42
Pharmacology of drugs in extr apyramidal disorders Prof.Aznan Lelo,dr,PhD,SpFK & dr Datt en Bangun,MSc,SpFK
| Date post: | 14-Apr-2018 |
| Category: |
Documents |
| Upload: | winson-chitra |
| View: | 217 times |
| Download: | 0 times |

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 1/42
Pharmacology of drugs in
extrapyramidal disorders
Prof.Aznan Lelo,dr,PhD,SpFK
&dr Datten Bangun,MSc,SpFK

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 2/42
Definition:
• Neurologic syndromes in which abnormal
movement occur due to:
= a disturbance of fluency and speed of voluntarymovement or :
= the presence of unintended extra movements
Extrapyramidal syndrome
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 3/42
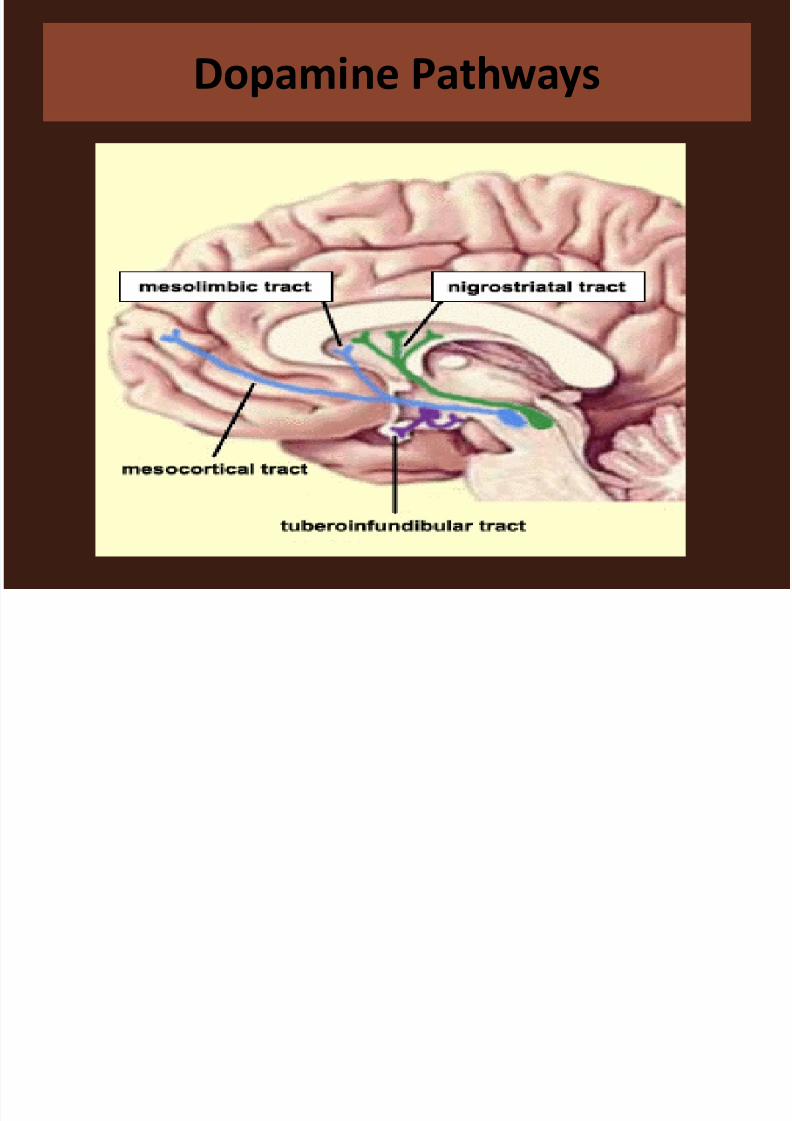
Dopamine Pathways

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 4/42
Dopamine functions
• Motor control - nigrostriatal system
– Deficiency results in rigidity, tremor and difficulty initiating movement
• Behavioural effects - mesolimbic system
– Overactivity in rats leads to abnormal behavior
•
Endocrine control - tubero-infundibular system – Dopamine and dopamine agonists suppress
prolactin release, dopamine antagonists may stimulate it
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 5/42
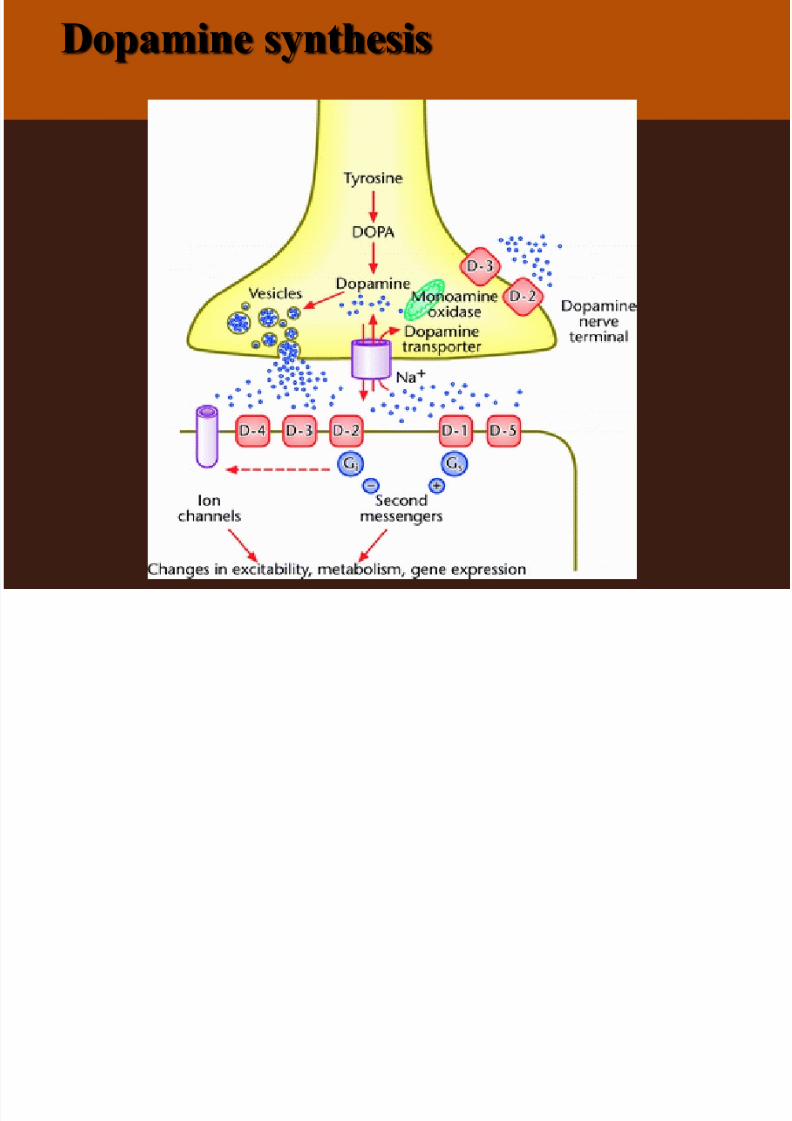
Dopamine synthesis

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 6/42
Pathogenesis
• Results from dysfunction of the extrapyramidal system
• Basal ganglion:caudate, putamen, globus pallidus,
subthalamic nucleus, and substantia nigra
• motor area of cortex--> basal gangalion(organizing
movement commands)
# affects the size and speed of movements
# selection of components of movements or thesequencing of multi-step movements

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 7/42
Drug-induced EPS(1)
• EPS secondary to pharmacologic agents are the
most common.
• The risk of developing a drug-induced EPS begins at
the onset of treatment with an offending agent.
• Acutely: within hours or a few days
• Subacutely: over several weeks
• Late or delayed onset: six months or longer afterexposure(tardive)
• short-term therapy of minimal therapeutic dosages
should be the strategy employed
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 8/42
Drug-induced EPS (2)
Five classes of drugs are known to affect central
dopaminergic systems
• Central stimulants:act as indirect dopamine agonist ex.
Amphetamine• Levodopa:a precursor of dopamine
• Direct dopamine agonist:ex. Bromocriptine
•Presynaptic dopamine antagonists: ex. Reserpine
• Antagonize or block central dopamine receptors:
neuroleptics, metoclopramide〈primperam〉
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 9/42
What is Parkinsons?
•Parkinsons is a brain disorder
• Occurs when neurons in a part of the brain called
the substantia niagra die or become impaired
• These neurons produce dopamine
• Use to be called “shaking palsy”
* Dr. James Parkinson first
discovered the disease in 1817
* 1960’s chemical difference in
brain were identified
* 2000 – Michael J. Fox
Foundation

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 10/42
What is Parkinson’s Disease?
• movement disorder
• slowly progressive
• tremor at rest
• Akinesia: inability to
move
• Bradykinesia: slow
movements• postural reflex
impairment
• affects over 1 million
Americans
• Avg. age of onset: 58
• 40% of PD patients
are under age 60
• Decrease in
neurotransmitterdopamine
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 11/42
Pathophysiology
• Normally Dopamine & Ach neurotransmitters worktogether to enable motor neurons to refinevoluntary movement
• Parkinson's results from the degeneration of dopamine-producing nerve cells in the brain,specifically in the substantia nigra and locuscoeruleus
• Clients have lost 80% or more of their dopamine-producing cells by the time symptoms appear

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 12/42
Dopamine
• Neurochemical thatsupports fine motor activity,blood pressure, focus,inspiration, intuition,enthusiasm, and joy, amongother functions.
• Dopamine Agonist: Drugs
that copy the effects of thebrain chemical dopamineand increase the amount of dopamine that is availableto the brain for use.

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 13/42
13

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 14/42
What are the Symptoms of
Parkinsons?
The clinical appearance of Parkinsons is marked by
four cardinal, signs:
• Tremor (or trembling) atrest
• Akinesia and Bradykinesia
• Rigidity
• Postural Instability

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 15/42
In normal conditions
acetylcholine release from the striatum (cholinergic
neurons)is strongly inhibited by dopamine (depleted from
the nigrostriatal neurons).
Joint GABA-ergic neurons then opposite excitatory
function of glutamate neurones connected to the motor
cortex
Neurodegeneration of the dopaminergic neurons
(Subs.nigra)+ loss of dopamine (the striatum) leads to
both hyperactivity of these cholinergic striatal neurons+ blockade of GABA-ergic cells (Subst.nigra). The result is
an increase in excitatory activity of glutamate + the motor
cortex
muscle rigidity, tremor, hypokinesia
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 16/42
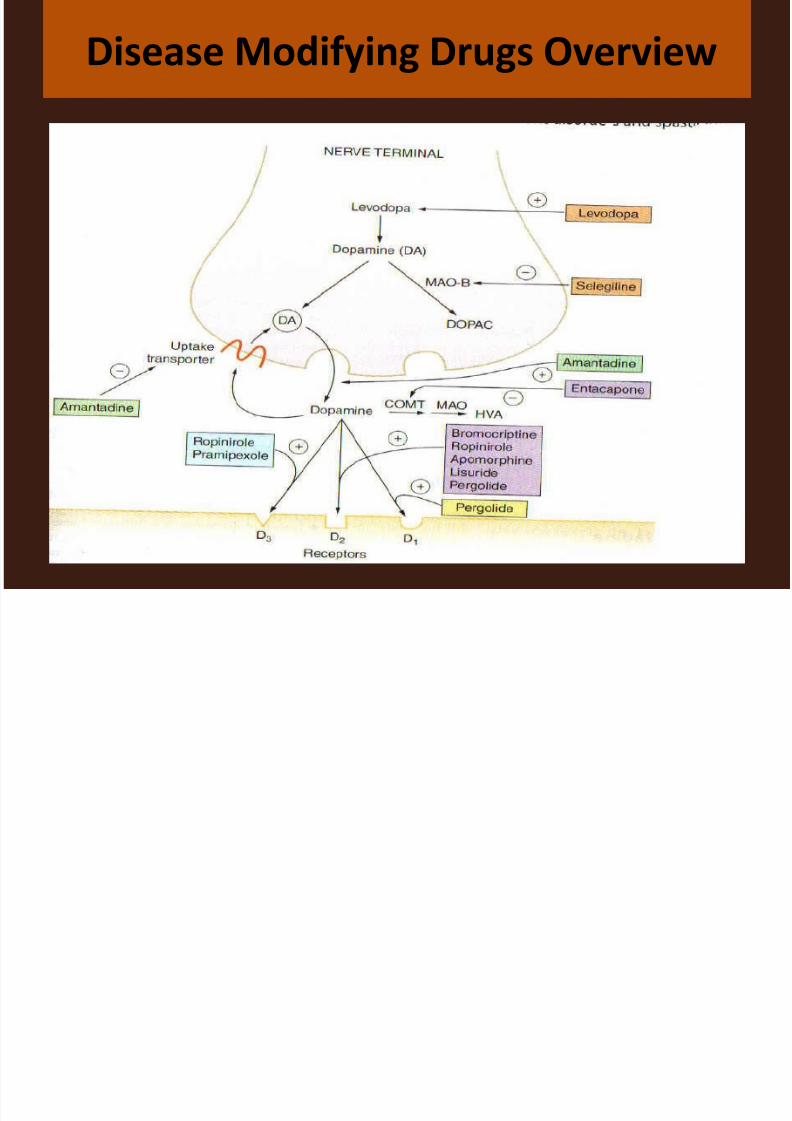
How to treat deficit of dopamine?
A.INCREASE IN DOPAMINERGIC ACTIVITY (1) dopamine precursors (replacement of dopamine)
(2) MAO-B blockade
(3) increase in dopamine release
(4) blockade of amine neuronal reuptake(5) dopamine receptors agonists
B.
How to treat excitatory function of cholinergic and glutaminergic neurons?
MUSCARINIC ACETYLCHOLINE RECEPTOR ANTAGONISTS

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 17/42
Disease Modifying Drugs Overview
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 18/42
How to treat deficit of dopamine?
Levodopa (L-DOPA) the first-line drug
Levodopa dopamine
Dopamine does not penetrate the blood-brain barrier.
DOPA conversion to dopamine in the periphery, which
would cause troublesome adverse effects …… is largely
prevented by the decarboxylase inhibitor.
Since the inhibitor does not penetrate the blood-brain
barrier, decarboxylation occurs rapidly within the brain
(95% of the levodopa dose).
Dopa decarboxylase
(1) dopamine precursors (replacement of dopamine)
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 19/42
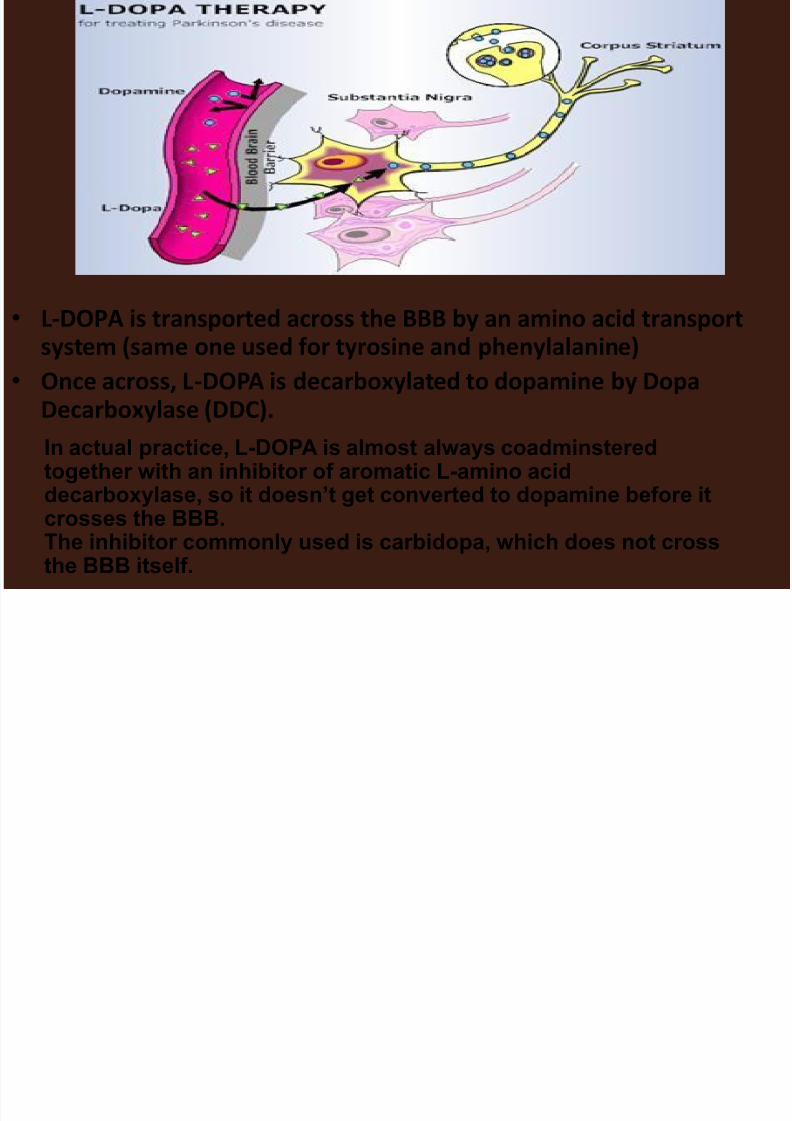
• L-DOPA is transported across the BBB by an amino acid transportsystem (same one used for tyrosine and phenylalanine)
• Once across, L-DOPA is decarboxylated to dopamine by Dopa
Decarboxylase (DDC).In actual practice, L-DOPA is almost always coadminsteredtogether with an inhibitor of aromatic L-amino aciddecarboxylase, so it doesn’t get converted to dopamine before itcrosses the BBB.The inhibitor commonly used is carbidopa, which does not crossthe BBB itself.

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 20/42
How to treat deficit of dopamine?
Levodopa (L-DOPA)
• About 80% of parkinsonian patients show initialimprovement with levodopa, particularly of rigidity and hypokinesia, and about 20% arerestored virtually to normal motor function. Somesymptoms (cognitive decline, dysphagia) are notimproved.
• W i t h t i m e the effectiveness of levodopagradually declines:
= it reflects: the natural progress of disease
+
receptor down-regulation
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 21/42
Levodopa
• A natural amino acid that the brain converts into
dopamine (replacement therapy) used since the
1960’s
• This is an example of a “prodrug”, that is, amolecule that is a precursor to the drug and is
converted to the actual drug at an appropriate
place in the body.
To make it slow release, combined with benserazide
(an enzyme inhibitor) to create co-beneldopa or co-
careldopa (Sinemet)
•
Dose = 50, 100 or 200mg (12.5, 25 or 50mg)

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 22/42
Levodopa (L-DOPA)
• Pharmacokinetics:
– Absorbed by the small intestine by an activetransport system
–Decarboxylation occurs in peripheral tissues (gutwall, liver and kidney
• decrease amount available for distribution – 1% of anoral dose
•
Extracerebral dopamine amounts causing unwantedeffects (benserazide)
– Short half-life

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 23/42
Levodopa (L-DOPA)
Adverse effects (type A)
= dyskinesia - involuntary writhing movements develop in themajority of patients within 2 years of starting levodopatherapy :
• affect the face and limbs
• are dose-dependent (disappear if the dose is reduced)
= ‘on-off ’ effect – rapid fluctuation in clinial state ,where
hypokinesia and rigidity suddenly worsen (for anything froma few minutes to a few hours) and then improve again(probably the fluctuations reflect the changing plasma
levodopa concentration) = Others:
• nausea and anorexia, hypotension,
• by increase dopamine activity in the brain----schizophrenia-like syndrome with delusions and hallucinations
• confusion, disorientation, insomnia (in 20% of patients)

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 24/42
How to treat deficit of dopamine?
INCREASE IN DOPAMINERGIC ACTIVITY
(1) dopamine precursors (replacement of dopamine)
(2) MAO-B blockade(3) increase in dopamine release
(4) blockade of amine neuronal reuptake
(5) dopamine receptors agonists
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 25/42
Disease Modifying Drugs Overview
H t t t d fi it f d i ?

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 26/42
How to treat deficit of dopamine?
Ad.2 MAO-B blockade • Dopamine is oxidized by monoamine oxidase B
(MAO-B).
• MoA: prolongs the effects of levodopa as MAO-Bdegrades dopamine
Pharmacokinetics:= completely absorption, short half-life
Adverse effects:= N, V, Dia, Constipation; dry mouth, sore throat;
transient dizziness; insomnia, confusion andhallucinations
Early stage – prescribed on it is own to delay need for levodopa and there is good evidence for its slowing
down of PD progression
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 27/42
How to treat deficit of dopamine?
Ad.2 MAO-B blockade
MAO-B inhibition:
• protects dopamine from intraneuronal degradation
• lacks the adverse peripheral effects of non-selective MAO -
Inhibitors used to treat depression• does not provoke the ‘cheese reaction’
• Selegiline
a selective inhibitor for MAO-B, which predominates in
dopamine containing regions in the CNS
Combination of levodopa + selegilin is more effective
in relieving symptoms and prolonging life

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 28/42
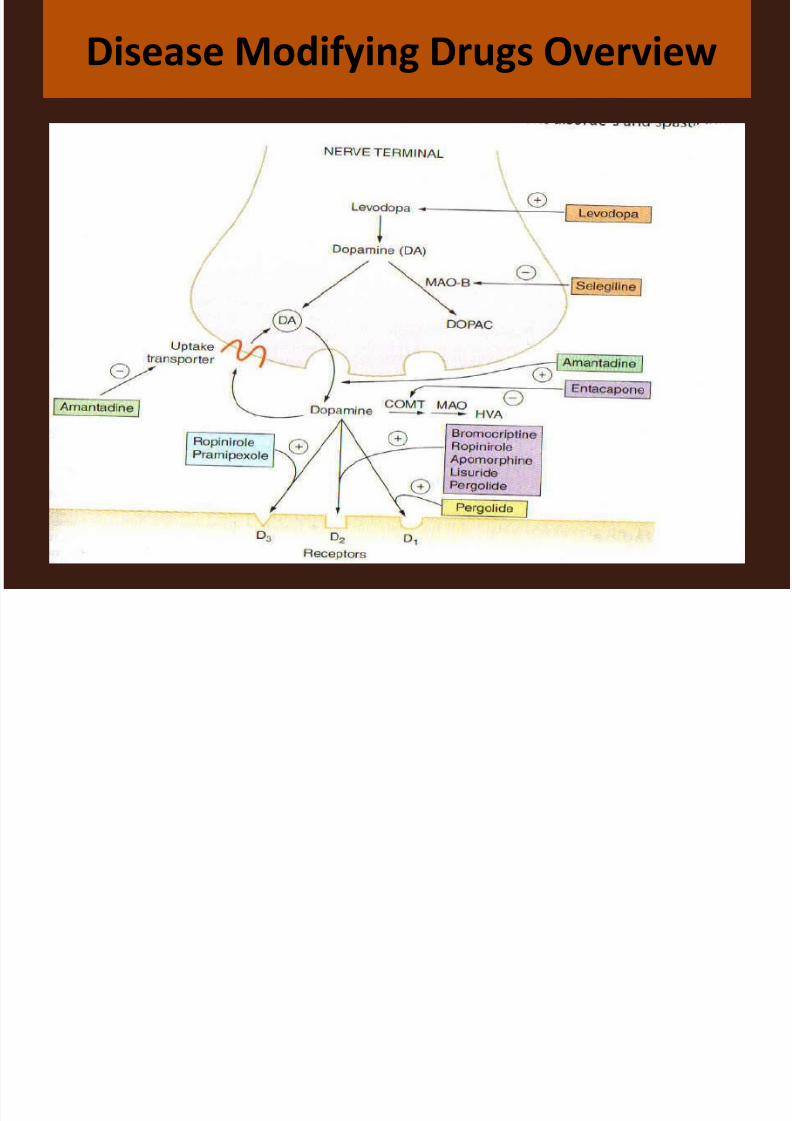
How to treat deficit of dopamine?
INCREASE IN DOPAMINERGIC ACTIVITY
(1) dopamine precursors (replacement of dopamine)
(2) MAO-B blockade
(3) increase in dopamine release(4) blockade of amine neuronal reuptake
(5) dopamine receptors agonists
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 29/42
Disease Modifying Drugs Overview
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 30/42
ad. dopamine receptors agonists-
a.increase in dopamine release-b. blockade of amine neuronal reuptake
potent agonists at dopamine D2 receptors in the CNS:
= bromocriptine derived from the ergot alkaloids
- lisuride and pergolide
= amantadine :
- increases dopamine release,
- activates D2 receptors
- less active, more tolerated
How to treat deficit of dopamine?

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 31/42
Dopamine receptor Agonists
• Dopamine agonists mimic dopamine's function in
the brain.
• They are used primarily as adjuncts to
levodopa/carbidopa therapy.
• They can be used as monotherapy but are generallyless effective in controlling symptoms, with Side
effects similar to those produced by levodopa
- Bromocriptine (Parlodel®)- Pergolide (Permax®)- Pramipexole (Mirapex ®)
-Ropinirole (Requip®)-Apomorphine
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 32/42
Dopamine receptor agonists
• Apomorphine (APO-go):
– SC administration
– Rescue therapy – rapid onset with a short
duration of action (~50mins)• Bromocriptine (Parlodel); Pergolide (Celance);
Ropinirole (Requip)
•
Direct agonists of dopamine receptors in thebrain
– ?longer lasting therapeutic effects that Levodopa

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 33/42
Dopamine receptor agonists
• Adverse effects:
– Use gradual dose titration
– Nausea+ Vomitting (particularly Apomorphine)
– Dyskinesia
– Hallucinations and confusion
– Peripheral vasospasm (Raynaunds)
– Respiratory depression (Apomorphine
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 34/42
COMT (Catechol-O-Methyl Transferase Inhibitors )
• These new class of Parkinson's medications
augment levodopa therapy by inhibiting the COMT
enzyme, which metabolizes levodopa before it
reaches the brain.
• Inhibiting COMT increases the amount of levodopa
that enters the brain.
•
These drugs are only effective when used withlevodopa
- Entacapone (Comtan®)- Tolcapone (Tasmar®)

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 35/42
Catechol-O-methltransferase inhibitors –
(COMT-I)
– MoA: inhibits the breakdown of levodopa
– Pharmacokinetics: variability of absorption,
extensive first-pass metabolism, short half-life
– Adverse effects: dyskinesias, hallucinations; N, V,
Dia and abdominal pain
–
New combination – Levodopa/carbidopa/entacapone (Stalevo) as 1
tablet (50, 100, 150mg
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 36/42
Amantadine (Symmetrel)
• Originally an antiviral drug, now used as conjunctive therapy fordyskinesis effects produced by Levodopa
• MoA:
– stimulates/promotes the release of dopamine stored in the
synaptic terminals – Reduces reuptake of released dopamine by pre-synaptic
neuron
• Pharmacokinetics:
–
Well absorbed, long half-life, excreted unchanged by thekidney
• Adverse effects:
– Not many
– Ankle oedema, postural hypotension, nervousness,insomnia, hallucinations (high dose)
H i f i f h li i

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 37/42
How to treat excitatory function of cholinergic
and glutaminergic neurons?
Anticholinergics
= reduce the relative overactivity of the
neurotransmitter acetylcholine to balance the
diminished dopamine activity.= This class of drugs is most effective in the
control of tremor, and they are used as adjuncts to
levodopa.
= Side effects associated with anticholinergic
drugs include dry mouth, blurred vision,
constipation, and urinary retention
A ti i i /A ti h li i D
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 38/42
Antimuscarinic/Anticholinergic Drugs:
– Trihexyphenidyl (Broflex, Artane, Agitane);
Benztropine (Cogentin); Orphanadrine (Disipal);
Procycline (Kemadrin, Arpicolin)
–Less common drugs but they affect Ach basedinteractions
– MoA: blocking cholinergic (Ach) receptors to
restore balance
– Pharmacokinetics: fairly well absorbed, extensive
hepatic metabolism, intermediate to long half-lifes
– Adverse effects: dry mouth and confusion
7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 39/42
Symptom Management Drugs
• PD is multidimensional, therefore there are a
number of clinical presentations that require
supplementary agents
– Drug-Drug reactions is the problem
– Major area is depression

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 40/42
Antidepressants
• Amitriptyline (Tryptizol), imipramine (Tofranil),
Nortriptyline (Allegron), Iofepramine (Gamanil)
• MoA: block re-uptake of noradrenaline and
serotonin => Sedative actions, can help withdrooling and loss of appetite
• Adverse effects: sleepiness, dry mouth, increased
hunger, cardiac arrhythmias and changes in BP
• Can interfere with the effects of levodopa!

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 41/42
Other Drugs to Avoid
Generic Name Brand Name Prescribed for
Prochlorperazine Stemetil N +V, Dizziness
Prephenazine Triptafen Depression
Flupentixol Fluanxol/Depixol Confusion,
Hallucinations
Chlorpromazine Largactil“
Pimozide Orap “
Sulpiride Dolmatil “

7/27/2019 K.14 NewBMS 2011,Pharmacology of Extrapyramidal Disorders
http://slidepdf.com/reader/full/k14-newbms-2011pharmacology-of-extrapyramidal-disorders 42/42
Thank you


![PHARMACOLOGY GASTROINTESTINAL DISORDERS Dr. Marwa Shaalan [ Pharm.D]](https://static.documents.pub/doc/80x56/56649f515503460f94c74e41/pharmacology-gastrointestinal-disorders-dr-marwa-shaalan-pharmd.jpg)














