June 6-10, 2004 CRI Workshop, Haifa Treatment Planning for Radiofrequency Ablation of Liver Tumors Ariela Sofer, George Mason University Masami Stahr, George Mason University Bradford J. Wood, National Institutes of Health
Transcript
June 6-10, 2004 CRI Workshop, Haifa
Treatment Planning for Radiofrequency Ablation of
Liver Tumors
Ariela Sofer, George Mason UniversityMasami Stahr, George Mason University
Bradford J. Wood, National Institutes of Health
June 6-10, 2004 CRI Workshop, Haifa
Agenda
• Introduction:Liver Cancer and Radiofrequency Ablation
• The Temperature Distribution
• Challenges in Treatment Planning
• Final Thoughts
June 6-10, 2004 CRI Workshop, Haifa
Agenda
• Introduction:Liver Cancer and Radiofrequency Ablation
• The Temperature Distribution
• Challenges in Treatment Planning
• Final Thoughts
June 6-10, 2004 CRI Workshop, Haifa
Primary and Secondary Liver Tumors
• Primary liver cancer is among the most common cancers worldwide:– Over one million new cases annually– Death rate ~ occurrence rate
• Even higher rates for colorectal carcinoma metastases (“secondary tumors”) in the liver
• Surgical resection - the gold standard of therapy
• But most patients are poor candidates for surgery
• Radiofrequency ablation - a promising treatment option for unresectable hepatic tumors.
June 6-10, 2004 CRI Workshop, Haifa
Radiofrequency Ablation (RFA)
• A noninvasive technique for killing tumors by heat.
• A needle electrode is placed at the tumor site and an electrical current applied. This generates frictional heat. Heat in excess of 50oc will kill the tumor.
June 6-10, 2004 CRI Workshop, Haifa
Ablation Treatment Planning
Determine the number of needles, their position, size, and power applied, to guarantee that the entire tumor is killed while damage to vital healthy tissue is limited.
June 6-10, 2004 CRI Workshop, Haifa
• May be safely performed on an outpatient basis with conscious sedation
• Complex cases may require general anesthesia and overnight observation.
• Commonly performed percutaneously
• May also be implemented in open or laparoscopic surgery
• Treatment sessions about 10--30 minutes long.
Features of RFA
June 6-10, 2004 CRI Workshop, Haifa
• Can treat small and (sometimes) mid-size tumors.
• May convert an inoperable patient into a surgical candidate.
RFA for Liver Tumors
June 6-10, 2004 CRI Workshop, Haifa
• No long-term, prospective randomized clinical trials yet. However, early results are optimistic and suggest that RFA provides safe and effective local treatment of some cancers, with very small complication rates.
• Failures of RFA often associated with under-ablation and/or failure to create an adequate tumor-free margin
• Higher success rates for HCC tumors than for metastases
RFA for Liver Tumors
June 6-10, 2004 CRI Workshop, Haifa
The Needle Electrodes
A variety of RF needle electrodes in different sizes and configurations.
June 6-10, 2004 CRI Workshop, Haifa
The RFA Procedure
A closed-loop circuit is made by placing grounding pads on the thighs and connecting then in series with the generator, and the needle electrode.
Ultrasound and/or CT used for guidance
June 6-10, 2004 CRI Workshop, Haifa
At 50oc protein is damagedpermanently and cell membranes fuse. Coagulation necrosis.
Alternating current at high frequency (500 KHz) is applied. Tissue ions are agitated as they attempt to follow the changes in direction of AC.
Frictional heat. Heat extends to adjacent tissue by
conductance
RF Heating Mechanism
June 6-10, 2004 CRI Workshop, Haifa
More on Thermal Damage
45oC: heating for several hours irreversible damage
42oC: tissue susceptible to chemo / radiation
50oC: heating 4-6 minutes irreversible damage
60oC-100oC: near immediate protein coagulation
100oC-110oC: tissue vaporizes and carbonizes
June 6-10, 2004 CRI Workshop, Haifa
Factors Impeding Ablation
• Temperatures > 100oC: – Charring of tissue close to needle that
prevents transfer of heat to tissue further away.
– Vaporization. Gas acts as insulator.
• Blood vessels near the tissue:– convection of thermal energy away
Killed tumor cells are replaced by fibrosis and scar tissue
CT: Pre-treatment CT: 6 months after
RFA Before and After
Consecutive CT images - the input to the 3-D optimization
June 6-10, 2004 CRI Workshop, Haifa
The Ablation Process
• Nitrogen micro-bubbles gradually create a hyperechogenic area on ultrasound that provides a rough estimation of the treated tissue
• Larger tumors can be treated by multiple needles with overlapping treatment regions. Because of changes in conductivity of ablated tissues, and because microbubbles can obscure visualization, the deepest tumor regions should be treated first.
June 6-10, 2004 CRI Workshop, Haifa
Other Thermal Ablation Techniques
• Microwave Ablation
• Laser Ablation
• Ultrasound Ablation
• Cryoblation
June 6-10, 2004 CRI Workshop, Haifa
Agenda
• Introduction:Liver Cancer and Radiofrequency Ablation
• The Temperature Distribution
• Challenges in Treatment Planning
• Final Thoughts
June 6-10, 2004 CRI Workshop, Haifa
Temperature Distribution: the Bioheat Equation
change in energy stored within
heat conduct
ed in
heat conducted out
heat generated within
= +-
tissuedensity
specific heat
thermal conductivit
y
T=T(x,t) temp.
• = div
=grad
heat loss toblood perfusionRFA heat
source
June 6-10, 2004 CRI Workshop, Haifa
T=T(x,t) temp.
heat loss toblood
perfusion
The Bioheat Equation: The Heat Source
RFA heat source
V=V(x,t) electricalpotential
electricalconductivit
y
June 6-10, 2004 CRI Workshop, Haifa
The Bioheat Equation – Boundary Conditions
Electrical Potential
Temperature
June 6-10, 2004 CRI Workshop, Haifa
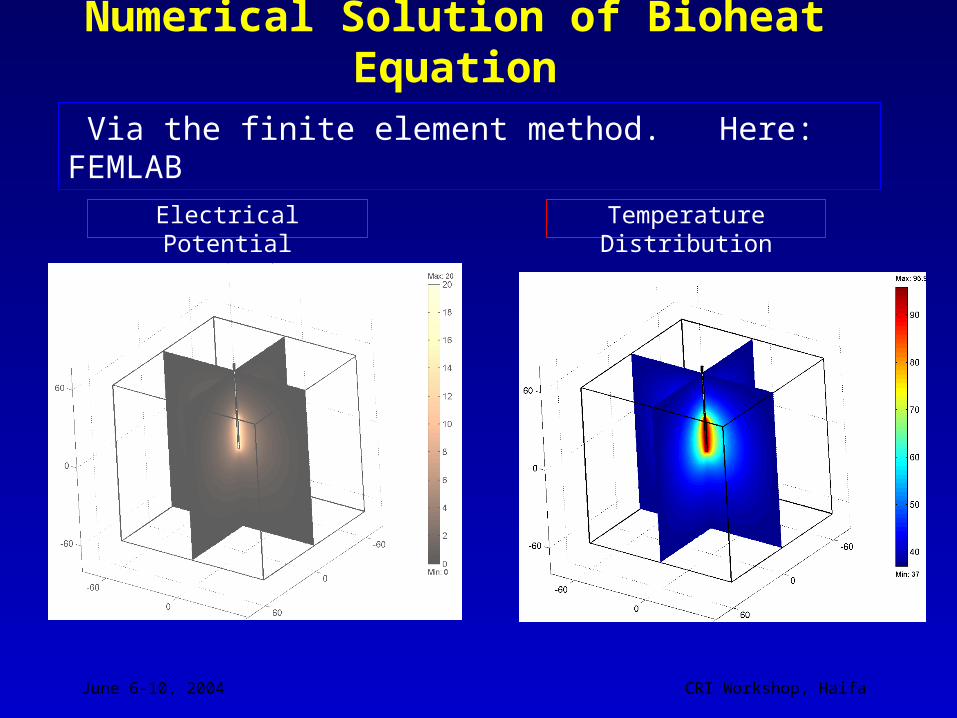
Numerical Solution of Bioheat Equation
Via the finite element method. Here: FEMLAB
Electrical Potential Temperature Distribution
June 6-10, 2004 CRI Workshop, Haifa
Numerical Solution of Bioheat Equation: Slice
Electrical Potential Temperature Distribution
June 6-10, 2004 CRI Workshop, Haifa
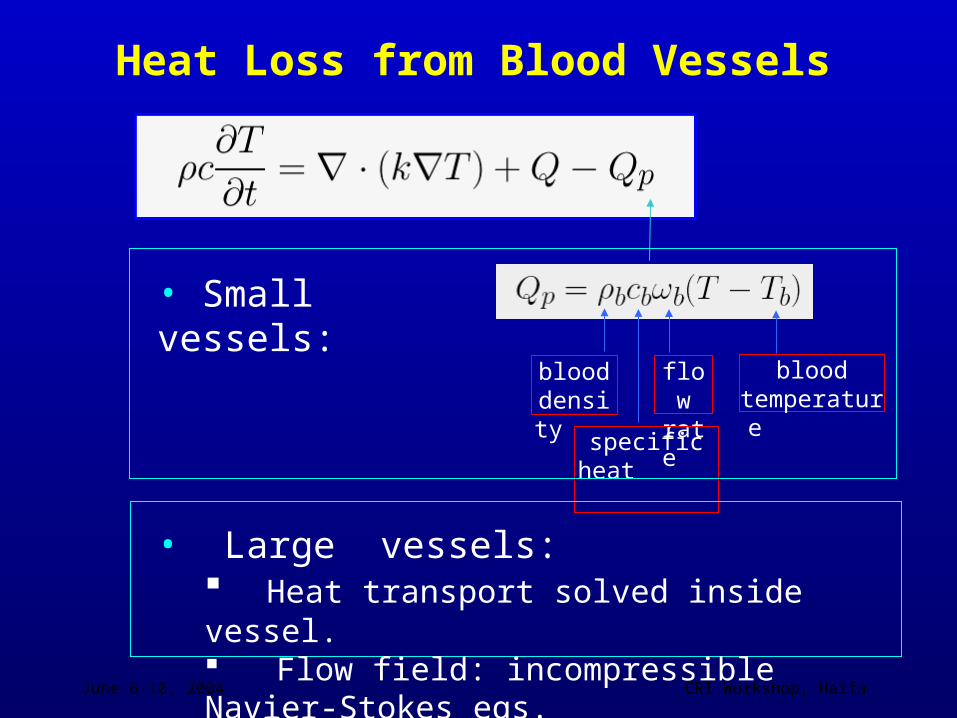
Heat Loss from Blood Vessels
blood density
flow rate
blood temperatur
e
specific heat
• Small vessels:
• Large vessels: Heat transport solved inside vessel. Flow field: incompressible Navier-Stokes eqs.
June 6-10, 2004 CRI Workshop, Haifa
Effect of Blood Flow (Large Vessel)
needle
blood vessel
convective heat transport by blood
June 6-10, 2004 CRI Workshop, Haifa
Agenda
• Introduction:Liver Cancer and RadioFrequency Ablation
• The Temperature Distribution
• Challenges in Treatment Planning
• Final Thoughts
June 6-10, 2004 CRI Workshop, Haifa
The Ideal Ablation Treatment Plan
Entire tumor (+ 1cm margin) is
killed
No thermal damage to critical organs
In reasonable time!
Limited damage to healthy tissue
June 6-10, 2004 CRI Workshop, Haifa
Further Considerations
No. of puncture holes
Is resection part of overall treatment plan?
Convenient access
June 6-10, 2004 CRI Workshop, Haifa
Treatment Planning Features
• Small number of decision variables:– Number of needles and their
configuration– Placement of needles
• But (potentially) lots of state variables:– Temperature at grid points on volume of
interest
• Temperature requires solution of a set of coupled partial differential equations
June 6-10, 2004 CRI Workshop, Haifa
Treatment Planning Features (cont’d)
Temperature “dose” is not cumulative
IMRT key factor:
Total dose
RFA key factor:
Maximum dose
June 6-10, 2004 CRI Workshop, Haifa
Challenge: Constraints Governed by PDE’s
•Each 3-D PDE solution takes many minutes
•The optimization involves repeated PDE’s
•Moreover, as needle position changes, the needle boundary “moves” and entire mesh changes
•But treatment plans must be available within just a few hours
June 6-10, 2004 CRI Workshop, Haifa
Challenge: Large Tumors - Multiple Needles
Overlapping spheres? Overlapping cylinders?
Images from Dodd. et als, Radiographics 2000
Added combinatorial complexity!
June 6-10, 2004 CRI Workshop, Haifa
Challenge: What Objective? What Constraints?
Minimize: underheating in tumorWhile prohibiting damage to critical structure limit damage to normal tissue But - may lead to many slightly underheated cells. Or to an awkward lesion shape Minimize: damage to critical structureWhile killing every cell in tumor limiting damage to normal tissue May not be achievable or medically acceptable
Minimize: damage to normal tissueWhile: killing every cell in tumor prohibiting damage to critical structureBut - may not be achievable
June 6-10, 2004 CRI Workshop, Haifa
Challenge: Those Pesky Coefficients
Factors affecting thermal properties of tissue:
– normal tissue– cirrhotic tissue– HCC– metastases– vascularization– effect of temperature on parameters
June 6-10, 2004 CRI Workshop, Haifa
Challenge: Complexity of Energy Sources
• Needle Electrodes:– Single, multiple, multi tined
• Energy Deposition– Pulsed, impedance regulated, internally
cooled
• Adjuvant Therapies– Use of saline solution to alter electrical and
thermal conductivity
June 6-10, 2004 CRI Workshop, Haifa
Agenda
• Introduction:Liver Cancer and Radiofrequency Ablation
• The Temperature Distribution
• Challenges in Treatment Planning
• Final Thoughts
June 6-10, 2004 CRI Workshop, Haifa
Final Thoughts
• RFA treatment planning poses many complex mathematical and practical challenges
• Much to learn from the radiation therapy community
• Research relevant not only to RFA, but other thermal ablation modalities









































![John Jay: Founding Father by Walter Stahr [Excerpt]](https://static.documents.pub/doc/80x56/55336462550346457f8b48ac/john-jay-founding-father-by-walter-stahr-excerpt.jpg)







