94
Problem 1 Julita Suhardi Emergency Medicine Block
| Date post: | 03-Jun-2018 |
| Category: |
Documents |
| Upload: | zhul-thaa-purpleholic |
| View: | 229 times |
| Download: | 0 times |
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 1/94
Problem 1
Julita Suhardi
Emergency Medicine Block
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 2/94
Cardiac Arrest
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 3/94
Description
• Sudden death:
– Death within 24 hours of symptom onset
– Initial presentation in 50% of patients with
cardiovascular disease• Factors affecting survival:
– Initial rhythm
– Time to successful defibrillation
• Incidence of re-arrest in neurologically intactsurvivors:
– 30% at 1 year and 60% at 5 years
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 4/94
Etiology
• Acute coronary ischemia:
– Underlying etiology in 50% of arrests
– Myocardial irritability leads to ventricular
fibrillation• Primary dysrhythmia:
– Congenital and acquired electrical abnormalities
–
Hypertrophic/dilated cardiomyopathy – Myocarditis
• Cardiac rupture
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 5/94
• Pericardial tamponade
•
Metabolic abnormalities• Noncardiac etiologies:
– Consider especially in cases of pulseless electrical
activity
– Tension pneumothorax
– Hemorrhage
– Massive pulmonary embolus
– Sepsis
– Severe acidosis
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 6/94
• Drugs or toxins:
– Antidysrhythmics
– Digoxin
– Beta-blockers
– Calcium channel blockers
– Tricyclic antidepressants
– Cocaine
– Heroin
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 7/94
Signs and Symptoms
• Unresponsiveness
• Pulselessness
• Shallow, gasping respirations may persist for a fewminutes
• Occasionally preceded by: – Chest pain
– Dyspnea
– Palpitations
– Seizure activity• Immediately prior to arrest:
– Shock or hypotension
– Impaired mentation
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 8/94
Tests
Lab
• Indicated only when successful Return ofspontaneous circulation (ROSC) is achieved:
– Electrolytes – Blood urea nitrogen/creatinine
– Creatinine kinase with isoenzymes, cardiac troponin
– Arterial blood gas (avoid arterial puncture in
thrombolysis candidates). – CBC
– Therapeutic drug levels
– Toxicological testing
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 9/94
Imaging
• ECG:
– Establish or rule out acute coronary syndrome
• Chest radiograph:
– Endotracheal tube position
– Cardiac silhouette
– Pneumothorax
• ECG: – Pericardial effusion
– Wall motion abnormality
– Valvular dysfunction
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 10/94
Differential Diagnosis
• Syncope
• Seizure
•
Acute stroke• Hypoglycemia
• Acute airway obstruction
• Head trauma• Toxins
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 11/94
Treatment : Pre Hospital
• CPR or active compression-decompressionCPR (ACD-CPR)
• Confirm underlying rhythm
• Early defibrillation of ventricular tachycardia(VT) or ventricular fibrillation (VF):
– Automated external defibrillator
–EMT-D or layperson
• Consider CPR before defibrillation in cases of ifarrest >5 minutes.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 12/94
Treatment : Pre Hospital
• Secure airway and provide adequate
respirations:
– Endotracheal intubation
– Laryngeal mask airway
• Post-resuscitation care:
– Identify cause of arrest
– 12-lead ECG
– Monitor vital signs
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 13/94
Treatment : Pre Hospital
• Transport to the closest facility:
– If return of spontaneous circulation, consider
transport to center equipped for interventional
cardiac care.
– Pediatric critical care center for children
• Termination of resuscitative efforts:
– Persistent, confirmed asystole
– Prolonged arrest
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 14/94
Initial Stabilization
• Initiate advanced cardiac life support (ACLS).
• Perform standard CPR as long as no pulse is palpable.
• Consider ACD-CPR:
– Stop CPR only briefly to check cardiac rhythm or intubate.
• Secure the airway
• Obtain IV access
• Cardiac monitor• Therapy based on the underlying rhythm according
to ACLS protocols
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 15/94
ED Treatment : Pulseless VT or VF
• Immediate defibrillation with up to threecountershocks: – 200 J
– 200“300 J
– 360 J• If defibrillation is unsuccessful:
– Epinephrine
– Vasopressin
•
If refractory to defibrillation and epinephrine: – Amiodarone
– Lidocaine
– Procainamide
– Magnesium for Torsades de Pointes
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 16/94
ED Treatment : Asystole
• Dismal prognosis if this is the presenting
rhythm
• Confirm in two or more leads
• Epinephrine
• Atropine
•
Consider transcutaneous pacing for severebrady-asystolic rhythm.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 17/94
ED Treatment : Pulseless Electrical
Activity
• Epinephrine
• Atropine
• Treat for reversible cause of pulseless
electrical activity – Pneumothorax
– Cardiac tamponade
–Hypoxia
– Pulmonary embolus
– Hypovolemia (hemorrhage)
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 18/94
ED Treatment : Post-Resuscitation
• Treat the underlying cause of the arrest.
• ECG to establish presence of acute coronary
syndrome:
– Immediate catheterization or thrombolysis for ACS
• Ventilatory support
• Continue antidysrhythmic therapy.
• Correct electrolyte abnormalities.
• Initiate volume resuscitation and provide
inotropic support as needed
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 19/94
Medication (Drugs)
• Amiodarone
• Atropine
•
Epinephrine• Lidocaine
• Magnesium
• Procainamide• Sodium bicarbonate
• Vasopressin
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 20/94
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 21/94
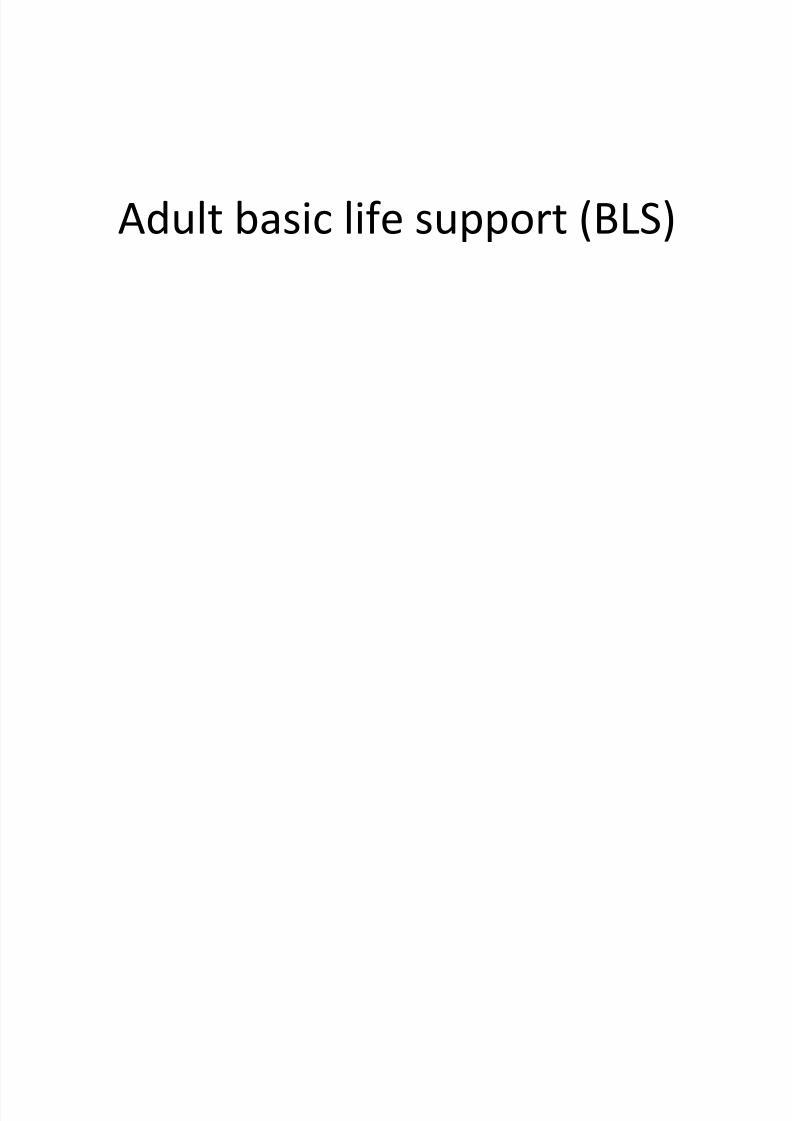
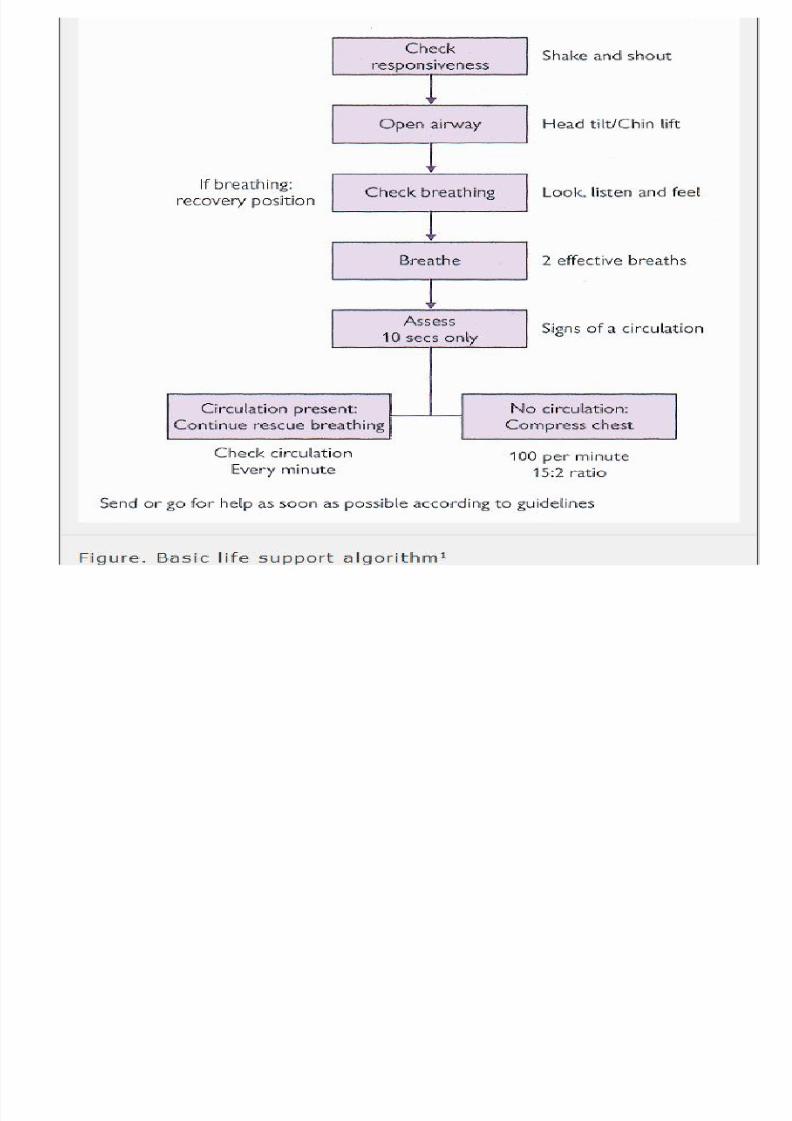
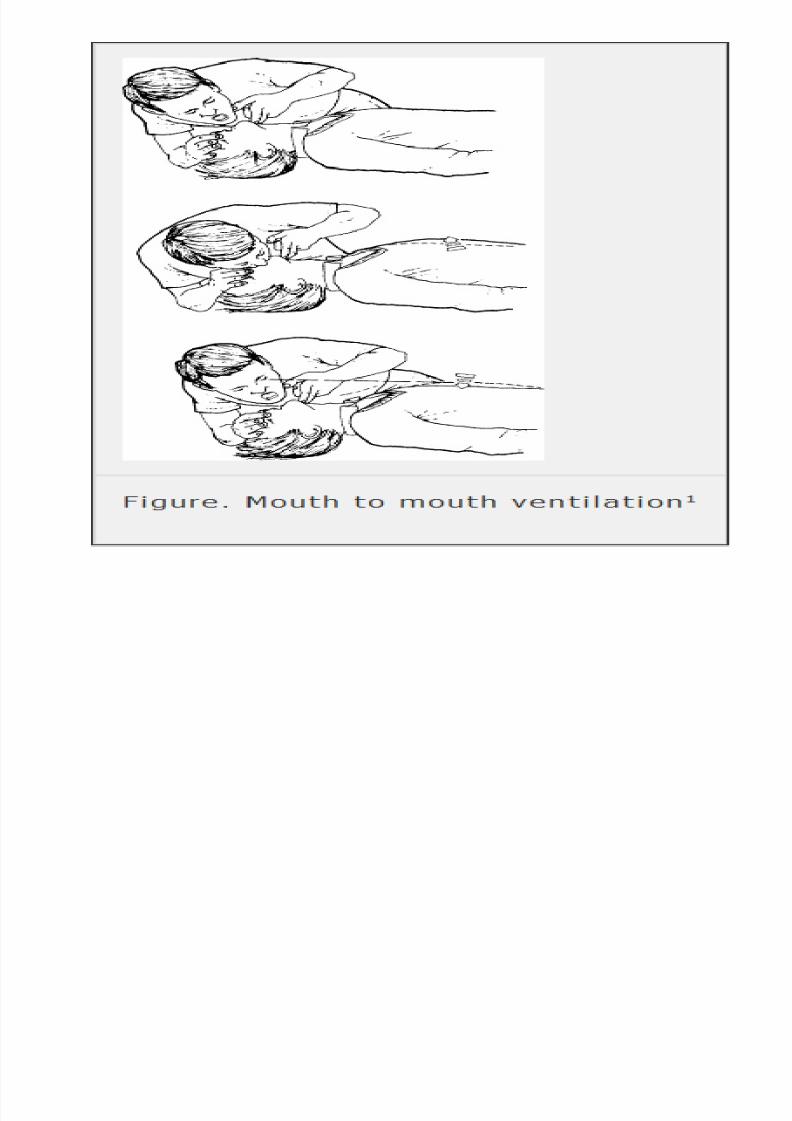
Adult basic life support (BLS)
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 22/94
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 23/94
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 24/94
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 25/94
PEA
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 26/94
PULSELESS ELECTRICAL ACTIVITY (PEA)
• Unresponsive state
• No respiration, pulse, or BP
•
Identifiable electrical rhythm on monitor butno pulse
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 27/94
Etiology
• failure of the normal cardiac pumping
mechanism
• obstruction to cardiac filling or output
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 28/94
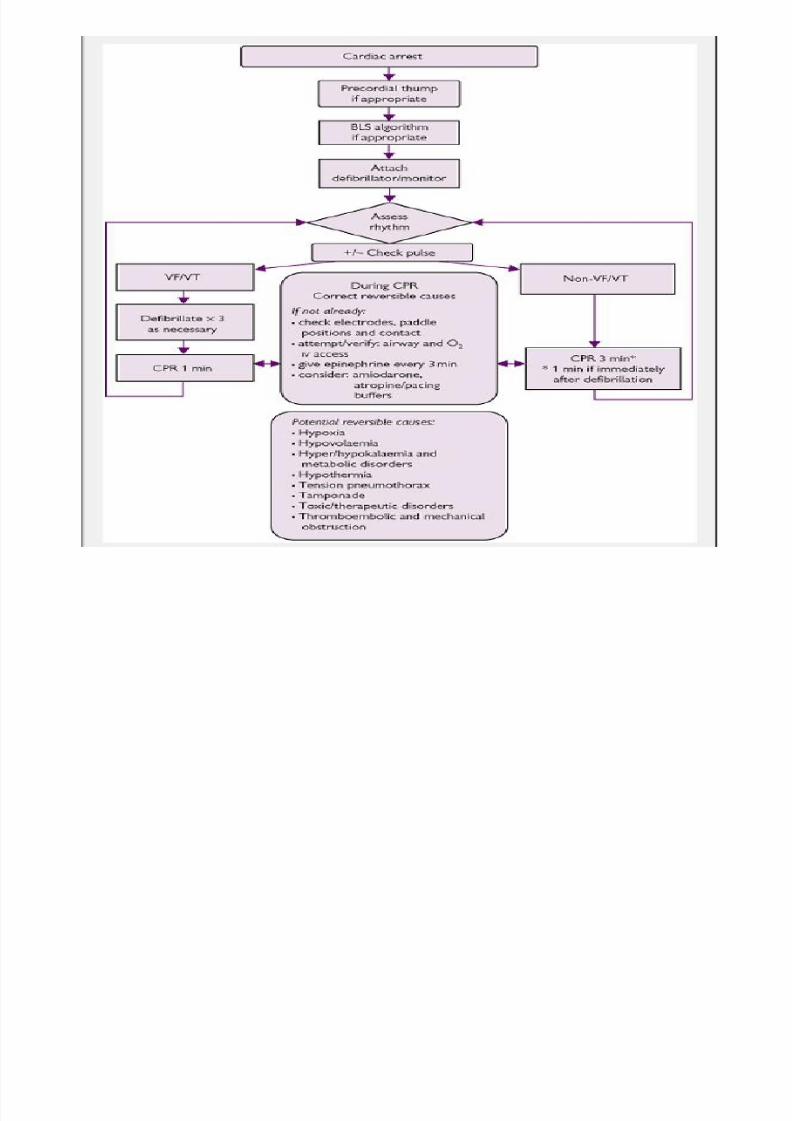
Etiology
4H's
• Hypoxia
• Hypovolaemia
• Hyper/hypokalaemia/metabolic disorders
• Hypothermia
4T's
• Tension pneumothorax
• Tamponade (cardiac)
• Toxic substances (eg overdose)
• Thromboembolic/mechanical obstruction
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 29/94
PULSELESS ELECTRICAL ACTIVITY (PEA)
1. Unresponsiveness,no respiration or pulse Call for help.
2. Begin CPR, provide oxygen and attach
manual monitor-defibrillator when availablewithout interrupting CPR.
3. When device is attached, stop CPR to assess
rhythm. If identifiable rhythm noted onmonitor, immediately resume CPR beginningwith compressions.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 30/94
PULSELESS ELECTRICAL ACTIVITY (PEA)
4. Consider and treat possible causes:
• Trauma Hypokalemia/hyperkalemia
•
Tension pneumothorax Hypovolemia• Thrombosis (pulmonary Hypoxia or coronary)
• Hypoglycemia
•Tamponade, cardiac Hypothermia
• Toxins Hydrogen ion (acidosis)
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 31/94
PULSELESS ELECTRICAL ACTIVITY (PEA)
5.Continue CPR using five cycles of 30
compressions and 2 breaths; check the
rhythm every 2 minutes.
6.Consider insertion of an advanced airway
(ETtube, LMA, or Combitube) if basic airway
management is inadequate.
7.If PEA persists epinephrine 1 mg,
vasopressin 40 U IV/IO to replace epinephrine.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 32/94
PULSELESS ELECTRICAL ACTIVITY (PEA)
8.Atropine 1 mg IV/IO heart rate on the ECGis less than 60 bpm.
9.Continue CPR; check the rhythm every 2
minutes.10.If the rhythm is not shockable with no pulse,
resume CPR and repeat steps 4 –8.
12.Stable ECG rhythm returns with adequatebreathing and circulation, monitor andreevaluate.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 33/94
ASYSTOLE
• Unresponsive state, no respiration, pulse, or
BP
• ECG shows flat line; no electrical activity
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 34/94
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 35/94
ASYSTOLE
4. Consider and treat possible causes:
• Trauma Hypokalemia/hyperkalemia
• Tension pneumothorax Hypovolemia
• Thrombosis (pulmonary Hypoxia or coronary)
• Hypoglycemia
•Tamponade, cardiac Hypothermia
• Toxins Hydrogen ion (acidosis)
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 36/94
ASYSTOLE
5.Continue CPR using five cycles of 30
compressions and 2 breaths; check the
rhythm every 2 minutes.
6.Consider insertion of an advanced airway
(ETtube, LMA, or Combitube) if basic airway
management is inadequate.
7.If asystole persists epinephrine 1 mg,
vasopressin 40 U IV/IO to replace epinephrine.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 37/94
ASYSTOLE
8. Consider atropine 1 mg IV/IO if the ECG stillshows asystole.
9.Continue CPR; check the rhythm every 2
minutes.10.If the rhythm is not shockable with no pulse,
resume CPR and repeat steps 4 –8.
12. If asystole persists, consider resuscitationprotocols were followed and reversible causesidentified.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 38/94
Acute Coronary Syndrome:
Myocardial Infarction
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 39/94
Description
• Imbalance in myocardial blood supply and
oxygen requirement
• Acute cardiac ischemia encompasses a
spectrum of disease processes:
– Unstable angina pectoris
– Acute myocardial infarction (AMI)
– ST elevation myocardial infarction (STEMI)
– Non-STEMI
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 40/94
Etiology
• Atherosclerotic narrowing of coronary vessels
• Vasospasme although this is usually at rest
and considered unstable if new onset
• Microvascular angina or abnormal relaxation
of vessels with diffuse vascular disease
• Plaque disruption
• Thrombosis
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 41/94
Etiology
• Arteritis:
– Lupus
– Takayasu disease
– Kawasaki disease
– Rheumatoid arthritis
• Prolonged hypotension
• Anemia
– Hemoglobin <8 g/dL
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 42/94
Etiology
• Hyperbarism or elevations incarboxyhemoglobin
• Coronary artery gas embolus
• Thyroid storm• Structural abnormalities of coronary arteries:
– Radiation fibrosis
– Aneurysms – Ectasia
• Cocaine- or amphetamine-induced vasospasm
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 43/94
Etiology
• Cardiac risk factors include:
– Hypercholesterolemia
– Diabetes mellitus
– Hypertension – Smoking
– Family history in a first-degree relative less than55 years old
– Men, age >55 years
– Postmenopausal women
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 44/94
Signs and Symptoms
• Chest pain:
– Most common presentation of myocardial
infarction (MI)
– Substernal pressure
– Heaviness
– Squeezing
– Burning sensation – Tightness
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 45/94
Signs and Symptoms
• Anginal equivalents (MI without chest pain):
– Abdominal pain
– Syncope
– Diaphoresis
– Nausea or vomiting
– Weakness
• May localize or radiate to arms, shoulders,
back, neck, or jaw
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 46/94
Signs and Symptoms
• Associated symptoms:
– Dyspnea
– Syncope
– Fatigue – Diaphoresis
– Nausea
– Vomiting
• Symptoms are usually reproduced by exertion,eating, exposure to cold, or emotional stress.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 47/94
Signs and Symptoms
• Symptoms commonly last 30 minutes or more.• Symptoms may occur with rest or during
exertion.
• Often preceded by crescendo angina
• May be improved or relieved with rest ornitroglycerin
• Symptoms generally unchanged with position or
inspiration• Positive Levine sign or clenched fist over chest is
suggestive of angina.
• Blood pressure (BP) is usually elevated during
symptoms.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 48/94
Physical Exam
• Physical exam is usually unrevealing.
• Occasional physical findings include:
– S3 or S4 due to left ventricular systolic or diastolic
symptoms
– Papillary muscle dysfunction resulting in mitral
regurgitation
– Diminished peripheral pulses
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 49/94
• Tests
– ECG
• Lab
– CK-MB and troponin I or T
– Hematocrit
– Coagulation profile
– Creatinine
• Diagnostic Procedures/Surgery – See Cardiac Testing
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 50/94
Differential Diagnosis
• Anxiety• Aortic dissection
• Biliary colic
• Costochondritis
• Esophageal reflux• Esophageal spasm
• Herpes zoster
• Hiatal hernia
•
Mitral valve prolapse• Myocardial infarction
• Panic disorder
• Peptic ulcer disease• Pneumonia
• Psychogenic
• Pulmonary embolus
• Unstable angina
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 51/94
Treatment
• Pre Hospital
– IV access
– Aspirin
– Oxygen
– Cardiac monitoring
– Sublingual nitroglycerin for symptom relief
– 12-lead ECG, if possible, with transmission orresults relayed to receiving hospital
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 52/94
• Alert
– All chest pain should be treated and transported
as a possible life-threatening emergency.
– Do not administer thrombolytics or heparin if
aortic dissection is suspected.
• Initial Stabilization – IV access
– Oxygen
– Cardiac monitoring
– Oxygen saturation
– Continuous BP monitoring and pulse oximetry
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 53/94
ED Treatment
• STEMI requires reperfusion therapy as soon as
possible:
– Thrombolytics should be used if percutaneous
coronary intervention is not readily availablewithin a 90-minute time frame (see Reperfusion
Therapy, Cardiac).
•
Patients with non-STEMI, if started onglycoprotein IIb/IIIa inhibitors and if they
subsequently receive a stent, benefit from a
PCI within a 48-hour time frame.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 54/94
• Aspirin should be administered first to all
patients with suspected MI unless the patient
has a known allergy.
• If BP is >90–100 mm Hg systolic, administer
sublingual nitroglycerin, nitropaste, or IV
nitroglycerin assuming no ECG criteria of rightventricular infarct:
– Symptoms that persist after three sublingual
nitroglycerin tablets are strongly suggestive ofAMI or noncardiac etiology
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 55/94
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 56/94
• Beta-blockers should be administered if no
contraindications (e.g., bradyarrhythmias,
heart rate <60, congestive heart failure,hypotension, or obstructive pulmonary
disease) are present.
• Clopidogrel may be of benefit acutely whenadded to standard therapy by reducing the
odds of AMI patients having another occluded
artery, or a second heart attack or death by36% after 1 week of hospitalization.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 57/94
• Statin therapy reduces clinical events in
patients with stable coronary artery disease.,
this may also extend to patients experiencing
an acute ischemic coronary event.
• If patient is in cardiogenic shock, patient
should be transported to a cardiac
catheterization laboratory for angioplasty and
intra-aortic balloon pump as soon as possible
(see Congestive Heart Failure).
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 58/94
• Bradydysrhythmia associated withhypotension should be treated with atropine
or external pacing:• Conduction disturbances:
– First-degree aortic valve (AV) block and Mobitz I(Wenckebach) are often self-limited and do not
require treatment. – Mobitz II, complete heart block, new right bundle
branch block (RBBB) in anterior MI, RBBB plus leftanterior branch block or left posterior fascicular
block, left bundle branch block plus first-degreeAV block may require a temporary transvenouspacemaker.
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 59/94
Medication (Drugs)
• Amiodarone
• Aspirin
• Clopidogrel (Plavix)
• Enoxaparin (Lovenox)
• Heparin
•
Lidocaine• Magnesium
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 60/94
• Glycoprotein IIb/IIIa inhibitors:
– Eptifibatide
– Irofiban (Aggrastat)
– Abciximab (ReoPro)
• Nitropaste:
• Thrombolyt
• Metoprolol
• Morphine
• Nitroglycerin
• Nitroglycerin
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 61/94
MI ( non ST ELEvation )
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 62/94
Description
• Non-ST-elevation myocardial infarction
(NSTEMI) is a part of a clinical syndrome that
includes unstable angina.
• Probable cause is the generation of a subtotalcoronary occlusion or functional collateral
circulation:
– Often indicates an incomplete ischemic event
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 63/94
Description
• Coronary plaque disruption:
– Endothelial disruption exposes subendothelial
collagen and other platelet-adhering ligands, von
Willebrand factor (vWF), and fibronectin. – Release of tissue factors activates factor VII and
extrinsic pathway
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 64/94
Description
• Thrombus generation:
– Platelet adhesion via glycoprotein (GP) Ia/IIa to
collagen:
• Platelet activation: release of ADP, thromboxane A2, andserotonin alters the platelet GP IIb/IIIa receptor
vasoconstriction
• Platelet aggregation: GP IIb/IIIa receptor binds fibrinogen
molecules, cross-links platelets
local platelet plug – Platelet stabilization: thrombin converts fibrinogen
to fibrin, provides fibrin mesh, stabilizes platelet
aggregate
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 65/94
Etiology
• Coronary thrombosis
• Coronary artery spasm, idiopathic or cocaine
induced
• In situ thrombosis/hypercoagulable states
• Embolic event
• Arteritis
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 66/94
Signs and Symptoms (Diagnosis)
History• Pain:
– Pressure or tightness or heaviness
– Substernal, epigastric
– +/- radiation to arm, jaw, back
• Nausea, vomiting
• Diaphoresis
• Cough
• Dyspnea
• Anxiety
• Light-headedness
• Syncope
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 67/94
Signs and Symptoms (Diagnosis)
Physical Exam
• Hypertension
• Hypotension
• Arrhythmias
• S4 heart sound
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 68/94
Essential Workup
• ECG,
• cardiac markers,
• chest radiograph
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 69/94
TEST
Lab• Cardiac markers:
– Troponins: specific indicators of myocardial infarction
– Creatine kinase (CK
–Myoglobin
– LDH
• CBC
• Serum electrolytes including magnesium
•ESR: nonspecific marker of inflammation, rises within 3days, elevated for several weeks
• PT/PTT/INR for patients on warfarin
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 70/94
TEST
Imaging
• ECG:
– ST-segment depression or transient elevation
indicates increased risk – T-wave inversion in regional patterns does not
increase risk but helps differentiate cardiac pain fromnon cardiac pain
•
Chest radiograph: – To assess heart size, pulmonary edema/congestion or
identify other causes of chest pain
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 71/94
TEST
Imaging
• Echocardiography:
– To identify wall motion abnormalities and assess
left ventricular function• Radionuclide studies:
– Thallium or sestamibi scanning: identifies viablemyocardium
– Technetium 99: identifies recently infarctedmyocardium
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 72/94
Differential Diagnosis
• ST-elevation myocardial infarction• Pulmonary embolus
• Aortic dissection
•
Acute pericarditis• Pneumothorax
• Pancreatitis
• Pneumonia
• Esophageal spasm/gastroesophageal reflux• Esophageal rupture
• Musculoskeletal pain (diagnosis of exclusion)
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 73/94
Treatment
Pre Hospital
• IV access
• Oxygen administration
• Cardiac monitoring and treatment of
arrhythmias
• Aspirin, analgesia, anxiolytics
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 74/94
Treatment
Initial Stabilization
• Oxygen administration
• IV access
• Cardiac monitoring and treatment of
arrhythmias
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 75/94
Treatment
Initial Stabilization
• Oxygen administration
• IV access
• Cardiac monitoring and treatment of
arrhythmias
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 76/94
Medication
• Aspirin
• Beta-blockers:
– Atenolol
– Esmolol
– Metoprolol
– Propranolol
• Clopidogrel
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 77/94
Medication
• Calcium channel blockers
– Diltiazem
– Verapamil
• GP IIb/IIIa inhibitors:
– Abciximab
– Eptifibatide
– Tirofiban
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 78/94
Medication
• Heparins:
– Enoxaparin
– Unfractionated heparin
• Lorazepam
• Morphine sulfate
• Nitroglycerin
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 79/94
Shock kardiogenik
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 80/94
Description
• Inadequate tissue perfusion due to cardiac
dysfunction
• Underlying mechanisms in acute myocardial
infarction (AMI): – Pump failure:
• left ventricle (LV) infarct
•
Infarct in pre-existing LV dysfunction• Reinfarction
i i
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 81/94
Description
– Mechanical complications:
• Acute mitral regurgitation
• Ventricular septal defect
• LV rupture
• Pericardial tamponade
– Right ventricular (RV) infarction
E i l
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 82/94
Etiology
• AMI• Sepsis
• Myocarditis
• Myocardial contusion
• Valvular disease• Cardiomyopathy
• Left atrial myxoma
• Drug toxicity: – Beta-blocker – Calcium channel blocker
– Adriamycin
Si d S
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 83/94
Signs and Symptoms
• ABCs and vital signs: – Patent airway (early)
– Labored breathing and tachypnea (early); respiratoryfailure (late)
–Diffuse crackles or wheezing
– Hypoxia
– Hypotension:• Systolic blood pressure <90 mm Hg
• Decline by at least 30 mm Hg below baseline level
– Tachycardia
– Weak pulses
Si d S
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 84/94
Signs and Symptoms
• General:
– Cyanosis
– Pallor
– Diaphoresis
– Dulled sensorium
– Decrease in body temperature
– Urine flow of less than 20 mL/h
Si d S t
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 85/94
Signs and Symptoms
• Cardiac:
– Ischemic chest pain
– Systolic apical blowing murmur
– Gallop rhythm:• S3 reflects severe myocardial dysfunction
• S4 is present in 80% patients in sinus rhythm with AMI
–
Systolic click:• Suggests rupture of the chordae tendinae
Si d S t
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 86/94
Signs and Symptoms
• Neck:
– Jugular venous distention
• Abdominal:
– Epigastric pain
– Nausea and vomiting
• Neurologic:
– Obtundation
T t
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 87/94
Test
Electrocardiogram
• Normal ECG does not rule out AMI.
• Findings of AMI (ST-elevations in two or more
contiguous leads)
• May occur in non-ST-elevation acute coronary
syndrome
• Dysrhythmias
• LV hypertrophy
T t
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 88/94
Test
Chest Radiography
• Pulmonary congestion
• Pleural effusion
• Cardiomegaly
• Pneumonia
•
Pneumothorax• Pericardial effusion
T t
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 89/94
TestEmergent Echocardiography
• Transthoracic echocardiography (TTE) with colorDoppler
• LV contractility looking for hypokinesis, akinesis ordyskinesis
• Acute mitral regurgitation or septal defects
• RV dilatation, tricuspid insufficiency, high pulmonaryartery and RV pressures suggest pulmonary embolism
• RV hypokinesis or akinesis, RV dilatation, normalpulmonary pressures suggest RV infarction
• Pericardial effusion, right atrium or RV diastolic collapsesuggest cardiac tamponade
L b
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 90/94
Lab
• B-type natriuretic peptide (BNP): – Diagnostic and prognostic value
• Creatine kinase (CK), CK-Mb, troponin
• Electrolytes and renal function – Acute renal failure is a strong predictor of
mortality
• CBC:
– Identify anemia or elevated WBC
• Drug levels (e.g., digoxin)
Diff ti l Di i
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 91/94
Differential Diagnosis
• Obstructive shock
• Distributive shock
• Hypovolemic shock
Treatment
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 92/94
Treatment
Pre Hospital
• ABCs, IV access, O2, monitor
• Consider fluid bolus if no crackles.
• Aspirin
• Nitroglycerin or morphine sulfate for chest
pain in absence of hypotension
• Transport AMI patients to facility with 24-hour
cardiac revascularization capability.
Treatment
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 93/94
Treatment
Initial Stabilization• ABCs
• Two large bore peripheral IV lines
• Cardiac monitor
• Endotracheal intubation for airway compromise: – Consider etomidate for induction (minimal effect on
blood pressure)
• Fluid challenge (100–250 mL normal saline) inabsence of pulmonary congestion
• Foley catheter to monitor urine output
Treatment
8/12/2019 Julita (Problem1-KGD) (01)
http://slidepdf.com/reader/full/julita-problem1-kgd-01 94/94
Treatment
Medication (Drugs)• Dobutamine
• Dopamine
• Furosemide• Milrinone
• Nitroglycerin
• Nitroprusside• Norepinephrine

















