OHSU Parkinson Center April 30, 2017 Linda Bryans, MACCC SLP-L Allison Lindauer, NP, PhD Lisa Mann, RN Aimee Mooney, MSCCC-SLP-L Jennifer Wilhelm, PT, DPT, NCS Rosanne Yee, OTR-L Key Challenges in Team Care Late Stage PD OHSU PARKINSON CENTER
Transcript
OHSU Parkinson Center
April 30, 2017 Linda Bryans, MACCC SLP-L Allison Lindauer, NP, PhD Lisa Mann, RN
Key Challenges in Advancing PD Nutrition, Feeding & Swallowing
Rosanne Yee, OTR Linda Bryans, MA, CCC-SLP
OHSU Parkinson Center
What? When? How? • What foods?
– Can be decided by ability to swallow, ability to manipulate food to mouth and foods that aid bowel movements (for constipation)
• When to eat? – Can be dependent on medications, energy level to maintain
proper posture during meal • How to make food?
– Can be decided on ability/endurance of balance and standing, energy and ability to use kitchen equipment, making the consistency allowed for swallow
• How much food? – Can be decided by caloric intake needed to maintain levels of
physical and cognitive activities, swallow abilities per bite
Interdisplinary Approach= Interplay with other team members
OHSU Parkinson Center
Nutrition • Important to understand the role nutrition
plays in both neuroprotection and neurodegeneration.
• Recent studies have revealed the promise of some nutrients in reducing the risk of PD and other nutrients may be involved with increasing the risk or quicken disease progression
• Important to understand effects of food on medications
(The emerging role of nutrition in Parkinson's disease Seidl. Et al. Front. Aging Neurosci., 07 March 2014)
OHSU Parkinson Center
Nutrients that may be Associated with an Increased Risk or Progression of PD • Dairy products
– the possible presence of neurotoxins, like pesticides in dairy products may increase the risk of PD
– mainly milk-strong positive association with the consumption of milk, but not cheese or yoghurt has been reported
(The emerging role of nutrition in Parkinson's disease Seidl. Et al. Front. Aging Neurosci., 07 March 2014)
Presenter
Presentation Notes
case of organic dairy products Milk May increase one's risk of PD
OHSU Parkinson Center
Nutrients that may be Associated with a Decreased Risk or Progression of PD
• Phytochemicals-Fruits and vegetables are rich sources of antioxidants
• Omega-3 polyunsaturated fatty acids-neuroprotective and has anti-inflammatory potential
• Soy-primary protein in soy appears to be neuroprotective • Caffeine- decrease triggers for neuroinflammation in
neuropathways may contribute to neuroprotection • Tea-Polyphenols in green and black tea provide potent
antioxidant-radicals • Alcohol-moderate consumption lowers the risk of PD. Red wine
especially neuroprotective (The emerging role of nutrition in Parkinson's disease Seidl. Et al. Front. Aging Neurosci., 07 March 2014)
Presenter
Presentation Notes
plant chemicals that have protective or disease preventive properties OM3-There have been no direct studies in PD patients that address whether omega-3s are neuroprotective, however, one study showed that supplementation with omega-3 reduced depression in PD patients Caffeine studies suggest that the beneficial effects of caffeine may be limited to men and post-menopausal women not receiving hormone-replacement therapy Tea-couple studies show 2-3 cups a day and decrease risk of PD and showed delay onset of motor symptoms Alcohol Great consumption raises the risk
OHSU Parkinson Center
Nutrients: Questionable Role in PD
• Fat-saturated may increase risk of PD vs. high fat diet (8% protein) provided symptomatic and beneficial disease modifying activity
• Meat- red meat heme iron content may act as a toxin when not digested properly vs higher intake of iron is associated with neuroprotection in PD
• Carbohydrates-high glycemic index decrease the risk of PD vs High carbohydrate diets are associated with an increased risk of type 2 diabetes, which numerous studies indicate type 2 diabetes is associated with an increased risk of PD
(The emerging role of nutrition in Parkinson's disease Seidl. Et al. Front. Aging Neurosci., 07 March 2014)
Presenter
Presentation Notes
Fat-link with protein may be reason for increase risk? Meat- iron derived from meat?
OHSU Parkinson Center
Nutrition and Medication Interactions
• All types of protein can interfere with Carbidopa-Levodopa absorption
• It is best to take the medication 30 to 60 minutes before eating protein and 1 to 2 hours after protein
• Take the medication along with foods that don’t contain proteins.
(National Parkinson Foundation (2017))
Presenter
Presentation Notes
Pt sometimes don't end up eating enough because they are scared that the meds will not work if they eat If taking long acting or taking meds every 2 hours pts to consult doctors Supplemental handout for Low protein foods
OHSU Parkinson Center
Meal Preparation
• Barriers to participation and completion: – Fatigue (PT and SLP) – Posture (PT) – Pain (PT) – Vision (Neuro-opt/neuro-ophth) – Tremor (PT) – Rigidity (PT) – Cognition (SLP)
Presenter
Presentation Notes
Fatigue-Physical how much chopping stirring moving around and cognitive fatigue keeping track next steps Posture- can decrease and limit reach causing increase risk of falls/burns Pain-in back from standing too long,in arms from repetitive actions Vision-poor lighting, decrease contrast sensitivity, reaching, cutting,mixing, stirring off,walking in kitchen off because depth perception is off or double vision Tremor-reaching, cutting,mixing, stirring effected, transporting/carrying items in kitchen tremor could be in trunk or neck Rigidity-reaching all ingredients and kitchen equipment for cooking Cognition-trouble with attention, memory, mulitasking, timing
OHSU Parkinson Center
Meal Preparation: OT Interventions • keep handles in and use the back burners if having balancing
problems • changing body positions: sit perching stool • good lighting • contrast colours: Equipment • gather ingredients all together before cooking • re-arrange kitchen for easier access to items used frequently • simple and less time depending recipes (limit multi task recipes) • use alarms/timers • use checklist to keep track of what has been done • Pacing: prep things throughout day, use crockpot
Presenter
Presentation Notes
Supplementary list of adaptive equipment
OHSU Parkinson Center
Eating and Drinking • Barriers to participation and completion: • Dexterity • Wrist rigidity • Bradykinesia • Tremor • Decreased appetite (meds and olfactory issues) • Rigidity (increase caloric expenditure) • Posture • Vision • Fatigue (hand to mouth and chewing)
Presenter
Presentation Notes
Dex-Trouble holding, gathering food and moving utensil with fingers Wrist-level off and adjust as food gets closer to mouth Brady-slowness getting food to mouth Tremor-gathering food on utensil, food may fall off if not gathered correctly, missing mouth App-most PD med may cause nausea and loss of smell can impact taste Rigidity-not having the ROM to get food to mouth Posture-can effect the reach,strength and endurance of U/E action hand to mouth Vision-unable to see food on plate, depth perception of aiming at food off, Repetitive motion of eating and chewing
OHSU Parkinson Center
Eating and Drinking: OT Interventions
• modify routines of meals: time of meals, texture, amount, environment
• only needed items on table • smaller portions • posture and proximity to table • Use of both hand • contrasting colours, proper lighting • adaptive equipment (plate guard, built up handles, off
set spoon and fork, liftware, Readi-steady glove, rocker knife, ergo knife, “nosey” cup, small opening bottles, non slip mats, box to raise eating surface)
Presenter
Presentation Notes
Straws are questionable. Helpful for tremor and neck pain and/or rigditity but not helpful for swallow
OHSU Parkinson Center
Feeding Habits that effect Swallowing
Observation during ADL’s: • Difficulty looking
down at the plate (make sure plate is in line of vision) • Mouth stuffing and rapid drinking • Tremor or stiffness interfere with self-feeding • Listening to patient/family about length of
mealtimes • Is my patient fatigued
from malnutrition or dehydration related to Dysphagia?
Presenter
Presentation Notes
what are things Im looking for to refer to other disciples like stop or avoid eating some foods, drooling,coughing,neck pain looking down at plate/bowl, forgetting to use the interventions
OHSU Parkinson Center
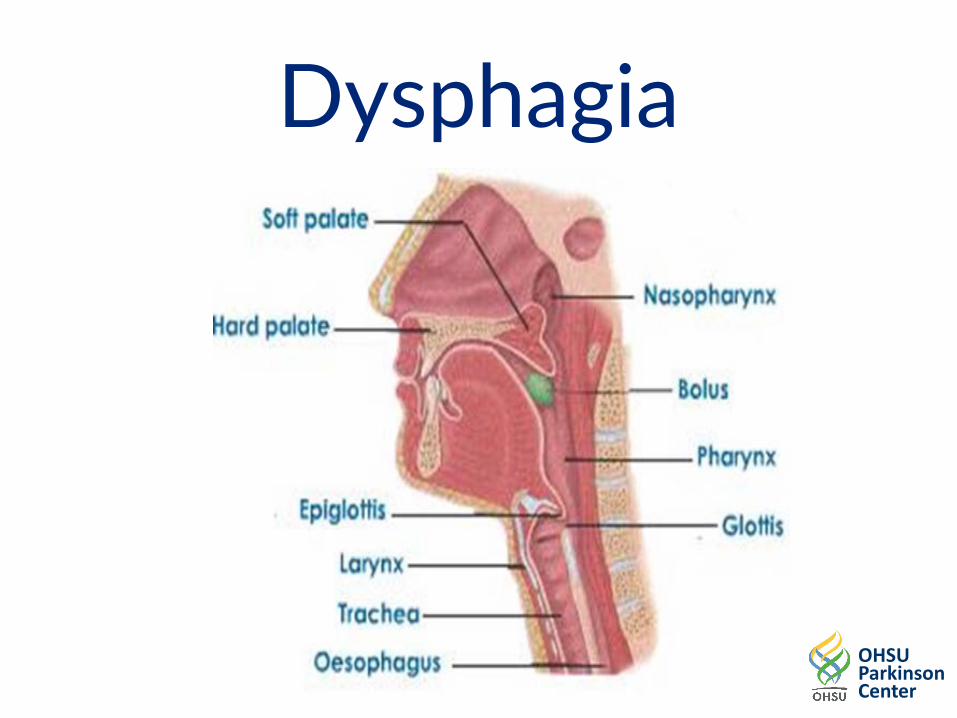
Dysphagia
OHSU Parkinson Center
Dysphagia in PD • Oral phase: PD can cause rigidity, tremor or dyskinesias in the muscles in the
tongue, jaw, lips and face which can impact the oral stage of the swallow. – Reduced or effortful chewing - Repetitive or excessive tongue movement (“tongue pumping") – Drooling - Reduced A-P transit – Decreased initiation - Oral residue
• Pharyngeal phase. PD can cause the swallow to be delayed, reduce pharyngeal contraction, reduced UES opening, reduce airway protection and reduce pharyngeal sensation.
– Choking or coughing while eating or drinking – Wet vocal quality after eating or drinking – Frequent throat clearing while eating or drinking – A sensation of food sticking in the throat
• Esophageal phase: PD can cause tightness in the cricopharyngeus muscle, reduced esophageal peristalsis and esophageal reflux.
– Heartburn – Food coming back up into the throat or mouth after swallowing – Coughing after eating – Frequent coughing or throat clearing
-Tjaden. Speech and Swallowing in Parkinson's Disease (2008)
Presenter
Presentation Notes
Oral phase deficits probably occur most frequently in PD and are usually first s/s of dysphagia- Yorkston et al (2004) Rosenbeck & Jones (2007) In red: Team members can be on the look out for these issue as PWP do not always appreciate s/s of dysphagia and will deny or simply not report. Reduced cough/airway protection Silent aspiration
OHSU Parkinson Center
PD Dysphagia Stats • 40-90% of persons with PD have dysphagia
– Rosenbeck & Jones (2007) – Leopold & Kagel (1997)
• Subjective dysphagia in 1/3 of community dwelling PD pts (higher numbers in advanced PD)
• Patients may remain clinically asymptomatic • Patients may have poor awareness of dysphagia • 15% of PD patients show silent aspiration • Dysphagia is more prevalent in advanced PD but often
does not correlate with disease severity • Moderate dysphagia: "The potential for aspiration that
is minimized by swallowing techniques and diet modifications"
– Yorkston, Miller, Strand (2004)
OHSU Parkinson Center
Cough • Airway protective mechanisms such as swallowing and
cough may play a role in aspiration pneumonia • Cough is an important defense mechanism
– Important to remove mucus, foreign bodies from airways by generating a high expiratory flow
• Impairment of cough – Motor dysfunction – Sensory dysfunction
• In early stages of PD, the motor component of cough was impaired
• In late advanced stages of PD, both the motor and the sensory component of cough were impaired -Ebihara et al (2003) Impaired efficacy of cough in pts with PD
Presenter
Presentation Notes
It's important to talk about cough and airway protection in PD as impairment of cough can play a role in aspiration pna We think about cough as having two areas of dysfunction including motor dysf (strength of cough) and sensory dysf. (laryngeal sensation that triggers cough)
OHSU Parkinson Center
Dysphagia Assessment • Clinical Assessment of Swallowing • Objective evaluation
– Modified Barium Swallow Study
(MBSS)
– Fiberoptic Endoscopic Evaluation of Swallowing (FEES)
– Fernandez & Lapane. (2002) Predictors of mortality among nursing home residents with a diagnosis of Parkinson's disease.
OHSU Parkinson Center
Dysphagia Management
• Pt and caregiver education regarding s/s of dysphagia and aspiration
• Regular evaluations of pts with documented dysphagia • Compensatory Strategies
– Upright posture – Small bites/sips – Increase sensory input – Alternating liquids and solids – Chin tuck (maybe)
• Texture modification -Tjaden (2009)
Presenter
Presentation Notes
Sensory input:cold/hot, carbonated, highly seasoned foods,cold foods, sour foods.Luke warm and bland is worst Efficacy of these interventions can be established with MBS or FEES
OHSU Parkinson Center
Therapeutic Exercises • Active ROM exercises for tongue, lips, larynx • Sustaining high pitch which engages pharyngeal
wall contraction • Effortful swallow to improve BOT retraction,
clearance of residue • Mendelsohn Maneuver to increase laryngeal
elevation • Shaker exercises to improve hyolaryngeal
excursion
Presenter
Presentation Notes
Need for targeted exercises can be determined with MBSS or FEES
OHSU Parkinson Center
EMST and swallow safety • Promising treatment
– Expiratory Muscle Strength Training (EMST) – Randomized, blinded, sham-controlled study – EMST 5X/week for 4 weeks for 20 min per day – EMST group demonstrated improved swallow safety
as evidence by improved PA scores – EMST group demonstrated improvement of
hyolaryngeal function during swallow
– Troche et al (2010) Aspiration and swallowing in PD and rehabilitation with EMST
OHSU Parkinson Center
Improving Cough in PD • Promising treatment
– EMST to improve cough – 10 mid stage PD pts with penetration or
aspiration on MBS – 4 weeks of EMST – Significant decrease in duration
of the Compression Phase Duration and Expiratory Phase Rise Time; decrease in EPRT resulted in significant increase in cough Volume Acceleration
– Significant decreases in PA scores after treatment
Presenter
Presentation Notes
EMST-Aspire Products. PEMax-maximal exp pressure(start at 75% of this) Calibrated, one way, spring-loaded valve to overload the exp muscles mechanically The valve blocks the flow of air until sufficient exp pressure is produced The physiologic load on the targeted muscles can be increased or dec depending upon the device setting Result:HIGHER EXP FLOWS DURING COUGH
OHSU Parkinson Center
Contributing factors to dysphagia in mid-late stage • Cognitive impairment • Impulsivity when self feeding • UE Tremor • Dyskinesias • Poor awareness of dysphagia • Posture • Fatigue • Vision
Presenter
Presentation Notes
Can impact safe PO intake,weight maintenance, duration of meals PWP can benefit from CUES, CG training,adaptive equipment OT?=SLP
OHSU Parkinson Center
A word about drooling • Reported in >56% of pts • Secretion management vs sialorrhea
– 55% of PWP c/o xerostomia • Changes in sensation • Things that were once automatic are no longer automatic • Oropharyngeal dysphagia • Treatments:
urinary retention, drowsiness) or adrenergic receptor antagonists • Strategies:
– Think swallow – Before talking – Before bending – When concentrating – Intermittently
-Srivanitchapoom, Pandey & Hallett (2014)
Presenter
Presentation Notes
Poor secretion management: excessive pooling and poor control of saliva Sialorrhea: overflow or overproduction of saliva Many studies show that pts with pd produce less saliva than normal; can be related CL Dysphagia in PD: bradykinesia, reduced tongue fnction Increase awareness
OHSU Parkinson Center
When to talk about tube feeding…. • Important to understand pt's wishes • Usually in later stages of PD but some pts are more
proactive • s/s of dysphagia that are progressing • Conversation in conjunction with neurology/PCP • Offer support and understanding of implications of
TF • What does it mean to have TF?
– NPO? – Recreational PO? – Burden of PO – Extends life? – Prevents aspiration?
OHSU Parkinson Center
I takes a village..... • Keep an eye out • Weight Loss • Food/liquid avoidance • Taking longer to finish a meal • Coughing with water • Wet/gurgly vocal quality • Congestion • Fever
OHSU Parkinson Center
Key Challenges in Advancing PD Falls - Vision
Jennifer Wilhelm, PT, DPT, NCS Rosanne Yee, OTR-L
OHSU Parkinson Center
Falls
• Early PD: • 181 newly dx PWP vs 173 controls
– 64.1% of PWP fell over 7 years – 15% fell prior to dx; 13% within 1 year – Relative risk to controls: 3.1 – Higher rates of falls: higher age, UPDRS, PIGD
phenotype, dementia and lost to f/u
Hiorth Y et al; J Neurol 2017
OHSU Parkinson Center
Falls
• Hospital in Australia retrospectively looked at 342,265 fall-related hospital admissions ≥65 years
• 2.5% of falls were in PWP – Higher rate of admission – Longer hospitalization stay
Paul SS et al; Eur J Neurol 2017
OHSU Parkinson Center
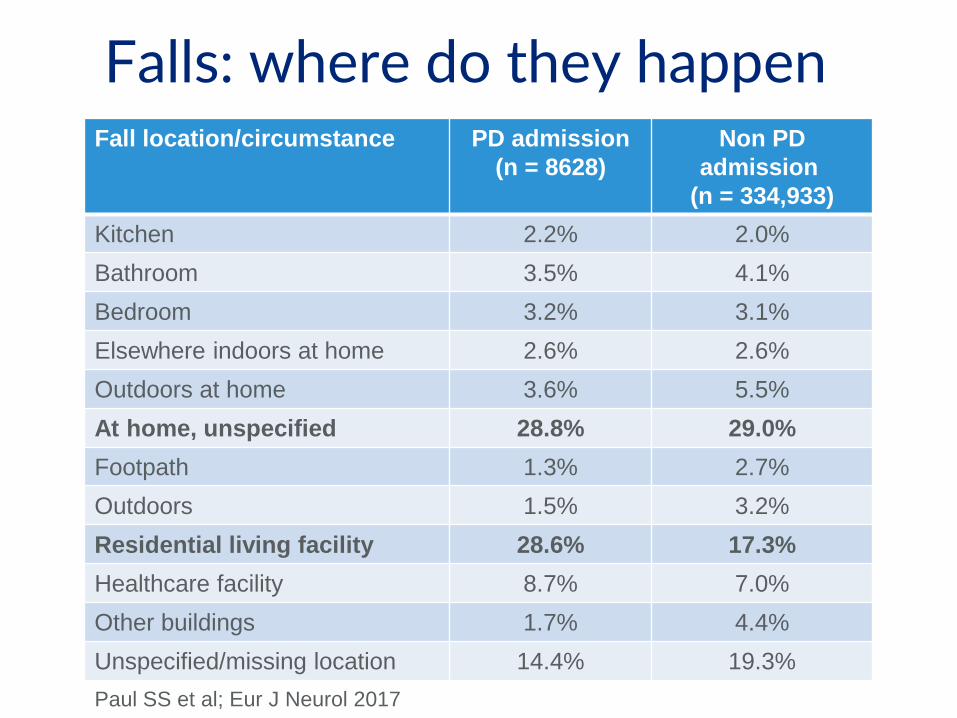
Falls: where do they happen Fall location/circumstance PD admission
(n = 8628) Non PD
admission (n = 334,933)
Kitchen 2.2% 2.0% Bathroom 3.5% 4.1% Bedroom 3.2% 3.1% Elsewhere indoors at home 2.6% 2.6% Outdoors at home 3.6% 5.5% At home, unspecified 28.8% 29.0% Footpath 1.3% 2.7% Outdoors 1.5% 3.2% Residential living facility 28.6% 17.3% Healthcare facility 8.7% 7.0% Other buildings 1.7% 4.4% Unspecified/missing location 14.4% 19.3% Paul SS et al; Eur J Neurol 2017
OHSU Parkinson Center
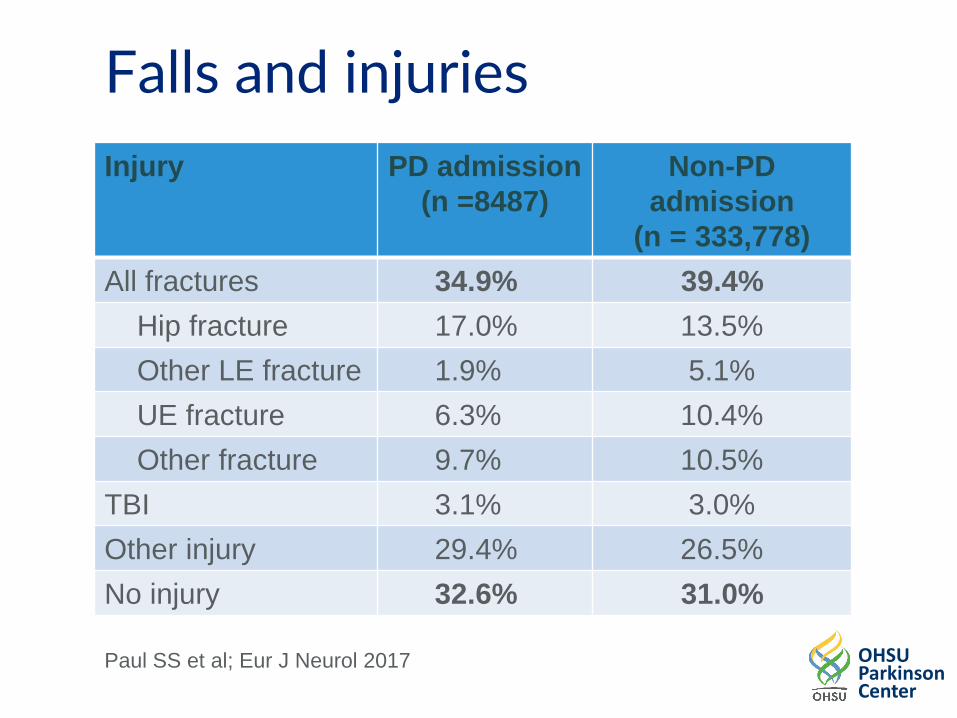
Falls and injuries Injury
PD admission (n =8487)
Non-PD admission
(n = 333,778) All fractures 34.9% 39.4% Hip fracture 17.0% 13.5% Other LE fracture 1.9% 5.1% UE fracture 6.3% 10.4% Other fracture 9.7% 10.5% TBI 3.1% 3.0% Other injury 29.4% 26.5% No injury 32.6% 31.0%
Paul SS et al; Eur J Neurol 2017
OHSU Parkinson Center
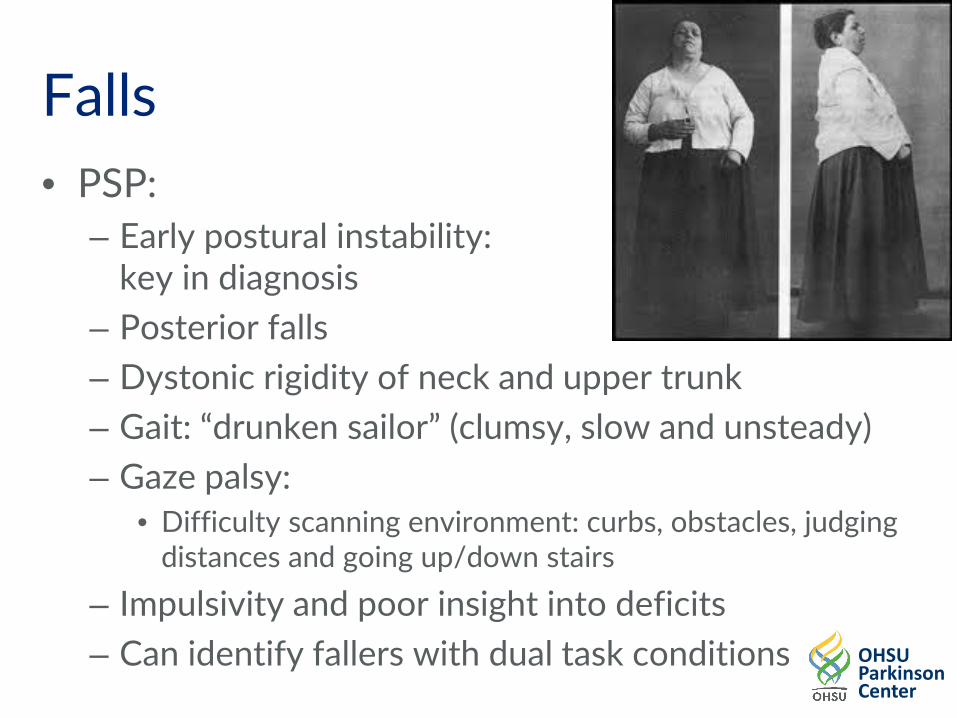
Falls • PSP:
– Early postural instability: key in diagnosis
– Posterior falls – Dystonic rigidity of neck and upper trunk – Gait: “drunken sailor” (clumsy, slow and unsteady) – Gaze palsy:
– Impulsivity and poor insight into deficits – Can identify fallers with dual task conditions
OHSU Parkinson Center
Falls
• PSP: Rapid progression of gait deficits – n = 50 pts with PSP followed
• To death (n = 21; mean duration 53.6 mo) • In ongoing fashion (n = 29; mean duration 46.2 mo)
– Loss of independent walking, inability to stand unassisted and requiring use of wheelchair
• Once you met 1 milestone: high probability of reaching others within 8 months
• All milestones occurred 59-62 mo from symptom onset; 36-39 mo from 1st visit
Goetz CG et al; Neurology. 2003
OHSU Parkinson Center
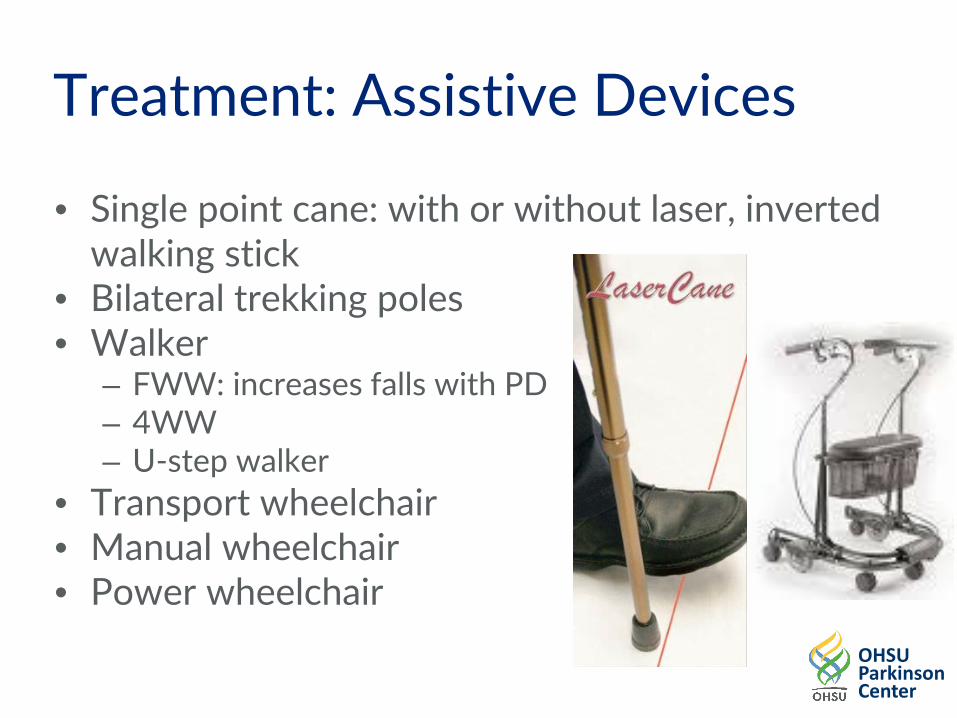
Falls: PT
• PSP – Heel wedge in shoe: shift COG anterior – U-step walker – Increase step height to improve clearance – Posterior stepping strategies – Increase base of support for ADLs: “Strong
stance” – Work with OT regarding visual scanning
and SLP regarding impulsivity
OHSU Parkinson Center
Falls
• MSA: – Can include cerebellar signs leading to ataxia – Often with bilateral involvement – Bradykinesia and rigidity – Initial symptoms in trunk and LEs – Can occur due to orthostatic hypotension – Often with urinary incontinence
OHSU Parkinson Center
Falls
MSA-C • Coordination
exercises • Narrow BOS • Unstable
surfaces • Strengthen
trunk and hip/shoulder girdle muscles
MSA-P • Similar
treatments as PD
MSA-A • Address
orthostatic hypotension
• 4WW with seat
• Transport wheelchair
OHSU Parkinson Center
Falls • Late Stage PD (study of n = 50; mean
duration of disease 17.94 yrs; H&Y 4/5) – Increased rate of falling with course of disease – Falls occurred in 50% of patients
• 28% had daily falls • 30% falls caused by freezing
– Caused an extreme impact on patients’ perceived health status
Coelho M et al; J Neurol. 2010 Sep;257(9):1524-32
OHSU Parkinson Center
Falls: PT • Late Stage PD (study of n = 24; mean duration of
disease 11 yrs; H&Y 4) – Impaired postural control in quiet stance: both static
and dynamic – Decreased ability to balance when vision or
proprioception is disturbed • Delay in adapting balance strategy with sensory changes
– High reliance on vision: even if it is conflicted – Postural strategies usually are ineffective to keep
balance and avoid falls: especially if dynamic conditions or if sensory info is conflicting
Colnat-Coulbois S et al; Neuroscience. 2011
OHSU Parkinson Center
Falls: PT
• Late Stage PD – Sensory integration training
• Try to decrease vision • Unstable surface: start with a towel
– Postural reactions: ankle, hip and stepping – Assistive equipment
• 4WW vs U-step walker: look at context • Wheelchair
Dry eyes and Decrease blink rate -Decrease tear production autonomic dysfunction solution use artificial tear, oral omega 3-6 and consciously increase blink freq Blepha means eye lid. Inflammed eye lid related to dry eyes. bacteria on the surface of the eye causing inflamation distortion of vision and pain Blepharospams abnormal, involuntary blinking or spasm of the eyelids. The reflex type occurs in response to certain stimuli, such as a sudden visual threat or auditory or tactile stimulus while Apraxia of eyelid opening is non-paralytic motor abnormality characterized by difficulty in opening the eyes at will in the absence of visible contraction �
OHSU Parkinson Center
Falls/Vision: OT Ocular Disorders Functional scan –Saccades tend to be slow and display delayed initiation –Pursuit movements become jerky and slow eye movements (cog-wheel) Depth Perception –Vergence becomes insufficient due to slowness of eye teaming and can result in eyestrain, headaches and double vision (diplopia) –Solution: eye exercises focused on concise movement and referral to neuro ophthalmology or neuro optometry
Presenter
Presentation Notes
Saccades-small rapid controlled movement of the eye that targets one point to another. Pursuits- tracking movements of the eyes designed to keep on a moving stimulus clearly. Vergence- both eyes together moving in different directions, (inward-convergence or apart divergence), while looking at an object in focus as it moves toward or away from our eyes.
OHSU Parkinson Center
Falls/Vision: OT Visual Disorders • Visual Processing
– Contrast sensitivity-problems seeing in low light during walking, ADLs and night driving. Solution: increase light. If too much glare yellow filtering glasses. Referral to Low vision optometry
– Colour discrimination-trouble with all colours except black and white. Solution: contrast colors
Presenter
Presentation Notes
Contrast sensitivity-the ability to differentiate the level of light emitted from a object or area. Colour discrimination-the ability to distinguish subtle differences in colour some studies say more trouble with red-green axis or blue-yellow axis
OHSU Parkinson Center
Falls/Vision: OT Visual Disorders
• Visual Processing – Visuoperceptual issues:
• Detection of motion • Human movement • Facial recognition
Presenter
Presentation Notes
Moving objects and people PD pt can bump into or be bumped
OHSU Parkinson Center
Falls/Vision: OT Visual Disorders • Visuospatial issues:
– Perception of space – Recognition of line orientation – Mental 3D rotation of object – ID figure embedded in complex figures – Visuospatial problem solving – Depth perception – Spatial working memory
Visuospatial dysfunction specifically associated to fatigue. (Is fatigue associated with cognitive dysfunction in early PD? B.M. Kluger at el. Parkinsonism and Related Disorders 37 (2017) 87-91)
Presenter
Presentation Notes
Visuospatial impairments related to freezing of gait Space perception awareness of the relative positions of their own bodies and objects around them. Line orientation in space Spatial Working Memory requires retention and manipulation of visuospatial information. Possible complaints of fatigue could be do to tasks that requires visuospatial attention or calculations Possible complaints of fatigue could be do to tasks that requires visuospatial attention or calculations
OHSU Parkinson Center
Falls/Vision: OT • PSP the predominant visual defects are:
– Vertical gaze palsy-vertical saccades slow and hypometric, both up and down direction
– impaired vergence – inability to modulate the linear vestibulo-
ocular reflex appropriately for viewing distance.
(The Disturbance of Gaze in Progressive Supranuclear Palsy: Implications for Pathogenesis A.L. Chen et al. Front Neurol. 2010; 1: 147.)
Presenter
Presentation Notes
Although some aspects of all forms of eye movements are affected in PSP these are the predominant � These vertical saccades and vergence eye movements habitually work in together to enable visuomotor skills that are important during locomotion (stairs curbs, uneven surfaces) hands free
OHSU Parkinson Center
Falls/Vision: OT • MSA Typical ocular features include:
– Blepharospasm-abnormal, involuntary blinking or spasm of the eyelids.
– excessive square-wave jerks-fixation instability – mild to mod saccade hypometria-undershooting
movement that is equal in magnitude but opposite in direction
– Nystagmus-involuntary movement of eye (Visual signs and symptoms of multiple system atrophy. Armstrong, Clin Exp Optom 2014 Nov;97(6):483-91.)
Presenter
Presentation Notes
Less typical features include slowing of saccadic eye movements, the presence of vertical gaze palsy, visual hallucinations Aspects of primary vision such as visual acuity, colour vision or visual fields are usually unaffected
OHSU Parkinson Center
Falls/Vision: OT OTs evaluate functional vision to understand how it hinders and facilitate occupational performance • Modify and adapt the environment • Increase contrast • Reduce patterns • Improve lighting • Magnification • Organization • Simplify tasks • Improve search of environment • Refer as needed to neuro-ophthalmologist/neuro-
optometrist
Presenter
Presentation Notes
no research yet supporting increased speed and ability of eye movements.
OHSU Parkinson Center
Falls: OT Examine home environment: • Rails for both sides stairs • Vertical grab bars when reaching overhead or opening doors • Remove clutter and throw rugs • Re-arrange environment to widen walking path and make
items more accessible • Good lighting and mark edges corners with contrasting colour
tape • Lower bars in clothes closet • Sit for shower, grooming and dressing • Education of family for future equipment needs for rapidly
progressing disease
OHSU Parkinson Center
Falls: OT Retropulsion triggers • carrying things in both hands in front • pulling or dragging anything ex. tools for house
and garden work Retropulsion compensation strategies • carry objects with handles at the side • use push rolling kitchen, laundry, garden cart to
transport items • sit to do self care
OHSU Parkinson Center
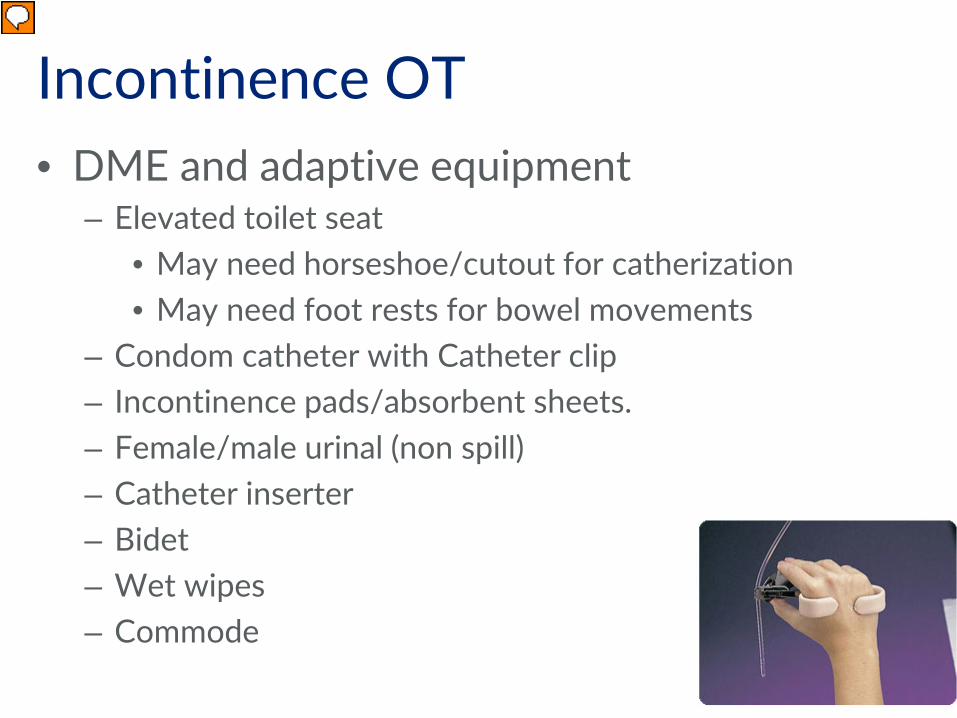
Key Challenges in Advancing PD Incontinence
Jennifer Wilhelm, PT, DPT, NCS Rosanne Yee, OTR-L
OHSU Parkinson Center
Incontinence • Seen primarily with MSA; can be early sign
due to autonomic dysfunction – 90.9% of MSA patients report symptoms
• PSP: 53.3% of patients report symptoms • Linked directly to quality of life
OHSU Parkinson Center
Incontinence
• MSA and end stage PD – Storage problems: frequency, urgency, urge
incontinence, noctureia
• MSA - can also have and may need to catherized
OHSU Parkinson Center
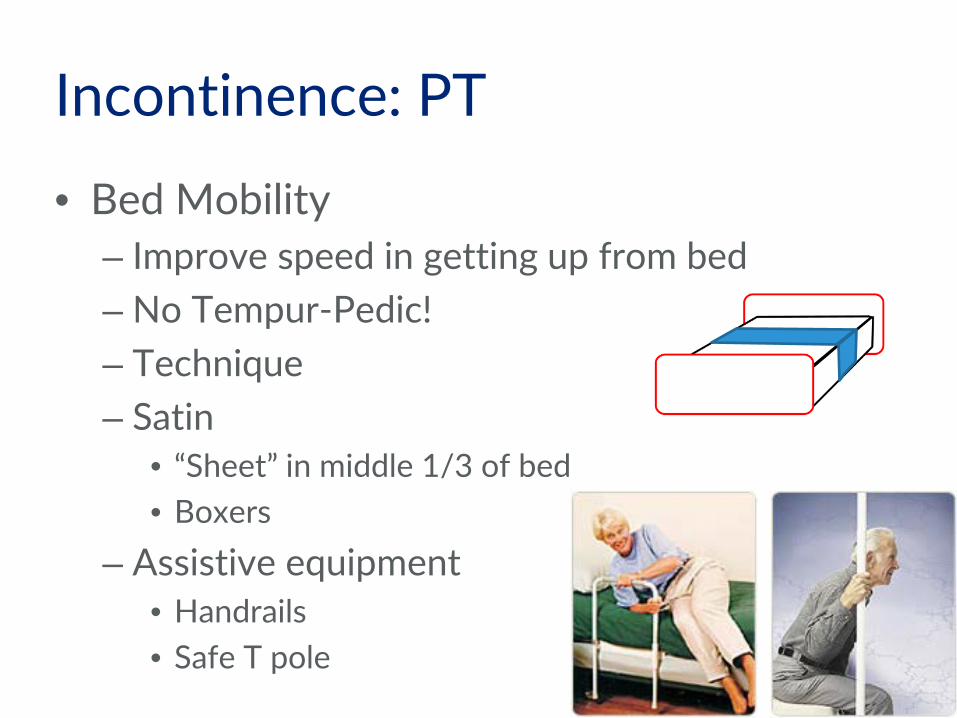
Toileting –behavioral modifications
Bladder • Record current habits/routine by using voiding diary • Monitor pm fluid intake
Bowel • Fiber and fluids • Height of toilet. • Exercise • Routine • Stress/rushing
Orthostatic Hypotension • Drop is SBP of at least 20 mm Hg or DBP of at least
10 mm Hg within 3 min of standing • Usually worse in the morning: nocturnal polyuria
results in reduced overall fluid volume • Other contributing factors
– Prolonged supine position – Quick position changes – Warm environment: lower BP in general – Ingestion of food
• Can lead to falls • Often multi-factorial for treatment
OHSU Parkinson Center
Orthostatic Hypotension
• MSA: commonly seen due to autonomic dysfunction – Occurs in 53-68% of patients – Causes falls in 54.6% of patients – Only 12% of patients were symptomatic with 24 hr
testing • PSP: less common
– Present in 8-13.3% of patients, usually with no symptoms
Colosimo C et al; J Neurol. 2010 Schmidt C et al; Mov Disord. 2009
OHSU Parkinson Center
Orthostatic Hypotension • Late stage PD (H&Y IV-5): often observed
– Present in 26% of patients; 8% of patients having syncope
– May not be as large of a problem: limited mobility prevents quick sit to stand
• 96% of patients had dysautonomic symptoms – Can occur due to medications (dopamine
agonists) – Incidence increases with higher age and longer
– Maneuvers to increase BP: 20/10 mm Hg; 30 sec intervals • Squatting • Lower body muscle tensing • Crossing legs • Bending over
Krediet CT et al; Clin Auton Res. 2008 Krediet CT et al; Circulation. 2002
OHSU Parkinson Center
Orthostatic Hypotension • Home evaluation/DME evaluation
– Commode next to bed – Barrier free way of getting to the
bathroom – Using bedside equipment – Condom catheter or bedside urinal – Good lighting
• Caregiver training
OHSU Parkinson Center
Orthostatic Hypotension: PT • Monitor vitals during treatment • Exercise: swimming due to hydrostatic
pressure • LE exercises in bed or at EOB
– Hold knees to squeeze the legs before rising; do 10 times on each leg.
Fujimoto K; J Neurol. 2009
OHSU Parkinson Center
Orthostatic Hypotension: PT
• Implications for exercise – Study of MSA pts (n=15)
• Exercise: Supine position, pedaling cycle ergometer at workloads of 25, 50 and 75 W, each for 3 min
• BP ↓ and stayed low for 10 min post exercise
• Vasodilation of skeletal muscle without compensatory vasoconstriction in other large vascular beds
Smith GD et al; J Physiol 1995
OHSU Parkinson Center
Key Challenges in Advancing PD Cognition
Aimee Mooney, MS, CCC-SLP-L
OHSU Parkinson Center
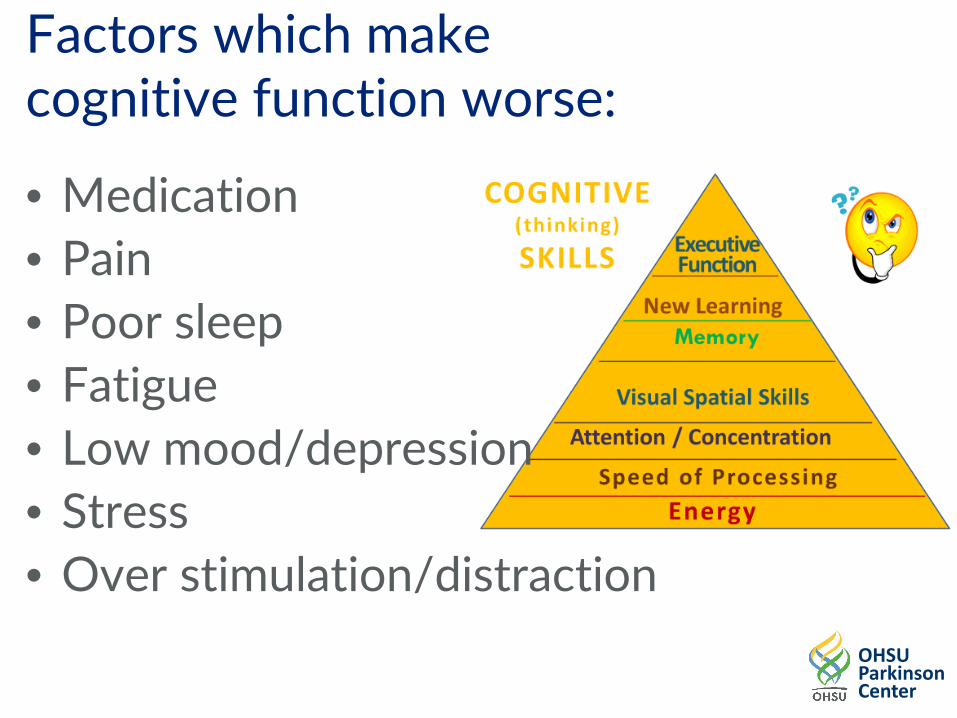
Cognition in PD Incidence: >40% experience cognitive impairment after 10 years, 75% of people have Dementia Type: heterogenic; yet: Working Memory Processing Speed Executive Functioning Learning Efficiency (slower, more reps)
Impact: Independence (driving), Safety, Quality of Life, Carepartner Burnout, Emotional and Psychological Health
OHSU Parkinson Center
Continuum of Cognitive Changes in PD Mild cognitive impairment is common in nondemented Parkinson's disease (PD) patients and may be a harbinger of dementia. The Movement Disorder Society commissioned a task force to delineate diagnostic criteria for mild cognitive impairment in PD. The proposed diagnostic criteria are based on a literature review and expert consensus.
Presenter
Presentation Notes
Litvan, I., Goldman, J. G., Tröster, A. I., Schmand, B. A., Weintraub, D., Petersen, R. C., Mollenhauer, B., Adler, C. H., Marder, K., Williams-Gray, C. H., Aarsland, D., Kulisevsky, J., Rodriguez-Oroz, M. C., Burn, D. J., Barker, R. A. and Emre, M. (2012), Diagnostic criteria for mild cognitive impairment in Parkinson's disease: Movement Disorder Society Task Force guidelines. Mov. Disord., 27: 349–356. doi:10.1002/mds.24893
OHSU Parkinson Center
PD-MCI Criteria
I. Inclusion criteria • Diagnosis of Parkinson's disease as based on the UK PD Brain Bank Criteria20
• Gradual decline, in the context of established PD, in cognitive ability reported by either the patient or informant, or observed by the clinician • Cognitive deficits on either formal neuropsychological testing or a scale of global cognitive abilities (detailed in section III) • Cognitive deficits are not sufficient to interfere significantly with functional independence, although subtle difficulties on complex functional tasks may be present II. Exclusion criteria • Diagnosis of PD dementia 18
• Other primary explanations for cognitive impairment (e.g., delirium, stroke, major depression, metabolic abnormalities, adverse effects of medication, or head trauma) • Other PD-associated comorbid conditions (e.g., motor impairment or severe anxiety, depression, excessive daytime sleepiness, or psychosis) that, in the opinion of the clinician, significantly influence cognitive testing
administering clinically, culturally and linguistically appropriate approaches to diagnosis and assessment of cognitive-communication disorders of dementia across the course of the underlying disease complex
Intervention: identifying appropriate
evidence-based practice techniques for direct intervention with persons with dementia and indirect intervention through their caregivers and environmental modifications.
Counseling: to individuals with
Dementia and their significant others about nature of their dementia and its course
Collaboration: To develop intervention plans for maintaining cognitive-communication and functional abilities at highest level throughout the disease course
Case Management: serve as
coordinator or team leader to ensure appropriate and timely delivery of comprehensive management plan
Patient Education: Key for all SLP Interventions for deficits in Cognition
• Patient and Caregiver education about cognition strengths and weaknesses, their impact on ADL’s, and type of supervision required
• Patient and Caregiver education about factors which contribute to difficulties with cognition (fatigue, stress, pain, depression, anxiety, sleep, meds)
OHSU Parkinson Center
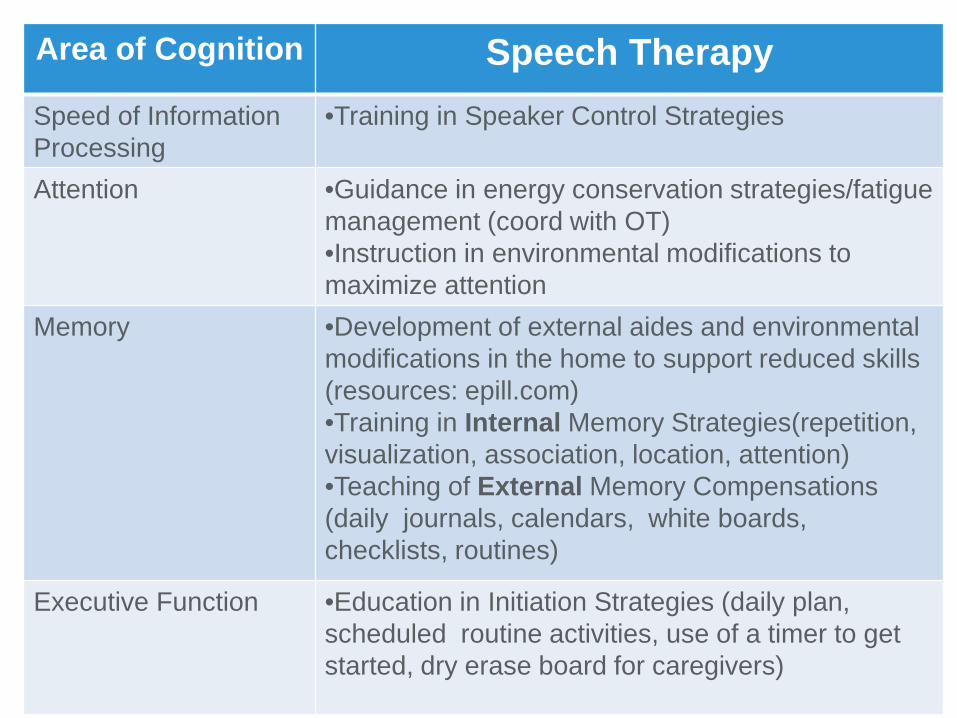
Area of Cognition Speech Therapy Speed of Information Processing
•Training in Speaker Control Strategies
Attention
•Guidance in energy conservation strategies/fatigue management (coord with OT) •Instruction in environmental modifications to maximize attention
Memory
•Development of external aides and environmental modifications in the home to support reduced skills (resources: epill.com) •Training in Internal Memory Strategies(repetition, visualization, association, location, attention) •Teaching of External Memory Compensations (daily journals, calendars, white boards, checklists, routines)
Executive Function •Education in Initiation Strategies (daily plan, scheduled routine activities, use of a timer to get started, dry erase board for caregivers)
OHSU Parkinson Center
SLP Treatment for Energy & Speed of Processing and Attention Training in energy conservation
strategies/fatigue management (coord with OT) Training in Speaker Control Strategies
Environmental Modification to
maximize attention (ie, reduce distractions, do one task at a time)
OHSU Parkinson Center
SLP Treatment for Memory Patient Education: Memory is an ACTIVE
process; you must consciously manipulate the information to get in into your brain.
Memory has 3 Stages: Input: when information is coming into
your brain; effected by: Storage: maintaining information;
consolidation with info you already know Retrieval: ability to access information
when it is needed.
OHSU Parkinson Center
Memory Strategies: the “why” • Remember to take medications as prescribed • Remember to use good posture strategies • Remember and keep medical appointments • Remember how to use adaptive equipment
and assistive devices • Remember to use safety swallow precautions • Remember golf score or bridge score • Remember stories that your granddaughter
tells you
OHSU Parkinson Center
Internal Strategies Repetition Association Visualization Location Mnemonics First Letter
External Strategies Write it down!!! Calendar/dry erase board Diary/memory book Paper & Pencil by each
Academy of Neurologic Communication Disorders and Sciences
Evidence Based Practice Guidelines for the Management of Communication Disorders in
Neurologically Impaired Individuals : DEMENTIA
• Spaced Retrieval Training • Montessori-Based Interventions • Validation Therapy • Graphic and Written Cues • FOCUSED Caregiver Training Program
OHSU Parkinson Center
Montessori-based interventions
• Based on work done with children by Maria Montessori in the early 1900s and continuing today.
• Basic technique is to create structured,
stimulating activities that are appropriate to an individual's cognitive abilities, allowing engagement in tasks and the opportunity for social interaction.
• Activities can be conducted individually with clients or in groups.
OHSU Parkinson Center
Validation therapy
• A method of communication initially described by Naomi Feil, a gerontological social worker
• Basic technique is to validate (through
words, gestures) what the person with dementia says, regardless of accuracy or basis in fact, rather than correcting or re-orienting the person
OHSU Parkinson Center
Graphic and written cues • Basic technique involves providing written
factual information and/or familiar photos to facilitate communication
• Capitalizes on recognition memory and the
ability to read aloud, both of which may be relatively preserved in many individuals with Alzheimer's dementia
• Photographs and words can be incorporated
into memory books/wallets, memo boards, and activity calendars
OHSU Parkinson Center
FOCUSED caregiver training program FOCUSED is an acronym for the key features of the communication enhancement program: F = functional and face-to-face; O = orient to topic; C = continuity of topic-concrete topics; U = unstick any communication blocks; S = structure with yes/no and choice questions; E = exchange conversation--encourage interaction; D = direct, short, simple sentences Designed to be used with both family and professional caregivers
OHSU Parkinson Center
Cognitive Intervention: 5 evidence-based principles for enhancing learning in Dementia
1. Strengthen memory traces with repetition 2. Engage the non-declarative memory system:
active involvement promotes better learning 3. Reduce errors during learning. Minimizing
errors during learning is essential b/c every time an error is repeated, this erroneous response is strengthened. (Spaced Retrieval)
4. Structure intervention so clients focus attention on a single task
5. Use salient cues to aid successful retrieval (free recall harder than cued recall or forced choice)
OHSU Parkinson Center
Other considerations re: Cognition
• Cognitive Stimulation • Maintain participation in as many activities
as possible- and train caregivers about this!!
OHSU Parkinson Center
Utilizing the knowledge and power of Neuroplasticity
• Neuroplasticity: The ability of the brain to change and adapt to circumstances of injuries by forming new pathways, making new cells and getting bigger.
• Patient Message: “You can make a difference in the course of your disease by what you choose to do.” – Exercise – Cognitive Fitness – Emotional Resilience
OHSU Parkinson Center
Recommendation • Exercise in Stimulating environment
with a range of cognitive and sensory stimulating activates
• Watermeyer, T. J., Hindle, J. V., Roberts, J., Lawrence, C. L., Martyr, A., Lloyd-Williams, H., ... & Clare, L. (2016). Goal Setting for Cognitive Rehabilitation in Mild to Moderate Parkinson’s Disease Dementia and Dementia with Lewy Bodies. Parkinson’s Disease, 2016.
• Vlagsma, T. T., Koerts, J., Fasotti, L., Tucha, O., Van
Laar, T., Dijkstra, H., & Spikman, J. M. (2016). Parkinson's patients’ executive profile and goals they set for improvement: Why is cognitive rehabilitation not common practice?. Neuropsychological rehabilitation, 26(2), 216-235.
OHSU Parkinson Center
Key Challenges to Late Stage PD
Communication Linda Bryans, MA, CCC-SLP-L
Aimee Mooney, MS, CCC-SLP-L
OHSU Parkinson Center
Patient’s Communication
Care Path
Stage 1 Normal Speech
Processes
Stage 2 Detectable Speech
Disturbance
Stage 3 Reduction in speech
intelligibility
Stage 4 Natural speech
supplemented by Augmentative and
Alternative Communication
Stage 5 No Functional
Speech
What’s going on with your speech and writing?
Is your voice soft? Are you or others noticing changes in your voice?
Do others ask you to repeat? Is your voice soft? Are you noticing stuttering or mumbling?
Is your voice soft? Are you mumbling? Are you talking less or avoiding some communication situations?
Are you giving up on conversations? Is your voice inaudible? Are you communicating less, to a smaller group of people? Have you limited your topics and messages?
Do you rely on nonverbal ways of communicating with your carepartner, family and friends? Have you stopped or limited your participation in conversations?
Assessment
Your PCO health care provider or Speech-Language Pathologist (SLP) will listen for any changes in your voice, loudness or speech.
Your SLP will listen to your speech and voice and evaluate for changes in loudness, voice quality, articulation and overall speech intelligibility. An ENT or SLP may look at your voice box.
Your SLP will listen to your speech and voice and evaluate for changes in loudness, voice quality, articulation and overall speech intelligibility . Your SLP will help you identify best strategies for your needs.
Your SLP will: -Listen to your speech and voice and evaluate for changes in overall speech intelligibility. -Evaluate of your communication needs. -Conduct a formal augmentative and alternative communication (AAC) assessment.
Your SLP will help you identify the best speech generating device and low technology options to meet your communication needs.
Intervention
If your voice is noticeably soft or hoarse, you may benefit from Lee Silverman Voice Treatment (LSVT) to improve loudness and quality of your voice.
If your voice is noticeably soft or hoarse and speech slurred, you may benefit from Lee Silverman Voice Treatment (LSVT) to improve loudness and quality of your voice.
-You may benefit from LSVT to improve loudness and speech. -Have an attention getting strategy -Consider voice amplification as needed -Suggest changes in your environment for more effective communication
No matter how difficult it is to “talk”, you CAN still communicate. Consider a speech generating device to use when oral speech is inadequate. Consider voice amplification if voice is weak and volume is low.
Consider a speech generating device for functional communication and daily needs. You will learn how to use the speech device for conversation and telephone.
Patient Education Your SLP will give you information about possible changes in your speech and communication due to PD. Other services are available through the PCO.
Your SLP will provide you with information about: -LSVT -Ways to make your speech more understandable -Ways to enhance your written and verbal communication -Planning and preparation for further changes in communication.
Your SLP will discuss enhancement techniques: -LSVT -Loudness and rate exercises if needed -Learning to use low technology strategies -Preparing for other “tools” for speech and written communication.
Your SLP will provide you and your communication partners will information about resources for a communication system. The system will most likely include: -Your natural speech, gestures, and facial expressions; -Low and/or high tech
i t
Your SLP can help provide information and ways to change your communication system as needed. The ways you use your communication system are based on the time of day, medication regimen, your communication partners, and the disease progression.
Presenter
Presentation Notes
These are pts in stages 4 and 5. they may be struggling more to communicate, withdrawing from communication situations, not participating as they once did. This is where is gets more difficult to optimize communication. This is where the real work begins. Most SLPs are aware of the need to approach these pts from a multimodality perspective. OT/PTs need to be aware that these pts can benefit from intervention…..maximizing commmc by supporting commc with nonverbal or combines methods.
OHSU Parkinson Center
Late Stage PD • Stages 4 and 5 • Most patients have had LSVT….maybe • More barriers to successful LSVT outcomes • Complexity of communication disorder in context
of progression of disease and other health issues • May need to used combined interventions • Care Partner support and education
Presenter
Presentation Notes
These pts may be hard to capture. Usually have had DBS, physicians may not see benefit of referring back to SLP As a team, we need to be aware of these pt’s specific needs and their potential to communicate, even at end stage.
OHSU Parkinson Center
How can I help my pt with advanced PD? • Prioritizing needs and interventions
– What is important to my pt? • Refresher LSVT with multimodality communication support as
needed….and if pt is able/interested • Team approach to managing complex problems in PD
– SLP spear heads communication – OT can facilitate access of supports – PT can support with positioning – All disciplines can support communication
• Refer to SLP if pt is struggling with cognition or communication • Encourage use of loud voice, communication supports, communication
strategies
• Care Partner support and education
Presenter
Presentation Notes
TEAM: Neuro (fellow, PA, NP), SLP, PT, SW, RN What is most important to patient and CG? Identifying more pts at end stage
OHSU Parkinson Center
Treatment considerations
Four purposes of communication
(Light, 1988) – Express wants and needs
– Information exchange
– Social closeness
– Social etiquette
“Communication is not only the essence of being human, but
also a vital property of life.” John Piece
Presenter
Presentation Notes
Pts need to be able to do more than just communicate basic needs. When we review Light’s 4 purposes of communication, we see that commc serves to exchange information, provide social closeness and social etiquette. Impt to remember that communication is not only the essence of being human, the also a vital property of life. Recent research by Holt-Lundstad and collegues has demonstrated that social connectedness or lack there of is a risk factor for mortality – on the same par as obesity, smoking, etc***
OHSU Parkinson Center
OHSU Parkinson Center
Communication Disorders in Older Adults -Palmer et al (2016)
Predictor of: Smaller social networks
Fewer positive social
exchanges
Less frequent participation in social
activities
Higher levels of loneliness
Potentially leading to:
Social isolation
Reduced social
participation
Increased loneliness
Placing older adults at risk for:
Increased risk for mental and physical
health problems
Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: a meta-analytic review. Kawachi,I.,&Berkman,L.F.(2001).Social ties and mental health.
Presenter
Presentation Notes
We know that pts with PD do demonstrate decreased participation (Werthhiemer et al ***; Miller et al ***
OHSU Parkinson Center
PD are at risk for decreased participation and social isolation
• PD patients socialize less • PD patients avoid participation in
communication
• Wertheimer, Gottuso, Nuno, Walton, Duboille, Tuchman, & Ramig (2014) • Miller, et al (2006)
Presenter
Presentation Notes
We know from the work of C Baylor and N Miller that PD pts change patterns depending upon a variety of variables that contribute to interfere with communication. Interference can be functional or emotional. Pts make decisions based on symptoms, environment and personal priorities.
OHSU Parkinson Center
Keeping pts engaged and staying socially connected…including 4 purposes of communication
endurance • Social participation • Consider complexity of communication challenges
– Hypokinetic dysarthria – Cognitive communication challenges – Apathy?
• Amplification – Personal amplifier – Amplified telephone
• Augmentative Alternative Communication – Supported communication
• Care partner education
Presenter
Presentation Notes
So, what we all want to do is Keep pts engaged and socially connected. What commc situations or environments is the pt w/d from or avoiding. Not playing bridge, not answering or talking on the phone. Looking at what your pt needs and wants. OT/PT be on the look out for withdraw from participation…refer
OHSU Parkinson Center
Communication Supports
Presenter
Presentation Notes
Identify current strategies and what is working We all use all these things; when we work with families, we’re not introducing a brand new system; just shifting the balance = better buy-in
OHSU Parkinson Center
A shift toward aided approaches Fried-Oken, Beukelman & Hux, (2012)
• Expressive language less efficient
• Verbal participation decreases • Telephone use declines or is
avoided • Conversations become
imbalanced
OHSU Parkinson Center
Communication demands Settings
• Employment • Home • Groups • Community events
Partners
• Familiar/Unfamiliar Topics
• Familiar vs. unfamiliar
Modes of communication • Telephone • Face to face, spontaneous • Written • Electronic (email, text)
OHSU Parkinson Center
Partners and Modes:
Partners • Primary partner? • Most skilled? • Spends most time with ? • Willing to learn new
communication skills? • Willing to teach others
how to communicate with individual?
Modes • Influence by the situation,
intent, content and individuals involved
• Performance is multi-modal
• Modes uniquely constrain types of information conveyed
OHSU Parkinson Center
Communication Supports
UNAIDED: Natural • Speech • Vocalization • Gestures • Eye gaze • Body language • Sign language • Partner co-
construction
AIDED: Low & High tech • Paper and pencil • Communication
books boards and cards
• Speech generating devices
• Mobile technologies and apps
flex
ible
mu l t i -modal
Presenter
Presentation Notes
Aided- low tech to high tech (starting with speaking computers); on a natural continuum We talk about each person as having a full communication system with many modes to comm. Left = unaided (just using body) or another person (person who can’t think of the word and their wife knows it)- things that don’t require any THING; on right are aided approaches (aids or tools) tools range from low-tech all the way to high tech tools; We all use all these things; when we work with families, we’re not introducing brand new things; just shifting the balance = better buy-in
OHSU Parkinson Center
Low tech options – Paper/pencil
– Communication books
– Photo albums
– Pictures
– Newspapers
– Communication boards
– White board
OHSU Parkinson Center
Low tech options – Cards – Remnants – Written choice and
continuum lines – Paper and pencil – Lanyards
OHSU Parkinson Center
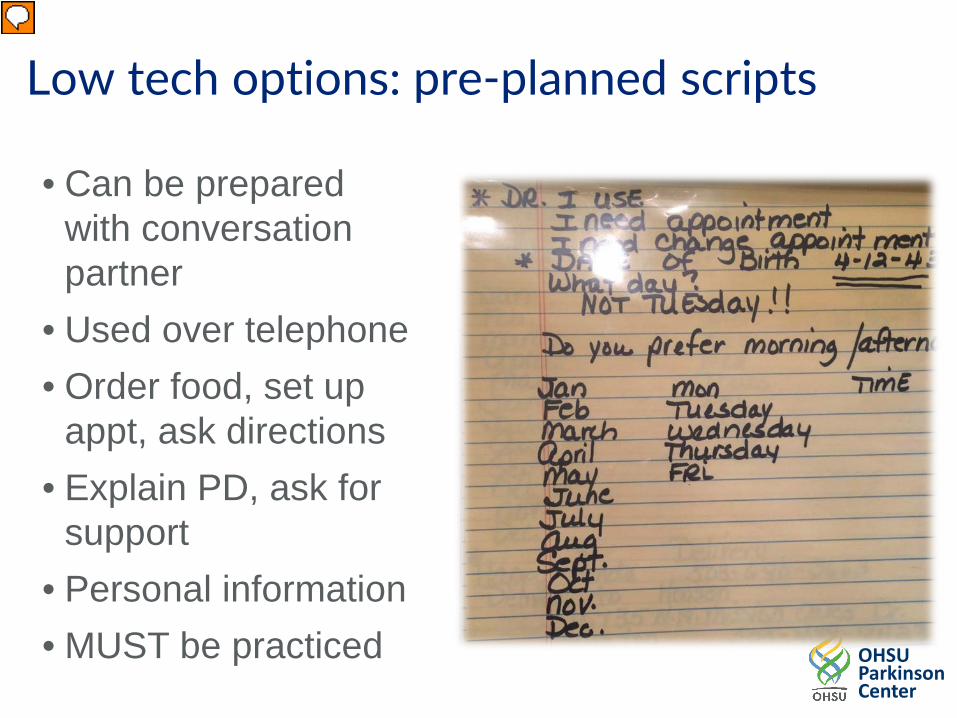
Low tech options: pre-planned scripts
• Can be prepared with conversation partner
• Used over telephone • Order food, set up
appt, ask directions • Explain PD, ask for
support • Personal information • MUST be practiced
• Magazine/Ads/Newspaper • Maps • Museum brochures • Newsletters (school,
neighborhood) • Numbers • Paper & pen/writing • Photos & photo albums • Post it notes • Scrap book • Show Me • Skype
Presenter
Presentation Notes
What do we notice?? We ALL Do these things!
OHSU Parkinson Center
High tech options
• Dedicated speech generating devices
• Mobile technology devices
OHSU Parkinson Center
Mobile Technology • Social acceptance • Consumer empowerment in accessing assist • Connections to social network • Native applications • Multiple Communication applications: ProLoquo2Go Lingraphica SmallTalk Pictello Scene and Heard Verbally Sounding Board Doceri White Board
Presenter
Presentation Notes
“I bought this for my Mom”… But she gets so confused going from page to page… Still need to do PERSON to TECHNOLOGY matching!!
OHSU Parkinson Center
Shift to environmental modifications “Engineering the environment” means ... • Using ALL previous compensations and
determining what CURRENTLY fits.
• training use of natural supports • training partners
OHSU Parkinson Center
Natural environmental supports • Pointing to weather pictures in newspaper to
indicate time of day • Using mail received from the bank to indicate
questions about finances • Flipping through pictures in photo book during
family visit • Remnant boxes • Sharing news about religious services by looking at
bulletin together • Native apps on mobile devices (weather, photos,
calendar, maps, etc)
OHSU Parkinson Center
As person with PD loses speech/voice/language, partner assumes more responsibility for interaction and message co-construction.
Evidence shows training is effective in improving communication activities and participation.
• identify vocabulary for external lexicon • support use of tools in different settings • initiate conversation during late stages of PD • train other partners
Communication Partner training (see updated Systematic review by Simmons-Mackie et al, 2016)
Presenter
Presentation Notes
Turner & Whitworth (2006) 9 studies of communication partner training in aphasia reported favorable outcomes Type or severity of aphasia did not matter Bradley & Douglas (2008) 19 studies of communication partner training in aphasia reported favorable outcomes Wilkinson, R. & Wieleart, S. (2012) 6 studies of ‘conversation analytic’ approaches reported positive outcomes of dyad training Simmons-Mackie 2014 IARC Update since the Simmons-Mackie et al. 2010 systematic review 14 additional published research articles All 14 reported positive outcomes from partner training
OHSU Parkinson Center
Communication Partner training:
Communication ramp!
Communication access
Minimizes communication disability
OHSU Parkinson Center
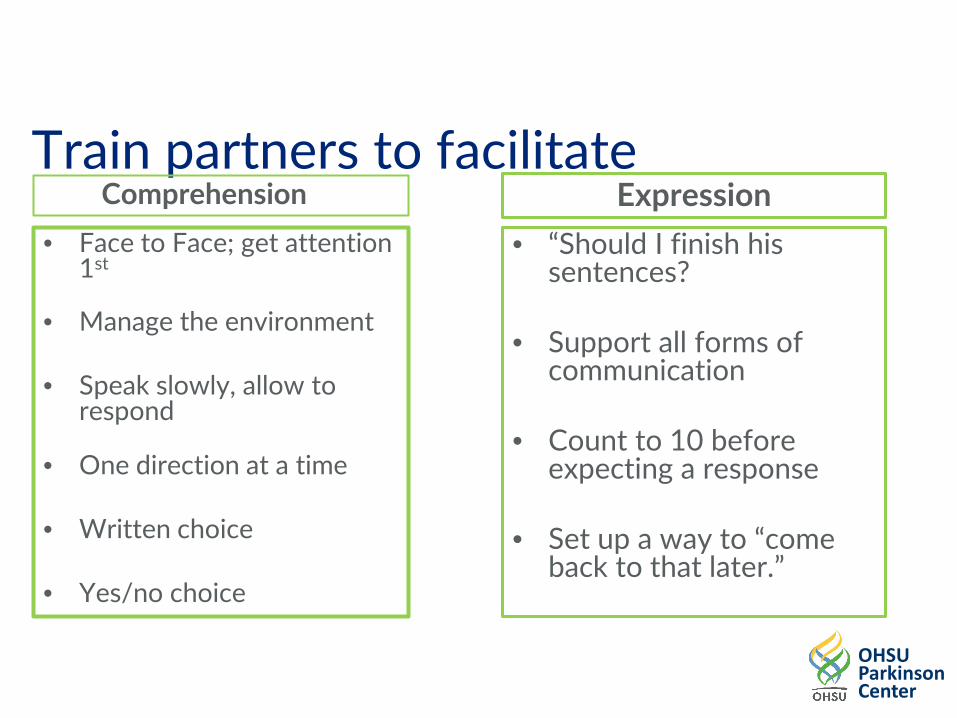
Train partners to facilitate Comprehension
• Face to Face; get attention 1st
• Manage the environment • Speak slowly, allow to
respond • Augmented inpwith pictures
• One direction at a time • Written choice • Yes/no choice
Expression • “Should I finish his
sentences? • Support all forms of
communication • Count to 10 before
expecting a response • Set up a way to “come
back to that later.”
OHSU Parkinson Center
Training Communication Partners 1. ID partner behaviors that elicit desired client
outcomes 2. Start small and expand after mastery 3. Use Systematic Instruction CHOOSE to take strategic approach: imPAACT Program (Kent-Walsh &
McNaughton, 2005) Communication Partner Instruction Model
5 Instructional Components: Video Review, Modeling, Role Play, Verbal Rehearsal, Coached practice The ImPAACT (Improving Partner Applications of Augmentative Communication Techniques) CPI designed to assist stakeholders with learning, generalizing, and applying strategies supporting individuals with CCN
OHSU Parkinson Center
Amplification
• Crutch or support • When amplification should be considered • Amplified telephone application
– Public Utility Commission (PUC) – http://www.puc.state.or.us/rspf/tdapapp.pdf
Presenter
Presentation Notes
When pts are withdrawing from communication Case: Steve, gradual intro to amp. Started with public speaking, gradually with wife and friends. Became more accepted by him and his friends/family
OHSU Parkinson Center
PUC Speech-to-Speech
• http://www.oregonrelay.com/ • 711 or 877-735-7525 • Speech-to-Speech (STS) allows a
speech-disabled person to voice his/her conversation.
• A specially trained STS operator repeats the words of the person with a speech disability or synthesizer output to the other person.
• No special equipment is needed to use this service
OHSU Parkinson Center
Team supported communication How can we work together as a team to support communication?
– Can they provide input regarding their care/goals/needs? (express needs)
– Can they tell you about their weekend? (exchange
info) – Can you get to know them? (social closeness)
– Can your pt greet you? (social etiquette)
OHSU Parkinson Center
Supporting participation For example…. • Intervention several years ago with group tx,
LSVT, medialization thyroplasty • Withdrawing from conversations • “It’s not just being heard” • Fast moving conversations • Initiation
– He just doesn’t talk at home • Refresher LSVT in context of conversational
strategies • Involving wife, family and friends • Invite PWP to participate • Practice strategies to stay in conversation
Presenter
Presentation Notes
Seen in NSC with his wife. Beginning to w/d from conversations. NEEDS FOR SUPPORT SHIFTING FROM LOUD TO COGNITION AND SPEAKER CONTROL Speaker control strategies (Aimee): ask to slow down, one thing at a time, ask to repeat or clarify, take notes, etc
OHSU Parkinson Center
Key Challenges in Late Stage PD
Pain
Jennifer Wilhelm, PT, DPT, NCS
OHSU Parkinson Center
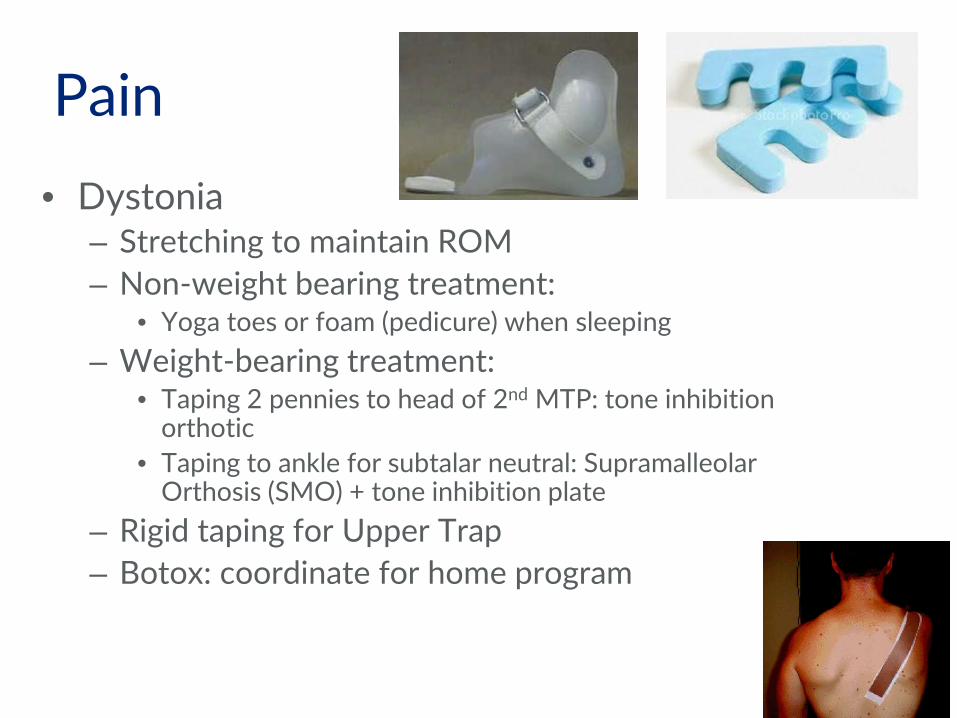
Pain
• Pain and PD: Recent cross-sectional survey (n =181; Germany; H&Y 1-5) – 95% of PWP reported pain
Addresses localization, intensity, and frequency of pain as well as its relationship with motor fluctuations or musculoskeletal pain.
OHSU Parkinson Center
OHSU Parkinson Center
Pain
• Late stage PD – Varies greatly between studies
• 24% of patients reported severe, disabling pain • 67.3% of PD patients (avg 6 yr duration) with pain
(Negre-Pages (2008): see next slide) – Paresthesias: 20% – Dystonia: 48%
Coelho M et al; J Neurol. 2010
OHSU Parkinson Center
Pain
• MSA: – 70.6% of pts had complaints of pain
associated with disease progression – Often affect extremities > neck/spine – Most common: sensory symptoms
• Cold or burning sensations • Paresthesia • Numbness
– Dystonia: can be related to levodopa
OHSU Parkinson Center
Pain
• MSA/(PSP): Antecollis (head drop) – Stretching – Positioning (work with OT) – Tilt-in-space wheelchair – *Botox NOT used due to concerns with
swallowing
OHSU Parkinson Center
Pain • PSP:
– 40%-56% of patients reported symptoms – Often non-specific – Dystonia: axial (antecollis or extension of neck)
or flexion of hands – Case study for chronic neck pain
• IV administration of lidocaine x 30 min every 2 wks: dramatic improvement in pain for 10 days and improvement in QOL
Colosimo et al; J Neurol. 2010 Shrag A et al; Mov Disord. 2010 Schlesinger I et al; Clin Neuropharmacol. 2009
OHSU Parkinson Center
Pain
• Musculoskeletal – Related to rigidity, postural changes and co-
morbidities • Dystonia
– Occurs during “off” or peak dose • Neuropathic
– Radicular pain from compressive root lesions, focal or peripheral neuropathy
• Central – Unusual burning, unrelated to motor phenomena – Neurontin
• Akathisia: inner restlessness – Restless leg syndrome
OHSU Parkinson Center
Pain • Musculoskeletal
– Most common type of pain – Found in #1 low back, knee, shoulder – Re-balance muscles: stretch the flexors – Education: joint protection – Rotational exercises to decrease rigidity – Bracing – Consider ortho or pain consult: injections or