35
Kaley Luna, Montana McGuire, Emily Miller and Britney Morgan Coronary Artery Disease
| Date post: | 02-Jan-2016 |
| Category: |
Documents |
| Upload: | victor-moody |
| View: | 34 times |
| Download: | 0 times |

Kaley Luna, Montana McGuire, Emily Miller and Britney Morgan
Coronary Artery Disease
Introduction• The purpose of this case management project was to provide
information about coronary artery disease (CAD) on Lee County
residents and to describe how these complications can be
prevented
• This project provides information about Lee County and the health
statistics related to it, follows a CAD patient through the disease
management process, describes how CAD patients are managed
after being discharged from the acute care setting, and describes
a community intervention program that can help prevent further
complications associated with CAD
Learner Objectives• To know the effects of
coronary artery disease (CAD) on Lee County residents
• To be able to describe how complications of CAD can be prevented
• To know what exercise training is and how it can help prevent complications from CAD

Lee County Demographics
• The total population was 133,010 in 2008• 98,000 were Caucasian (74%)• 35,000 were African American or
another race (26%)• 11,843 were over the age of 65
(9%)• In 2008, the average life expectancy
at birth was 77.3 years• 842 deaths occurred in 2008
• Total death rate = 6.3 per 1,000 people

Lee County Health Statistics
• In 2008, 209 deaths were due to cardiovascular disease (total death rate = 157.1 per 100,000 people)• Caucasian death rate = 154.9 per
100,000 people• African American death rate =
163.4 per 100,000 people• Male death rate = 154.9 per
100,000 people• Female death rate = 159.4 per
100,000 people

Alabama Health Statistics • Alabama has the fourth highest
death rate from cardiovascular disease in the nation
• In 2008. . .– The total population was
4,661,900– 47,601 deaths occurred– Cardiovascular disease was the
cause of 12,091 of those deaths• Total death rate = 259.4 per
100,000 people
United States Health Statistics
• Over 81 million adults have one or more types of cardiovascular disease– Over 17 million of these have coronary artery disease
• In 2006, 1 out of every 6 deaths was due to coronary artery disease
• Lifetime cardiovascular disease incidence rates for Americans greater than 40 years of age– Two in three for men– One in two for women
• In 2007, 616,067 people died from heart disease– Total death rate = 204.3 per 100,000 people

Cardiovascular Disease Mortality
• The Healthy People 2010 target rate of deaths from cardiovascular disease = 166 deaths per 100,000 people
Lee County Alabama United States Healthy People 2010 Goal0
50
100
150
200
250
300
Cardiovascular Disease Mortality Rates
Mor
talit
y Ra
te p
er 1
00,0
00 p
eopl
e
Graph 1.0

Community Resources
• East Alabama Medical Center– Cardiology department
• 11 cardiologists on staff• 9 outreach clinics in 5 counties
– Cardiac catheterization laboratory– Cardiac and thoracic surgery– Cardiopulmonary rehabilitation
program• Nurses, dieticians, exercise
physiologists

Community Nursing Diagnoses
• At risk of complications from coronary artery disease among the population of Lee County related to noncompliance with the recommended rehabilitation program after discharge from an acute care setting
• At risk of coronary artery disease among the population of Lee County related to approximately 23% of the population being African American
• At risk of coronary artery disease among the population of Lee County related to 9% of the population being over 65 years of age
The patient is a retired sixty-one year old African American male from
Lee County, Alabama. He is 66 inches tall, 82.2 kilograms in weight with a
body surface area (BSA) of 1.92 and a body mass index (BMI) of 29.
His medical history consists of significant CAD, hypercholesterolemia, insulin dependent
diabetes mellitus, hypertension, and peripheral neuropathy. He is not sure of his family
history but believes his mother had heart disease. The patient denies using tobacco
products or illicit drugs but has drank beer on occasion.
Patient History

• His medical record states that he experienced a myocardial infarction in the year 2000. In 2008, a cardiac stress test was performed. The test results were normal with an ejection fraction of 55 percent.
• Medications between 2008 and present:– Coreg– Aspirin– Plavix– Hydrochlorothiazide– Terazosin– Simvastatin– Lotrel– Vasotec
Patient History
Patient History
• Over the past few months he has been experiencing atypical chest pain, nonexertional in nature, with some
radiation across his chest from left to right. Another stress test was performed and was found to be
abnormal which led doctors to do a cardiac catheterization procedure. Angiographic findings showed left main luminal disease, 75-80 percent
blockage in the left anterior descending artery and right coronary artery. His ejection fraction is now 25-30
percent. From these findings doctors agreed that it was necessary to perform a CABG.

Patient History
• The CABG was performed on September 2, 2010, and he was admitted to the cardiovascular intensive care unit after surgery (CVICU). Following a full recovery in the CVICU and a short stay on the step-down unit, the patient was discharged home.

American Heart AssociationCAD Practice Guidelines
• BP 140/90 mmHg or less• LDL Cholesterol 100 mg/dl• Smoking cessation counseling• Anti-platelet therapy• Diabetes management (Hb A1c <7%)
• Renin-angiotensin-aldosterone system blocker
• Beta-blocker therapy

Smoking Cessation
“Epidemiologic evidence clearly links smoking with adverse outcomes in
patients who manifest coronary heart disease. Patients who continue to
smoke after experiencing a myocardial infarction have a 50% higher risk of recurrent coronary events compared to non-smokers” (Mohiuddin et al.,
2007)

Treatment Guidelines
• The American Heart Association established guidelines for the secondary prevention of CAD.
• The following are the AHA’s guidelines:• Maintain a blood pressure reading less than 140/90 mmHg or less
than 130/80 mmHg if the pt. has a chronic kidney disease or diabetes
• A LDL cholesterol of <100 mg/dl• Smoking cessation counseling• Anti-platelet therapy• Diabetes management • Renin-angiotensin-aldosterone system blocker therapy• Beta-blocker therapy

Cost Analysis
Hospital Charges$3,493
$2,638.46
$2,355.93
$9,538.80
$2,257.00
$7,032.50
$701.00
$1,102.00
Total Room Charges
Total Pharmacy
Total Drugs
Total Supplies
Total Laboratory
Total OR Services
Total Anesthesia
Total Respiratory

Case Management• Case management is
important in CAD patients to ensure that they are receiving proper treatment and follow-up appointments with their physicians.
• Case management can help a patient find the right community treatment program to meet their needs.
• Case managers can be the missing puzzle piece!

Community Treatment Options for Patients with CAD
• Cardiac Rehabilitation– Available in Lee
County through East Alabama Medical Center
• Home Health Services– Available in Lee
County through services such as Alacare Home Health Services

Community Intervention Program
Exercise Training and Coronary Artery Disease
Gibralta Masonic Lodge #173November 9, 2010

Literature Review
• Three systematic reviews were analyzed in order to develop this community intervention program
The reviews showed that exercise training slows the progression of CAD and can reduce the morbidity and mortality associated with CAD by improving exercise capacity, reducing overweight and obesity, and reducing cholesterol levels

Purpose Objectives
• To provide patients with CAD with information regarding the possible benefits of ET programs on preventing complications and progression of CAD
• Identify learning needs and risk factors of participants
• Provide participants with an overview of coronary artery disease
• Describe the benefits of ET programs
• Explain how participants can incorporate an ET program into their lives
• Provide participants with a list of current ET gyms and walking trails in Lee County

Teaching Strategies• Participants were asked to take a
short quiz about their learning needs and risk assessment
• Participants also received a handout that summarized our teaching
• After the presentation, participants completed an evaluation of the community intervention program

Physical Activity Heart Health Quiz
Patient Teaching Handout

Patient Teaching ContentCoronary artery disease (CAD) is a condition in which the coronary arteries, the vessels that supply the heart with blood, become damaged. Plaque, which is made up of cholesterol-containing deposits, is usually the cause of CAD. As plaque builds up in the coronary arteries, less blood is allowed through them. This causes the heart to receive less blood and oxygen. Over time, this decreased amount of blood flow can cause chest pain and shortness of breath. When plaque completely blocks a coronary artery, a heart attack can happen.

• Risk Factors:– Positive family history of
CAD– Smoking– High blood pressure– High cholesterol– Physical inactivity– Overweight and obesity– Poor diet– Diabetes
• Modifiable risk factors are things that can be changed such as overweight, obesity, and smoking
• Non-modifiable risk factors are things that cannot be changed such as heredity and age
• Although leading a sedentary lifestyle has been identified as one of the major modifiable risk factors for cardiovascular disease, nearly seventy percent of adults in the United States lead a sedentary lifestyle or are considered relatively inactive

Exercise Training• Exercise training (ET) is a “planned,
structured, and repetitive bodily movement done to improve or maintain one or more components of physical health”
• Participants in formal ET programs have had reductions in BMI, body fat percentage, blood pressure, cholesterol, and inflammation
• ET has been identified as a valuable way to prevent further complications from CAD because it helps slow the progression of vascular disease
• ET programs have also been shown to reduce subsequent hospitalization costs associated with CAD morbidity
Exercise Prescription• ET programs are composed of four
different factors: mode of activity, frequency, duration, and intensity– Aerobic forms of ET include walking,
jogging, swimming, stair climbing, cycling, aerobic dance, and using elliptical trainers
– Resistance forms of ET include using hand weights, weight machines, and elastic bands
– ET should be performed for at least thirty minutes per day at least five times per week, preferably six to seven times per week
– ET should consist of a moderate level of intensity
Exercise Training in Lee County• The city of Auburn has six walking
trails available for public use. The trails range from one fourth of a mile to two and one fourth miles. Use of these trails is free to the public.
The city of Opelika has an indoor walking track and pool at the Opelika SportsPlex. The cost for use of these two facilities is 60 dollars per person each year
• The Chewacla State Park, located in Auburn, also has an array of walking and biking trails. These trails range from one fifth of a mile to one and two-fifths miles. The intensity of the trails ranges from easy walking to moderately difficult hiking. Entrance into the Chewacla State Park costs two dollars per person on weekdays and three dollars per person on weekends
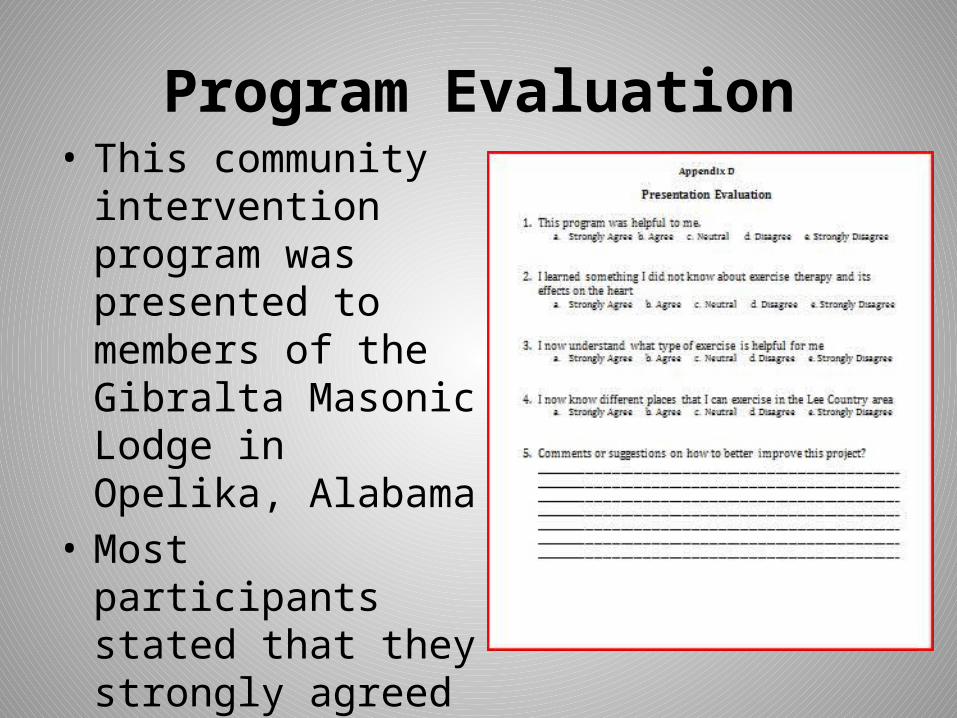
Program Evaluation• This community
intervention program was presented to members of the Gibralta Masonic Lodge in Opelika, Alabama
• Most participants stated that they strongly agreed with each statement

Conclusion• What is CAD?
CAD is a condition in which the coronary arteries become damaged by plaque buildup. This causes the heart to receive less blood and oxygen.
• What are the complications of CAD?
Chest pain, shortness of breath, heart attack
• How can complications of CAD be prevented?Exercise at least 30 minutes a day, most days of the week. Consume a healthy diet.
ReferencesAlabama Department of Conservation and Natural Resources. (2010). Retrieved from http://www.alapark.com/chewacla/Alabama Department of Public Health. (2010). Retrieved from http://www.adph.org/healthstats/assets/chp08.pdfAlacare. What is home health care?. Retrieved from http://www.alacare.com/what-is-home-health-careAmerican Heart Association. (2010). Heart Disease and Stroke Statistics 2010 Update: A Report From the American Heart Association [Date file]. Retrieved from: http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.109.192667Artham, S., Lavie, C., Milani, R., Chi, Y., & Goldman, C. (2008). Benefits of Exercise Training in Secondary Prevention of Coronary and Peripheral Arterial Disease. Vascular Disease Prevention, 5(3), 156-168. Retrieved from Academic Search Premier database.Centers for Disease Control and Prevention. (2010). Retrieved from http://www.cdc.gov/nchs/fastats/heart.htmCity of Auburn Parks and Recreation Department. (2010). Retrieved from http://www.auburnalabama.org/parks/Default.aspx?PageID=626City of Opelika Parks and Recreation Department. (2010). Retrieved from http://www.opelika.org/Default.asp?ID=455East Alabama Medical Center. (2010). Retrieved from http://www.eamc.orgFung Ping, L., Lai Ming, Y., Laher, I., Xiaoqiang, Y., Zhen Yu, C., & Yu, H. (2008). Exercise, Vascular Wall and Cardiovascular Diseases. Sports Medicine, 38(12), 1006-1024. Retrieved from Academic Search Premier database.Healthy People 2010. (2010). Retrieved from http://www.healthypeople.gov/Document/HTML/Volume1/12Heart.htmKaralis, D. (2009). Intensive lowering of low-density lipoprotein cholesterol levels for primary prevention of coronary artery disease. Mayo Clinic Proceedings, 84(4), 345-352. Retrieved from Academic Search Premier database. Lavie, C., Thomas, R., Squires, R., Allison, T., & Milani, R. (2009). Exercise Training and Cardiac Rehabilitation in Primary and Secondary Prevention of Coronary Heart Disease. Mayo Clinic Proceedings, 84(4), 373-383. Retrieved from Academic Search Premier database.Lee County. (2005). Retrieved from http://www.leeco.us/contact_us/index.htmlMayoClinic.com. (2010). Coronary artery disease. Retrieved from http://www.mayoclinic.com/health/coronary-artery-disease/DS00 Mohiuddin, S., Mooss, A., Hunter, C., Grollmes, T., Cloutier, D., & Hilleman, D. (2007). Intensive smoking cessation intervention reduces mortality in high-risk smokers with cardiovascular disease. CHEST, 131(2), 446-452. doi:10.1378/chest.06-1587. PayScale. (2010). Hourly rate snapshot for registered nurse (RN) jobs. Retrieved from http://www.payscale.com/research/US/Job=Registered_Nurse_(RN)/Hourly_RateSmith, S.C., Allen, J., Blair, S.N., Bonow, R.O., Brass, L.M., Fonarow, G.C., Taubert, K.A. (2006). AHA/ACC Guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update. Journal of the American Heart Association. doi:10.1161/CIRCULATIONAHA.106.174516Sole, M.L., Klein, D.G., Moseley, M.J. (2009). Cardiovascular alterations. In M. Iannuzzi & J. Ehlers (Eds.), Introducation to Critical Care Nursing (pp. 343). St. Louis, MO: Saunders. SugeryPlanet. (2006). Retrieved from http://www.surgeryplanet.com/left/find-cost.htmlU.S. Census Bureau. (2010). Retrieved from http://quickfacts.census.gov/qfd/states/01/01081.html

















