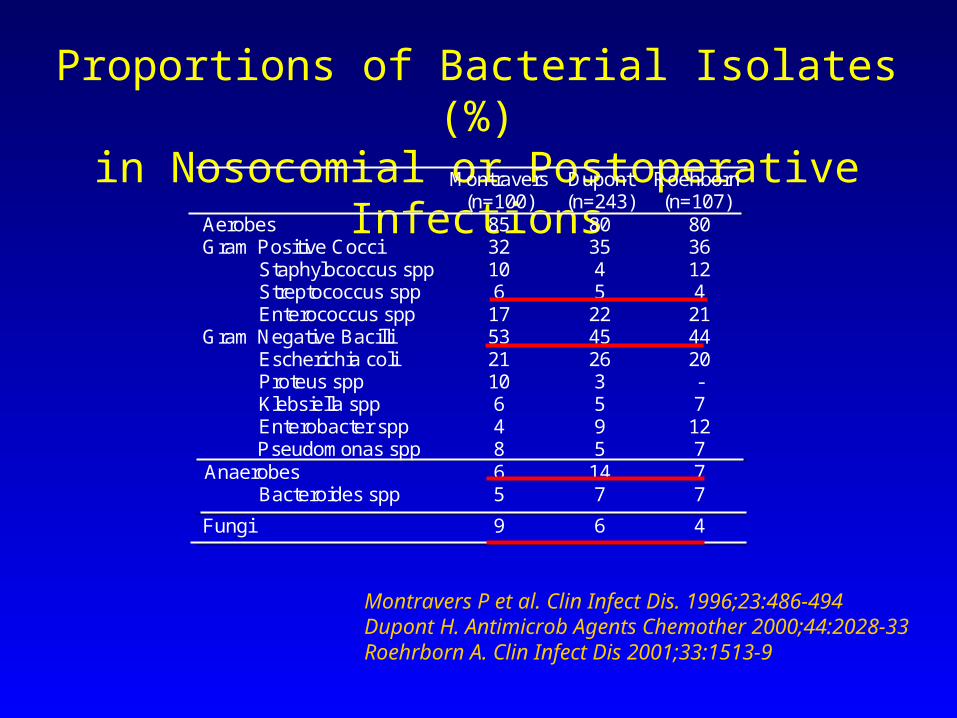
Proportions of Bacterial Isolates (%)in Nosocomial or Postoperative Infections
Montravers P et al. Clin Infect Dis. 1996;23:486-494Dupont H. Antimicrob Agents Chemother 2000;44:2028-33Roehrborn A. Clin Infect Dis 2001;33:1513-9
Montravers (n=100)
Dupont (n=243)
Roehborn (n=107)
Aerobes Gram Positive Cocci
Staphylococcus spp Streptococcus spp Enterococcus spp
Gram Negative Bacilli Escherichia coli Proteus spp Klebsiella spp Enterobacter spp
Pseudomonas spp
85 32 10 6
17 53 21 10 6 4 8
80 35 4 5
22 45 26 3 5 9 5
80 36 12 4
21 44 20 - 7
12 7
Anaerobes Bacteroides spp
6 5
14 7
7 7
Fungi 9 6 4

Microbiology
• Gram negative aerobic organisms are associated with acute lethality
• Anaerobic organisms predispose to abscesses Onderdonk Infect Immunol 1997
• Eradication of anaerobes predisposes to overgrowth of E.coli and colonization with Candida spp and VRE Berg Infect Immunol 1981 Thomakos Chemotherapy 2003 Donskey NEJM 2000
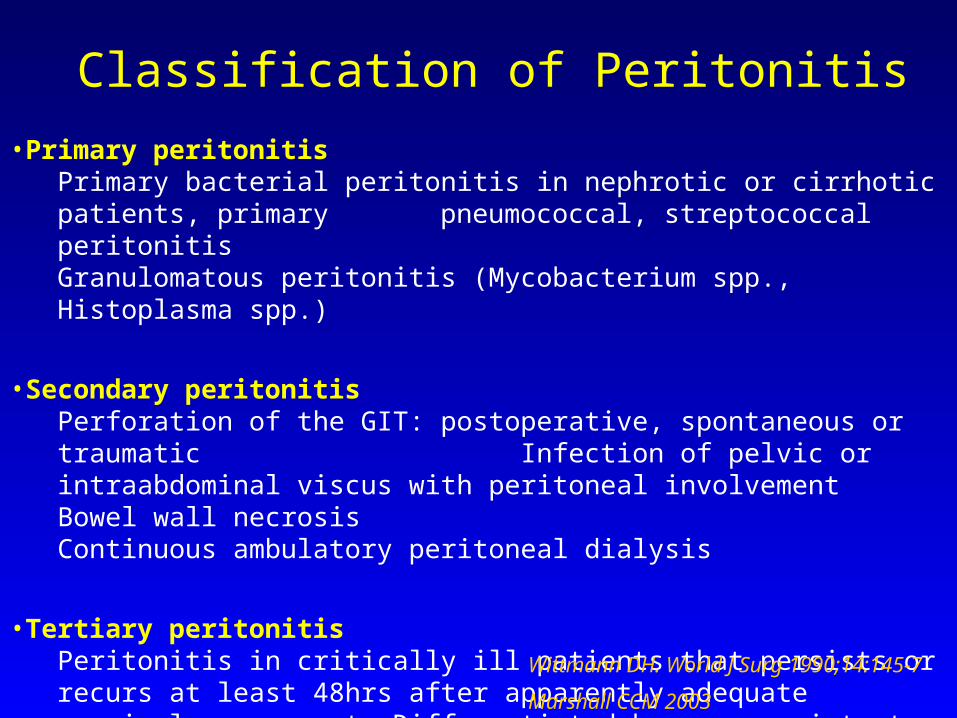
•Primary peritonitisPrimary bacterial peritonitis in nephrotic or cirrhotic patients, primary pneumococcal, streptococcal peritonitisGranulomatous peritonitis (Mycobacterium spp., Histoplasma spp.)
•Secondary peritonitisPerforation of the GIT: postoperative, spontaneous or traumatic Infection of pelvic or intraabdominal viscus with peritoneal involvement Bowel wall necrosisContinuous ambulatory peritoneal dialysis
•Tertiary peritonitisPeritonitis in critically ill patients that persists or recurs at least 48hrs after apparently adequate surgical management. Differentiated by more resistant organisms and poor response to surgery and antibiotics
Wittmann DH. World J Surg 1990;14:145-7
Classification of Peritonitis
Marshall CCM 2003

Classification of peritonitis
SeverityOutcome is determined by age, delay in diagnosis and
therapy, inappropriate therapy, APACHE, anatomic source of infection, presence of resistant pathogens Barie Curr Opin Crit Care 2001
Published trials of antibiotic therapy have enrolled patients with a mean APACHE of 8 Barie Arch Surg 1997
Severe infection may reasonably be defined as an APACHE ≥ 15

Microbiology of PeritonitisPrimary Peritonitis Secondary Peritonitis Tertiary Peritonitis
Gm-negative bacteria Gm-negative bacteria Gm-negative bacteria
Eschecheri coli E. coli 32-61 % Pseudomonas
Klebsiella Enterobacter 8-26% Enterobacter
Klebsiella 6-26% Acinetobacter
Proteus 4-23%
Gm-positive bacteria Gm-positive bacteria Gm-positiv bacteria
S. aureus (MRSA) Enterococci 18-24% Enterococci
Enterococci Streptococci 6-55% Coagulase-negative
Pneumococci Staphylococc 6-16% Staphylococci
Anaerobic bacteria
Bacteroides 25-80%
Clostridium 5-18%
Fungi 2-15% Fungi Candida
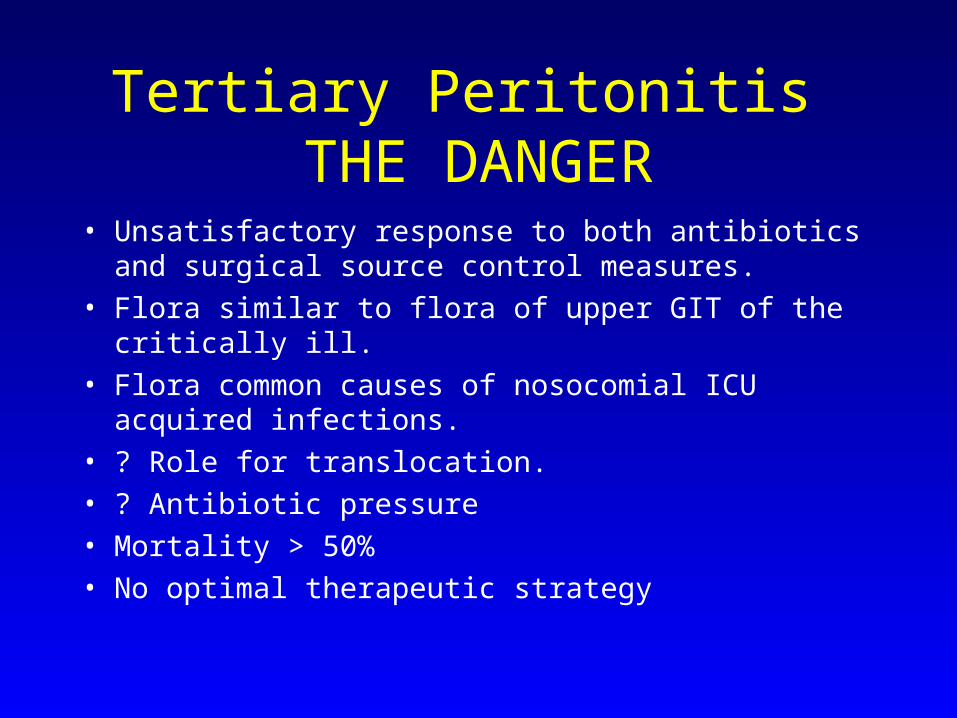
Tertiary Peritonitis THE DANGER
• Unsatisfactory response to both antibiotics and surgical source control measures.
• Flora similar to flora of upper GIT of the critically ill.• Flora common causes of nosocomial ICU acquired
infections.• ? Role for translocation.• ? Antibiotic pressure• Mortality > 50%• No optimal therapeutic strategy

The Microbiology of Tertiary Peritonitis
• Most surgeons do not dare to leave these patients without antibiotics before the decision to reoperate
• These “interval” antibiotics may have a major impact on the microbiology and the efficacy of subsequent treatment. (Although many other factors contribute to survival)
• The microbiology of postoperative peritonitis differs significantly from that of community-acquired disease, and specific antibiotic therapy is required, DESPITE the doubtful impact on survival.
• The treatment of CAIAI by 3rd generation cephalosporins and metronidazole is not adequate for tertiary peritonitis because –
gm(+) bacteria are not covered gm(+) bacteria outnumber gm(-) bacteria Enterobacter which is most threatening, is also not sufficiently covered.
Roehrborn A, CID 2001

Intra-abdominal InfectionDIAGNOSIS
• Difficult in the critically ill.• History unobtainable.• Level of conciousness masks physical examination.• Important : Clinical setting
Unexplained signs of sepsis
Unexplained organ dysfunction
Radiographic studies – the whole range.
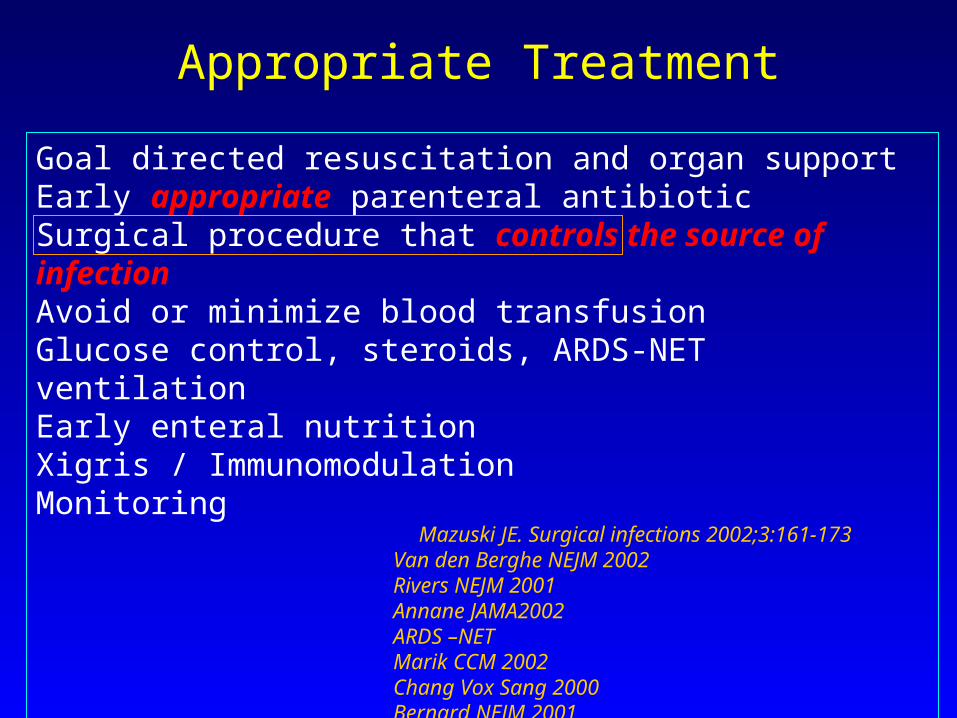
Goal directed resuscitation and organ supportEarly appropriate parenteral antibioticSurgical procedure that controls the source of infection Avoid or minimize blood transfusionGlucose control, steroids, ARDS-NET ventilationEarly enteral nutritionXigris / ImmunomodulationMonitoring
Mazuski JE. Surgical infections 2002;3:161-173 Van den Berghe NEJM 2002 Rivers NEJM 2001 Annane JAMA2002 ARDS –NET Marik CCM 2002 Chang Vox Sang 2000 Bernard NEJM 2001
Appropriate Treatment
Appropriate Treatment
Source Control
• Drainage (open vs percutaneous)• Debridement (early vs. delayed)• Diversion of bowel content.• Restore intestinal continuity.• Open abdomen techniques.• Intra-abdominal pressures.• Planned relaparotomy. Marshall JC, CCM 2003; 31:8:2228
Appropriate TreatmentSelecting an Antibiotic Regimen
• Consider patient – specific toxicity.• Cost.• Local microbiological surveillance for resistance patterns• ? Duration of treatment Adequate source control – adjuvant treatment for 5 - 7 days.• ? Role of anti-enterococcal therapy • ? Role of antifungal therapy• ? Role of antibiotic therapy in tertiary peritonitis – does it contribute. Resistance to common empiric regimens. Narrow spectrum agents according to MCS Avoid anti-anaerobic activity.
Bartlett JG. Med Clin North Am. 1995;79:599-617
Principles of Antibiotic Therapy
Initiated as soon as the diagnosis established and surgery planned– Early administration– Parenteral route
• AB must differ from antibiotic prophylaxis used in the unit Mazuski Surgical infections 2003
AB must target Enterobacteriaceae and anaerobes directly responsible for the immediate prognosis and development of abscesses
AB should also target β- lactam susceptible gram pos cocciSolomkin IDSA Guidelines CID 2003

Considerations in determining appropriate therapy:
Raymond DP et al. Surg Infect 2002
Kollef MH. Clin Infect Dis 2000;31(Suppl 4)
Defining Appropriate Therapy
• Site of perforation
• Dose and dosing frequency( PK/PD)
• Prior antibiotic treatment
• Nosocomial / Health Care Associated / Community Acquired.
• Prevalent pathogens (ESBL, acinetobacter)
• Severity
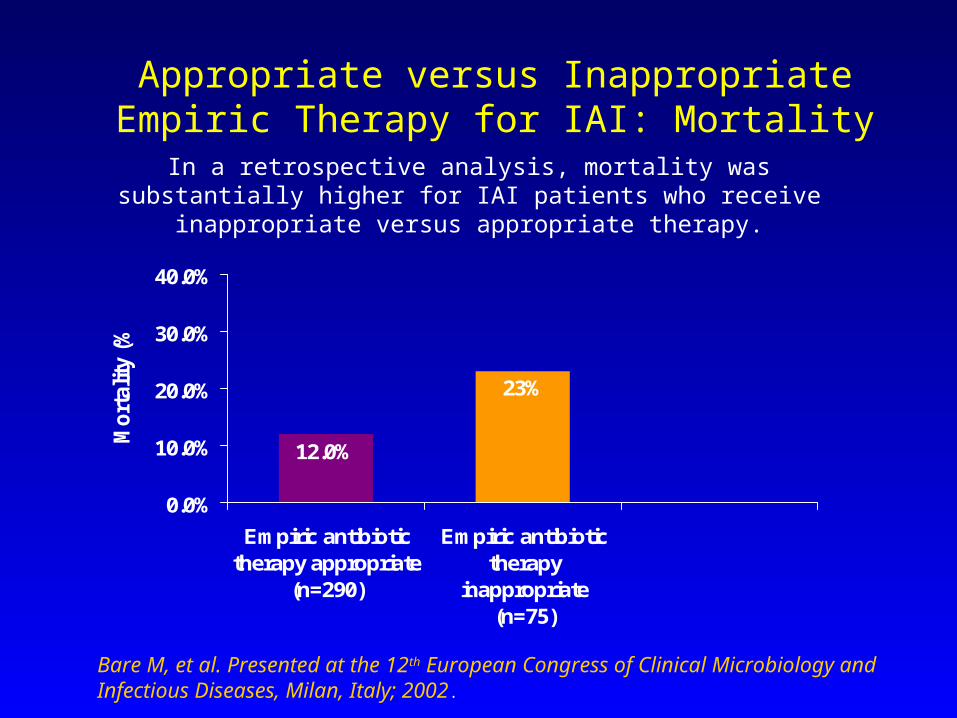
Appropriate versus Inappropriate Empiric Therapy for IAI: Mortality
In a retrospective analysis, mortality was substantially higher for IAI patients who receive inappropriate versus appropriate therapy.
Bare M, et al. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases, Milan, Italy; 2002.
12.0%
23%
0.0%
10.0%
20.0%
30.0%
40.0%
Empiric antibiotictherapy appropriate
(n=290)
Empiric antibiotictherapy
inappropriate(n=75)
Mo
rtal
ity
(%)
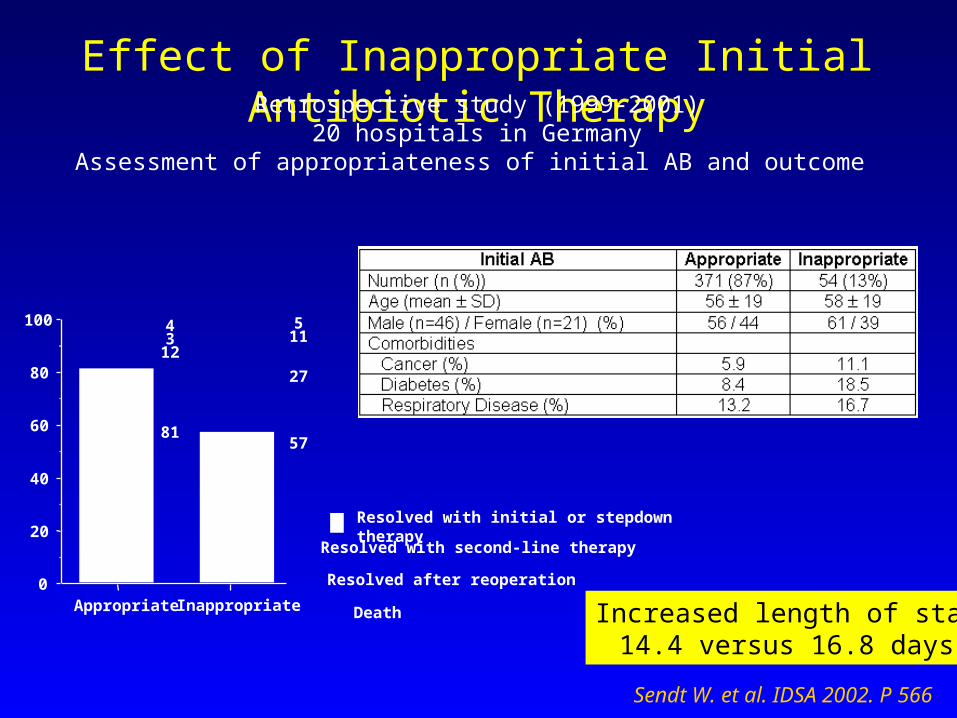
Effect of Inappropriate Initial Antibiotic TherapyRetrospective study (1999-2001)
20 hospitals in GermanyAssessment of appropriateness of initial AB and outcome
Sendt W. et al. IDSA 2002. P 566
Death
Resolved after reoperation
Resolved with second-line therapy
Resolved with initial or stepdown therapy
0
20
40
60
80
100
Appropriate Inappropriate
43
12
81
511
27
57
Increased length of stay14.4 versus 16.8 days

Davey P, et al. Presented at the International Society of Pharmacoeconomics and Outcomes Research Sixth Annual International Meeting; May, 2001.
Appropriately treated IAI patients incurred significantly lower hospitalization costs versus inappropriately treated patients
348 patients from three Scottish hospitals from 1993 to 1997
Appropriate Versus Inappropriate Therapy: Cost of Hospital Stay
£4,190
£7,705
£2,862
£4,770
£0
£2,000
£4,000
£6,000
£8,000
Appropriate EmpiricAntibiotic (n=129)
Inappropriate EmpiricAntibiotic (n=33)
Hos
pita
l Cos
t (P
ound
s S
terl
ing)
Mean
Median

Kollef MH, et al. Chest. 1999;115:462.
• Prospective cohort study by Kollef et al• 2000 patients admitted over an 8-month period to a
19-bed medical ICU and an 18-bed surgical ICU• Study aim: to determine if inadequate empiric
antibiotic therapy is a risk factor for mortality• Sponsors: CDC, Bayer
Inadequate Antimicrobial Treatment: Effect on Mortality
Definitions
• Inadequate antibiotic therapy was defined at the time culture and susceptibility reports became available
• Absence of antimicrobial agents directed at a specific type of organism (eg, absence of antifungal agents for Candidemia)
• Administration of an antibiotic to which the organism was resistant (eg, use of ceftazidime for Klebsiella with ceftazidime MIC >256)

Impact of Inadequate Empiric Choice
Multivariate analysis – inadequate antibiotic treatment was the most important independent risk factor for death
Kollef MH, et al. Chest. 1999;115:462.
Antimicrobial Treatment Mortality
Inadequate 52%
Adequate 12%
RR 4.3 (95% CI, 3.5 to 5.2; p <0.001)
More Evidence
• At least 5 other studies have shown comparable findings
• Delays in receipt of appropriate therapy have also been associated with excess hospital mortality
• These concepts have been incorporated into the official statement of ATS and IDSA on management of hospital-acquired pneumonia (Am J Respir Crit Care Med. 2005;171:388)

Why do we get empiric therapy wrong?
The most frequent reason is resistance to the antibiotic chosen


Recent Publications confirm resistance linked to overuse of traditional antibiotics
“…Neither third-generation cephalosporins nor quinolones appear suitable for sustained use in hospitals as “workhorse” antibiotic therapy….”
What is “collateral damage”?
• Adverse effects of antibiotics on ecology of normal flora of gut or skin
• Selection of drug-resistant organisms• Unwanted colonization or infection with MDR’s• Third generation cephalosporins and quinolones are
the most frequently implicated (VRE, C difficile, ESBL K pneumoniae, beta-lactam resistant Acinetobacter spp)
• Quinolones (MRSA, resistant Ps aeruginosa
Neither 3rd generation cephalosporins nor quinolones appear suitable as “workhorse” antibiotics in hospitals.

How do we get resistant organisms in a hospital?
HorizontalTransfer
Via hands
Transfer of Patient from
Anotherfacility
ResistantOrganismsSelected Byantibiotics
Transfer of Resistance
Genes
The Growing Resistance Problem
The Growing Resistance ProblemMechanisms of resistance
• Altered balance of accumulation (impermeability and efflux)
Loss of porin protein channels in outer membrane (All AB’s except aminoglycocides)
Acquired efflux pumps to eject antibiotics (may be broad or narrow spectrum)
• Enzymic inactivationBeta-lactamases (pen, ceph, carba)Aminoglycocide modifying enzymes
• Alteration of targetPenicillin-binding proteins (beta-lactams)Ribosomal methylation (Macrolides)DNA gyrase mutation (Floroquinolones)
The Growing Resistance Problem• Well documented and increasing• Restrict treatment options• Result in clinical failures• Some encoded by chromosomally located genes –
limiting potential for spread to other bacteria• Some encoded by plasmids and transposons –
facilitating spread to other bacterial species • Induction – a reversible regulatory process due to an
inducer initiating eg enzyme synthesis (AmpC beta lactamase in Enterobacter spp)
• Selection – an irreversible process – individuals within a mixed population (eg spontaneous mutants producing the same AmpC beta lactamase) increase
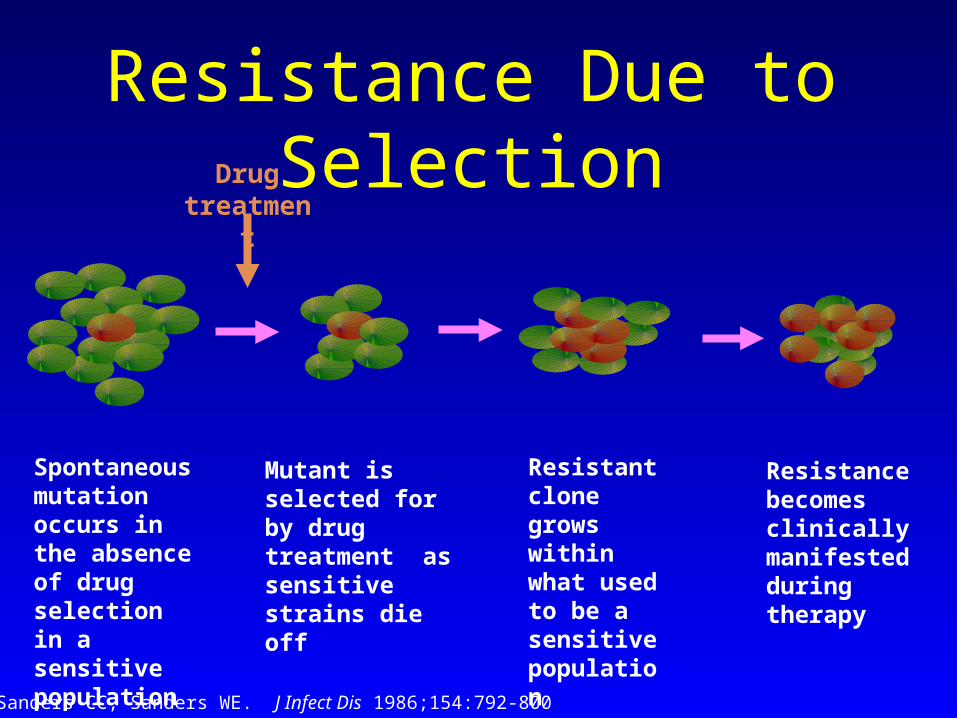
Resistance Due to Selection
Spontaneous mutation occurs in the absence of drug selection in a sensitive population
Drug treatment
Sanders CC, Sanders WE. J Infect Dis 1986;154:792-800
Mutant is selected for by drug treatment as sensitive strains die off
Resistance becomes clinically manifested during therapy
Resistant clone grows within what used to be a sensitive population
ESBLs
• Extended• Spectrum• Beta-• Lactamases
ESBLs
• First described in Klebsiella• 10-30% of most enteric Gram negative bacilli are now
ESBL producers • Leads to resistance to third generation
cephalosporins plus many other classes• Biggest risk factor is third generation cephalosporin
use
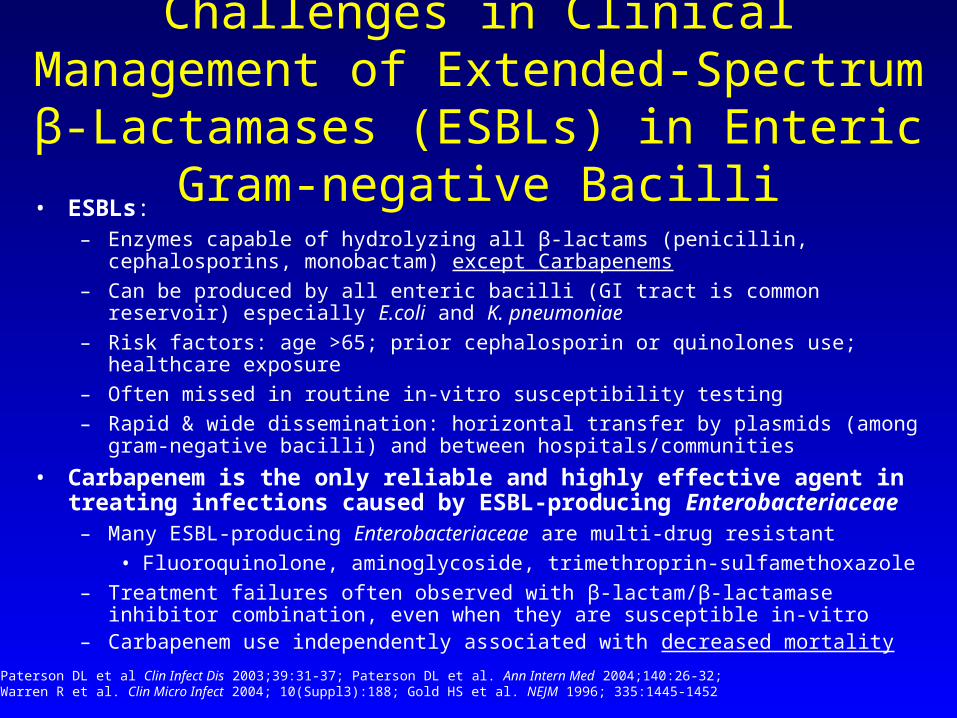
Challenges in Clinical Management of Extended-Spectrum β-Lactamases (ESBLs)
in Enteric Gram-negative Bacilli• ESBLs:
– Enzymes capable of hydrolyzing all β-lactams (penicillin, cephalosporins, monobactam) except Carbapenems
– Can be produced by all enteric bacilli (GI tract is common reservoir) especially E.coli and K. pneumoniae
– Risk factors: age >65; prior cephalosporin or quinolones use; healthcare exposure
– Often missed in routine in-vitro susceptibility testing
– Rapid & wide dissemination: horizontal transfer by plasmids (among gram-negative bacilli) and between hospitals/communities
• Carbapenem is the only reliable and highly effective agent in treating infections caused by ESBL-producing Enterobacteriaceae
– Many ESBL-producing Enterobacteriaceae are multi-drug resistant
• Fluoroquinolone, aminoglycoside, trimethroprin-sulfamethoxazole
– Treatment failures often observed with β-lactam/β-lactamase inhibitor combination, even when they are susceptible in-vitro
– Carbapenem use independently associated with decreased mortality
Paterson DL et al Clin Infect Dis 2003;39:31-37; Paterson DL et al. Ann Intern Med 2004;140:26-32;Warren R et al. Clin Micro Infect 2004; 10(Suppl3):188; Gold HS et al. NEJM 1996; 335:1445-1452
Patient Selection
Contamination vs. infection may often be a gray area
For example where there is:• Extensive contamination shortly pre-op• Infection of an abdominal viscus removable by surgery
Antibiotics can be given for 24 hrs or less in traumatic perforations with early operation
Fabian Surgery1992
Bozorgzadeh Am J Surg 1999 Kirton J Trauma 2000
This should be similar with iatrogenic perforation and alsopossibly with early repair of gastro duodenal perforation
Schein Br J Surg 1994

Consensus is that treatment is necessary for• Colonic perforation > 12hrs• Gastro duodenal > 24hrs• Similarly Class 2 evidence that antibiotics are
necessary for 24hrs or less for acute or gangrenous appendicitis and cholecystitis without perforation or infected peritoneal fluid
Andaker Acta Chir Scand !987 Schein Br J Surg 1994
Patient Selection

Duration of Therapy
5-7 days has been the recommended duration Bohnen Arch Surg 1992
Protocol directed therapy i.e.2 days for limited infection 5 days for extensive infectionHave been as successful as historical controls Andaker Acta Chir Scand !987
Schein Br J Surg 1994
Therapy directed to clinical response is successful and limits duration Lennard Ann Surg 1982 Smith J hosp Infect 1985 Taylor Am Surg 2000
Persistence of signs of sepsis indicates a need for surgical intervention, not prolonged antibiotics
Lennard Ann Surg 1982 Lennard Arch Surg 1980
There is limited data that prolonged courses might work where source control cannot be achieved Visser Eur J Surg 1998
High cost in terms of resistance
Duration of Therapy

Antibiotic RegimensMild to moderate community acquired infectionamoxicillin / clavulanate cefuroxime; ceftriaxone; cefotaxime / metronidazoleSevere community acquired infections or nosocomial
sepsisamoxicillin / clavulanate ± aminoglycoside piperacillin / tazobactamcarbapenemscefepime + metronidazolecipro -levofloxacin + metronidazoleaminoglycoside +metronidazole or clindamycin

• There is little guidance in the literature on which regimen is superior
• Antimicrobials have been designed to test equivalence and most patients entered into studies have had non-severe community acquired infections
• Since most regimens appear to be equivalent, cost considerations, toxicity and likely organism are more important considerations
Antibiotic Regimens
Solomkin CID 2003Mazuski Surgical Infections 2002

• The expanded gram negative spectrum of some agents confers no advantage in CAIAI and may contribute to increased resistance
• Agents routinely used to treat nosocomial sepsis in the ICU should not be used for CAIAI
Antibiotic Regimens
Solomkin CID 2003Mazuski Surgical Infections 2002Shlaes CID 1997McGowan New Horiz 1996

Enterococci: controversial
Treatment failure due to enterococci seems more common in a higher risk group :age APACHE, non appendiceal sepsis, post operative or nosocomial infection Mazuski Surgical Infection 2002 Sitges-Serra Br J Surg 2002 Linden Curr Infect Dis Rep 2003
Routine coverage for enterococci is not necessary for CAIAI. They should be treated when cultured from patients in health care settings Solomkin CID 2003
Antibiotic Therapy

Monotherapy with a Broad-Spectrum Beta-Lactam Is as Effective as It’s Combination with an Aminoglycoside in Treatment of
severe Generalized Peritonitis: a Multicenter Randomized Controlled Trial.
H. DUPONT, C. CARBON, and J. CARLET for THE SEVERE GENERALIZED PERITONITIS STUDY GROUP.
Antimicrobial Agents and Chemotherapy, Aug. 2000,
p. 2028-2033.

Aminoglycosides in Peritonitis1. The 1980s - ? Synergism - lack of broad spectrum beta-lactams2. Recent literature reviews – no clear evidence to support the
use of aminoglycosides for the treatment of peritonitis.
• Aminoglycoside activity is reduced by intra-abdominal acidosis and hypoxia, and the presence of drug binding purulent debris.
• Despite the marked post-antibiotic effect on gm(-) bacilli, no study has proven this for intra-abdominal infection.
• Doubt about synergism with beta-lactams – the emergence of resistant strains such as Ps aeruginosa is not prevented.
• Increased incidence of nephrotoxicity.

0
2
4
6
8
10
12
14
Per
cent
Res
ista
nce
3rd generation cephalosporin-resistant Klebsiella pneumoniae
0
5
10
15
20
25
30
Per
cent
Res
ista
nce
Fluoroquinolone-resistant Pseudomonas aeruginosa
Non-Intensive Care Unit Patients
Intensive Care Unit Patients
Increasing Antimicrobial Resistance among Pathogens Causing Hospital-
Onset Infections
Source: National Nosocomial Infections Surveillance (NNIS) System
12 Steps to Prevent Antimicrobial Resistance: Hospitalized Adults
Open Management of the Abdomen and Planned Reoperations in Severe
Bacterial Peritonitis.• Despite this approach, mortality continues to be high,
(42% in hospital)• Both short and long term morbidity are appreciable.
(particularly the number of abdominal wall defects)• Value of this technique rests on the fact that other
conventional surgical methods often fail to control severe bacterial peritonitis.


Antibiotics and Pancreatic Necrosis
• Death from acute severe pancreatitis results from infection and MODS late in the course of illness.
• Necrotising pancreatitis involving at least one third of the organ, are at highest risk of secondary infection and death.
• Based on recent studies, early antibiotic prophylaxis in patients with necrotising pancreatitis has been suggested and most practitioners use imipenem for this task.????????????
“There is general agreement that the development and extent of
pancreatic necrosis are the most important indicators of disease
severity” Necrosis correlates with length of
hospitalisation, development of complications, numeric systems
and death.
Challenges of caring for the patient with Challenges of caring for the patient with severe pancreatitis in the critical care severe pancreatitis in the critical care environment.environment.• Timing / indications for admission and monitoring in theTiming / indications for admission and monitoring in the Intensive Care or High Care Unit. Intensive Care or High Care Unit.• Should patients with SAP receive prophylactic antibiotics?Should patients with SAP receive prophylactic antibiotics?• The role of nutritional support in the management ofThe role of nutritional support in the management of patients with SAP. patients with SAP.• What is the role of surgery in the management of patientsWhat is the role of surgery in the management of patients with SAP with SAP
- indications- indications- optimal timing- optimal timing- less invasive approaches - less invasive approaches
•Interventions for gallstone pancreatitisInterventions for gallstone pancreatitis•Targeting the inflammatory response in patients with SAPTargeting the inflammatory response in patients with SAP Nathens: CCM 32 (12) 2004Nathens: CCM 32 (12) 2004

Infected Necrosis• Definitions of pancreatic infections:
Pancreatic infection Infected necrosis Pancreatic abscess Infected pancreatic pseudocyst
• The incidence of infection correlates with the presence of intra- and extrapancreatic necrosis
• General infection rate of pancreatic tissue 7-12%
• 80% of deaths from acute pancreatitis due to septic complications
Diagnosis of infective necrosis
• Difficult to distinguish sterile from infected necrosis
• Distinction is important, infected necrosis without intervention - 100% mortality
• CT-guided FNA - sensitivity 90%
- specificity 99%
continue ...
Diagnosis of infective necrosis
• FNA is recommended for patients with acute necrotizing pancreatitis who’s clinical condition:
Deteriorate
Fail to improve despite progressive supportive care
• Surveillance aspiration should be repeated when clinically indicated

MILD APIntestinal Edematous pancreatitis
Daily CRP
US Biliary lithiasis
Impacted stone EPT
After AP
Laparoscopic CCE
SEVERE APNecrotizing Pancreatitis
ICU treatment + antibiotic prophylaxisDaily CRP, IL-8, procalcitonin, Apache II scoring
Increasing severity cCT
Clinical sepsis
FNA
Negative
Sterile necrosis
Nonsurgical managementResponders
Definitive Conservative
treatment
Non responders
to ICU
Clinical sepsis:
SurgeryNecrosectomy + closed
Lavage / open packing
Positive
Infected necrosis
Surgical management
Ulm Protocol for treatment of AP-amylase
pancreatic lipase
CRP, LDH

QUESTION 2: SHOULD PATIENTS WITH SEVERE ACUTE PANCREATITIS RECEIVE
PROPHYLACTIC ANTIBIOTICS?
Recommendations:
1. Do not administer prophylactic systemic antibacterial or antifungal agents routinely for patients with
necrotising pancreatitis. 2. Routine selective decontamination of the gut should not
be used for necrotising pancreatitis.
3. SDD is promising and further study is warranted in SAP.

How can we get AB Rx right?• The problem -- How to ensure adequate (early
appropriate) yet not excessive use of antimicrobials. -- …a liberal protective approach vs
restrictive antibiotic control…• High risk patients demand liberal empiric use of
broad-spectrum antimicrobials to reduce the risk of morbidity and mortality due to nosocomial infections.
• The use and abuse of broad-spectrum agents, prescribed to treat the critically ill, dramatically increases the prevalence of MDR pathogens.
MRSA
VREESBL producers - Ps aeruginosa, Acinetobacter, Klebsiella,
EnterobacterCandida
How can we get ABRx right?
STRATEGISE!!!
• Close examination of a unit specific antibiogram to help devise empiric regimens with the greatest likelihood of covering the organisms posing the greatest risk.
• Computer-assisted antimicrobial decision-support systems to:
Improve antimicrobial selectionTo control costsTo decrease emergence of resistance
A patient specific antibiogram.
How can we get ABRx right?
STRATEGISE!!!
• CPIS as an objective measure to guide antimicrobial
therapy in patients with pulmonary infiltrates.• Invasive management or diagnostic strategy based
on bronchoscopic sampling.

Ertapenem
• The third commercially available carbapenem• Activity similar to imipenem or meropenem except
lacks activity against:
Pseudomonas aeruginosa
Acinetobacter
Enterococci
Stenotrophomonas.• Highly active against ESBL producing organisms• Conventional dose is 1 gram q 24 hr IV
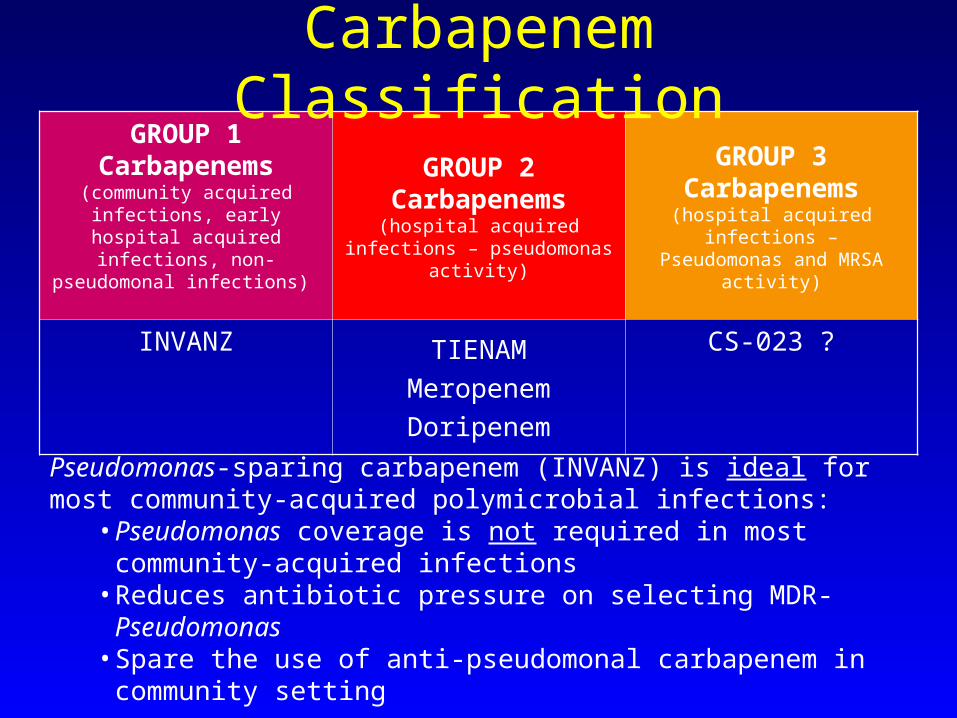
GROUP 1Carbapenems
(community acquired infections, early hospital acquired
infections, non- pseudomonal infections)
GROUP 2Carbapenems
(hospital acquired infections – pseudomonas activity)
GROUP 3Carbapenems
(hospital acquired infections –Pseudomonas and MRSA
activity)
INVANZ TIENAM
Meropenem
Doripenem
CS-023 ?
Pseudomonas-sparing carbapenem (INVANZ) is ideal for most community-acquired polymicrobial infections:
• Pseudomonas coverage is not required in most community-acquired infections
• Reduces antibiotic pressure on selecting MDR-Pseudomonas • Spare the use of anti-pseudomonal carbapenem in community
setting
Carbapenem Classification
ErtapenemActivity excellent against Enterobacteriaceae and other
fermenters, anaerobes and β- lactam susceptible enterococci Livermore JAC 2003
Solomkin Ann Surg 2003
633 patients :moderate to ? severe peritonitis
50% complicated appendicitis randomized to receive ertapenem 1g dly vs. tazocin 3.375g 6hrly
This showed equivalence -favourable responses were seen in 19/26(vs.23/26) patients in whom pseudomonas was cultured and in 50/56(vs24/37) in whom enterococci were cultured

Ertapenem 1 g once a day (n=203)
Piperacillin/Tazobactam 3.375 g every 6 hours (n=193)
Success rate was defined as clinical and microbiologic resolution of the index infection requiring no additional antimicrobial therapy.
100
80
60
40
20
0
Su
cces
s ra
te, %
92%88% 87%
81%
End of IV Therapy(approximately 8 days)
Final Assessment(test of cure, primary endpoint; 4–6 weeks
post-therapy)
Data computed from statistical model adjusted for strata.
Ertapenem vs. Piperacillin/Tazobactam: Over 90% Success Rate at End of IV
Therapy
Solomkin JS et al. Ann Surg 2003;237:235-245.
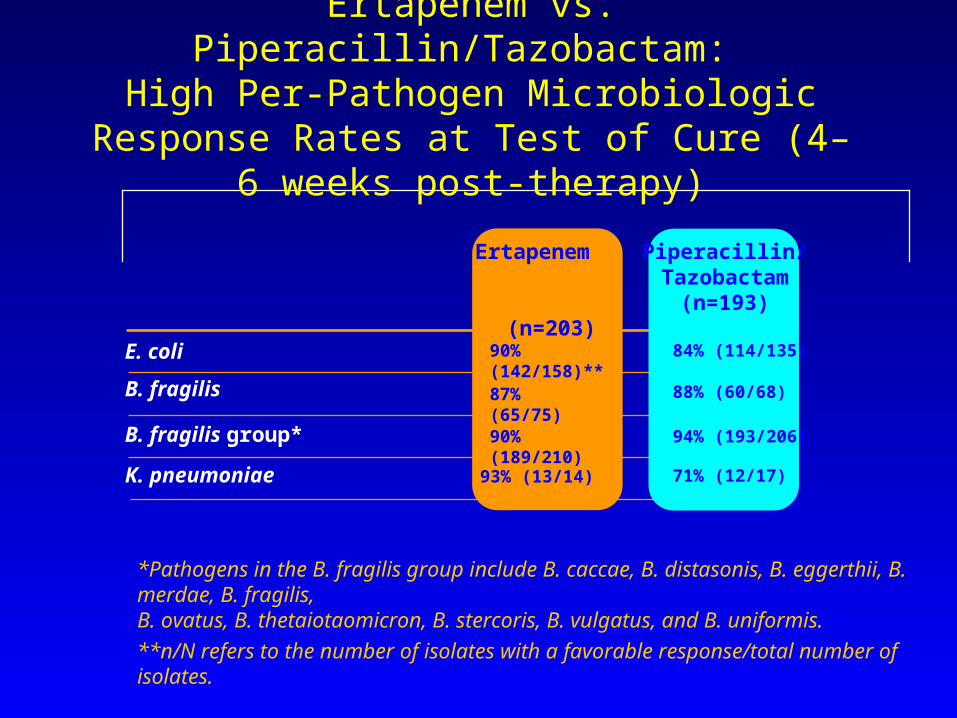
*Pathogens in the B. fragilis group include B. caccae, B. distasonis, B. eggerthii, B. merdae, B. fragilis, B. ovatus, B. thetaiotaomicron, B. stercoris, B. vulgatus, and B. uniformis.
**n/N refers to the number of isolates with a favorable response/total number of isolates.
Ertapenem vs. Piperacillin/Tazobactam: High Per-Pathogen Microbiologic Response
Rates at Test of Cure (4–6 weeks post-therapy)
K. pneumoniae
90% (189/210)B. fragilis group*
90% (142/158)**E. coli
B. fragilis
Ertapenem
(n=203)
87% (65/75)
71% (12/17)
94% (193/206)
84% (114/135)
Piperacillin/Tazobactam
(n=193)
88% (60/68)
93% (13/14)
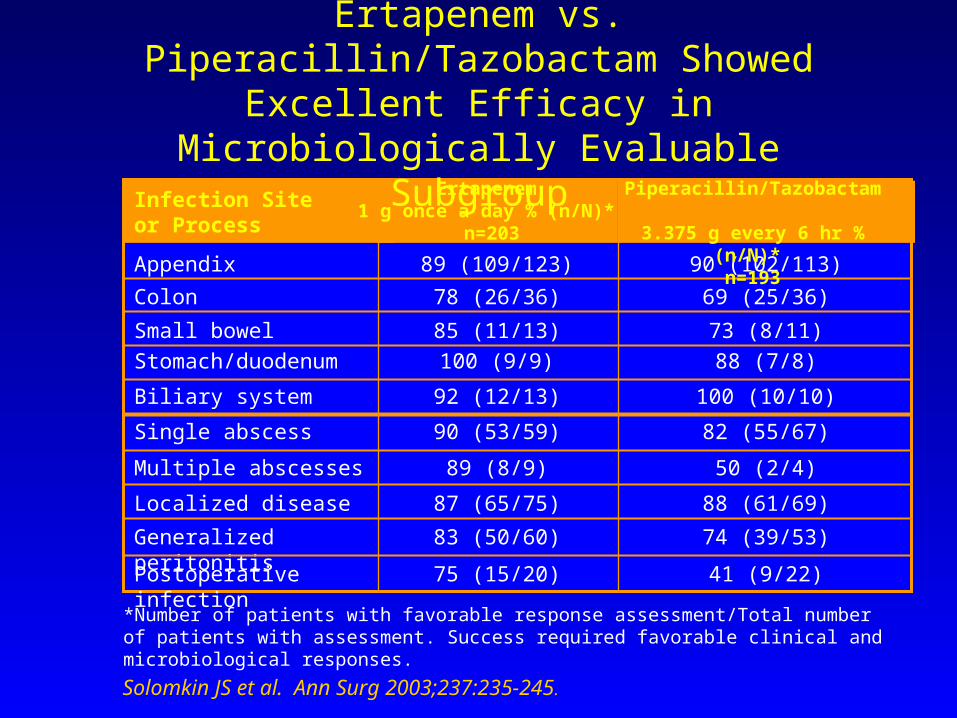
41 (9/22)75 (15/20)Postoperative infection
74 (39/53)83 (50/60)Generalized peritonitis
88 (61/69)87 (65/75)Localized disease
50 (2/4)89 (8/9)Multiple abscesses
82 (55/67)90 (53/59)Single abscess
100 (10/10)92 (12/13)Biliary system
88 (7/8)100 (9/9)Stomach/duodenum
73 (8/11)85 (11/13)Small bowel
69 (25/36)78 (26/36)Colon
90 (102/113)89 (109/123)Appendix
Infection Site or Process
*Number of patients with favorable response assessment/Total number of patients with assessment. Success required favorable clinical and microbiological responses.
Ertapenem vs. Piperacillin/Tazobactam Showed Excellent Efficacy in Microbiologically Evaluable
Subgroup
Solomkin JS et al. Ann Surg 2003;237:235-245.
Ertapenem 1 g once a day % (n/N)*
n=203
Piperacillin/Tazobactam 3.375 g every 6 hr % (n/N)*
n=193
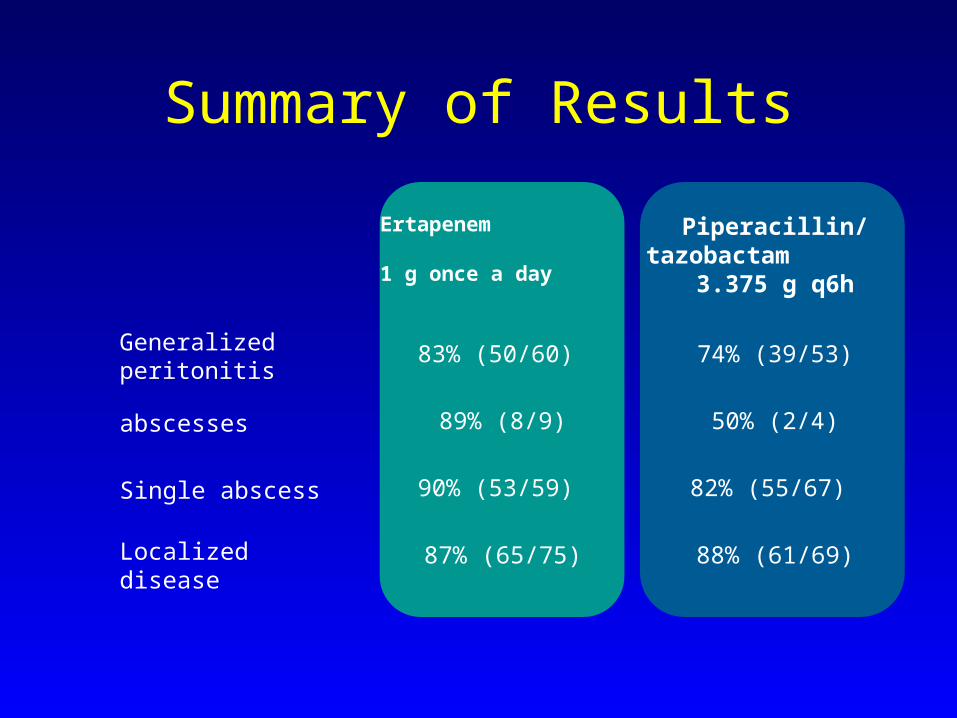
Summary of Results
88% (61/69)87% (65/75)Localized disease
82% (55/67) 90% (53/59) Single abscess
50% (2/4)89% (8/9)abscesses
74% (39/53)83% (50/60) Generalized peritonitis
Piperacillin/ tazobactam
3.375 g q6h
Ertapenem 1 g once a day
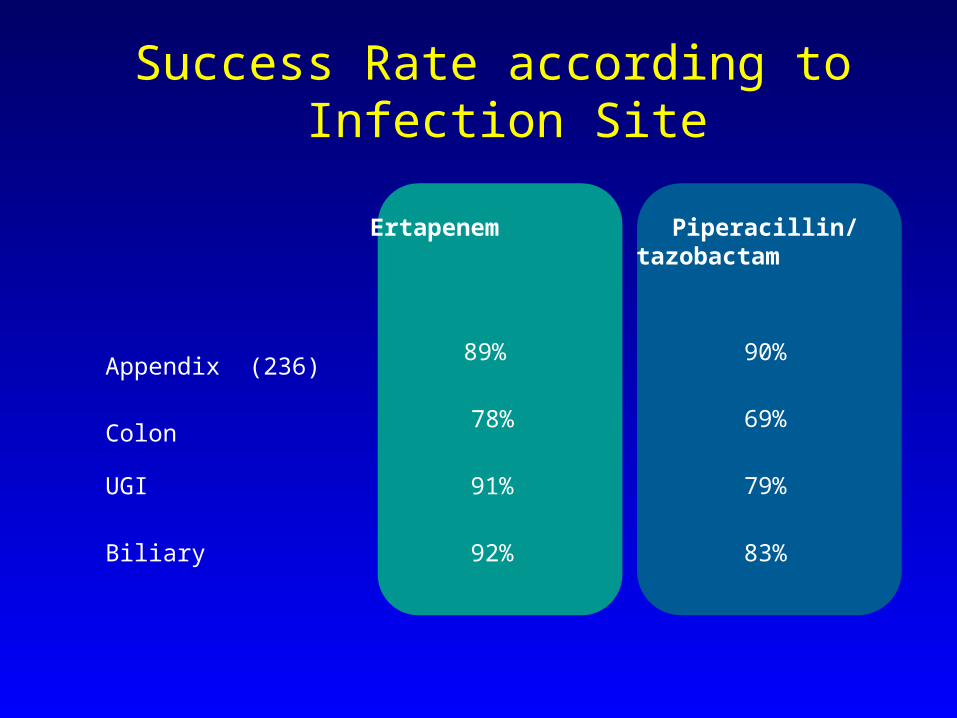
Success Rate according to Infection Site
83%92%Biliary
79%91%UGI
69%78%Colon
90%89% Appendix (236)
Piperacillin/tazobactam
Ertapenem
Yellin AAC 2002
Ertapenem 1g and 1.5g/day(51) vs. ceftriaxone 2g daily and metronidazole 500mg 8 hrly (59) followed by switch to cipro and metronidazole after 3 days of IVI therapy for complicated IAI
• 1g group 84% vs. 85% had favourable clinical and microbial responses
• 1.5g group 83%vs77%• Well tolerated ,safe
Ertapenem

0
20
40
60
80
100
Su
ccess r
ate
, %
Clinical and Microbiological Success (4–6 weeks post-therapy)
84% 85%
Yellin AE et al. Int J Antimicrob Agents 2002; 20:165-173.
Ertapenem vs. Ceftriaxone plus Metronidazole:
High Microbiological and Clinical Success
Rates at Test of Cure Ertapenem 1 g once a day (n=31)
Ceftriaxone 2 g daily plus metronidazole500 mg every 8 hours (n=41)
Success rate was defined as clinical and microbiologic resolution of the index infection requiring no additional antimicrobial therapy.
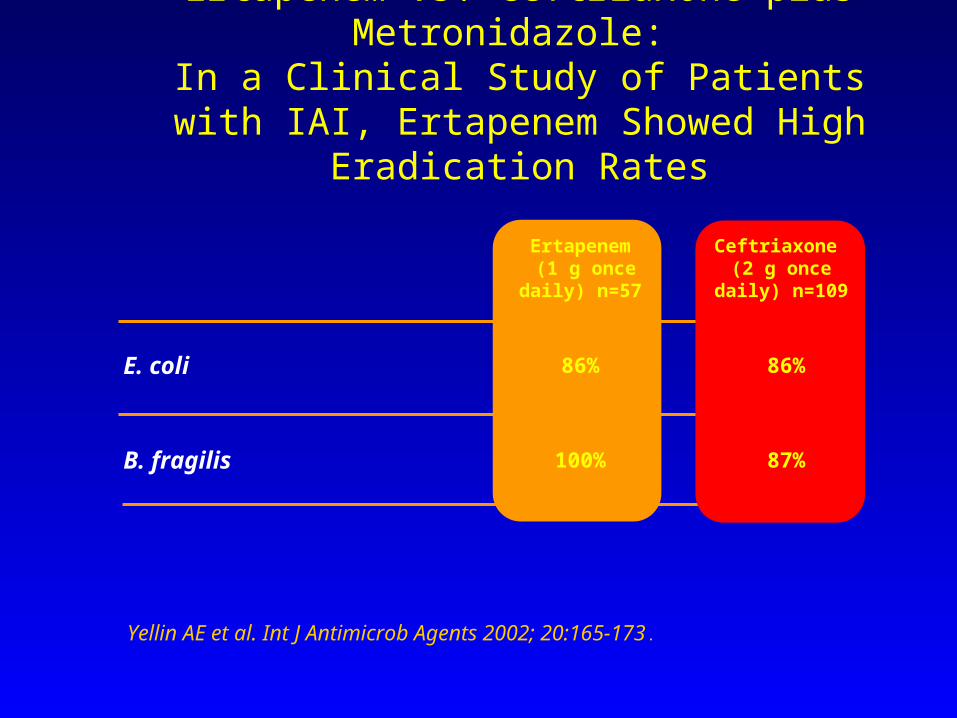
87%100%B. fragilis
86%86%E. coli
Ceftriaxone (2 g once daily)
n=109
Ertapenem (1 g once daily)
n=57
Yellin AE et al. Int J Antimicrob Agents 2002; 20:165-173.
Ertapenem vs. Ceftriaxone plus Metronidazole:
In a Clinical Study of Patients with IAI, Ertapenem Showed High Eradication Rates
Yellin AE et al. Int J Antimicrob Agents 2002; 20:165-173.
Ertapenem vs. Ceftriaxone plus Metronidazole:
Conclusions
In patients with IAI:• Ertapenem, one gram, one dose, once a day, was
effective compared with 2 g of ceftriaxone administered once daily plus 500 mg metronidazole administered in three divided daily doses.
• The tolerability of ertapenem was comparable to ceftriaxone plus metronidazole.

2 Friedland I et al. 3rd ACCP, San Margherita, Italy, October 16-19, 2003 (Poster #57)
1 Friedland I et al. 13th ECCMID, Glasgow, UK, May 10-13, 2003
0
5
1015
20
25
30
Ertapenem1,2 Piperacillin/tazo1 Ceftriaxone/Met2
per
cen
t
Baseline End of therapy End of therapy and/or test of cure
% R % R % ESBL % R % ESBL% ESBL
• 2 separate OASIS trials confirmed that Ertapenem:– Reduced ESBL-producing organisms during therapy– Had minimal or no risk of resistance development during therapy
• Stable against ESBLs; thus minimal selection for resistant Enterobacteriaceae
• Is Pseudomonas-sparing; thus minimal selective pressure on MDR-Pseudomonas
• Once daily administration and the absence of activity against Pseudomonas and Acinetobacter could mean a greater role in community acquired infections; however is the extended gram (-) spectrum necessary?
• Should it be reserved for hospital acquired ESBL infections exclusively, allowing a reduction in usage of other carbapenems, reserving these agents for Acinetobacter and Pseudomonas ?
• Should the necessity for appropriate initial therapy lead us to utilize ertapenem and de-escalation in community acquired infections.
Ertapenem

“…The prevalence of extended-spectrum -lactamase (ESBL) production by Klebsiella pneumonia approaches 50% in some countries in eastern Europe and Latin America…”
“Use of carbapenem (primarily imipenem) was associated with a significantly lower 14-day mortality than was use of other antibiotics active in vitro.”
Recent Publications confirm role of carbapenems in treating ESBL infections


Are we wasting antipseudomonal therapy?
• UTI – quinolones• CAP – quinolones• Aspiration – piperacillin/tazobactam• Cellulitis – quinolones, piperacillin/tazobactam• Intra-abdominal infections – pip./tazobactam


Figure. Fluoroquinolone Use and Resistance Rates in Pseudomonas aeruginosa and Gram-Negative Bacilli
National fluoroquinolone use data were obtained from IMS HEALTH Retail and Provider Perspective (Plymouth Meeting, Pa). The increasing rates of ciprofloxacin resistance correlate with the steadily increasing fluoroquinolone use (r = 0.976, P<.001 for P aeruginosa; r = 0.891, P = .007 for gram-negative bacilli; r = 0.958, P<.001 for years of observation). The 1990-1993 data points represent composite susceptibility3 and fluoroquinolone use for those 4 years.
New antipseudomonal drugs available in the next 5 years
Pittsburgh protocol
• ICUs – antipseudomonal agents unrestricted (except quinolones)
• Outside of ICUs – all antipseudomonal drugs need prior approval
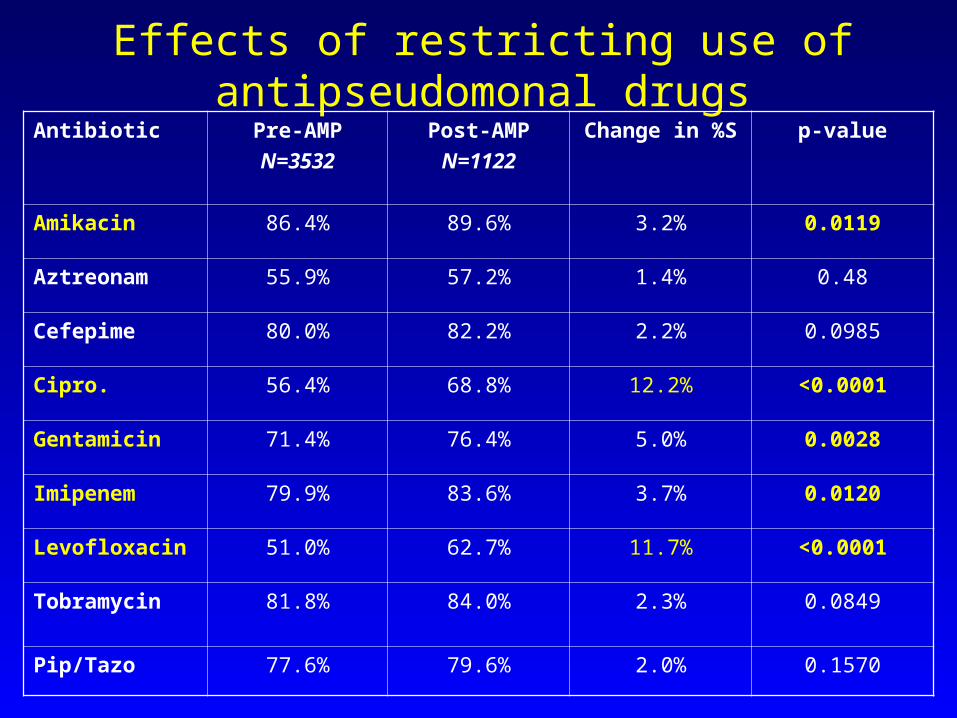
Effects of restricting use of antipseudomonal drugs
Antibiotic Pre-AMP
N=3532
Post-AMP
N=1122
Change in %S p-value
Amikacin 86.4% 89.6% 3.2% 0.0119
Aztreonam 55.9% 57.2% 1.4% 0.48
Cefepime 80.0% 82.2% 2.2% 0.0985
Cipro. 56.4% 68.8% 12.2% <0.0001
Gentamicin 71.4% 76.4% 5.0% 0.0028
Imipenem 79.9% 83.6% 3.7% 0.0120
Levofloxacin 51.0% 62.7% 11.7% <0.0001
Tobramycin 81.8% 84.0% 2.3% 0.0849
Pip/Tazo 77.6% 79.6% 2.0% 0.1570
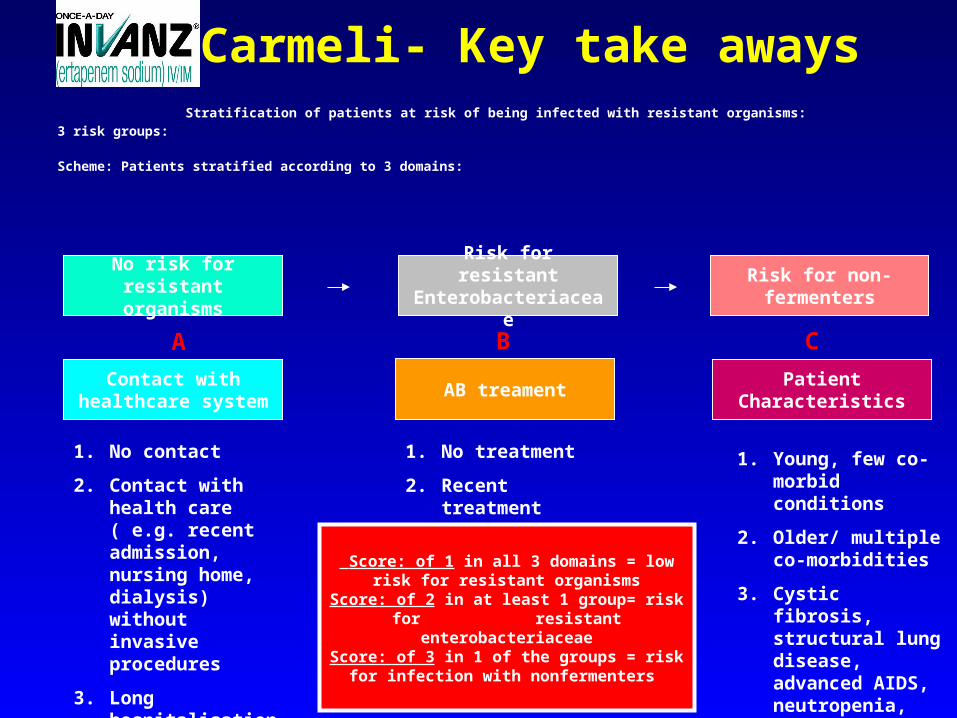
Carmeli- Key take aways Stratification of patients at risk of being infected with resistant organisms:
3 risk groups:
Scheme: Patients stratified according to 3 domains:
No risk for resistant organisms
Risk for resistant Enterobacteriaceae
Risk for non-fermenters
Patient Characteristics
AB treamentContact with
healthcare system
A B C
1. No contact
2. Contact with health care ( e.g. recent admission, nursing home, dialysis) without invasive procedures
3. Long hospitalisation/ invasive procedures
1. No treatment
2. Recent treatment
1. Young, few co-morbid conditions
2. Older/ multiple co-morbidities
3. Cystic fibrosis, structural lung disease, advanced AIDS, neutropenia, other severe immunodeficiency disorders
Score: of 1 in all 3 domains = low risk for resistant organisms
Score: of 2 in at least 1 group= risk for resistant enterobacteriaceae
Score: of 3 in 1 of the groups = risk for infection with nonfermenters
It is not rocket science….
• Clean your hands between patients– Beware taking herpes simplex, C. difficile and MRSA home
with you!
• Antibiotics are not the answer for every culture or every fever
• Optimize empiric therapy based on local epidemiology
• Find alternatives to antipseudomonal drugs

Areas for Future Research
• Appropriate specimen processing.• Role of routine Antimicrobial susceptibility testing.• Definition of appropriate duration of AB therapy.• The impact of prolonged therapy (oral regimens)• Impact of empirical therapy on tertiary peritonitis.• Confirmation of the pattern of infecting organisms in
tertiary peritonitis.
Solomkin JS, CID 2003



Reasons for exclusion from clinical and microbiological evaluability
Ertapenem Piperacillin/
Tazobactam
Number of patients not evaluable N = 120 N = 117
Reasons patients were not evaluable
No baseline pathogen identified 52 52
Inadequate duration of therapy 32 22
4-6 week followup visit missing 24 25
Concomitant antibiotics used (not for suspected intra-
abdominal failure)
13 12
Confounding events/other1 11 10
Inadequate source control 9 13
Not complicated intraabdominal infection 8 9
All baseline pathogens were resistant 6 7
Prestudy antibiotics >24 hours (in absence of failure) 6 5
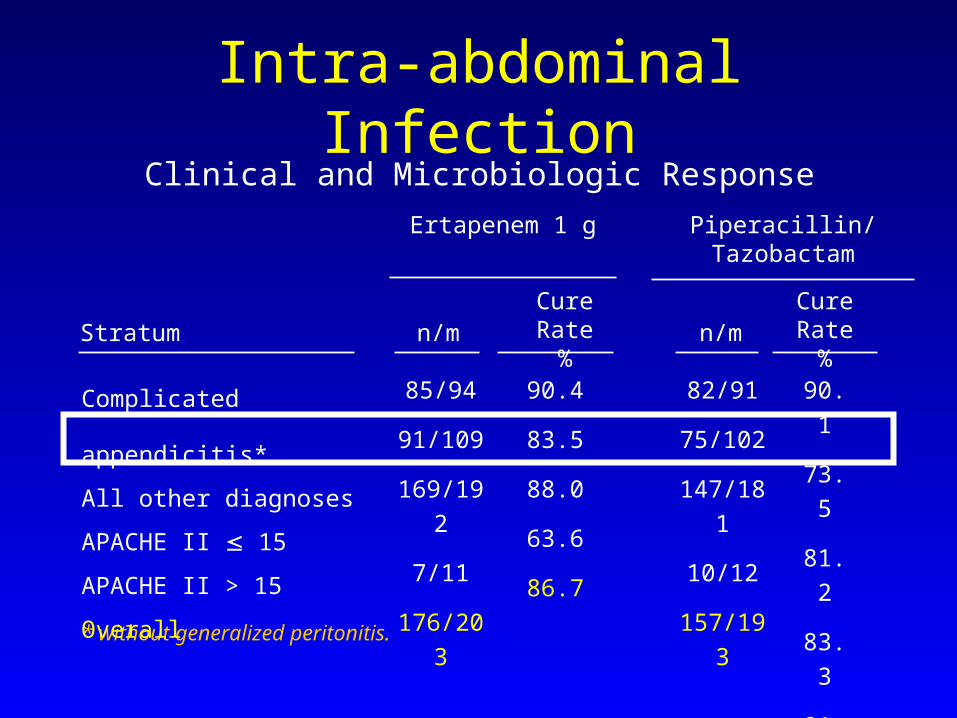
Intra-abdominal Infection
* without generalized peritonitis.
Ertapenem 1 g
n/mCure Rate
%
Complicated appendicitis*
All other diagnoses
APACHE II 15
APACHE II > 15
Overall
Stratum
Piperacillin/Tazobactam
n/m
85/94
91/109
169/192
7/11
176/203
90.4
83.5
88.0
63.6
86.7
82/91
75/102
147/181
10/12
157/193
90.1
73.5
81.2
83.3
81.3
Cure Rate%
Clinical and Microbiologic Response
• Roy Infect Dis Obstet Gynecol 2003 :Acute pelvic infections
Ertapenem

Excluded Diagnoses
• Traumatic bowel perforation with operation within 12 hours• Perforation of gastroduodenal ulcers operated upon within 24
hours• Simple cholecystitis• Simple appendicitis • Infected necrotizing pancreatitis• Staged abdominal repair or open abdomen technique

Appropiate Treatment
• Source control• Resuscitation• Physiological support of organ systems.• Monitoring Metabolic Respiratory Haemodynamic Nephrological Intra-abdominal pressures• Antibiotics based on knowledge of the probable flora.
Optimising Antibiotic Treatment in Serious
Infections D Paterson
Hospital-acquired MRSA
• ICU vs non-ICU– Proportion of nosocomial S. aureus isolates which are
MRSA in non-ICU areas now approaches proportion in ICUs
• Hospital size– Hospitals with less than 200 beds now have same
proportion of isolates which are MRSA as in hospitals with more than 500 beds
Source: CDC 2004
Vancomycin – current recommendations
• Dose at 1 gram every 12 hours only for wound infection, cellulitis etc
• Give 20-25 mg/kg every 12 hours for endocarditis and pneumonia (this will often mean 1.5 gram q 12hr IV)
• Only check trough levels (no need for peak levels) – aim for 10-20 μg/mL in most patients
Linezolid
• An oxazolidinone (only member of that class which is currently available)– Dose is 600mg q12 hr IV or PO– Second-line agent in pneumonia failing to respond to high-
dose vancomycin– Marrow toxicity– Lactic acidosis, peripheral neuropathy and optic neuritis
increasingly recognized

Daptomycin
• A lipopeptide (the only agent of this class currently available)
• IV formulation only (once per day)• Inactivated by surfactant• Rapidly bactericidal – appears at least as good as
vancomycin for bacteremia and endocarditis• Can cause CPK elevations

Tigecycline
• Glycylcyline (first of this class available)• Synthetic modification of tetracycline• Low blood levels, high tissue levels• Substantial rates of nausea/vomiting• Thus far, only approved for skin/soft tissue and intra-
abdominal infections
Despite the availability of new drugs….
• Antistaphylococcal penicillins are still the drugs of choice for methicillin susceptible Staphylococcus aureus

Community-acquired MRSA
• MMWR 1999;48:707 “Four pediatric deaths from community-acquired MRSA”
• “MRSA is an emerging community-acquired pathogen among patients without established risk factors for MRSA; eg, no recent hospitalization, no recent surgery, no residence in a long-term care facility and no injecting drug use”
CA-MRSA (II)
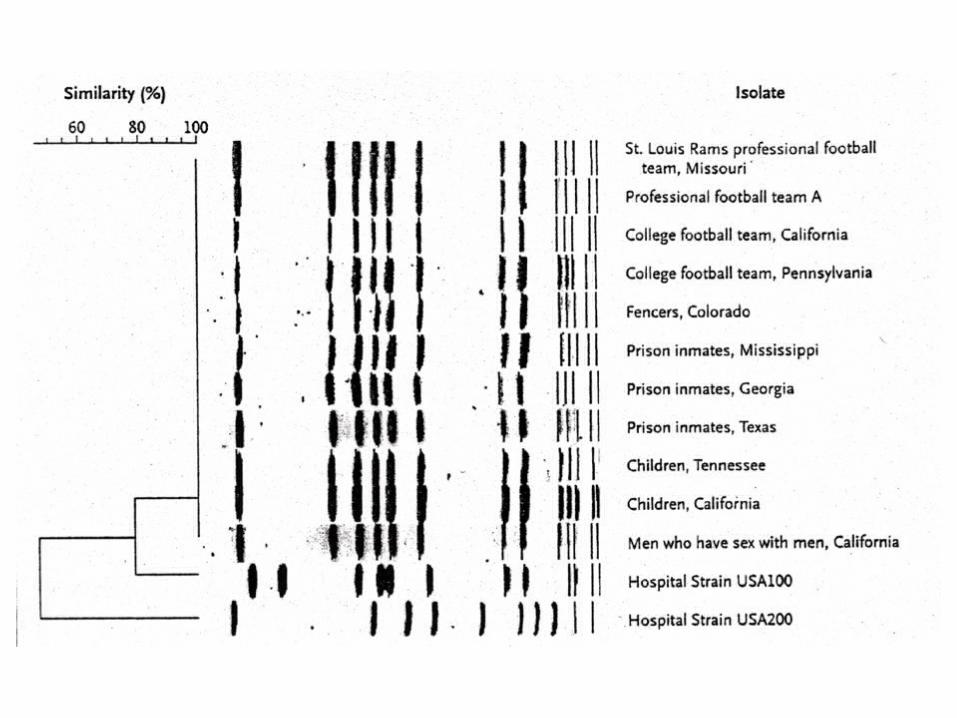
• The proportion of all “community-acquired” Staphylococcus aureus strains in the US which are MRSA, ranges from 9-20%, depending on the geographic region
• In the U.S., one PFGE type (“USA 300 strain”) is found throughout the country
• CA-MRSA has smaller resistance gene (SCCmecIV) • CA MRSA has gene for Panton-Valentine leukocidin
(PVL) toxin
CA-MRSA (III)
• Almost 90% of cases are skin infections, often first detected as clusters of abscesses (“spider bites”) – PVL is a necrotizing cytotoxin
• Various epidemiologic settings– Sports participants– Jails, military recruits– Men who have sex with men
CA-MRSA pneumonia following influenza
• 17 cases presented by CDC at IDSA 2004• Age range 8 months to 62 years• 4/17 had traditional MRSA risk factors• Fever of at least 39o C and hemoptysis were typical• 3/17 had radiologically evident cavitation/necrosis• 13/17 admitted to ICU• 5/17 died, with median of 7 days from symptom onset
to death

VISA/VRSA
• hVISA (heteroVISA)– Typically patients who fail prolonged vancomycin Rx– Numerous cases, but issues with detection
• VISA– 13 cases in USA (MIC 8-16)– 30 “near-VISAs” (MIC=4)
• VRSA– 4 cases thus far (MIC ≥ 32)
VRSA
• Four distinct isolates since July 2002• No relationships between the isolates• One patient was never known to have received
vancomycin but had dual VRE and MRSA carriage• Two isolates known to have mecA and vanA together• Enterococcus faecalis is known to be the donor of
vanA in one strain
VRE
• Rates appear to have stabilized• Still an issue because:
– Linezolid and daptomycin resistance noted and probably increasing
– Potential source of vancomycin resistance in staphylococci



Clostridium difficile
• Several case-control studies have linked quinolone use to resurgence of hospital-acquired C. difficile
• Most strains are quinolone resistant• An epidemic strain is circulating in North America and
Europe which is quinolone resistant and produces a new toxin (binary toxin)
• No evidence of metronidazole resistance
Muto ICHE 2005; McEllistrem CID 2004

Clostridium Difficile: Quebec “Superbug”
Pepin J, et al. CMAJ 2004;171:466; Pepin J, et al. Clin Infect Dis 2005;40:159.
1991-1992 2003 Odds Ratio
Cases 169 390 3.0
Complicated 7.1% 18.2% 2.2
Metro failure 10% 26% 2.6
Relapse 21% 47% 2.3

Enterobacter cloacae
• Emergence of resistance to third generation cephalosporins in approximately 20% of patients during treatment (Chow Ann Int Med 1991)
• Cefepime is comparatively stable to AmpC• 33% of Enterobacter cloacae isolates in my hospital
produce ESBLs• ESBLs in Enterobacter cloacae may compromise
cefepime activityLevison CID 2002
ESBLs in Salmonella
• Kruger et al AAC November 2004• 160 isolates from 13 hospitals in South Africa• 16% were ESBL producers (especially Salmonella
Isangi and Typhimurium)• “Hidden resistance” to ceftriaxone and cefotaxime

ESBL producers and “hidden” resistance
• % of ESBL producing Klebsiella which are:– Ceftriaxone “susceptible”: 36%– Ceftazidime “susceptible”: 19%
Paterson J Clin Micro 2001;39:2206-2212
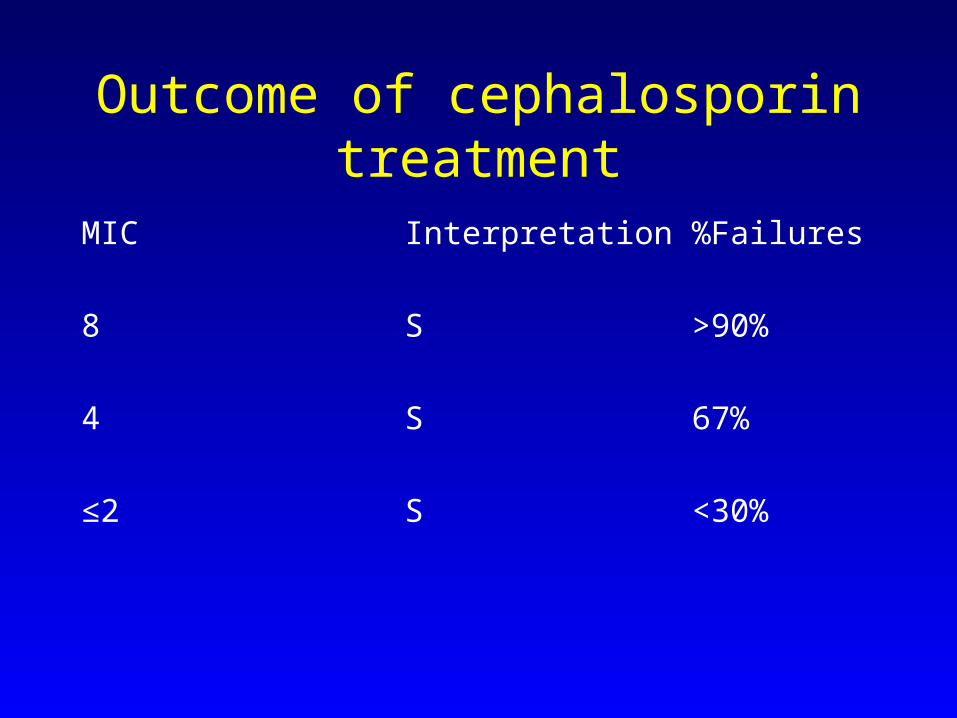
Outcome of cephalosporin treatment
MIC Interpretation%Failures
8 S >90%
4 S 67%
≤2 S <30%
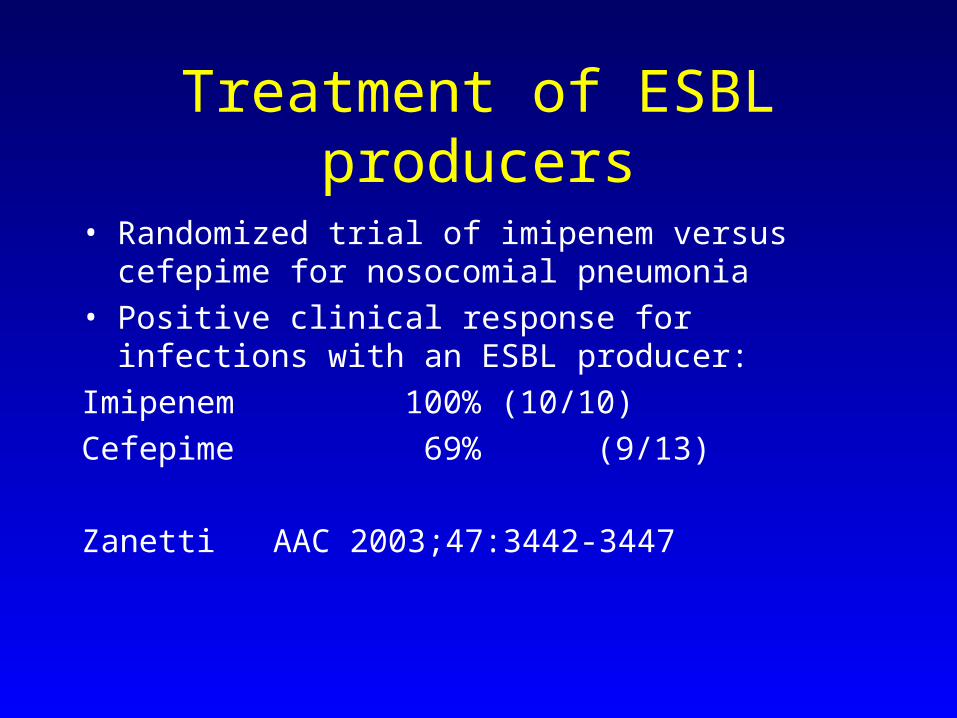
Treatment of ESBL producers
• Randomized trial of imipenem versus cefepime for nosocomial pneumonia
• Positive clinical response for infections with an ESBL producer:
Imipenem 100% (10/10)
Cefepime 69% (9/13)
Zanetti AAC 2003;47:3442-3447

Observational studies
All cause 14 day
mortality
Imipenem alone 3.7% (1/27)
Quinolone alone 36.3% (4/11)
Beta-lactam alone 44.4% (4/9)
(non-carbapenem)
Paterson CID 2004:39:31-37
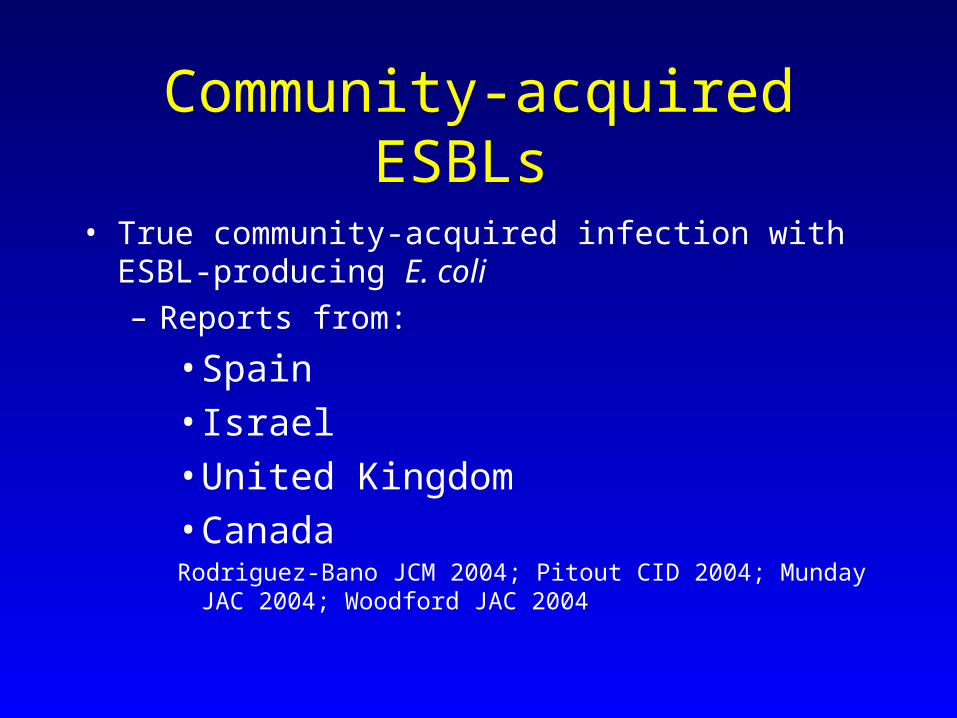
Community-acquired ESBLs
• True community-acquired infection with ESBL-producing E. coli– Reports from:
• Spain• Israel• United Kingdom• CanadaRodriguez-Bano JCM 2004; Pitout CID 2004; Munday JAC 2004;
Woodford JAC 2004

Community-acquired ESBLs (III)
• Typical picture is urinary tract infection (sometimes associated with bacteremia), due to ESBL producing E. coli, in elderly females
• Isolates are resistant to typical first line agents for UTI such as ciprofloxacin, TMP/SMX, gentamicin and ceftriaxone
Rodriguez-Bano JCM 2004; Pitout CID 2004; Munday JAC 2004; Woodford JAC 2004

The effects of space travel on antibiotic resistance
• Tixador R et al. Acta Astronaut 1985;12:131-134
• Cytos 2 experiment (French-Soviet manned flight July 1982)
• Bacteria became more resistant when taken into outer space
Management of Intra-Abdominal Infection (IAI)
J P Pretorius
Head: Surgical Intensive Care Unit Pretoria Academic Hospital


















