Page 1
Long dedication to his country and his legacy as a unifying Long dedication to his country and his legacy as a unifying national leader…respected internationallynational leader…respected internationally
Ban KiBan Ki--Moon: Moon: PastPast UN chief UN chief
The Most Beloved King ForeverThe Most Beloved King Forever
King Bhumibol Adulyadej King Bhumibol Adulyadej
Page 2
Perioperative Care forPerioperative Care forKidney Kidney TransplantionTransplantion
Anesthetic Point of View Anesthetic Point of View
Experience from Experience from 22,,000 000 casescases
Siriwan JirasirithamSiriwan JirasirithamProfessor Emeritus of Anesthesiology Professor Emeritus of Anesthesiology
Department of Anesthesiology Ramathibodi Hospital Mahidol University THAILAND
Page 3
Sirikit Building for Sirikit Building for Excellent Center of Organ TransplantationExcellent Center of Organ Transplantation
Page 4
Safe Anesthesia for Kidney Transplantation
• Topics for discussion :
- Deceased donor management
- Recipient evaluation and preparation
- Anesthesia for kidney transplantation
Page 5
Ramathibodi Hsp
Annual Rate of Kidney Transplantationin Thailand
Page 6
Ramathibodi Hsp
Accumulated Rate of Kidney Transplantationin Thailand
Page 7
106111
118122
148
138
186
120
140
160
180
200
No.
Kidney Transplantation
In Ramathibodi Hospital
Today Today --23102310//15215231 31 October October 20172017
311
33
20
36 38 3439
43 46
58
7680 78
44
5766
91
45 44
61
75 72
82
106
0
20
40
60
80
100
86 88 90 92 94 96 98 00 02 04 '06
'08 10 12 14 16 Yr.
Total = 1839 casesTotal = Total = 2309 2309 casescases
Page 8
Kidney graft survival : Rama vs UNOS
0.50
0.75
1.00
Kaplan-Meier survival estimates
0.00
0.25
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15years
Living DDKT
Donor type 5-year graft survival 10-year graft survival
RAMA KT UNOS RAMA KT UNOS
DDKT 93% 70% 80% 40%
LRKT 94% 82% 78% 60%
Atiporn Ingsathit Ramathibodi Transplant Registry
Page 9
The Real Hero The Real Hero
Page 10
Deceased Donor Kidney Procurement
27/12/16
Page 11
Ramathibodi Organ Procurement TeamRamathibodi Organ Procurement Team
Page 13
Donor Promotion in Thailand
Education, workshop all over the country
Extended criteria donors
Extreme age : Newborn, pediatrics
: Elderly upto 72 year-old
Donor with comobid diseases
Donor with increasing creatinine level Donor with increasing creatinine level
Donor with HBs Ag
Future TrendsFuture Trends
-- Donation after circulatory death (DCD)Donation after circulatory death (DCD)
-- Kidney pair donation (KPD)Kidney pair donation (KPD)
-- Donor with HIVDonor with HIV
Page 14
Deceased donor: CharacteristicsDeceased donor: CharacteristicsP
erce
nt o
f gi
ven
ch
arac
teri
stic
s Hypotension, 92.8%
Last creatinine
Per
cent
of
giv
en c
har
acte
rist
ics
Year
Age >50 yr, 25.3%
Last creatinine >1.5 mg/dl, 53.1%
Stroke, 32.4%
CPR, 15.6%
Thai Red Cross National Organ Donation CenterThai Red Cross National Organ Donation Center
Page 15
1. Shortage of organ donation
2. Family denying or refusing to donate the organ
3. Loss of potential donor at ward ; ICU
Problems of organ donation :
Rapid deterioration of potential donor’s hemodynamic
Declaration of brain death : not in time
Cardiac arrest and failure of resuscitation process
Page 16
Criteria for Criteria for IDEALIDEAL Potential Cadaveric Donor Potential Cadaveric Donor
1. Age < 65 years
2. No previous kidney disease
3. Anti HIV negative
4. No history of malignancy.4. No history of malignancy.
5. No active generalized infection
6. Normal BUN , Cr
7. Urine output > 0.5 mL / kg
8. No intraperitoneal contamination
9. Not in state of shock
10.Warm ischemic time < 60 minutes
Page 17
Unsuitable of potential donor : Unsuitable of potential donor :
High fever with sepsis
High baseline creatinine level High baseline creatinine level
Hepatitis infection : Hepatitis B, C
Exclusion criteria : AIDS , Cancer
Page 18
Recipients : Recipients : Severe comorbidity or uncontrolled underlying
diseases
Active disease at the moment : acute diarrhea.
Not well prepared, dialysed , anemia, volume ,
electrolyte , coagulopathy , antiplatelet
Positive Cross Match
Page 19
Potential donor care and Potential donor care and
management management : :
Criteria of potential donor
Progression of brain death
Criteria of declaration of brain death
Management of brain death donor
Page 20
Diagnosis of Brain Death
Preconditioning : apnoeic coma following known etiology
: resulting in irreversible brain damage
Exclusions : reversible causes of coma must be excluded
Sedative drugs (narcotics, hypnotics, tranquillizers, elicits)
NMB drugs (use nerve stimulator : TOF) NMB drugs (use nerve stimulator : TOF)
Hypothermia (must be > 34oC)
Circulatory, metabolic, endocrine disturbances
Physiological consequence of BD
Must be corrected ( consciousness)
Level of hormone concentration
E’lytes, BS, ABG
Page 21
• Clinical Testing :
- Apnea at PaCO2 = 50 mmHg
Clinical Diagnosis of Brainstem Death
- 5 Brain stem reflexes:
1. No pupilary response to light
2. No corneal reflexes
3. No vestibule-ocular reflexes
4. No motor response, CN,somatic
5. No gag reflex- to bronchial stimuli
Page 22
In Thailand In Thailand 6 6 hours duration for clinical Tests ofhours duration for clinical Tests of
Brain Stem function absence Brain Stem function absence Brain Stem function absence Brain Stem function absence
Page 23
CV parameters Target range
HR 60-120 beats min-1
SAP >100 mmHg
MAP >70 mmHg but < 95 mgHg
CVP 6-10 mmHg
Cardiovascular Targets for Potential Cardiovascular Targets for Potential OOrgan rgan DDonorsonors
CVP 6-10 mmHg
PAOP 10-15 mmHg
SV variation <10%
FTc (Flow time corrected) on esophageal Doppler 330-360 ms
CI >2.1 L. min-1 m-2
Mixed venous saturation >60%
Continuing Education in Anaesthesia. Critical Care & Pain, MAY, 2012.
Page 24
Cardiovascular Management
GOAL
Normovolemia
Maintain adequate blood pressure Maintain adequate blood pressure
Optimize cardiac output
Promote organ perfusion
Early management to potential organ donor
Page 25
Donor for Lung Retrieval
Minimized crystalloid infusion
Avoid high CVP (<10 cmH2O)
MAP > 70 mmHg, Systolic BP > 85 mmHg MAP > 70 mmHg, Systolic BP > 85 mmHg
Early inotropic support
Keep urine flow ~ 1 mL/kg/hr
Page 26
Donor for Heart retrieval :
Best choice of inotrope alpha - adrenergic agent
(metaraminol, phenylephrine)
Maintain coronary perfusion pressure
Limit in myocardial O2 consumption
(heart rate)
Page 27
1. myocardial energy
2. glycogen storage
3. lactate accumulation and free fatty acids
ADVANTAGE OF HORMONE
THERAPY IN BRAIN DEAD DONOR
3. lactate accumulation and free fatty acids
4. Inhibit natural course of metabolic deterioration
5. Improve cardiac, renal functional stability in recipient
6. inotropic and bicarbonate requirement
7. Improve graft function *
Page 28
Inflammatory process => role of steroid therapy
methylprednisolone 14.5 mg/kg/day
significant improve oxygenation
Follette DM, et al. J Heart Lung Transplant 1998:17:423-9.
Crit Care and Pain : 2012.
Page 29
Institutional Guideline after Brain DeathInstitutional Guideline after Brain Death
Sequels Cause Management
1. Hypotension - Neurogenic shock - IV fluid resuscitation
- Hypovolemia - Inotropic support• Diuretics Dopamine 10 mcq/kg/min• Fluid restriction Dobutamine <15 mcq/kg/min• Diabetes Incipidus DI Epinephrine <0.1 mcq/kg/min
• • • • Diabetes Incipidus DI Epinephrine <0.1 mcq/kg/minNE and dopamine 2-4 mcq/kg/min
- Myocardial contussion- E’lyte imbalance- Hormonal imbalance- Catecholamine-induced
cardiomyopathy
• •
Page 30
Sequela Cause Management
2. Arrhythmia -- CNS injury - Possible atropine resistant
: Bradycardia - Hypothermia - Chronotropic drugs
- E’lyte imbalance - Temporary venous pacing
- Acid-base abnormal
Institutional Guideline after Brain DeathInstitutional Guideline after Brain Death
- Acid-base abnormal
- MI
3. Hypoxemia - Central or pulmonary - PaOPaO22 100100--150150 mmHgmmHg
PaCOPaCO22 3535--45 45 mmHgmmHg
pH pH 77..3535--77..4545 mmHgmmHg
PEEP PEEP < < 77..55 cmHcmH22OO
FiOFiO2 2 < < 00..4 4 (heart(heart--lungs)lungs)
Page 31
SequelSequelss CauseCause ManagementManagement
4. DI - Pituitary or - Volume replacementhypothalamic - Vasopressin (0.1u/min)dysfunction DDAVP (0.3ug/kgIV.)
- Keep urine 1.5-3 mL/kg/hr
Institutional Guideline after Brain DeathInstitutional Guideline after Brain Death
- Keep urine 1.5-3 mL/kg/hr- Correct E’lytes- Inotropic support
5. Hypothermia -Loss of hypothalamic - Early aggressive warming Temp. regulation - Maintain T > 35oC
6. Anemia - Hemorrhage - Blood transfusion :- Hemodilution Keep Hct > 30%
Page 32
Kidney Transplantation Kidney Transplantation ::
Indication : ESRD
Donor : Living donor
Deceased donorDeceased donor
Technique : Kidney procurement
Kidney implantation
Immunosuppression : Cyclosporine
: Tacrolimus
: Mycophenolate Mofetil
: Steroids
Page 33
ESRD–patient : high risk for Anesthesia / Surgery
Complication in peri-operative period
Cardiovascular diseasesCardiovascular diseases
Atherosclerosis
Hypertension: poorly controlled Hypertension: poorly controlled
Diabetes mellitus
Coronary artery disease : MI, CABG, PCI with stent
Congestive heart failure
Antiplatelet / Anticoagulants
Page 34
Safety and Mortality Factors :
Effective and adequate hemodialysis : pre/post transplantation
Surgical technique : Experienced surgical team
Modern, new anesthetic agents Modern, new anesthetic agents
New immunosuppression drugs
Monitorings * *
Page 35
Coronary artery disease cause of death
Stroke
Myocardial infarction
Ischemic limbs
Waiting list : CVS evaluationWaiting list : CVS evaluation
: Genetics
: Smoking
: History of HT, dyslipidemia
: Hyperparathyroid disease
Page 36
CVS evaluation :
Physical examination
Electorcardiogram
Chest X-ray
Exercise stress test Exercise stress test
Echocardiogram
Thallium scan
Coronary angiography
CABG, angioplasty
Page 37
Hemodialysis
: severity of HT from fluid overloaded
: Fluid status evaluation (over ; under ?)
: Volume loss from dialysis (BW)
: 24 hr. before surgery
: 4 hr duration of HD
body fluid volume, plasma volume
K, HCO3
Hct, platelet function
Page 38
Acid-base status, electrolyte imbalance :
Metabolic acidosis
Na , Cl , K , CO2
NaHCONaHCO33 if • HCO3 < 15 mEq/L
• pH < 7.2
Respiratory acidosis
Clinical of • dyspnea
• conscious change
• pH < 7.2
Page 39
Metabolic acidosis protein binding to drugs
Muscle relaxants
Local anesthetics Local anesthetics
Opioids
Inert agent after binding with proteins
Page 40
Respiratory system : Fluid overloaded
Pulmonary edema
Pleural effusion
Pneumonia Pneumonia
Atelectasis
hypoxemia, hypoxemia, hypocapniahypocapnia
Page 41
CXR : uremic lung
(perihilar pulmonary venous congestion)
Previous lung disease
Smoker PFT, ABG, SpO2
Abnormal CXR
lung infection after kidney transplantation
from immunosuppressive drugs
Aseptic technique !! Aseptic technique !!
Page 42
Hb level ~ 6-8 gm/dL
Hct ~ 20-25%
Compensate with : CO, 2, 3 DPG
Anemia : Occurs when creatinine > 3 mg/dL
Compensate with : CO, 2, 3 DPG
: hyperdynamic circulation
If Hb <6 gm/dL : Red blood cell transfusion
: synthetic erythropoietin
Now : keep Hb 10 – 12 gm/dL
Hct 32 – 34%
Page 43
Coagulation :
Abnormal bleeding
Coagulopathy
Occurs when Cr > 6 mg/dL
Abnormal platelet function Abnormal platelet function
platelet factor III
platelet counts
Heparin during HD
Uremic toxin
Page 44
Central nervous system :
Fatique
Memory loss
Myoclonus
Seizure
Coma
Death
adequate hemodialysisadequate hemodialysis
Page 45
Chronic HD
DDSDDS early H/D
rapidly change in ECF, E’lytes
•
• Dialysis dysequilibrium syndrome (DDS)
• Dialysis dementia (DD)
and cerebral edema
DDDD very severe form
chronic H/D
abnormal speech, dementia
seizure (death within death within 6 6 month)month)
Page 46
CNS evaluation :
Neuropathy : peripheral ?
If + HD ( cause : demyelination)
: autonomic ?
Valsava’s maneuver
baroreceptor reflex
Postural hypotension
Page 47
Endocrine system :
DM
growth retardation
reproductive system
Hyperparathyroidism
Uremic osteodystrophy
DMDM :: keep BS ~ 100-200 mg/dL
Page 48
GI system :
Nausea vomiting
Hiccup
Anorexia
GI bleeding GI bleeding
Diarrhoea / constipation
DELAYED gastric emptying timeDELAYED gastric emptying time
Ascites, albumin
Hepatitis B,C
**
Page 49
Immune system :
Decreasing immune response
Increasing sepsis
Aseptic technique Aseptic technique !!
Page 50
Problems resulting from Hemodialysis :
Residual heparinization … 10 hr.
Fluid shift : depletion / overloaded
Blood transmitted disease : Hepatitis
: HIV: HIV
: CMV
Bleeding/thrombosis of vascular access
Inadequate H/D
Page 51
Other pre-anesthetic evalulation :
Need - Well prepared and well evaluated patients
Look for : Congestive heart failure
: Pericardial, pleural effusions
: Myocardial ischemia : Myocardial ischemia
: DM autonomic neuropathy?
Consultation, referring systems
Hemodialysis within 24 hr. (if possible in DD)
BW : pre, post H/D, E’lyte , Hb/Hct, Platelet
Page 52
Vascular access precaution :
NotNot measuring NIBP at the vascular access site
NotNot starting IV line
Prevention of thrombosis
(Avoid hypotensive episode)
Page 53
Non-anesthetic drugs preparations :
Preparing : Methylprednisolone 1 gram
: Lasix 250 mg.
: 20% mannitol 250 mL: 20% mannitol 250 mL
: Antibiotics
: cefuroxime 1500 mg (zinacef®)
Page 54
Muscle relaxant for KT :
Cisatracurium
Atracurium
Mivacurium Mivacurium
Rocuronium
Page 55
Inhalation Anesthetics :
O2 : N2O / O2 : Air
Isoflurane
Sevoflurane Sevoflurane
Desflurane
Page 56
Nitrous oxide :
Routinely used with O2 : N2O = 50:50 / 60:40
Avoid using N2O … ileus
… surgical space
in pediatric Tx
… prolonged surgical time
… N/V
Page 57
Fluid management :
Isotonic saline --> adequate fluid volume
BV < 70 mL/kg --> delayed urine production
CVP guide (PA catheter)
NSS/BSS + colloid if large volume needed
Maximized hydration > Maximized hydration > 11,,500 500 mL mL ------ ATNATN
Pulmonary congestion ! in CHF patient
Page 58
Anesthesia for Kidney Transplantation :Anesthesia for Kidney Transplantation :
1. Preanesthetic evaluation and preparation :
Living related-recipient :
• Routine preparation : well prepared
• Elective case• Elective case
Deceased donor – recipient :
• Emergency : full stomach
: coexisting disease
: uncorrected ; uncontrolled underlying disease
Page 59
old age donor / recipient
Maximized / optimized condition
H/D … frequency / wk
… last H/D < 24 hr.
… B.W. pre-post H/D
Fluid overload / K / acidosis / HT
Preop. check E’lyte ; BUN ; Cr. ; CBC ; Ca ; Mg
Page 60
DM : delayed GET
: control DM : BS ~ 100 - 200 mg/dL
E’lyte : K < 5.5 mEq/L
LFT : albumin ; liver enzymes
Coagulogram, INR, Platelet function Coagulogram, INR, Platelet function
Severity of anemia
: Hct ~ 22 - 25%
: PRC 2 – 4 units FFP 2 - 4 units
: Avoid whole blood Transfusion
Do Not Transfuse Blood or Blood product before TransplantationDo Not Transfuse Blood or Blood product before Transplantation
Page 61
Premedication
: Benzodiazepine orally : MDZ / Lorazepam
: Avoid narcotics : morphine ; meperidine
: Anticholinergic : atropine IV
: Antihypertensive agent : precaution !
: Aspiration prophylaxis
Supplement steroid
Labs ; blood ; blood components
Oxygen supplementation
Page 62
2. Monitoring during anesthesia :
IHD, HT (severe), pulmonary disease :
ECG, NIBP
Invasive BP pediatric KT, comorbid diseases
CVP : IJV, subclavian : 10-12 cmH2O
: CHF, pulmonary edema, CAD, inadequate H/D
End tidal CO2
Page 63
Pulse oximeter
Nerve stimulator
Temperature (esophageal > nasopharynx)
Labs : Hb, Hct, E’lytes, BS, Cr. Labs : Hb, Hct, E’lytes, BS, Cr.
Bacterial filters
Aseptic techniques !
Page 64
Choice of anesthesia
Site : iliac fossa : Rt/Lt, extraperitoneal
Small children : retroperitoneal
Supine position Supine position
GA / RA (CEB)
Page 65
A. General anesthesia :
Anesthetic of choice : modern agents / machine
IV. Line ; large ; 2 lines
Induction : ? full stomach “rapid-sequence induction”
• Sleep dose • thiopental 3 mg/kg• Sleep dose
• Fentanyl 1 - 2 g/kg
• MDZ 2 - 3 mg
• thiopental 3 mg/kg
• propofol 0.5 – 1 mg/kg
Page 66
Intubation
Preoperative K – level = ?
NPO time : type / amount / time of meal
Succinylcholine K <5.0 ; 1-2 mg/kg ; full stomach
Nondepol. MR K >5.0 ; good NPO Nondepol. MR K >5.0 ; good NPO
atracurium ; cisatracurium
rocuronium
Awake intubation
Page 67
ET-tube : Sterile, PVC, low pressure cuff
: Oral approach
N2O : O2 = 1:1 (50% O2) / air : O2
Sevoflurane (FGF ~ 2 L/min) Sevoflurane (FGF ~ 2 L/min)
Desflurane (low flow < 1.5 L/min)
NG tube (orogastric tube)
Antibiotics: Cefuroxime 1.5 g
Page 68
Maintenance of general anesthesia
Maintain BP~ control level ( > 110-120 mmHg) **
Control ventilation : ventilator (ETCO2) + PEEP
Atracurium, cisatracurium : infusion route
: IV titrate route
Page 69
Declamping
: Bleeding acute volume loss
: Bradycardia : DM
: on -blocker
: Atropine, isoproterenol: Atropine, isoproterenol
: Cause : hyper K+ , acidosis,Temp
: Transient
Hyper K+ during KT
Page 70
Other drugs : during maintenance
• Dopamine : renal dose 1 - 2 g/kg/min
• 20% mannitol 1 gm/kg infusion (250 mL)
• Methyl prednisolone 1 gm. IV
• Lasix 250 mg. IVbefore declamping
• Lasix 250 mg. IV
Ischemic time : WIT, CIT, r-WIT : living - related
: CIT, r-WIT : deceased
LPRC, FFP, Platelets Transfusion
Page 71
Emergence : reversal agents
: extubation
: O2 supplement P.O
On mechanical ventilator if :On mechanical ventilator if :
• Old age, weak, conscious +
• Multiple coexisting diseases
• Not well prepared H/D
• Emergency case with unstable hemodynamics
• Fluid overload, pulmonary congestion
• Acute tubular necrosis (ATN) with massive fluid transfusion
Emergency H/D
Page 72
Maximize hydration : > Maximize hydration : > 11,,500 500 mL before mL before declampingdeclamping
Early graft function :
• Well prepared kidney graft
• Adequate blood volume
• Normal hemodynamics
Maximum hydration : graft failure 30% 5%
: incidence of ATN P.O
If blood volume < 70 mL/kg … delayed urination > 5 min.
Page 73
GoalGoal : CVP 10-12 / PCWP 12-15 mmHg
: system BP 140 – 160 mmHg
If If
• Infuse crystalloid > 40-90 mL/kg colloid
• Severe anemia ; blood loss > 200 mL.
: LPRC Tx after declamping
: keep Hct 25 - 28% 30% – 32% (now)
(especially in CAD patient)
*
Page 74
Hyperkalemia : causes :
Preoperative hyperkalemia ( > 5.5 mEq/L)
Succinylcholine intubation
Perfusate with high K+ (125 mEq/L)
Acidosis
Old age – blood donation
Monitors : Electrolytes ; Ca ; Mg.
: ECG : peak-T, deep-S, QT, PR prolonged
: flat-P wave
Page 75
CriticalCritical if : K > if : K > 66..5 5 mEqmEq/L/L
No urine from new kidney ( delayed graft functioning)
Serious arrhythmia Serious arrhythmia cardiac arrestcardiac arrest
Treatment : NaHCO3
: hyperventilation
: 10% CaCl2 10 mL IV
: glucose-insulin IV: glucose-insulin IV
: lasix 250 mg. IV : 2nd dose
Postoperative hemodialysis
Retained ET + mechanical ventilator
Keep mild respiratory alkalosis
pulmonary congestion / edema
Page 76
ATN or AKI ATN or AKI (deceased donor - 30% ): potential causes
: Not well hemodialysis before KT
: Fluid balance : volume depletion
: Vital Signs : unstable
: Cold Ischemic Time ( CIT ) > 24 hr.
: Conditions of deceased donor
: old age : old age
: nephrotoxic / vasopressor dose
: terminal Serum Cr. level
: not well perfused graft
: Surgical causes : injury of graft during procurement
: difficult surgical technique
Page 77
Steps of Kidney TransplantationSteps of Kidney Transplantation
• Deceased donor kidney donation
• Deceased donor management
• Deceased donor kidney procurement
•• Organ transportation
• Kidney implantation
• Kidney transplantation
Page 78
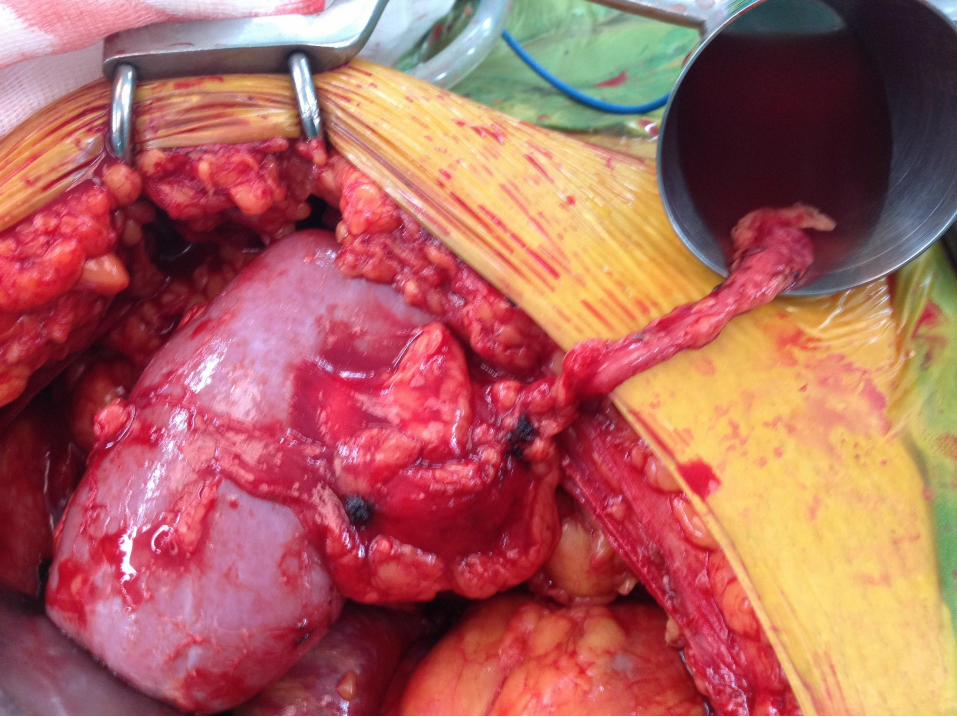
Kidney from Deceased donorKidney from Deceased donor
Page 79
Kidney from Deceased donorKidney from Deceased donor
Page 80
Kidney from Deceased donorKidney from Deceased donor
Page 81
การผา่ตดัเปลี�ยนไตKidney Transplantation
Page 84
28/07/12
Organ Transplant is the Miracle Organ Transplant is the Miracle
Page 85
PostPost--anesthetic care :anesthetic care :
1. Emergence :
- Turn off anesthetic agent
- Reversal of muscle relaxant - Reversal of muscle relaxant
- Extubate PACU / ICU (isolated ward)
- On O2 nebulizer ~50%
Page 86
2. Blood pressure :
- Keep ~ control level >120/70 – 150/160 mmHg
- Avoid hypertension :
MI, CHF
Pulmonary edema
Intracranial hemorrhage
Bleeding at anastomotic siteBleeding at anastomotic site
Anti hypertensive agent treatment : evaluate
LV function
Filling pressure
HR
- Hypotension : if good CVP dopamine infusion
Page 87
3. Fluid management :
Good graft functioning
Keep CVP ~ intraoperative level
Urine output > 500-1,000 mL/hr … up to 40 L/day
IV fluid : BSS + 5% D/W or 0.45% NSS
: 0.9% NSS + 5% D/N/2: 0.9% NSS + 5% D/N/2
Last hour urine + 50-100 mL/hr
300 ml + 100-200 mL/hr
Check E’lytes : K, Na, Ca, mg
ATN / AKI ATN / AKI Hemodialysis
keep maintenance volume
Page 88
4. Oliguria / anuria :
11. . PrerenalPrerenal : inadequate renal BF
: LV dysfunction : compliance
BP : drugs
Fluid therapy
Px arrhythmiaPx arrhythmia
Correct abn. E’lytes
If correct sys. BP < 120 mmHg ; CI < 2.5 L/min/m2
start inotropic support
Page 89
22. . InfrarenalInfrarenal ::
Bleeding : CVP ; anemia ; BP … acute
Anastomosis – stenosis/leakage … delayed
Anuria thrombosis of artery / vein graft
U/S, renal scan
Emergency reexploration surgical correction
Graft loss ?
Renal biopsy
Page 90
33. . PostrenalPostrenal ::
Kinking / blood clot in urinary system
Irrigation urinary catheter
fluid, lasix 250 mg. infusion
Investigate --> renogram, renal scan, U/S
Page 91
4. Postoperative pain control :
Opioid : Oral ; IV ; PCA
: MO 3-4 mg IV prn.
NSAID : renal clearanceNSAID : renal clearance
: GFR
: interstitial nephritis
avoidavoid decrease in renal function
Page 92
5. Postanesthetic complication :
Nausea – vomitting
Respiratory function
Cardiovascular system
complication complication ------ 3333%%
HTHT
arrhythmia … cardiac arrestarrhythmia … cardiac arrest
hypo/hypertensionhypo/hypertension
Page 93
Pulmonary : Atelectasis
: Emergency management :- infection
: Pulmonary edema
DM : 3-16% P.O 4% need insulin treatment DM : 3-16% P.O 4% need insulin treatment
: Onset 3 mo. after KT, high dose steroid
: Risk factor : glucose intolerance
: HLA type B28
Page 94
Mortality rate after kidney transplantation
0.03 - 0.06 %
Risk : Age > 60 yearsRisk : Age > 60 years
: CAD
: DM
Page 96
Thank you for your attention Thank you for your attention