44
The Nordic Cochrane Centre Helbredstjek til raske Karsten Juhl Jørgensen Seniorforsker, dr.med. The Nordic Cochrane Centre
The Nordic Cochrane Centre
Helbredstjek til raske
Karsten Juhl Jørgensen Seniorforsker, dr.med.
The Nordic Cochrane Centre

The Nordic Cochrane Centre

The Nordic Cochrane Centre
Kommercielle helbredstjek i DK
• Gennemgik 56 websites som tilbød helbredstjek.
• “None of the websites quantified the expected benefit of screening or provided information on possible risks and harms. The majority of the tests offered (81%) were either recommended against, or there was a lack of evidence or recommendations.”
Larsen CG, Jørgensen KJ, Gøtzsche PC. Regular health checks: cross-sectional survey. PLoS ONE 7(3): e33694. doi:10.1371/journal.pone.0033694

The Nordic Cochrane Centre
Wilson og Jungner 19681
“In theory, screening is an admirable method of combating disease … [but] in practice, there are snags. The central idea of early disease detection and treatment is essentially simple. However, the path to its successful achievement (on the one hand, bringing to treatment those with previously undetected disease, and, on the other, avoiding harm to those persons not in need of treatment) is far from simple though sometimes it may appear deceptively easy.”
1. Wilson JMG, Jungner G. Principles and practice of screening for disease. Geneva: WHO; 1968. Available from: http://www.who.int/bulletin/volumes/86/4/07-050112BP.pdf

The Nordic Cochrane Centre
Wilson og Jungner kriterier (WHO)1
1. The condition sought should be an important health problem. 2. There should be an accepted treatment for patients with recognized disease. 3. Facilities for diagnosis and treatment should be available. 4. There should be a recognizable latent or early symptomatic stage. 5. There should be a suitable test or examination. 6. The test should be acceptable to the population.
7. The natural history of the condition, including development from latent to declared disease, should be adequately understood. 8. There should be an agreed policy on whom to treat as patients. 9. The cost of case-finding (including diagnosis and treatment of patients diagnosed) should be economically balanced in relation to possible expenditure on medical care as a whole. 10. Case-finding should be a continuing process and not a “once and for all” project.
1. Wilson JMG, Jungner G. Principles and practice of screening for disease. Geneva: WHO; 1968. Available from: http://www.who.int/bulletin/volumes/86/4/07-050112BP.pdf

The Nordic Cochrane Centre
”Udviddede WHO kriterier”1
1. The screening programme should respond to a recognized need. 2. The objectives of screening should be defined at the outset. 3. There should be a defined target population.
4. There should be scientific evidence of screening programme effectiveness. 5. The programme should integrate education, testing, clinical services and programme management. 6. There should be quality assurance, with mechanisms to minimize potential risks of screening. 7. The programme should ensure informed choice, confidentiality and respect for autonomy. 8.The programme should promote equity and access to screening for the entire target population. 9. Programme evaluation should be planned from the outset.
10. The overall benefits of screening should outweigh the harm.
1. http://www.who.int/bulletin/volumes/86/4/07-050112/en/
The Nordic Cochrane Centre
UK National Screening Committee1
“There should be evidence from high quality Randomised Controlled Trials that the screening programme is effective in reducing mortality or morbidity.“
1. http://www.screening.nhs.uk/criteria

The Nordic Cochrane Centre
Er der overhovedet brug for randomiserede forsøg?
• Sygdommene og deres relaterede risikofaktorer er grundigt studerede.
• Der findes veldokumenterede forebyggende behandlinger for mange tilstande
• Er det ikke godt nok?

The Nordic Cochrane Centre Pharoah P, Professor of Cancer Epidemiology, Univ. of Cambridge.
Red line: women screened for breast cancer Green line: non-screened women
Total mortality
The Nordic Cochrane Centre
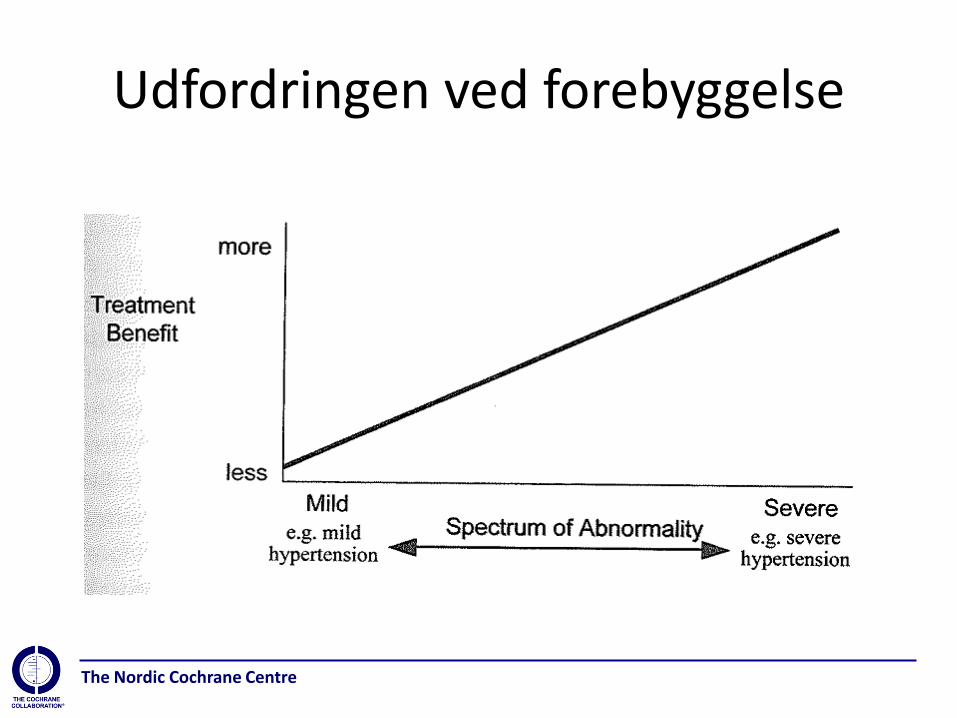
Udfordringen ved forebyggelse

The Nordic Cochrane Centre
Ændring i for behandlingsmål kolesterol
200 mg/dL svarer ca. til 5 mmol/L

The Nordic Cochrane Centre
Formål
At kvantificere gavnlige og skadelige virkninger ved helbredstjek, med hovedvægt på patientrelevante outcomes som morbiditet og mortalitet.

The Nordic Cochrane Centre
Kriterier for valg af studier
• Randomiserede forsøg som sammenlignede helbredstjek med ingen helbredstjek
• Voksne (>18 år), men screeningstudier i geriatriske populationer ekskluderedes
• Uselekterede for sygdom og risikofaktorer
• Helbredstejk defineret som screening for sygdom eller risikofaktorer i mere end ét organsystem vha. mere end én test

The Nordic Cochrane Centre
Primære outcomes
• Total mortalitet
• Sygdomsspecifik mortalitet

The Nordic Cochrane Centre
Sekundære outcomes
• Morbiditet • Nye diagnoser • Indlæggelser på hospital • Selv-rapporteret helbred • Antal henvisninger til specialist • Antal ikke-planlagte besøg hos praktiserende læge • Antal ekstra diagnostiske undersøgelser pga. Positive screeningtests • Udskrivning af ny medicin og brug af kirurgisk behandling • Sygefravær fra arbejde
The Nordic Cochrane Centre
Resultater
• 16 trials
• 2 trials publicerede aldrig resultater, 1 trial først efter reviewet.
• 14 trials blev inkluderet
– 232.659 deltagere
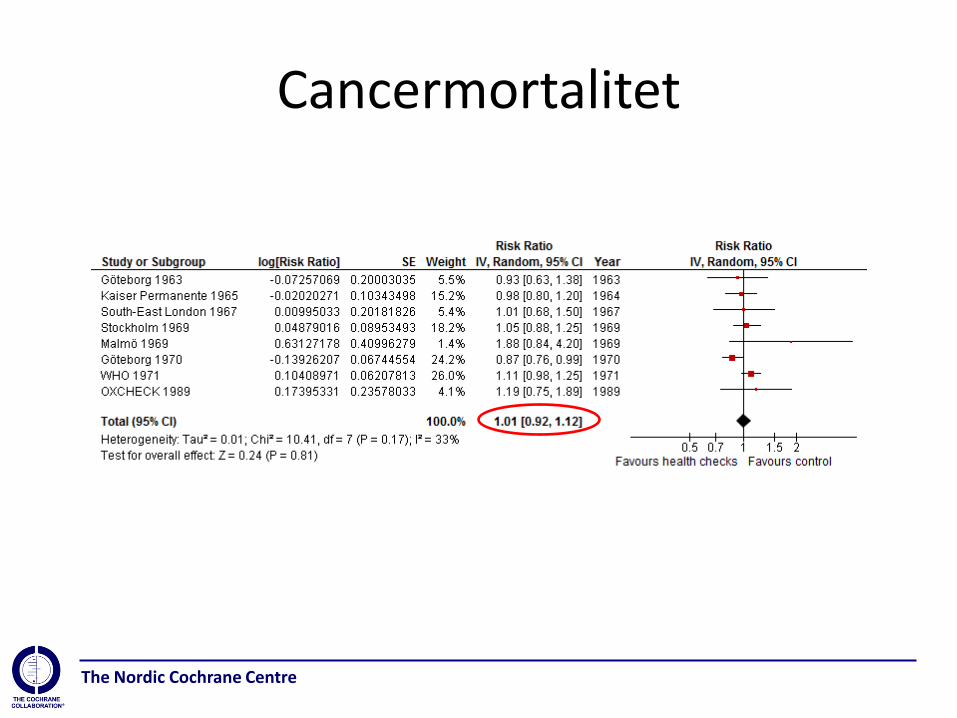
• 9 trials reporterede mortalitetsdata
– 11.940 dødsfald blandt 155.899 deltagere

The Nordic Cochrane Centre
Total mortalitet

The Nordic Cochrane Centre
Kardiovaskulær mortalitet
The Nordic Cochrane Centre
Cancermortalitet
The Nordic Cochrane Centre
Skadevirkninger
• Dårligt rapporteret.
• Et trial fandt en 20% stigning i det gennemsnitlige antal diagnoser på 6 år
• Ingen trials undersøgte det totale antal nye recepter, operationer, opfølgende undersøgelser eller henvisninger.
• Nogle trials fandt et øget forbrug af antihypertensiva, andre ikke.

The Nordic Cochrane Centre
Hvorfor fandt vi ingen effekt?
• Lav kontrast mellem grupperne?
– Lav deltagelse?
– ”forurening” af kontrolgruppen i visse trials?
• Virkede interventionen ikke?
– Selvselektion af deltagere?
– Screening for sygdom er mindre effektivt end vi troede?
– Lille risiko for skade opvejer lille chance for gavn?
– Er studierne for gamle?

The Nordic Cochrane Centre

The Nordic Cochrane Centre
Inter99
Screening for risikofaktorer for iskæmisk hjertesygdom (IHD) efterfulgt af gentagne livsstilssamtaler; 10 års opfølgning. 13,016 inviterede; 48,625 kontrolpersoner; 3,238 døde Hazard ratioer: IHD = 1.04; 95% CI 0.94–1.14 stroke = 0.99; CI 0.88–1.11 Kombinerede endpoints = 1.01; CI 0.93–1.09 Total mortalitet = 0.98; CI 0.90–1.08

The Nordic Cochrane Centre
Mulige problemer
• Screeningen – opfølgende undersøgelser? – sygeliggørelse? – psykiske skadevirkninger? – ’certificate of health’ effekt?
• Populationen – anderledes effekter af lægemidler i praksis end i de
farmakologiske forsøg? – anderledes balance mellem gavnlige og skadelige
virkninger? – anderledes compliance? – mindre absolut risiko?

The Nordic Cochrane Centre
Skærmklip taget: 08-05-2012; 08:07
Skærmklip taget: 08-05-2012; 09:48

The Nordic Cochrane Centre

The Nordic Cochrane Centre

The Nordic Cochrane Centre
Helbredstjek til lavtuddannede mænd
Sundhedsminister Nick Hækkerup: ”Jeg føler mig overbevist om, at hvis vi gør det her fornuftigt og rigtigt, vil folk også komme til at leve længere” Det er der jo bare ikke nogen evidens for? ”Nu er jeg jo heller ikke videnskabsmand, jeg er politiker.” Du må vel støtte dig op ad videnskaben? ”Næh… jeg er jo holdningsmenneske”
Politiken 19. august 2014

The Nordic Cochrane Centre
WHO-studiet (1971)
• 60.000 mænd ansat på 80 fabrikker, 5-6 års opfølgning.
• Blodtryk, kolesterol, vægt, spørgeskema om livsstilsfaktorer.
• Ingen effekt på total, kardiovaskulær eller kræftdødelighed.

The Nordic Cochrane Centre
NHS health check - 2009
• Højde, vægt
• Blodtryk
– højt: undersøg nyrefunktion
• Kolesterol
• Diabetes risiko
– høj: blodsukker
Livsstilsrådgivning
The Nordic Cochrane Centre
WE ESTIMATE THAT THIS PROGRAMME WILL:
• And each year will prevent at least:
– 9,500 heart attacks and strokes
– 2,000 deaths
– 4,000 people developing diabetes
Prevention figures are cautious estimates based only on known effective management applied to those at high risk
• Offer 3m vascular checks a year
• Cost about £250m before savings
The Nordic Cochrane Centre
POTENTIAL GAINS
1) Sustain gains in life expectancy otherwise at risk
2) Prevent significant illness and premature death
3) Avoid additional NHS acute service use and cost
4) Real opportunity to address inequalities at source

The Nordic Cochrane Centre
"I don't want the truth, I want something I can tell Parliament!"
NHS Diabetes and Kidney Care and the Department of Health published an eBulletin, “Response to the Cochrane review,” on the NHS Health Check programme’s website. It looks like serious criticism of our work, but it is unfounded and misleading.
We sent a response to the eBulletin to the national director of NHS Diabetes and Kidney Care and asked for it to be published on the website, but this was declined. The NHS letter stated that government had already decided that “NHS Health Checks will be carried out as a national priority,” that the website is not a forum for debating the merits of such checks, and that “there are other more appropriate places to discuss government policy.”
Why then did the programme publish its criticism on its website and not in a scientific journal?
Krogsbøll et al., BMJ 2013;347:f5227

The Nordic Cochrane Centre
20 Aug 2013
Interview and Letter by Krogsbøll et al.

The Nordic Cochrane Centre

The Nordic Cochrane Centre

The Nordic Cochrane Centre

The Nordic Cochrane Centre

The Nordic Cochrane Centre
Forslag til helbredstjek i DK
• Anamnese
• Højde, vægt, hofte og taljemål
• Blodtryk
• Kolesterol
• Blodsukker
• Spirometri
– kun rygere og folk med symptomer

The Nordic Cochrane Centre
Kommercielle helbredstjek i DK
• Gennemgik 56 websites som tilbød helbredstjek.
• “None of the websites quantified the expected benefit of screening or provided information on possible risks and harms. The majority of the tests offered (81%) were either recommended against, or there was a lack of evidence or recommendations.”
Larsen CG, Jørgensen KJ, Gøtzsche PC. Regular health checks: cross-sectional survey. PLoS ONE 7(3): e33694. doi:10.1371/journal.pone.0033694

The Nordic Cochrane Centre
Hvad med livsstilsændringer?
• Cochrane review
– 14 forsøg, 139,256 deltagere
• Generelle befolkninger
– ingen (målbar) effekt på total eller kardiovaskulær dødelighed
• Hypertension eller diabetes
– gavnlige effekter på dødelighed
Ebrahim S, Taylor F, Ward K, Beswick A, Burke M, Davey Smith G. Multiple risk factor interventions for primary prevention of coronary heart disease. Cochrane Database of Systematic Reviews 2011, Issue 1. Art. No.: CD001561.
The Nordic Cochrane Centre
Sammenhæng mellem blodtryk og dødelighed.
• Beta-blokkere reducerer blodtrykket med 11/6 mmHg. • ”Total mortality was not significantly different between beta-blockers and placebo (RR 0.99, 95%CI 0.88 to 1.11; I2=0%)” •“Total cardiovascular disease (CVD) was lower for beta-blockers compared to placebo (RR 0.88, 95%CI 0.79 to 0.97; I2=21%). This is primarily a reflection of the significant decrease in stroke (RR 0.80, 95%CI 0.66 to 0.96; I2=0%), since there was no significant difference in coronary heart disease (CHD) between beta-blockers and placebo.
Wiysonge CS, Bradley HA, Volmink J, Mayosi BM, Mbewu A, Opie LH. Beta-blockers for hypertension. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD002003.

The Nordic Cochrane Centre
Hvem deltager i helbredstjek?
• Pill et al (1988) inviterede 1570 mænd og kvinder i alderen 20-45 til helbredstjek hos deres læge.
• De konkluderede: ”Offering cohorts of patients additional screening services is unlikely to be efficient or effective since it is the low-risk people already known to the doctor who are most likely to attend”.

The Nordic Cochrane Centre
Behandling af mild hypertension (140-159/90-99 mmHg)
•4 RCTs included with 8,912 participants. Treatment for 4 to 5 years with antihypertensive drugs as compared to placebo did not reduce total mortality (RR 0.85, 95% CI 0.63, 1.15), coronary heart disease (RR 1.12, 95% CI 0.80, 1.57), stroke (RR 0.51, 95% CI 0.24, 1.08), or total cardiovascular events (RR 0.97, 95% CI 0.72, 1.32). Withdrawals due to adverse effects were increased by drug therapy (RR 4.80, 95%CI 4.14, 5.57), ARR 9%.
Diao D, Wright JM, Cundiff DK, Gueyffier F. Pharmacotherapy for mild hypertension. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD006742.

















