99
KCOM Kaiser Clinical Ontology Modeling Peter Hendler and Michael Rossman With some copyrighted material from Matthew Horridge
| Date post: | 10-Dec-2015 |
| Category: |
Documents |
| Upload: | melissa-oleary |
| View: | 218 times |
| Download: | 0 times |

KCOMKaiser Clinical Ontology Modeling
Peter Hendler and Michael Rossman
With some copyrighted material fromMatthew Horridge

Why Do This?•Last year we stressed the cost
savings and simplicity added if different healthcare systems use a similar (canonical) base model
•This year we will show significant additional advantages if the model is created using Web Ontology Language OWL and Description Logics (DL)

Quick Review Why Canonical Models

4
Why Do We Need Them?
Clinical Models
Electronic health care systems have evolved separately over the decades
Most were created in isolation to solve one particular domain problem (Pharmacy, Lab, Radiology, Clinical Notes, Scheduling, Billing, Admissions Discharges and Transfers or Clinical Decision Support)
As a result they all have their own models, and they can not share clinical data without complex expensive interfaces being built

5
How Do These Systems Interoperate?
Clinical Models
All systems have a “data model” whether it is explicitly designed or is just the result of how the systems store data
You must map the “data model” from one system to the “data model” for the other system if they are to share data.
This requires too many expensive interfaces that goes up by N squared for N systems.
Every mapping or interface results in the loss of some meaning

6
Current state of information modeling at KP
Current Information Modeling in KP
All applications are proprietary or legacy “ad hoc” “one-off”
Each system has a unique persistence layer and data model
Each new project generates a new relational database and new analytics
Projects require the creationof unique interfaces with all the other programs and systems
Interfacing and integrating programs and systems is both expensive and time consuming
7
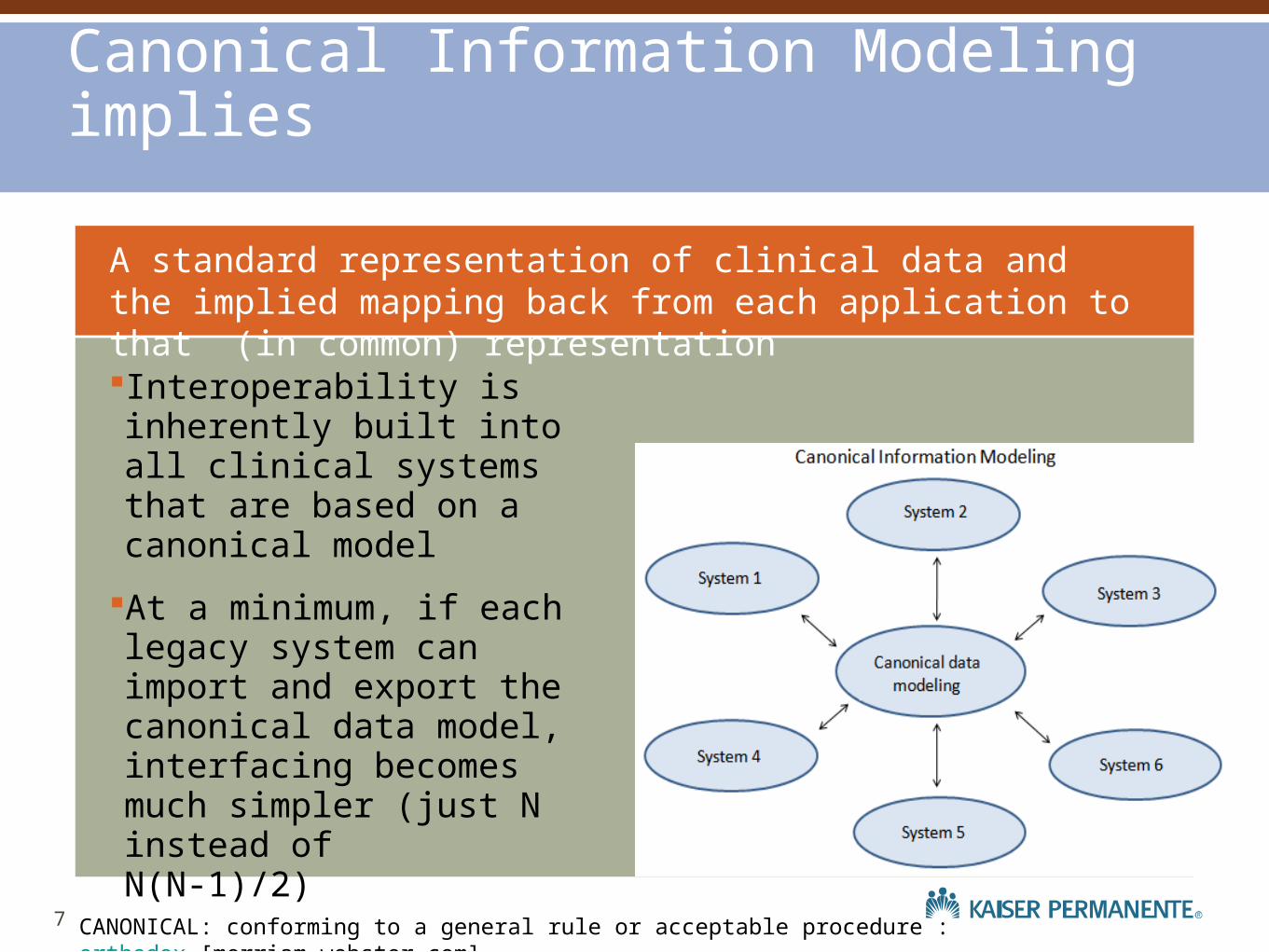
A standard representation of clinical data and the implied mapping back from each application to that (in common) representation
Canonical Information Modeling implies
Interoperability is inherently built into all clinical systems that are based on a canonical model
At a minimum, if each legacy system can import and export the canonical data model, interfacing becomes much simpler (just N instead of N(N-1)/2)
CANONICAL: conforming to a general rule or acceptable procedure : orthodox [merriam-webster.com]

Why Do This in OWL?
•How are relevant research and outcome studies done now?

Some Example Questions
• Do patients on NSAIDs get more GI bleeds?
• Do RA patients on biologic DMARDs get more non pulmonary TB?
• Do RA patients on non biologic DMARDs do as well as patients on any DMARDs plus biologic DMARDS?

And how are these questions answered today?


By Manual Chart Review Kat
•This does not change with an Electronic Health Record of unstructured data.
•Whether paper or electronic, non structured text and non Ontological terminologies (like ICD) require individual reading and evaluation by a reviewer
By using OWL in KCOM, these
queries can be automated!


Outline
•Three kinds of modeling kats
•Why use SNOMED / CMT, and OWL?
•What happens when you model the HL7 RIM backbone in OWL?
•Very Short Intro to OWL and Protege

Outline
• How does KCOM address these problems?
• The generalizable part of the model valid for all sub specialty domains
• The specialized parts of the Rheumatoid Arthritis Assessment Model (RAAM)
• The “Clinical Stories” used to create KCOM
• Walk through one semantic query

Three Kinds of Modelers
This is often the cause of communication problems between IT people with different training backgrounds and different ways of
looking at things.

19
Knows about RDBMS Kind of comfortable
Database Kitteh

20
Thinks in Unified Modeling Language (UML). Has lots of friends.
Object Oriented Kat
8

21
Is lonely, and misunderstood. But very powerful. He made SNOMED
Ontology Kat
9

Why Use SNOMED / CMT,
OWL?
Medical Terminology
•SNOMED•Ontology Description Logic•Concerned with clinical meaning, not billing•Fine grained enough to be clinically meaningful•Can be used for Outcomes measurements•Can be used by machines to make inferences

Inferences possible with SNOMED
•Strep throat is caused by streptococcus•Pneumococcal pneumonia is caused by pneumococcus•Streptococcus and pneumococcus are both sub types of gram positive cocci•Therefore both pneumococcal pneumonia and strep throat are gram positive cocci infections.

25
First Example Question Do patients on NSAIDs get more GI bleeds?
Without SNOMED or Ontology, clinical experts have to know the names and codes of all medications that are “a kind of” NSAID.
They have to know all the names of the hundreds of ICD9 codes that are “a kind of” GI bleed.
This requires Chart Review Kat and is error prone

26
Second Example Question
• Do RA patients on biologic DMARDs get more non pulmonary TB?
• How many ICD9/10 codes are “a kind of” RA
• How many ICD9/10 codes are “a kind of” DMARD?
• How many ICD9/10 codes are “a kind of” non pulmonary TB?
• Very difficult to do manually. Automatically done by SNOMED semantic search!

What happens when you model the HL7 RIM backbone in OWL?

28
4/8/2013 Kaiser Permanente © 2013

A Very Short Intro To OWL and
ProtegeIt’s all about triples

Protege
•Three main views
•Taxonomy: Only “Is A”
•OWL-Viz: Only “Is A”
•Definition: Where the triplets are defined

TaxonomyView

OWL Viz View

Definition View

OWL is all about Triplets

Domain and Range

Subclasses

Define CheeseyPizza

Define MargheritaPizza

Define SohoPizza

A Stated Taxonomy View

A Stated OWL-Viz View

An Inferred OWL-Viz View

Stated and Inferred Taxonomies

IsA
How It Looks ToThe Reasoner

IsA
How It Looks To the Reasoner

46
They could be
Myocardial Infarction and Acute Myocardial Infarction
The right side is the child of (subsumed by) the left side
Or they could be Pneumonitis and Infectious Pneumonitis
To the Reasoner it doesn’t matter, as long as it can keep track of all the symbols.
It is manipulating symbols but the result makes perfect sense and results in clinically useful inferences 4
6

What Does RAAM Model?

48
4/8/2013 Kaiser Permanente © 2013
49
What Goes In and Out of The Brain
Not trying to model the rules, or what happens in the brain of the expert who makes the decisions
Only modeling the data that a human expert clinician specialist brain needs to make it’s own assessment
Once the brain has made the assessment then we model the decision
This is “Decision Support” in a new way, no rules or suggested solutions, just support the decision maker with data

50
4/8/2013 Kaiser Permanente © 2013
The Reasoner Completely Understands the Entire Model Semantics
Detects InconsistenciesMakes Logical InferencesClassifies Clinical Data Automatically

51
4/8/2013 Kaiser Permanente © 2013
The Reasoner Knows All About The Whole Model

The generalizable part of the model valid for all sub specialty domainsSome example views into the model

53
4/8/2013 Kaiser Permanente © 2013

54
4/8/2013 Kaiser Permanente © 2013

55
4/8/2013 Kaiser Permanente © 2013

56
4/8/2013 Kaiser Permanente © 2013

57
4/8/2013 Kaiser Permanente © 2013

The Medical Specialty Domain
Specific Part

59
4/8/2013 Kaiser Permanente © 2013
60
4/8/2013 Kaiser Permanente © 2013

61
4/8/2013 Kaiser Permanente © 2013

62
4/8/2013 Kaiser Permanente © 2013

63
4/8/2013 Kaiser Permanente © 2013

64
4/8/2013 Kaiser Permanente © 2013

How KCOM is bound to SNOMED

66
4/8/2013 Kaiser Permanente © 2013
Individual Terms Bound to SNOMED-CT
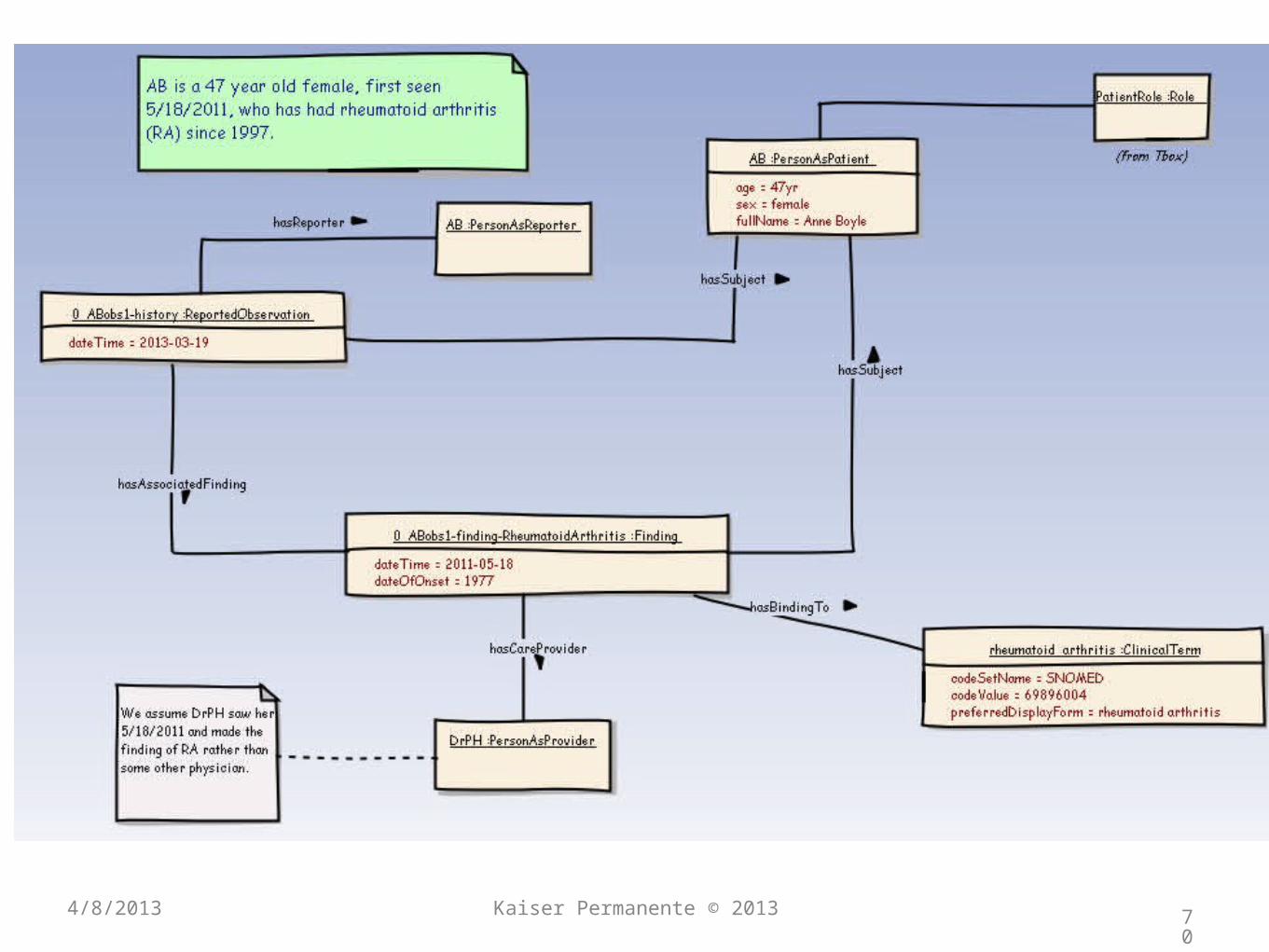
The Clinical Stories Used to Design
KCOM

Based on clinical cases
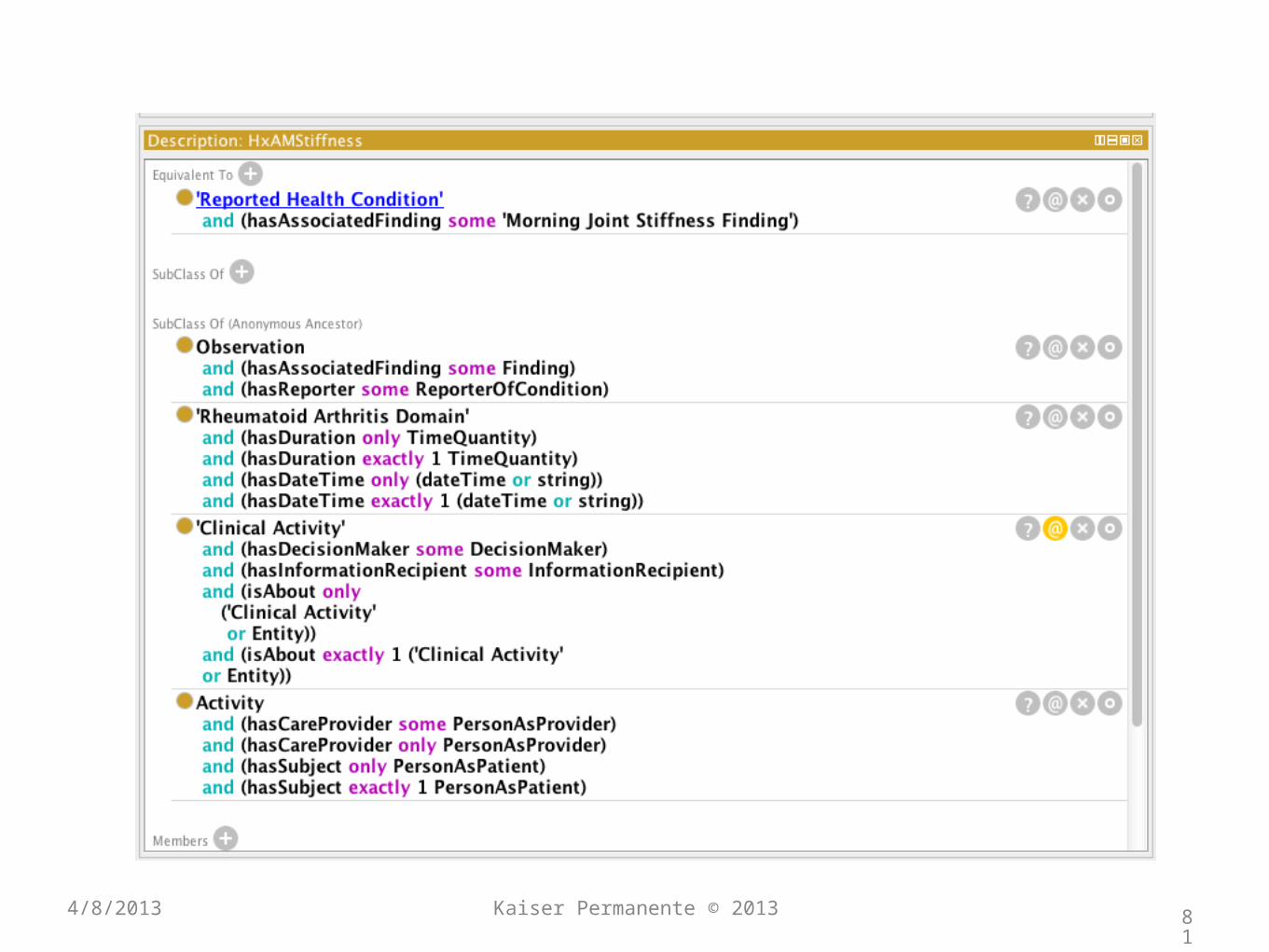
• When KCOM was first designed, we took six examples of clinical notes from Rheumatoid Arthritis Assessments
• They covered various clinical scenarios
• We will select six specific clinical statements from case number one and explore them in depth
• We will look at them in English, UML and finally in KCOM OWL

69
4/8/2013 Kaiser Permanente © 2013
70
4/8/2013 Kaiser Permanente © 2013

71
4/8/2013 Kaiser Permanente © 2013

72
4/8/2013 Kaiser Permanente © 2013

73
4/8/2013 Kaiser Permanente © 2013

74
4/8/2013 Kaiser Permanente © 2013

75
4/8/2013 Kaiser Permanente © 2013

76
4/8/2013 Kaiser Permanente © 2013

77
4/8/2013 Kaiser Permanente © 2013

78
4/8/2013 Kaiser Permanente © 2013
79
4/8/2013 Kaiser Permanente © 2013

80
4/8/2013 Kaiser Permanente © 2013
81
4/8/2013 Kaiser Permanente © 2013

82
4/8/2013 Kaiser Permanente © 2013

83
4/8/2013 Kaiser Permanente © 2013

84
4/8/2013 Kaiser Permanente © 2013

85
4/8/2013 Kaiser Permanente © 2013

86
4/8/2013 Kaiser Permanente © 2013

87
4/8/2013 Kaiser Permanente © 2013

And One Semantic Query Example

2Compare the number of gastrointestinal bleeds in RA patients in the following groups.Those who have and have not taken NSAIDs

Break this up into steps.First find Patients with RA
PersonAsPatient and subjectOf Observation hasAssociatedFinding Rheumatoid Arthritis(we will be using this basic query in all the other examples)
Now using this limited cohort of RA patients continue to query as follows to find the sub groups.

Now we find two sub groups, those who are not on NSAIDs and those that are.(we can do this for current use or past use which ever we choose)
PersonAsPatient and subjectOf Observation has MedicationAdministration has AssociatedMedication some NSAID.
(note the subsumption here is very useful. Otherwise you have to accumulate all the meds that are NSAIDs with the help of a clinical/pharmacy expert. In the KCOM case this clinical knowledge is part of the model itself)

PersonAsPatient and subjectOf Observation has MedicationAdministration has AssociatedMedicationONLY NOT NSAID (we will not explain the difference between “some” and “only” but this query gets those NOT on any kind of NSAID.
Now we have these two groups and we need to find in each one who has had GI bleed. The ICD9 or ICD10 has many different diagnosis that are all some kind of GI bleed. Not being able to use SNOMED subsumption is a fatal drawback. Because we are using SNOMED and because we are using OWL in our base clinical model we can simplify this complex query into.

PersonAsPatient and SubjectOf Observation hasAssociatedFinding some <<bleeding and has finding site gastro-intestinal structure>>
(the latter part is a post coordinated SNOMED expression I used just for demonstration We could also use instead the pre-defined SNOMED term 74474003:GastroIntestinal Hemorrhage (disorder)

It is important to point out. There are too many ICD9 and ICD10 codes that are all a kind of “Gastrointestinal Hemorrhage” and unless you happen to know all of them, you will miss some patients.This SNOMED Description Logic Subsumption query will catch all of them even if you don’t know what they are called. Even a clinical expert could not be expected to recall every possible kind of ICD9 or 10 term that is some kind of gastrointestinal bleed.

Conclusions
•Last year we stressed the advantages (in time money and simplicity) of using standard (canonical) models to integrate clinical systems

Conclusions
•This year we show that by using models based on Description Logic (OWL) and SNOMED we are able to use Semantic Searching to automate important and complex queries that would otherwise need manual chart reviewers and take much more time and expense.

Does Ontology Kat Work Well With
OWL?


Abbreviations
• RAAM: Rheumatoid Arthritis Assessment Model
• RDBMS: Relational DataBase Management System
• OO: Object Oriented
• KCOM: Kaiser Clinical Ontology/OWL Model
• DMARD: Disease Modifying AntiRheumatic Drug
• NSAID: Non Steroidal AntiInflammatory Drug
• OWL: Web Ontology Language
• DL: Description Logics

















