88
Kelly Shinkaruk, MD FRCPC HLT 123 October 17, 2009 1
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | logan-watkins |
| View: | 217 times |
| Download: | 0 times |

Kelly Shinkaruk, MD FRCPCHLT 123
October 17, 2009
1

Fluid Therapy ObjectivesBody Fluid CompartmentsFluid Requirements
Maintenance and Insensible LossesFluid DeficitThird SpaceBlood Loss
Types of Fluid and ResuscitationCrystalloidsColloids
2

Fluid Therapy ObjectivesIntravenous Access
Sites for Line InsertionAdvantages and DisadvantagesComplication RisksInsertion Techniques
3

Fluid Therapy ObjectivesBody Fluid CompartmentsFluid Requirements
Maintenance and Insensible LossesFluid DeficitThird SpaceBlood Loss
Types of Fluid and ResuscitationCrystalloidsColloids
4
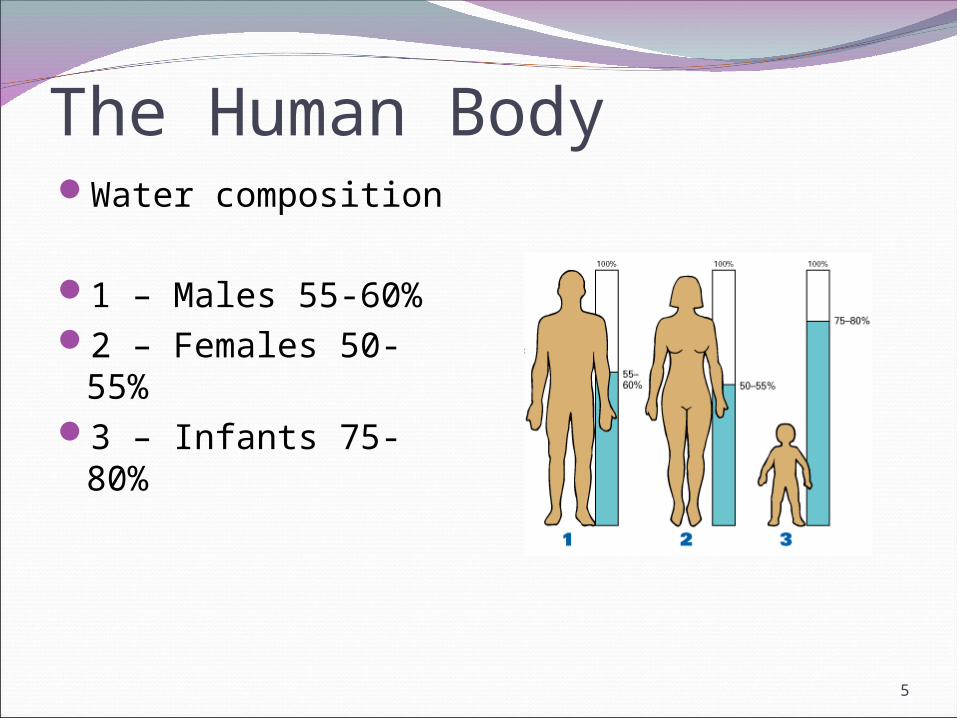
The Human BodyWater composition
1 – Males 55-60%2 – Females 50-55%3 – Infants 75-80%
5

Fluid Compartments60% water by
weight
Intracellular 2/3
Extracellular 1/3 Interstitial ¾ Intravascular 1/4
Intracellular
Interstitial
Intravascular
6
Differences in Body FluidsAge and Gender:
Prems – 90mL/kgChildren – 80mL/kgAdult Male – 70 -
75mL/kgAdult Female – 60 -
65mL/kg
Obesity:Water volume based
on ideal body weight (IBW)
IBW = 50kg + 2.3kg per inch over 5ft
7
Fluid Therapy ObjectivesBody Fluid CompartmentsFluid Requirements
Maintenance and Insensible LossesFluid DeficitThird SpaceBlood Loss
Types of Fluid and ResuscitationCrystalloidsColloids
8

Operative Fluid RequirementsDeficits
Overnight fasting Bowel preps: Liters of losses potentially Diuretics
Maintenance GI losses: 100-200 ml/day Insensible: 500-1000 ml/day Urinary: variable, >1000 ml/day
Ongoing Losses Blood loss Third space losses
9

Maintenance Fluids
First 10 kg of body weight = 4 ml/kg/hrSecond 10 kg = 2 ml/kg/hrEvery kg over 20 = 1 ml/kg/hr
80 kg person = 40 + 20 + 60 = 120 cc/hr
10

Fluid Requirements for SurgeryCalculated per hour during OR:
Fluid deficit (NPO for 6+ hours): 4/2/1Ongoing fluid requirements: 4/2/1Replacement of blood loss
Crystalloid 3:1, Colloid 1:1“Third-space” loss
4/6/8 rule: 4 ml/kg/h for minor surgery (hernias, wrist ORIF,
breast) 6 for moderate surgery (gyne, ortho, thoracics) 8 for major procedures (major bowel, vascular, trauma)
11

Clinical example29 yo 70 kg male with
femur fracture for ORIF NPO 12 hours
Calculate deficit ½ over first hour ½ over the rest of the
caseProvide maintenance
4 - 2 - 1 RuleReplace losses
3 to 1 for bleeding Third space (4-7
cc/kg/hr)
12

CalculationDeficit
Maintenance X hours NPO 110 cc/hr X 12 hours = 1320 cc 660 cc in first hour – the rest over the case
Maintenance 4 – 2 – 1 Rule = 110 cc/hr
Third spacing and bleeding 6 cc/kg/hr = 420 cc/hr
1190 cc of crystalloid in the first hour alone
13

Fluid Therapy ObjectivesBody Fluid CompartmentsFluid Requirements
Maintenance and Insensible LossesFluid DeficitThird SpaceBlood Loss
Types of Fluid and ResuscitationCrystalloidsColloids
14
What is osmolarity?
15

What is osmolarity?Osmolarity: a measure of how many
dissolved particles are in the bloodEquilibrium: dissolved particles “pull” water
across membranes so that total concentration of dissolved particles (osmolarity) is equal on each side (give or take, with some electrochemistry involved)
16

17

What is normal serum osmolarity?
18
OsmolarityHypertonic: more concentrated than plasmaHypotonic: less concentrated than plasmaIsotonic: the same concentration as plasma
19

OsmolarityIf you give too much hypotonic fluid, cells can
swell and burstIf you give too much hypertonic fluid, cells
can shrinkFast correction of electrolyte imbalances is
BADWhere is this most important?
The brain! WHY?
20
Types of FluidsClassification: based on their behaviour once
givenMostly go to ICF: free waterStay in ECF: crystalloidStay in plasma: colloid
21

Free Water
Pure water is NEVER given IV! It is very hypotonic and will burst RBCs and cause electrolyte imbalances!
Dextrose5% or D5W10 % or D10W50% or D50W (low
volume packages)
22
IMPORTANT NOTE:
Free WaterD5W: most commonly used
D10W and D50W usually used for low blood glucose levels, not free water deficit
Stats:Dextrose 5gm/dLpH 5.0 Osmolarity 253
IV infusion: little stays intravascularDextrose is actively transported into cells and
water follows it (equilibrium)
23

D5WPros:
Treats hypoglycemiaOften used preop
for diabetic patients who are NPOBody needs sugar
for long-term NPO
Cons:No good for
resuscitationCan cause hypo-
osmolarity and water intoxicationMay worsen brain
trauma
24
CrystalloidsUsed for fluid deficit, third space losses,
maintenanceEquilibrates in ECF (plasma/interstitial)When infused: about 1/3 stays in
intravascular space, and after ~ 10 minutes, the other 2/3 has diffused out of the plasma
When administering for blood loss, must use 3-5L for every 1L of bloodEx: 3L blood loss = 9-15L of RL!!
So we use other fluids for LARGE replacement!
25

CrystalloidsNormal Saline
Hyperosmolar 308 mosm/l Sodium 154 Chloride 154
Acidic relative to the plasma pH 5.0
Excessive administration results in: Hyperchloremic metabolic acidosis
1000 ml NS – redistributed along [Na] Extracellular - ISF 750 ml, only 250 ml
stays intravascular
26
CrystalloidsNormal SalinePros:
Good for initial resuscitation Cheap Readily available,
multiple sizes Widely used for OR
maintenance fluid Compatible with all drugs and blood products
Cons: Hyperchloremic,
hypernatremic metabolic acidosis (Use 3L or less) Large sodium load Use care with
heart failure, renal failure, brain injury, old age
27

CrystalloidsRinger’s LactateOsmolality 279 mOsm/L
Na+ 130 mmol/L Cl- 110 mmol/L Lactate 27 mmol/L K+ 4 mmol/L Ca++ 3 mmol/L pH 6.5
Closer to physiologic pH and Osmo
28
CrystalloidsRinger’s LactatePros:
Good for resuscitation More “physiologic” Contains K Less hyperosmolar
than saline No hyperchloremia
Cons: More expensive Not compatible
with some drugs or blood May worsen brain
swelling (not as bad as NS) Use caution with
elevated K, renal failure
29
ColloidsNS based fluidsContain osmotically active particlesLarge molecules unable to cross endotheliumProvide colloid oncotic pressure
Theoretically replenish intravascular volume and stay in this compartment much longer than crystalloids
30

ColloidsPentaspan ($70 per
500cc)
○ Normal Saline plus 10 g/100ml pentastarch
○ 250 kDa Protein○ pH 5.0○ High Na load just as with
NS
○ Renal excretion○ 70% cleared in 24 hours
in patients with normal GFR
○ Max dose 28 mL/kg over 24 hours (2 L)
Voluven
Normal Saline plus 6g/100mL hydroxyethyl starch
130 kDa Protein pH 5.0 High Na load just as
with NS
Renal excretion 70% cleared in 72 hours
in patients with normal GFR
Max dose 50 mL/kg over 24 hours (3.5L)
31

ColloidsPros:
Smaller infused volume
Replace blood loss 1:1
Prolonged ↑ Intravasc vol
Less edema Pulmonary, peripheral
Cons:No O2 carrying
capacityExpensiveDilutional
coagulopathyLeaky capillaries =
interstitial edemaIncreased
anaphylactoid reactions
32

ColloidsAlbumin
Human blood product Purified protein from human blood Large osmotically active protein increases oncotic
pressure Available as 5% and 25% solutions Similar risks to other blood products
Half-life 1.6 hours in plasma = 8 hours plasma elimination 20 days in the body
Increased morbidity compared to other colloids
33

Hypertonic solutionsHypertonic Saline
Available as 1.8%, 3%, 7.5%, 10% solutions Increases extracellular osmolality Promotes fluid shift from ICF to ECF
Rare indications: Trauma Symptomatic acute hyponatremia (TURP syndrome)
Unclear benefits – risk acute hypernatremia
34

Fluid Therapy ObjectivesIntravenous Access
Sites for Line InsertionAdvantages and DisadvantagesComplication RisksInsertion Techniques
35
Sites for Line InsertionPeripheral Intravenous Access
Central Intravenous AccessInternal Jugular (IJ)SubclavianFemoral
Intraosseous Access
36

Peripheral IV Access
37

Peripheral IV AccessAdvantages
Easy to placeMany points of
accessIf unsuccessful,
compressible siteFewer complications
than central accessLarge bore access
allows rapid infusion of large volumes
DisadvantagesVein may be difficult
to accessNot used for
prolonged administration of vasoactive drugs
Cannot be placed distal to site of surgery or injury
38

Central Venous Access
39
Central Venous AccessAdvantages
Reliable IV access when peripheral sites not available
Long term IV and vasopressor therapy
Large volume resuscitation
DisadvantagesSpecial equipment
requiredLonger time to
placeHigher complication
rateNeed for special
skill
40

ComplicationsMechanical
Arterial puncture (femoral > IJ > subclavian)Hematoma (femoral > SC > IJ)Hemothorax (only seen in SC)Pneumothorax (SC >> IJ)Cardiac Tamponade (SC = IJ)
InfectiousEmbolic
Wire/catheter embolism
41

Intraosseous Access
42

Intraosseous AccessAdvantages
Venous access when no other sites can be found
Useful if difficult, delayed, or impossible IV access
Used in burns or other injuries preventing alternate access
DisadvantagesNeed for special
equipment and skill
Requires pressure bag to provide reasonable flow of fluids
Osteomyelitis if long term
43

Whaddya do now???
44

Kelly Shinkaruk, MD FRCPCHLT 123
October 17, 2009
45

Blood Therapy ObjectivesBlood Components
Blood TransfusionPros and Cons of Blood Products
Indications for TransfusionAcceptable Blood LossFactors Related to Blood Administration
Complications Related to TransfusionLab and Point of Care TestingAdministration Techniques
46

Blood Therapy ObjectivesBlood ComponentsBlood TransfusionPros and Cons of Blood Products
Indications for TransfusionAcceptable Blood LossFactors Related to Blood Administration
Complications Related to TransfusionLab and Point of Care TestingAdministration Techniques
47

Blood ComponentsCells:
Red blood cells: carry oxygenPlatelets: imperative for clottingWhite blood cells: removed
Fluid: Plasma: Fluid with proteins (albumin), clotting
factors
Proteins: Clotting factors II-XII
48

Blood TransfusionAutologous bloodRecovered bloodPooled blood products
No “whole blood” anymoreRBCsplateletsPlasmaCryoprecipitate, factor VII
49

Autologous BloodPros:
Person’s own blood-low risk of transfusion reactions Can donate up to
4 units Whole blood:
coagulation factors, etc.
Cons: Anemic, heart
disease, transmissible diseases not eligible Whole blood only Anemia from
donation Expensive
50
Recovered Blood (Cell Saver)Pros:
Person’s own RBCs, washed No transfusion
reaction Can be used for
some Jehovah’s Witnesses
Cons: Expensive Surgical
contaminationBone InfectionCancer?
Not 100% recovery
51
Cell SaverWhen?
Major vascular proceduresMajor ortho proceduresMajor traumaSometimes used in neurosurgery/backsScoliosis surgery
52

Cell Saver
53
Packed RBCsPros:
1 unit = Hb by 10 g/l Best replacement
for excessive blood loss Stays in vascular
compartment Mix with saline for
faster infusion
Cons: Transfusion
reactions Expensive Freshness Risk/benefit ratio Cold
54

Frozen PlasmaPros:
Contains all coagulation factors (V and VIII unstable) Use for high
volume/ongoing transfusion or bleeding with coagulopathy used to be given for
elevated INR Now we have
octaplex!
Cons: Can contain
infectious particles Fluid overload
55

PlateletsIndications:
Acute thrombocytopenia (platelet deficiency)
Large volume transfusion + bleeding
One unit = increase platelet count by 5-10
Complications:Stored at room
temperatureHigh risk of
bacterial contamination/sepsis
56
CryoprecipitateContains
Factor VIIIFactor XIIIVon Willebrand’s FactorFibrinogen (Factor II)
Indications Coagulopathy in massive bleeding and transfusion Actively bleeding patients with Fibrinogen < 0.8-1.0 g/L VWD or Hemophilia A (Factor 8 deficiency)
Only in the absence of specific factor concentrates DDAVP is not available or ineffective
57

Blood Therapy ObjectivesBlood Components
Blood TransfusionPros and Cons of Blood Products
Indications for TransfusionAcceptable Blood LossFactors Related to Blood Administration
Complications Related to TransfusionLab and Point of Care TestingAdministration Techniques
58

Indication for TransfusionBlood products administered for
dangerous levels of blood loss Normal Hgb 120-150g/L Healthy patients tolerate >70g/L With systemic disease >90g/L
Start with PRBCsHistorically, transfuse Plts, FP, cryo only
when “indicated” low plts, surgical oozing, etc
Now moving to PRBCs : FP : Plts (1:1:1)
59
Acceptable Blood LossDepends on:
Preop HbVolume of blood lossCoexisting disease
Cardiovascular disease
Normal Hb level can be by ~25% with little stress…as long as intravascular VOLUME is maintained!
60

Acceptable Blood Loss (ABL)ABL= [ Hgbinitial – Hgbfinal / Hgbfinal ] X EBV
Example:
60 yo female for THR. Preop Hgb 120, Wt 75kg
We will accept Hgb of 75 post-op
EBV = 75kg x 60 cc/kg = 4500cc
ABL = [120-75 / 120] x 4500 = 1688 cc
We will allow her to lose 1700cc blood without transfusing her
61

Blood Volume How much blood do we have?
62
Preemie 90 ml/kg
Baby 80
Adult male 75 (less for obesity)
Adult female 65 (less for obesity)
“Acceptable loss” = ml/kg blood volume x kg body weight x % decrease in Hb

Factors Related to Blood AdministrationConsent
Discuss options early therefore alternatives can be considered
Ensure all questions answeredType and screen
Jehovah’s WitnessesMost will not accept allogenic productsMust verify what they will/won’t accept DOCUMENT IT IN THE CHART!
63

Blood Sparing TechniquesProcedures with high anticipated blood lossPreop techniques
Erythropoietin + Fe – at least 2wks preAutologous donation – at least 1mth pre
Intraop techniquesAntifibrinolytic therapy (tranexamic acid)Cell saverControlled hypotensionTourniquet“damage control” surgery
64

Blood Therapy ObjectivesBlood Components
Blood TransfusionPros and Cons of Blood Products
Indications for TransfusionAcceptable Blood LossFactors Related to Blood Administration
Complications Related to TransfusionLab and Point of Care TestingAdministration Techniques
65

Dangers of BloodTransfusion reactions
Clerical error: most common reasonTransmission of infectious particles:
Viruses Bacteria Prions?
Mad cow Kreutzfeld-Jacob
66

Dangers of Blood
67
1 : 500,000Death from sepsis
1 : 82,000Hepatitis B
1 : 3.1 millionHepatitis C
1 : 4.1 millionHIV transmission
RiskEvent
Risk of sepsis is even higher with autologous blood and platelets!
Complications of Blood Transfusion
Volume overloadheart failure, pulmonary edema
Temperature hypothermia from large amounts of cold
blood/fluidAir
if given under pressure, risk of air entering circulation (air trapping in lung, heart, brain)
Immune suppressionnon-specific suppression with blood product
administration 68
Complications of Blood Transfusion
Incompatibilityred blood cell, white blood cell, plasma
antibody reactionsMost common reason: clerical error
Dilutional coagulopathyInfection
blood screened for HIV, Hep C/B, syphilis, others
Not screened for all viruses!
69

Complications of Blood Transfusion
Biochemical abnormalitiesCitrate: anticoagulant in pRBCs, binds
calcium, may necessitate calcium replacementPotassium: high concentrations in pRBCs, with
low pH. Interreaction of pH and K may mean high or low K after transfusion
Microaggregatestiny clots in pRBCs may lodge in lungs (TRALI)
70

Symptoms of Blood ReactionsPain, rash, hives, edemaFever, chills, nausea, vomiting, SOBBP, HR, O2 sat, mental status changesPink or brown urineCirculatory collapse
71
TAKE-HOME MESSAGE
Any change in clinical condition after blood transfusion is suspect!! Stop transfusion and treat aggressively!!

Complications: What to DoSTOP blood product IMMEDIATELY!Notify other OR staff, blood bank.Send blood and samples from patient to
lab.O2, drugs as necessary to support vital
signs. Fluids, drugs to flush kidneys.Monitor for coagulation problems, treat as
necessary.72

Transfusing BloodDoes patient want blood?How much of this anemia is acute?Is blood loss more than “acceptable”?Will there be more blood loss? Is there a
coagulopathy causing this?Is the patient at risk from heart or
vascular disease?Have I tried to use other fluids without
success?73

Blood Therapy ObjectivesBlood Components
Blood TransfusionPros and Cons of Blood Products
Indications for TransfusionAcceptable Blood LossFactors Related to Blood Administration
Complications Related to TransfusionLab and Point of Care TestingAdministration Techniques
74

Lab and Point of Care TestingUsed for intra-op diagnosisRapid assessment of blood measurementsHelps guide ongoing therapyDifferent equipment
Hemocue for HgbHemochron for PTT/INRiStat for ABGs, lytes, Hgb
Traditional lab work also available – but takes far longer!
75

Lab and Point of Care TestingHemocue
Used for rapidly checking Hgb
Easy to use, no need for arterial access
Not as accurate as sending a CBC
76
Lab and Point of Care TestingHemochron Jr.
Measures coagulation parameters
PTT and INRNo need for arterial
access
77

Lab and Point of Care TestingiStat
Rapid assessment of blood gases, Hgb, electrolytes
Need arterial sample
More accurate than Hemocue
Same technology as ABG sampling machines
78

Lab and Point of Care TestingACT (activated clotting time)
Used during vascular proceduresMonitors effectiveness of high dose heparin
therapySample from undiluted site not contaminated
by heparin infusionHelps guide further dosing of heparin or
reversal of heparin with protamine
79

Blood Therapy ObjectivesBlood Components
Blood TransfusionPros and Cons of Blood Products
Indications for TransfusionAcceptable Blood LossFactors Related to Blood Administration
Complications Related to TransfusionLab and Point of Care TestingAdministration Techniques
80

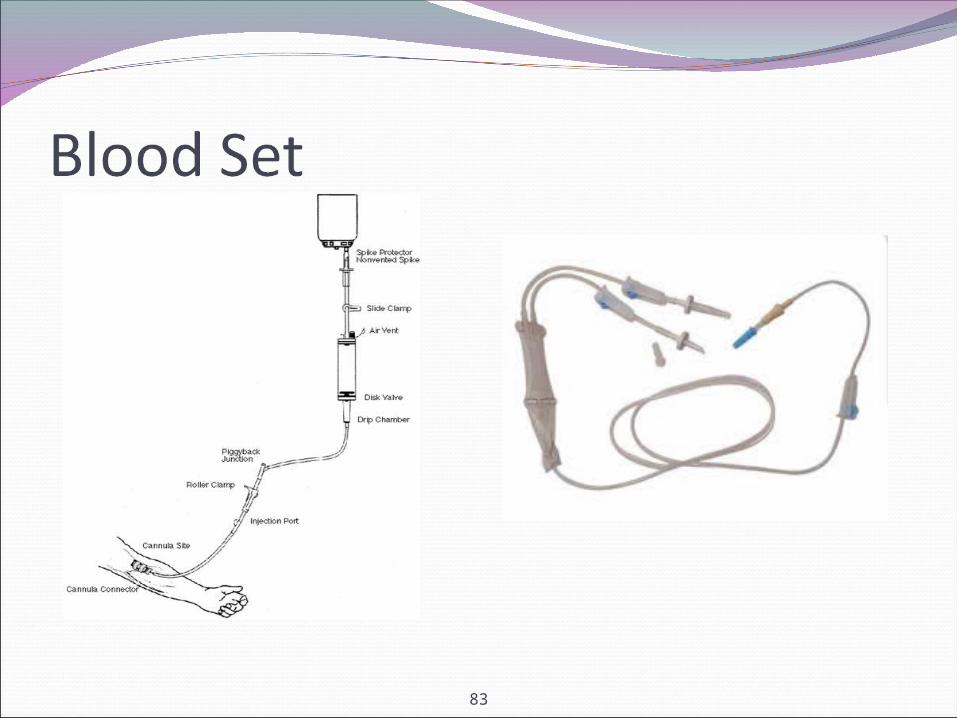
Administering Fluids and Blood ProductsEnsure at least one functional IVNormal Procedure
IV infusion set upFluid warmer - not necessary, often if >2hr
procedure or possibility of blood transfusionProcedure with anticipated transfusion
IV Blood setFluid warmer essential
81

Administering Fluids and Blood ProductsSome physicians now use infusion pumpsOccasionally administer meds by infusion
pumpVancomycinInsulin
82
83

Massive TransfusionDefinition
the replacement of TBV in less than 24 hours or…
more than half the EBV per hour. TOH has a massive transfusion protocol
In the binderIncludes studies/point of care, order of blood
products, factor VIIa, etc.Rapid infusion – Pressure bags, Level 1
84

85
CompatibilityPacked RBCFrozen PlasmaCryoprecipitatePlatelets
86
Administration SetFrozen PlasmaPacked RBCCryoprecipitatePlatelets
87
Questions???
88

















