83 http://www.futureofchildren.org Community-Based Injury Prevention Interventions Terry P . Klassen, J. Morag MacKay, David Moher, Annie Walker,Alison L. Jones Abstract Community-based interventions offer a promising solution for reducing child and adolescent unintentional injuries. By focusing on altering behavior, promoting envi- ronmental change within the community, or passing and enforcing legislation, these interventions seek to change social norms about acceptable safety behaviors. This arti- cle systematically reviews 32 studies that evaluated the impact of community-based injury prevention efforts on childhood injuries, safety behaviors, and the adoption of safety devices. Interventions targeted schools, municipalities, and cities. Most relied on an educational approach, sometimes in combination with legislation or subsidies, to reduce the cost of safety devices such as bicycle helmets. Results indicate that community-based approaches are effective at increasing some safety practices, such as bicycle helmet use and car seat use among children. The evi- dence is less compelling that such interventions increase child pedestrian safety, increase adolescent vehicle safety by reducing drinking and driving behaviors, or reduce rates of several categories of childhood injuries. Strong evidence supporting the effectiveness of community-based interventions is lacking, in part because few studies used randomized controlled designs or examined injury rates among children and youths as outcome measures. Nonetheless, this review identifies common elements of successful community-based approaches that should be replicated in future studies. First, the use of multiple strategies grounded in a theory of behavior change is critical. Second, to maximize success, interventions should be integrated into the community and approaches should be tailored to meet unique community needs. Third, com- munity stakeholders should be included in the development of community-based strategies. This community involvement and ownership of the intervention increases the likelihood of modeling and peer pressure, leading to widespread adoption of a safety behavior. Finally, when possible, a randomized controlled design should be used to maximize the trustworthiness of reported findings and aid decisions about where to invest resources in community-based approaches to injury prevention. C ommunity-based interventions offer one approach to reducing injuries by changing community norms and behaviors and by alter- ing the physical environment of communities to reduce the risk of injury. The community-based approach may have particular relevance for The Future of Children UNINTENTIONAL INJURIES IN CHILDHOOD Vol. 10 • No. 1 – Spring/Summer 2000 Terry P. Klassen, M.D., M.Sc., F.R.C.P.(C), is professor and chair, Department of Pedi- atrics, University of Alberta, Edmonton, in Alberta, Canada. J. Morag MacKay, M.Sc., is director of Plan-It Safe, Child and Youth Injury Prevention Centre at the Children’s Hospital of Eastern Ontario Research Institute in Canada. David Moher, M.Sc., is director of The Thomas C. Chalmers Centre for Systematic Reviews, Children’s Hospital of Eastern Ontario Research Institute, and assistant professor of pediatrics, and epidemiology and community medicine, at the University of Ottawa in Canada. Annie Walker, M.A., is a statistical consultant at Child and Youth Clinical Trials Network, Children’s Hospital of Eastern Ontario Research Institute, in Canada. Alison L. Jones is a research associate at The Thomas C. Chalmers Centre for Systematic Reviews, Children’s Hospital of Eastern Ontario Research Institute, in Canada.
Transcript
83
http://www.futureofchildren.org
Community-BasedInjury Prevention InterventionsTerry P. Klassen, J. Morag MacKay, David Moher,Annie Walker,Alison L. Jones
AbstractCommunity-based interventions offer a promising solution for reducing child andadolescent unintentional injuries. By focusing on altering behavior, promoting envi-ronmental change within the community, or passing and enforcing legislation, theseinterventions seek to change social norms about acceptable safety behaviors. This arti-cle systematically reviews 32 studies that evaluated the impact of community-basedinjury prevention efforts on childhood injuries, safety behaviors, and the adoption ofsafety devices. Interventions targeted schools, municipalities, and cities. Most relied onan educational approach, sometimes in combination with legislation or subsidies, toreduce the cost of safety devices such as bicycle helmets.
Results indicate that community-based approaches are effective at increasing somesafety practices, such as bicycle helmet use and car seat use among children. The evi-dence is less compelling that such interventions increase child pedestrian safety,increase adolescent vehicle safety by reducing drinking and driving behaviors, orreduce rates of several categories of childhood injuries. Strong evidence supporting theeffectiveness of community-based interventions is lacking, in part because few studiesused randomized controlled designs or examined injury rates among children andyouths as outcome measures. Nonetheless, this review identifies common elements ofsuccessful community-based approaches that should be replicated in future studies.
First, the use of multiple strategies grounded in a theory of behavior change is critical.Second, to maximize success, interventions should be integrated into the communityand approaches should be tailored to meet unique community needs. Third, com-munity stakeholders should be included in the development of community-basedstrategies. This community involvement and ownership of the intervention increasesthe likelihood of modeling and peer pressure, leading to widespread adoption of asafety behavior. Finally, when possible, a randomized controlled design should be usedto maximize the trustworthiness of reported findings and aid decisions about where toinvest resources in community-based approaches to injury prevention.
Community-based interventions offer one approach to reducinginjuries by changing community norms and behaviors and by alter-ing the physical environment of communities to reduce the risk of
injury. The community-based approach may have particular relevance for
The Future of Children UNINTENTIONAL INJURIES IN CHILDHOOD Vol. 10 • No. 1 – Spring/Summer 2000
Terry P. Klassen, M.D.,M.Sc., F.R.C.P.(C), isprofessor and chair,Department of Pedi-atrics, University ofAlberta, Edmonton,in Alberta, Canada.
J. Morag MacKay,M.Sc., is director of Plan-It Safe, Child andYouth Injury PreventionCentre at the Children’sHospital of EasternOntar io ResearchInstitute in Canada.
David Moher, M.Sc., isdirector of The ThomasC. Chalmers Centre forSystematic Reviews,Children’s Hospital ofEastern Ontario ResearchInstitute, and assistantprofessor of pediatrics,and epidemiology andcommunity medicine,at the University ofOttawa in Canada.
Annie Walker, M.A., isa statistical consultantat Child and YouthClinical Trials Network,Children’s Hospital ofEastern Ontario ResearchInstitute, in Canada.
Alison L. Jones is aresearch associate at TheThomas C. ChalmersCentre for SystematicReviews, Children’sHospital of EasternOntar io ResearchInstitute, in Canada.
84 THE FUTURE OF CHILDREN – SPRING/SUMMER 2000
http://www.futureofchildren.org
children, as interventions often target the safety awareness, attitudes, andbehaviors of the child and the parents. Gradually, as families engage insafety behaviors or use safety devices more frequently, new norms reflectingthe goals of the intervention emerge within a community. The process issimilar for youths; however, peer pressure also plays a considerable role inpromoting or inhibiting the adoption of safety behaviors within this popu-lation. Acceptance of new behaviors by the peer group may be crucial to aprogram’s success.
Although community-based interventions hold promise, there is a paucityof evidence examining the impact of these approaches on safety behaviors orinjury rates among children. This article defines community-based interven-tions and systematically reviews relevant literature to ascertain the effective-ness of such approaches in reducing childhood unintentional injuries (seethe article by DiGuiseppi and Roberts in this journal issue for a description ofa systematic review). The key characteristics of successful community-basedprograms are identified by comparing elements of programs that improvedsafety behaviors or reduced injury rates with elements of programs that failedto impact these outcomes.
Defining Community-BasedInterventionsIn this article, community-based interven-tions are those that target a group of individ-uals or a geographic community but are notaimed at a single individual. This definitionincludes cities, municipalities, and schools. Itexcludes interventions delivered in clinicalsettings and interventions targeting areas aslarge as states or countries, since injury pre-vention strategies focused at these levels arecovered elsewhere in this journal issue (seethe articles by DiGuiseppi and Roberts, andby Schieber, Gilchrist, and Sleet.)
Community-based interventions employa broad array of strategies that includeeducation/behavior change, engineering/technology, and legislation/enforcement.Educational strategies increase awareness ofinjury risk or the importance of risk-reducingbehaviors, and they may include mediabroadcasts, public service announcements,classroom instruction, or written material.Behavioral strategies have the same goal andmay involve incentives, negative feedback,and modeling. Alternatively, the goal ofengineering/technology interventions is toalter the physical environment (such as plac-ing speed bumps on neighborhood streetsor installing smoke detectors in homes) ormodify the design of safety devices (suchas bicycle helmets or child passenger
restraints). Finally, legislation/enforcementinterventions involve the passage andenforcement of new laws or the increasedenforcement of existing laws.
Evaluating Community-Based Injury PreventionStrategiesStudies were included in this review if theymet the following criteria: (1) the studyincluded a control group that did notreceive the intervention, (2) the target pop-ulation was between 0 and 19 years of age,(3) the study examined the effectiveness of acommunity-based intervention, and (4) thestudy reported injury rates or change in aninjury-reducing behavior. (See the Appen-dix at the end of this article for details aboutthe search strategy, methods, and analysisused in this systematic review.)
Although randomized controlled trials(RCTs) are the study design most likely toprovide unbiased estimates of the impact ofinterventions (see the article by DiGuiseppiand Roberts in this journal issue), thereview also included nonrandomized com-parison group studies for two reasons. First,a previous review of community-focusedinterventions found that most such studiesdid not use a randomized design to evalu-ate program impact.1 Second, the logisticsof randomization can be complicated in
85Community-Based Injury Prevention Interventions
http://www.futureofchildren.org
community-based injury prevention pro-grams. Certain interventions such as legisla-tion may defy randomization at thecommunity level and require a comparisonat a state or country level.
Thirty-two trials that evaluated the effect ofa community-based injury control interven-tion on child injury rates, safety behaviors,or the use of safety devices were identifiedin this review.2–33 This article focuses on the28 studies targeting bicycle helmet use,automobile restraint use, pedestrian safety,general injury prevention, and adolescentalcohol use and vehicle safety (see Tables 1to 5). The four other trials were aimed atreducing the frequency of play with guns,30
reducing football injuries,31 improvingroad safety behaviors of bicyclists,32 andimproving burn prevention practices.33
Because only one study addressed each ofthese outcomes and none of the interven-tions had a positive impact, these studiesare not discussed further in this review. Ofthe 28 remaining studies, 6 wereRCTs,2,3,17,21,22,28 and 22 were nonrandom-ized controlled trials.4–16,18–20,23–27,29 Most ofthe studies examined safety behaviors; onlyfour examined actual injuries.12,23–25
The Effectiveness of Community-BasedApproachesOverall, the impact of community-basedinterventions on child and adolescentsafety practices and injuries is mixed. Rela-tively strong evidence suggests that suchinterventions can increase bicycle helmetand motor vehicle restraint use among chil-dren. However, the success of these inter-ventions at improving child pedestriansafety, influencing adolescent alcohol useand vehicle safety, and reducing rates of abroad array of childhood injuries withincommunities is less evident.
Elements of Successful Community-Based ApproachesSuccessful community-based programsshare a number of common elements. Theuse of multiple strategies consistent with anunderlying theory of behavior change is crit-ical to success (see Box 1).34–36 Interventionsare more effective when they are integratedinto the community and when approachesare tailored to address unique community
characteristics such as ethnicity or socio-economic status. Effective programs activelyinvolve community stakeholders in theprogram-development process or holdpublic consultations to determine a pro-gram’s process and goals. As a program isspread across a community, its impact maybe increased by peer pressure and modelingby other community members.
In addition to successful programmaticelements, the design of community-basedtrials and the evaluation methodology usedalso influence program effectiveness. Themost informative and reliable results comefrom RCTs (see the article by DiGuiseppi
and Roberts in this journal issue). Whenrandomization of groups to interventionand control conditions is not possible, com-parison communities should be carefullyselected that are similar to the interventioncommunity in characteristics—such associoeconomic status, age, race/ethnicity,and baseline use of safety behaviors—thatmay be associated with the effectiveness ofthe program.
The outcomes that were measured alsoinfluence the interpretation of a program’seffectiveness; therefore, injury rates shouldbe used whenever possible. However, mea-suring safety behaviors may be a suitablealternative when evidence shows that adop-tion of the behavior (that is, bicycle helmetuse) is strongly associated with a decrease ininjury rates (that is, head injury). Less rigor-ous outcomes, such as changes in knowledgeor attitudes, should be avoided since the cor-relation between knowledge, attitudes, andbehaviors can be weak.37 Finally, regardlessof the outcomes selected, assessment of pro-gram effectiveness requires careful and thor-ough statistical analyses to control forspurious effects due to repeated measuresover time or bias.
Interventions are more effective when theyare integrated into the community and whenapproaches are tailored to address uniquecommunity characteristics such as ethnicityor socioeconomic status.
86 THE FUTURE OF CHILDREN – SPRING/SUMMER 2000
http://www.futureofchildren.org
Summarized below is the impact ofcommunity-based interventions on childand adolescent safety practices and injuryoutcomes based on this systematic review(see Tables 1 to 5). Results from specificstudies are discussed if they substantially con-tribute to the knowledge of the effectivenessof community-based interventions in gen-eral or if they illustrate critical aspects of aparticular program that influenced the pro-gram’s success or failure.
Programs Targeting BicycleHelmet UseBicycle injuries are a leading cause of injurydeath and disability among children.37 Bicycle-related head injuries result in approximatelyone-third of emergency department visits,
two-thirds of hospitalizations, and three-fourths of deaths related to bicycling (seethe article by Grossman in this journalissue).38 Several studies have shown thathelmet use decreases the risk of head injuryby 70% to 88%.38–43
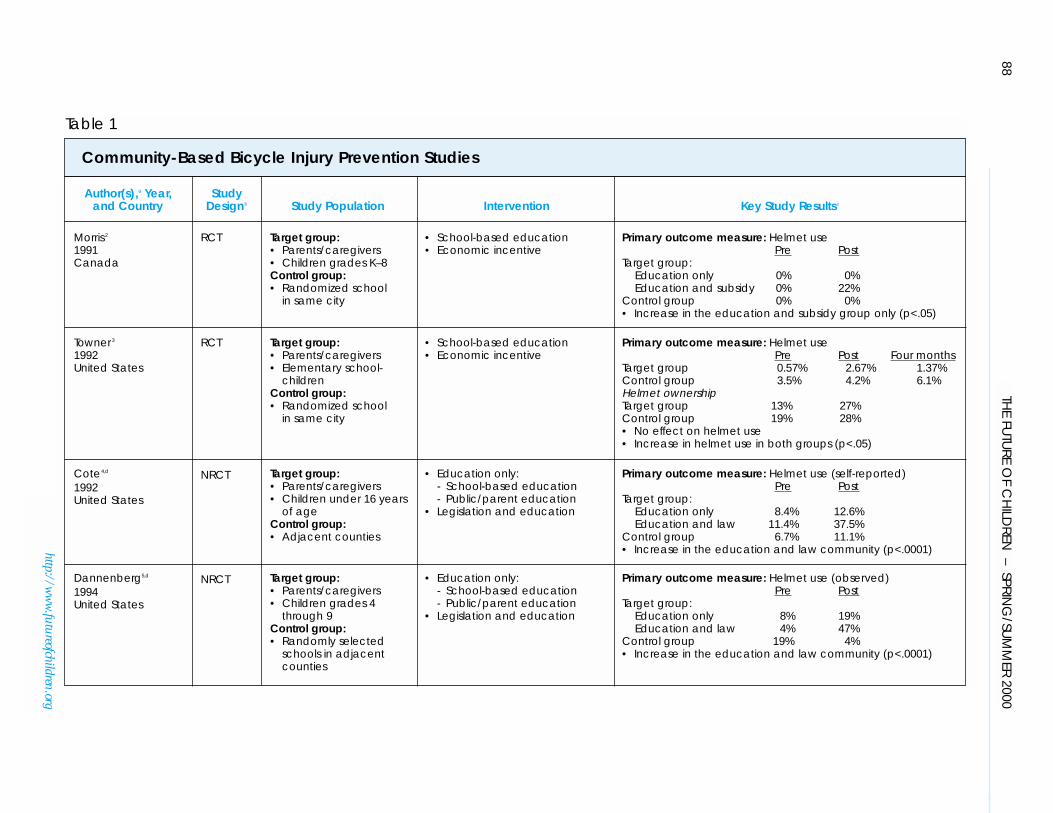
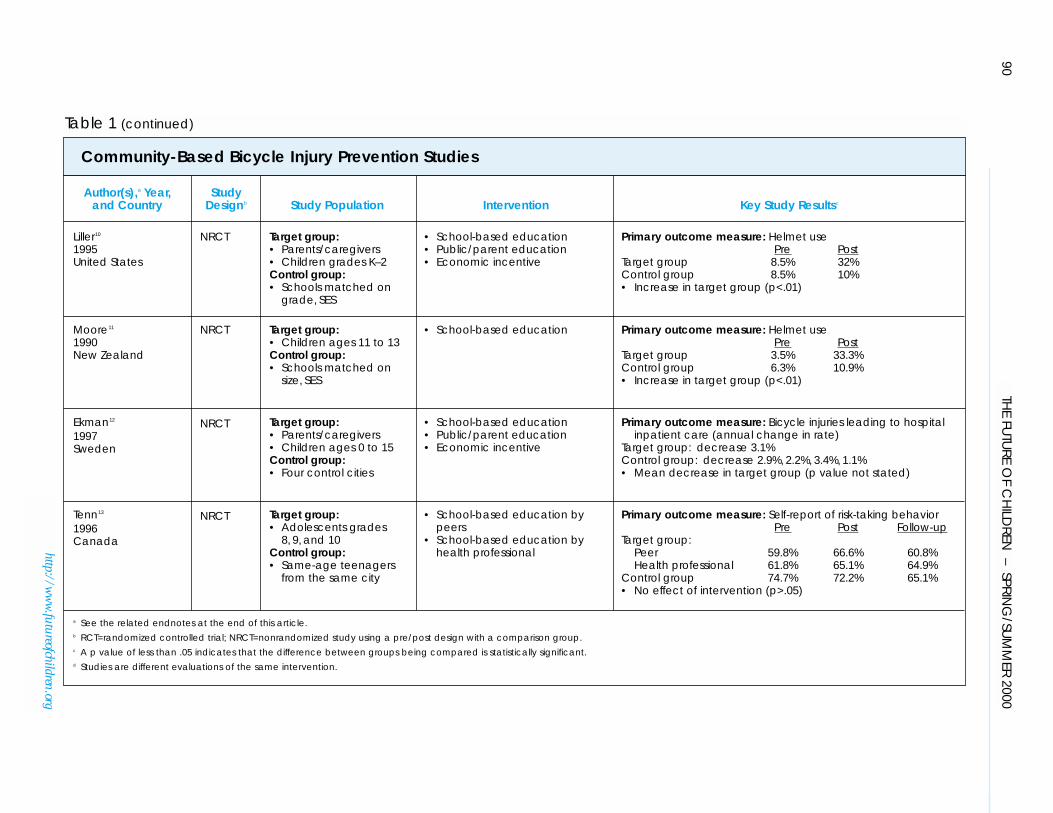
Eleven community-based programsaimed at increasing the use of bicycle hel-mets by children and adolescents were iden-tified in this review (see Table 1).2–13 Eightstudies, representing seven different pro-grams, reported a significant increase inhelmet use,2,4–7,9–11 and one study reported asignificant decrease in serious bicycle-relatedinjuries12 associated with the intervention inat least some subgroups examined. Twostudies found no difference in helmet use
Selected Health Behavior Frameworks Used in Community-Based Interventionsa
■ Health Belief Model:34 States that an individual’s readiness to alter behaviordepends on four conditions: (1) perceived threat or susceptibility to the condition;(2) perceived severity of the condition; (3) perceived benefits of the health actionin reducing susceptibility and/or the severity of the condition, weighed against;(4) perceived barriers or personal costs of the health action. According to theHealth Belief Model, community-based interventions should be designed to con-vince the target population of the threat of injury and their risk while simultane-ously instilling confidence that a particular action is effective in reducing their risk.
■ Social Learning Theory:35 Recognizes that behavior change occurs within a socialcontext and is influenced by both active involvement in the learning process andidentified consequences of the behavior change. Strategies such as modelingbehavior (that is, having someone physically demonstrate the desired behavior)and promoting external reinforcement (for example, offering money) or internalreinforcement (for example, instilling a feeling of pleasure or pride) are key tosuccessful behavior change. The ways in which social groups alter behavior supportsocial learning theory; members change their behavior as a result of modeling orreinforcement by others, or by their own active involvement in the group.
■ PRECEDE Model:36 Stands for Predisposing, Reinforcing, and Enabling Con-structs in Educational Diagnosis and Evaluation. The three constructs worktogether toward behavioral change. Predisposing factors include attitudes, beliefs,and values of the target population. Reinforcing factors include support for behav-ior change, such as support from family, peers, teachers, or health care providers.Continuance of a behavior relies on reinforcement. Enabling factors consist of theindividual skills necessary to adopt the proposed change, as well as the availabilityand accessibility of external resources to facilitate change. The educational diag-nosis is the examination of predisposing, enabling, and reinforcing factors in thespecific context of the proposed behavioral change. Evaluation is the quantifica-tion of the program’s impact.
a See related endnotes at the end of this article.
Box 1
following the intervention,3,8 and one studyreported no difference in self-reported risk-taking behaviors.13 A common element ofsuccessful programs was the use of multiplestrategies targeted at different audiences toaddress three pivotal barriers to helmet use:lack of awareness about the risks of bicyclingand the effectiveness of helmets, the cost ofhelmets, and the perception of negativepeer pressure regarding helmet use. Use ofmultiple strategies allows a program totackle more than one barrier to behaviorchange and to target more than one sub-population within the community. Theresult is a broad reception of the main cam-paign message, which is reinforced becauseit is sent and received in several ways.
An RCT conducted in Ontario, Canada,illustrates how multiple strategies can beused in a community-based program aimedat increasing bicycle helmet use among chil-dren and how the effects of each strategy canbe examined in combination and sepa-rately.2 Three schools similar in socio-economic status and catchment area wererandomly assigned to one of the followingconditions: no intervention, an educationalprogram aimed at increasing awareness ofthe importance of bicycle helmet use, or theeducational awareness program plus a sub-sidy that allowed helmets to be purchased ata discounted price.
Baseline observations revealed that noneof the children in any of the schools worebicycle helmets. One month after the pro-gram, 22% of the children in the education-plus-subsidy school were observed wearinghelmets, but none of the children in theother groups had adopted this safety prac-tice. These findings indicate that an educa-tional intervention supplemented by asubsidy to decrease financial barriers wassuccessful at increasing helmet use inthis population.
Although educational strategies coupledwith economic incentives are often success-ful at increasing bicycle helmet use, theireffectiveness may vary by the intensity andduration of the intervention. That is, thepresence of multiple strategies is a necessary,but not always sufficient, condition to ensurea successful program. For example, Townerand colleagues developed an elementaryschool–based intervention with multiple
components.3 Discount coupons toward thepurchase of bicycle helmets also were pro-vided. However, although helmet ownershipincreased in the study group following theintervention (13% preintervention versus27% postintervention), ownership increasedsimilarly in the control group (19% prein-tervention versus 28% postintervention).Thus, the increase cannot be attributed tothe intervention. In addition, the programfailed to increase helmet use in the targetedschools, perhaps because it was short induration and intensity.
Legislation is another strategy that hasbeen paired with educational campaigns incommunity-based interventions. In HowardCounty, Maryland, legislation was passedthat requires children under 16 years of age
to wear helmets when riding bicycles oncounty roads and paths. An educationalcampaign also was adopted that includedboth school and community components.The combined effect of legislation and edu-cation in Howard County was comparedwith the effect of education alone in adja-cent Montgomery County in two separateevaluations.4,5 A third community, BaltimoreCounty, served as a control community,where no formal educational or legislativeefforts were in place.
One evaluation found that approximately10 months after the legislation went intoeffect, there was a significant increase inobserved helmet use in the target population(4% preintervention versus 47% postinter-vention).4 Although observed helmet use alsoincreased following the educational interven-tion in Montgomery County (8% preinter-vention versus 19% postintervention), this
87Community-Based Injury Prevention Interventions
http://www.futureofchildren.org
A common element of successful programswas the use of multiple strategies targeted at different audiences to address three pivotal barriers to helmet use: lack of awareness about the risks of bicycling andthe effectiveness of helmets, the cost of helmets, and the perception of negative peerpressure regarding helmet use.
88TH
E FUTU
RE OF C
HILD
REN – SPRIN
G/SU
MM
ER 2000
http://ww
w.futureofchildren.org
Author(s),a Year, Studyand Country Designb Study Population Intervention Key Study Resultsc
Control group: Education only 0% 0%• Randomized school Education and subsidy 0% 22%
in same city Control group 0% 0%• Increase in the education and subsidy group only (p<.05)
Towner3 RCT Target group: • School-based education Primary outcome measure: Helmet use 1992 • Parents/caregivers • Economic incentive Pre Post Four monthsUnited States • Elementary school- Target group 0.57% 2.67% 1.37%
children Control group 3.5% 4.2% 6.1%Control group: Helmet ownership• Randomized school Target group 13% 27%
in same city Control group 19% 28%• No effect on helmet use• Increase in helmet use in both groups (p<.05)
Cote4,d NRCT Target group: • Education only: Primary outcome measure: Helmet use (self-reported) 1992 • Parents/caregivers - School-based education Pre PostUnited States • Children under 16 years - Public/parent education Target group:
of age • Legislation and education Education only 8.4% 12.6%Control group: Education and law 11.4% 37.5%• Adjacent counties Control group 6.7% 11.1%
• Increase in the education and law community (p<.0001)
Dannenberg5,d NRCT Target group: • Education only: Primary outcome measure: Helmet use (observed) 1994 • Parents/caregivers - School-based education Pre PostUnited States • Children grades 4 - Public/parent education Target group:
through 9 • Legislation and education Education only 8% 19%Control group: Education and law 4% 47%• Randomly selected Control group 19% 4%
schools in adjacent • Increase in the education and law community (p<.0001)counties
Table 1
Community-Based Bicycle Injury Prevention Studies
89C
om
mun
ity-Base
d In
jury Preve
ntio
n In
terve
ntio
ns
http://ww
w.futureofchildren.org
Author(s),a Year, Studyand Country Designb Study Population Intervention Key Study Resultsc
DiGuiseppi6 NRCT Target group: • School-based education Primary outcome measure: Helmet use1989 • Parents/caregivers • Public/parent education Pre 12 months 16 monthsUnited States • Children ages 5 to 15 • Economic incentive Target group 5.5% 10.5% 15.7%
Control group: Control group 1.0% — 2.9%• City with same • Increase in target group (p<.001)
characteristics
Parkin7 NRCT Target group: • School-based education Primary outcome measure: Helmet use1993 • Parents/caregivers • Public/parent education Pre PostCanada • Children ages 5 to 14 • Economic incentive Target group:
Control group: High income 4% 36%• Schools matched on Low income 1% 7%
grade, SES Control group:High income 4% 15%Low income 3% 13%
• Increase in high-income group only (p<.001)
Parkin8 NRCT Target group: • School-based education Primary outcome measure: Helmet use1995 • Parents/caregivers • Public/parent education Pre PostCanada • Children ages 5 to 14 • Economic incentive Target group:
Control group: Low income 4% 18%• Schools in same region Control group 3% 19%
• Overall increase across groups (p<.001)• No effect of the intervention (p>.05)
Farley9 NRCT Target group: • School-based education Primary outcome measure: Helmet use (observed)1996 • Parents/caregivers • Public/parent education Pre PostCanada • Children ages 5 to 12 • Economic incentive Target group:
Control group: High income 10.9% 33.7%• Children the same age Low income 3.1% 25.8%
from municipalities in Control group:another region High income 2.8% 11.8%
Low income 4.1% 15.2%• Overall increase in target group (p<.001)• Interaction high income versus low income (p<.01)
Table 1 (continued)
Community-Based Bicycle Injury Prevention Studies
90TH
E FUTU
RE OF C
HILD
REN – SPRIN
G/SU
MM
ER 2000
http://ww
w.futureofchildren.org
Author(s),a Year, Studyand Country Designb Study Population Intervention Key Study Resultsc
Liller10 NRCT Target group: • School-based education Primary outcome measure: Helmet use1995 • Parents/caregivers • Public/parent education Pre PostUnited States • Children grades K–2 • Economic incentive Target group 8.5% 32%
Control group: Control group 8.5% 10%• Schools matched on • Increase in target group (p<.01)
grade, SES
Moore11 NRCT Target group: • School-based education Primary outcome measure: Helmet use1990 • Children ages 11 to 13 Pre PostNew Zealand Control group: Target group 3.5% 33.3%
• Schools matched on Control group 6.3% 10.9%size, SES • Increase in target group (p<.01)
Ekman12 NRCT Target group: • School-based education Primary outcome measure: Bicycle injuries leading to hospital1997 • Parents/caregivers • Public/parent education inpatient care (annual change in rate)Sweden • Children ages 0 to 15 • Economic incentive Target group: decrease 3.1%
Control group: Control group: decrease 2.9%, 2.2%, 3.4%, 1.1%• Four control cities • Mean decrease in target group (p value not stated)
Tenn13 NRCT Target group: • School-based education by Primary outcome measure: Self-report of risk-taking behavior1996 • Adolescents grades peers Pre Post Follow-upCanada 8, 9, and 10 • School-based education by Target group:
Control group: health professional Peer 59.8% 66.6% 60.8%• Same-age teenagers Health professional 61.8% 65.1% 64.9%
from the same city Control group 74.7% 72.2% 65.1%• No effect of intervention (p>.05)
a See the related endnotes at the end of this article.b RCT=randomized controlled trial; NRCT=nonrandomized study using a pre/post design with a comparison group.c A p value of less than .05 indicates that the difference between groups being compared is statistically significant.d Studies are different evaluations of the same intervention.
Table 1 (continued)
Community-Based Bicycle Injury Prevention Studies
increase was not statistically significant. InBaltimore County, use actually decreasedsomewhat during the same time period (19%preintervention versus 4% postintervention).In the second evaluation, fourth-, seventh-,and ninth-grade students from randomlyselected schools in the three counties wereasked about helmet use before and one yearafter the Howard County law want intoeffect.5 Although self-reported helmet useincreased in all three counties, the increasewas greatest in Howard County. One yearfollowing the legislative mandate, school-children in Howard County were 2.3 timesmore likely to report helmet use on the mostrecent ride than children in the other twocounties. Thus, the combined effect of legis-lation and education increased helmet usemore than education alone.
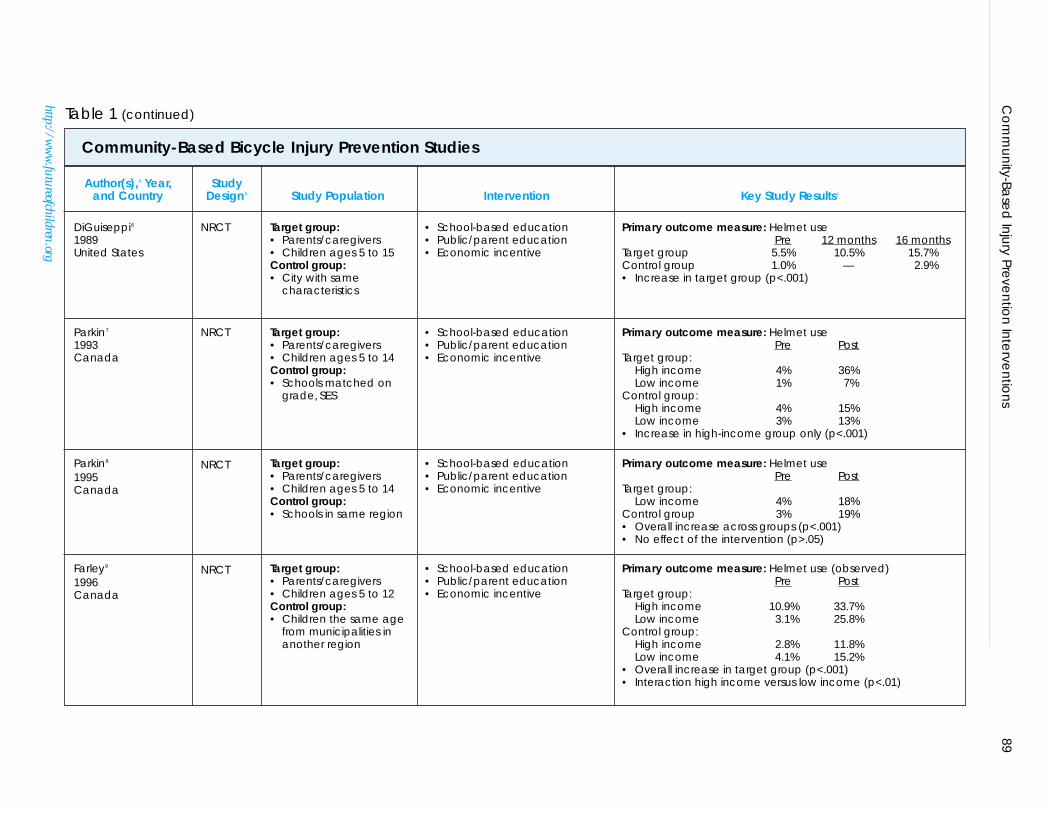
The Seattle Bike Helmet campaign isanother example of a comprehensivecommunity-based trial that used multiplestrategies to increase helmet use.6 This cam-paign had three specific objectives: to increaseparental awareness of the need to wear ahelmet when bicycling, to change peer pres-sure to make helmets “cool,” and to reducefinancial barriers to purchasing a helmet.Financial barriers were reduced by distribut-ing 100,000 helmet discount coupons to fam-ilies through physician offices, schools, youth
groups, and community events. In addition,1,300 helmets were sold at cost through theParent-Teacher Association, and another1,300 were donated to low-income children.
The Seattle campaign was successfulat increasing observed helmet use amongchildren ages 5 to 15, from a baseline rate of5.5% to nearly 16%, 16 months followingthe intervention. During the same timeperiod, observed helmet use among 5- to 15-year-olds remained stable in the controlcommunity of Portland, Oregon. Since the16-month campaign follow-up in Seattle, theobserved rate of helmet use among childrenhas increased even more, reaching 60% in1998. This increase in helmet use wasaccompanied by a two-thirds reduction inbicycle-related head injuries in the targetpopulation.44
Although these studies indicate that theuse of multiple strategies within a community-based intervention increased helmet use,other studies have found that the impact ofcomprehensive community-based programsvaries substantially with the socioeconomicstatus of the target population.45 In particu-lar, some community-based interventionsaimed at increasing bicycle helmet useamong children have been effective in high-income, but not low-income, communities.7–9
91Community-Based Injury Prevention Interventions
http://www.futureofchildren.org
PHOTO OMITTED
This is especially discouraging since chil-dren in low-income communities are oftenat higher risk for unintentional injuries.45
The studies discussed below illustrate theimportance of targeting economic barriersin a community as part of a community-based approach.
A series of evaluations were conducted of“Be Bike Smart,” a program that promotesbicycle helmet use among children ages 5 to14 in low- and high-income schools in asuburb of Toronto, Canada.7,8 This weeklongmultiple-strategy program included classroomteaching, peer presentations, and celebrityappearances to encourage helmet use among
children. Parents were targeted via mailingsand were invited to school activities. In con-junction with this educational program, bicy-cle helmets were sold at a 20% discount offthe regular price.7 In a subsequent “Be BikeSmart” campaign conducted only in low-income schools, the discount was raised to75% to further minimize financial barriers.8
Following both programs, children acrossgroups—regardless of whether or not theyreceived the intervention—demonstrated anincrease in observed helmet use. However,the intervention had a statistically signifi-cant effect on helmet use only in one sub-group: High-income children in theprogram that combined educational activi-ties with a 20% helmet discount were morelikely to wear a helmet following the inter-vention than were children in the controlgroup (36% versus 15%, respectively). Thelack of an intervention effect in low-incomecommunities was attributed to perceiveddangers or impracticalities of bicycling inhigh-density areas, differing belief systems,and financial and language barriers. Thus,results from the “Be Bike Smart” evaluationsindicate that additional reinforcement or
broader strategies may be necessary to over-come barriers to helmet use in low-incomecommunities.
In summary, results from the studiesincluded in this systematic review indicatethat community-based efforts can effectivelyincrease bicycle helmet use among children.To maximize the likelihood of success,efforts should be targeted broadly toincrease parents’ awareness of the impor-tance of helmet use, overcome resistance tohelmet use by educating children, subsidizehelmet costs, and pass regional legislationenforcing bicycle helmet use.
Even when these approaches areadopted, helmet use among children maynot be increased in all circumstances, anddifferent interventions may be required fordifferent populations. For example, low-income communities may be more difficultto influence with community-based bicycleinjury prevention programs. Regardless ofcommunity socioeconomic status, however,a common thread through several of thesestudies was the influence of peer pressureand modeling by adults. Children weremore likely to wear a bicycle helmet if theirfriends also wore a helmet or if they werewith an adult who also wore a helmet. Thiseffect is consistent with social learningtheory, which recognizes modeling and peergroup behaviors as both stimuli and activereinforcers of behavior change.35
Despite the positive impact of numerouscommunity-based interventions on chil-dren’s bicycle helmet use, the design ofthese evaluations and the limited outcomesexplored suggest that caution is warrantedwhen interpreting these results. Importantly,only two RCTs of community-based helmetpromotion programs were included in thisreview. In addition, nearly all studies focusedon helmet ownership or use; only onelooked at actual injuries.12 Future researchshould investigate the importance of bicyclepaths and general bicycle safety measures.
Programs TargetingMotor Vehicle Restraint UseIn 1996, motor vehicle occupant injuriesresulted in the deaths of 4,970 children andadolescents in the United States. Child pas-senger restraints for infants and young chil-dren, and adult shoulder-lap belts used
92 THE FUTURE OF CHILDREN – SPRING/SUMMER 2000
http://www.futureofchildren.org
A common thread through several of thesestudies was the influence of peer pressureand modeling by adults. Children were morelikely to wear a bicycle helmet if their friendsalso wore a helmet or if they were with anadult who also wore a helmet.
93Community-Based Injury Prevention Interventions
http://www.futureofchildren.org
correctly by children older than eight yearsof age, substantially reduce the probability ofserious injury or fatality (see the article byGrossman in this journal issue).46 Althoughchild safety restraint legislation has beenpassed in all 50 states, restraints are used foronly about 85% of infants and 60% oftoddlers.47 Furthermore, a large proportionof children are incorrectly restrained in carseats, and car seats are often installed incor-rectly in vehicles.48
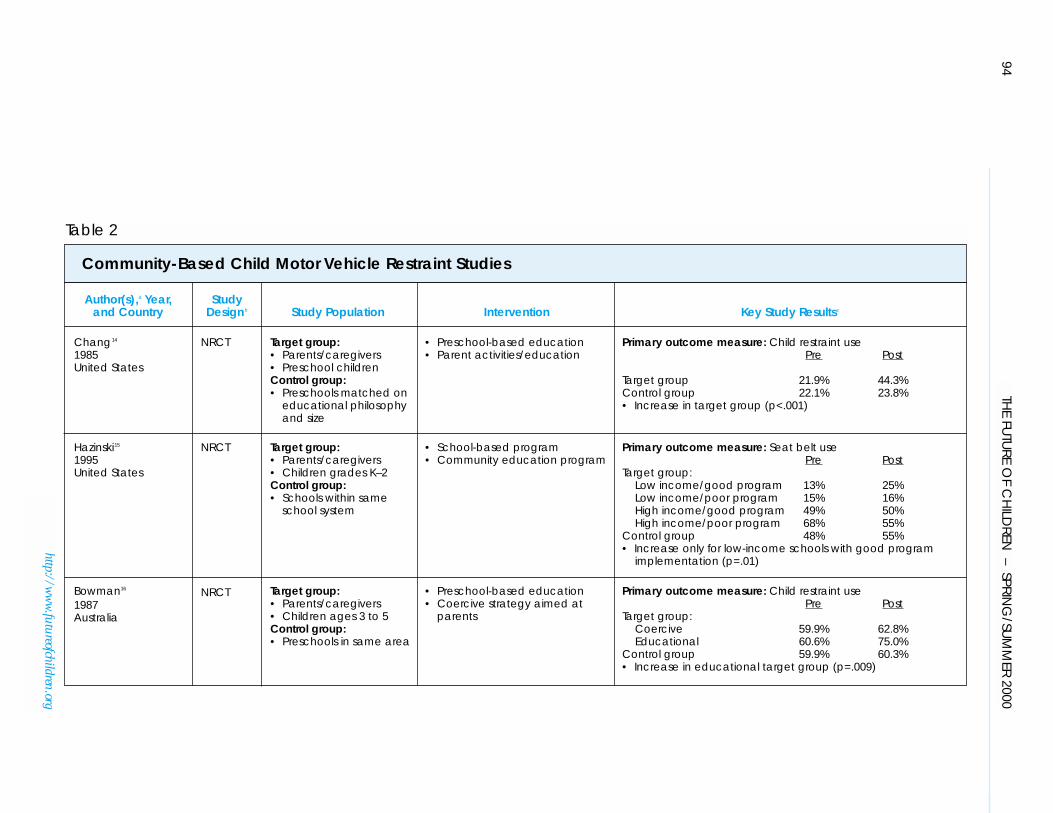
This review identified five community-based studies aimed at increasing motorvehicle restraint use among children14–17 oradolescents18 (see Table 2). (Interventionsfocused on increasing infant car seat use areprimarily delivered in clinical settings andare discussed in the article by DiGuiseppiand Roberts in this journal issue). Findingsfrom these studies indicate that multiple-strategy programs that educate preschool-ers, and programs that rely on parenteducation in concert with coercive tech-niques, can increase child motor vehiclerestraint use. However, interventions maybenefit more from the “carrot” than the“stick” approach to behavior change. Target-ing children’s behavior directly is particu-larly important, because child motor vehiclerestraint use is often inhibited when a childresists being restricted in a child safety seat anda weary parent succumbs to this resistance.Some of the most successful community-basedinterventions aimed at increasing childsafety restraint use focus primarily onincreasing compliance among children,with the theory that children may be trainedto serve as monitors of the family’s motorvehicle restraint behaviors.
The “Bucklebear” preschool-based cur-riculum, designed to increase child motorvehicle restraint use among preschool-agechildren in California, focused primarily onchildren to effect behavior change.14 Sixpreschools that adopted this curriculumwere compared with seven control pre-schools before they implemented the pro-gram and again three weeks afterimplementation. The program was success-ful, as evidenced by a significant increase insafety seat use among children in the inter-vention group (22% preintervention versus44% postintervention) with no changeamong controls (22% preinterventionversus 24% postintervention).
The Children’s Traffic Safety Program inTennessee is another school-based programaimed at increasing children’s motor vehiclerestraint use by targeting children and theirparents with a public education campaign.15
The program was based on the premise thatif young children (grades K–12) are taughtto adopt safety behaviors, they can theninfluence motor vehicle restraint use withintheir family. A community education cam-paign that included television, radio, andnewspaper features and public serviceannouncements ran parallel to the 10-weekschool-based curriculum. Control schoolswithin the same district did not receive theintervention. In addition to evaluating the
effect of the program on motor vehiclerestraint use, researchers also examined thevariation in impact by socioeconomic statusand the quality of program implementationat each school.
Program effectiveness was influenced byboth the quality of program implementationand socioeconomic status. Observed safetyrestraint use increased significantly only inlow-income schools with good programimplementation (13% preinterventionversus 25% postintervention), measured 5 to14 days after the intervention. In other inter-vention and control schools, the differencein motor vehicle restraint use before andafter the intervention was not significant.
Findings from this trial highlight the criti-cal importance of both program implementa-tion and the target population to a program’ssuccess. If program coordinators/teachers arenot adequately trained or do not presentthe program in the manner in which it wasdesigned, the impact may be diminished.Results from this trial mirror those
Some of the most successful community-basedinterventions aimed at increasing childsafety restraint use focus primarily onincreasing compliance among children, with the theory that children may be trainedto serve as monitors of the family’s motorvehicle restraint behaviors.
94TH
E FUTU
RE OF C
HILD
REN – SPRIN
G/SU
MM
ER 2000
http://ww
w.futureofchildren.org
Author(s),a Year, Studyand Country Designb Study Population Intervention Key Study Resultsc
Chang14 NRCT Target group: • Preschool-based education Primary outcome measure: Child restraint use1985 • Parents/caregivers • Parent activities/education Pre PostUnited States • Preschool children
Control group: Target group 21.9% 44.3%• Preschools matched on Control group 22.1% 23.8%
educational philosophy • Increase in target group (p<.001)and size
Hazinski15 NRCT Target group: • School-based program Primary outcome measure: Seat belt use 1995 • Parents/caregivers • Community education program Pre PostUnited States • Children grades K–2 Target group:
Control group: Low income/good program 13% 25%• Schools within same Low income/poor program 15% 16%
school system High income/good program 49% 50%High income/poor program 68% 55%
Control group 48% 55%• Increase only for low-income schools with good program
implementation (p=.01)
Bowman16 NRCT Target group: • Preschool-based education Primary outcome measure: Child restraint use 1987 • Parents/caregivers • Coercive strategy aimed at Pre PostAustralia • Children ages 3 to 5 parents Target group:
Control group: Coercive 59.9% 62.8%• Preschools in same area Educational 60.6% 75.0%
Control group 59.9% 60.3%• Increase in educational target group (p=.009)
Table 2
Community-Based Child Motor Vehicle Restraint Studies
95C
om
mun
ity-Base
d In
jury Preve
ntio
n In
terve
ntio
ns
http://ww
w.futureofchildren.org
Author(s),a Year, Studyand Country Designb Study Population Intervention Key Study Resultsc
Stuy17 RCT Target group: • Coercive parent strategy Primary outcome measure: Seat belt use 1993 • Parents/caregivers • Parent education Pre PostUnited States • Children ages two to six • Preschool education
Control group: Target group 54% 75%• Matched, randomized Control group 20% 30%
day care in the same city • Increase in use for both groups pre/post observation(p<.01) and between centers at post (p<.05)
Neuwelt18 NRCT Target group: • Educational Primary outcome measure: Seat belt use 1989 • High school students Pre PostUnited States Control group:
• High school students Target group 22.3% 29%in the same city Control group 42% 49%
KnowledgeTarget group 7.6% 8.4%Control group 7.5% 7.7%• No effect of intervention on seat belt use (p>.05)• Increase in knowledge in target group (p<.01)
a See the related endnotes at the end of this article.b RCT=randomized controlled trial; NRCT=nonrandomized study using a pre/post design with a comparison group.c A p value of less than .05 indicates that the difference between groups being compared is statistically significant.
Table 2 (continued)
Community-Based Child Motor Vehicle Restraint Studies
observed in bicycle helmet promotiontrials, reported earlier, in terms of differen-tial impact across socioeconomic status.However, whereas community-based pro-grams to increase bicycle helmet use weregenerally more effective in high-incomecommunities, this trial had a greater impactin low-income communities. This variationin results may be attributed to the muchlower baseline rates of restraint use in low-income than high-income schools in thisstudy, which allowed more room forimprovement. Despite the fact that low-income children demonstrated a signifi-cant increase in motor vehicle restraint use,
their postintervention use (16% to 25%)still was lower than the baseline use amonghigh-income children (49% to 68%).
A community-based trial in Australiacompared the effect of coercive tactics aimedat parents with an educational approachaimed at children.16 The coercive interven-tion threatened parents with random policechecks and fines, and it reminded them oflegislation mandating child safety restraintuse. The educational intervention relied onkits used by educators to teach preschoolchildren the importance of wearing automo-bile safety restraints. The rationale for teach-ing children was that this information would“filter up” to the parents and further increasethe use of child restraints.
Observations before and two weeks afterthe intervention revealed that only the edu-cational approach was effective at increasingautomobile safety restraint use amongpreschoolers (61% preintervention versus75% postintervention). Use did not increasein either the control or the coercive inter-vention groups. It was postulated that thecoercive intervention failed to impact safetyrestraint use because it did not deal with thefact that children often resist beingrestrained. In addition, the mere threat ofpolice involvement may not have been a
sufficient deterrent, and a more visiblepolice presence may be necessary.
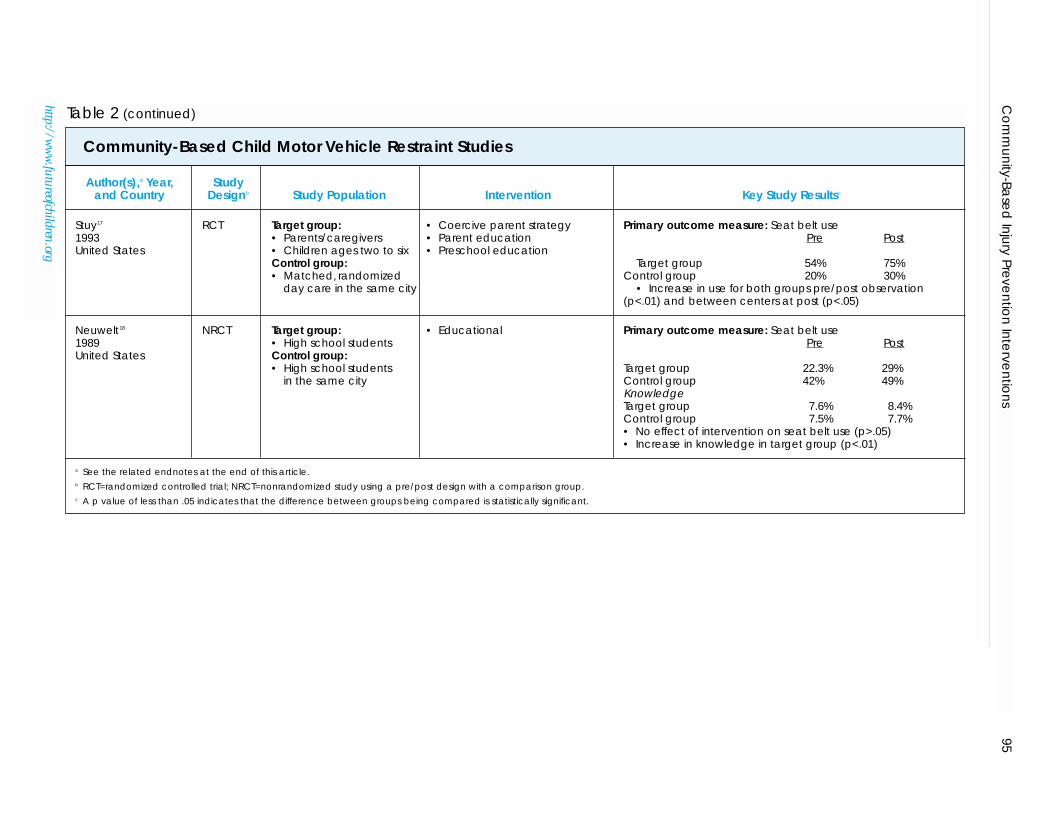
A positive approach to changing thesafety behavior of parents may have a greaterimpact on child safety restraint use thancoercive tactics. In an RCT aimed at increas-ing child safety restraint use, Stuy and col-leagues sought to alter the behavior ofparents by requiring them to sign a policystatement in which they agreed to complywith state laws and day-care center recom-mendations regarding child safety restraintuse.17 Based on the tenets of social learningtheory, Stuy and colleagues hypothesizedthat this program “buy-in” would help fostera sense of membership in a social group andthat parents would alter their behavior as aresult of modeling or reinforcement byother members or because of their ownactive involvement in the group. This strat-egy was combined with a comprehensiveeducational safety program in the school.
Child safety restraint use increased signif-icantly following the intervention in both theintervention (54% preintervention versus75% postintervention) and the control (20%preintervention versus 30% postinterven-tion) groups. Although child care centerswere randomly assigned to the interventionor control conditions, some differencesbetween the groups are worth noting. Specif-ically, the control centers had fewer whitefamilies, more single-parent families, andmore families with an annual income of lessthan $15,000. It is unlikely that these differ-ences substantially influenced the findings,however, and this “positive” approach wassuccessful at increasing child safety restraintuse. It also may be a less costly alternative tothe coercive approach described above, sinceit does not require visible enforcement.
Only one trial in this review, The OregonHead and Spinal Cord Injury PreventionProgram, was aimed at increasing shoulderand lap belt use among adolescents throughan educational campaign.18 This programrelied on a single strategy—providing emo-tionally charged information at a highschool assembly to change knowledge, atti-tudes, and behaviors regarding seat belt use.
The effectiveness of the program wasmeasured by observed seat belt use andquestionnaire measures of knowledge and
A positive approach to changing the safety behavior of parents may have agreater impact on child safety restraint use than coercive tactics.
96 THE FUTURE OF CHILDREN – SPRING/SUMMER 2000
http://www.futureofchildren.org
attitudes taken two weeks before and twoweeks after the intervention. The interven-tion was not associated with changes in seatbelt use or attitudes toward use. Only knowl-edge about the importance of seat belt useincreased following the intervention. Thismay be of little consequence, however, giventhe weak relationship between changes inknowledge and changes in injury behavior.37
Another study of this curriculum imple-mented in Washington State also found noconsistent change in knowledge, attitudes,or seat belt use associated with the interven-tion.49 Consistent with other community-based programs, these findings suggest thatsingle, one-time interventions to changebehavior are not successful.
In summary, several community-basedinterventions delivered in day-care or schoolsettings have increased motor vehiclerestraint use among young children. Theuse of multiple strategies to promote behav-ior change and a focus on increasingchildren’s acceptance of motor vehicle safetyseats appear critical to a program’s success.Additional well-designed RCTs of community-based interventions that use these strategieswould be useful to corroborate the findingsof the numerous nonrandomized studiesreported in this article. Rigorous community-based studies focusing on motor vehi-cle restraint use among adolescents alsoare needed.
Pedestrian Safety InterventionsPedestrian injuries among children andyouths accounted for nearly 19% of all pedes-trian deaths in 1996 (see the article by Gross-man in this journal issue). Preschool-agechildren are at particular risk, as they lackthe ability to judge the safety of street cross-ings and may be inadequately supervised bytheir parents.
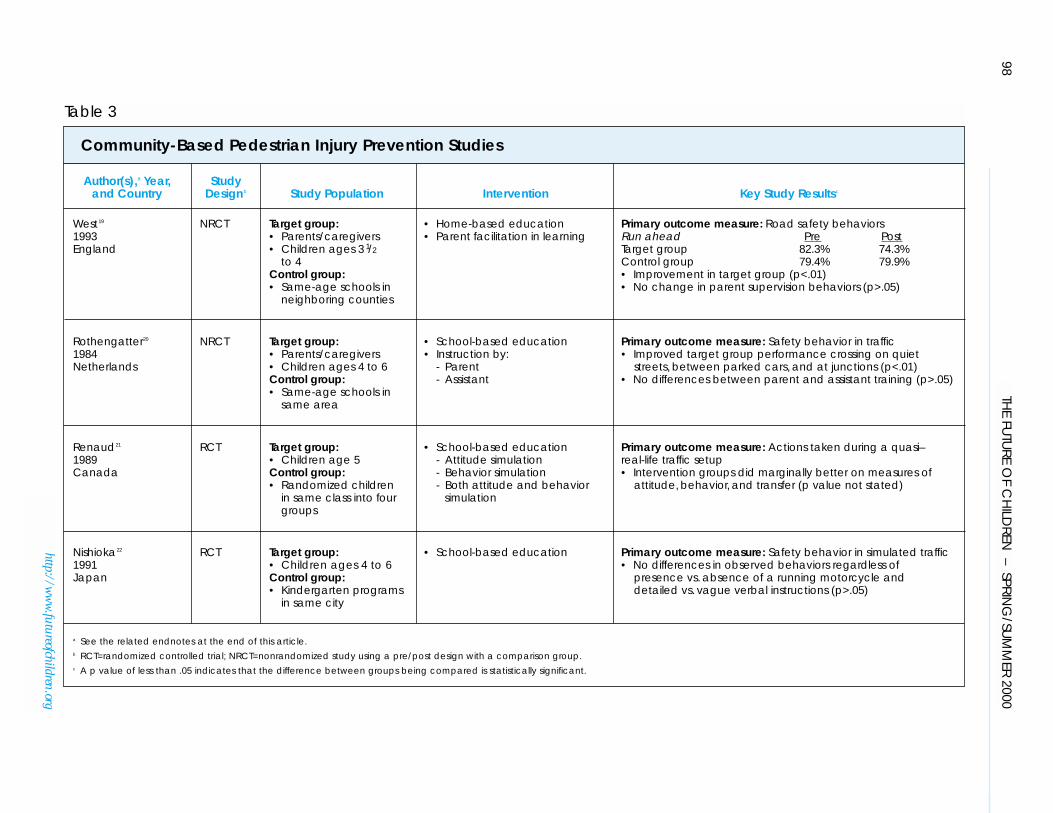
Four community-based studies aimed atreducing child pedestrian injuries met theinclusion criteria for this systematic review.These studies all targeted children betweenthe ages of three and six in school20–22 orhome19 settings (see Table 3). Two of thesewere RCTs that measured children’s trafficsafety behavior in simulated environments;they reported marginal21 or no improve-ment associated with the interventions.22
The two nonrandomized studies of childpedestrian interventions focused on parents
as supervisors and facilitators of children’sbehavior change.19,20 Both studies found thatwith appropriate training, parents or otheradults can positively impact children’s trafficsafety behavior. However, the one study thatreported numeric data found that even afterthe intervention nearly three-quarters ofchildren still ran ahead of their parents neartraffic, and participating parents did notdiffer from control parents in the amount orquality of their supervision.19
In summary, results from this review indi-cate that the benefit of community-basededucation aimed at improving traffic safetybehavior among young children is limited.The benefit of such interventions deliveredin a simulated setting is marginal at best, andthere is no evidence that children will
behave the same way in real-life settings.Although some evidence suggests thatcommunity-based interventions involvingparents or other instructors as supervisorsand facilitators can improve children’s trafficsafety behaviors, this improvement ismodest, and even after training, young chil-dren remain at substantial risk for pedes-trian injuries.
Developmentally, preschool-age childrenare not prepared to learn and react appro-priately to traffic.50 Therefore, physically sep-arating young children from traffic may be amore effective approach. Uncontrolled eval-uations of environmental approaches toreducing pedestrian injuries—such as bylowering speed limits, using speed bumpsand signs, or narrowing roads—have beenconducted, primarily in Europe, and arepromising.51–53 Future investigations usingrigorous methodological designs are neces-sary to quantify the benefits or shortcomingsof environmental approaches, because theyare gaining popularity over educationalinterventions.
97Community-Based Injury Prevention Interventions
Developmentally, preschool-age children are not prepared to learn and react appro-priately to traffic. Therefore, physically separating young children from traffic maybe a more effective approach.
http://www.futureofchildren.org
98TH
E FUTU
RE OF C
HILD
REN – SPRIN
G/SU
MM
ER 2000
http://ww
w.futureofchildren.org
Author(s),a Year, Studyand Country Designb Study Population Intervention Key Study Resultsc
West19 NRCT Target group: • Home-based education Primary outcome measure: Road safety behaviors1993 • Parents/caregivers • Parent facilitation in learning Run ahead Pre PostEngland • Children ages 3 1/2 Target group 82.3% 74.3%
to 4 Control group 79.4% 79.9%Control group: • Improvement in target group (p<.01)• Same-age schools in • No change in parent supervision behaviors (p>.05)
neighboring counties
Rothengatter20 NRCT Target group: • School-based education Primary outcome measure: Safety behavior in traffic1984 • Parents/caregivers • Instruction by: • Improved target group performance crossing on quietNetherlands • Children ages 4 to 6 - Parent streets, between parked cars, and at junctions (p<.01)
Control group: - Assistant • No differences between parent and assistant training (p>.05)• Same-age schools in
same area
Renaud21 RCT Target group: • School-based education Primary outcome measure: Actions taken during a quasi– 1989 • Children age 5 - Attitude simulation real-life traffic setupCanada Control group: - Behavior simulation • Intervention groups did marginally better on measures of
• Randomized children - Both attitude and behavior attitude, behavior, and transfer (p value not stated)in same class into four simulationgroups
Nishioka22 RCT Target group: • School-based education Primary outcome measure: Safety behavior in simulated traffic1991 • Children ages 4 to 6 • No differences in observed behaviors regardless of Japan Control group: presence vs. absence of a running motorcycle and
• Kindergarten programs detailed vs. vague verbal instructions (p>.05)in same city
a See the related endnotes at the end of this article.b RCT=randomized controlled trial; NRCT=nonrandomized study using a pre/post design with a comparison group.c A p value of less than .05 indicates that the difference between groups being compared is statistically significant.
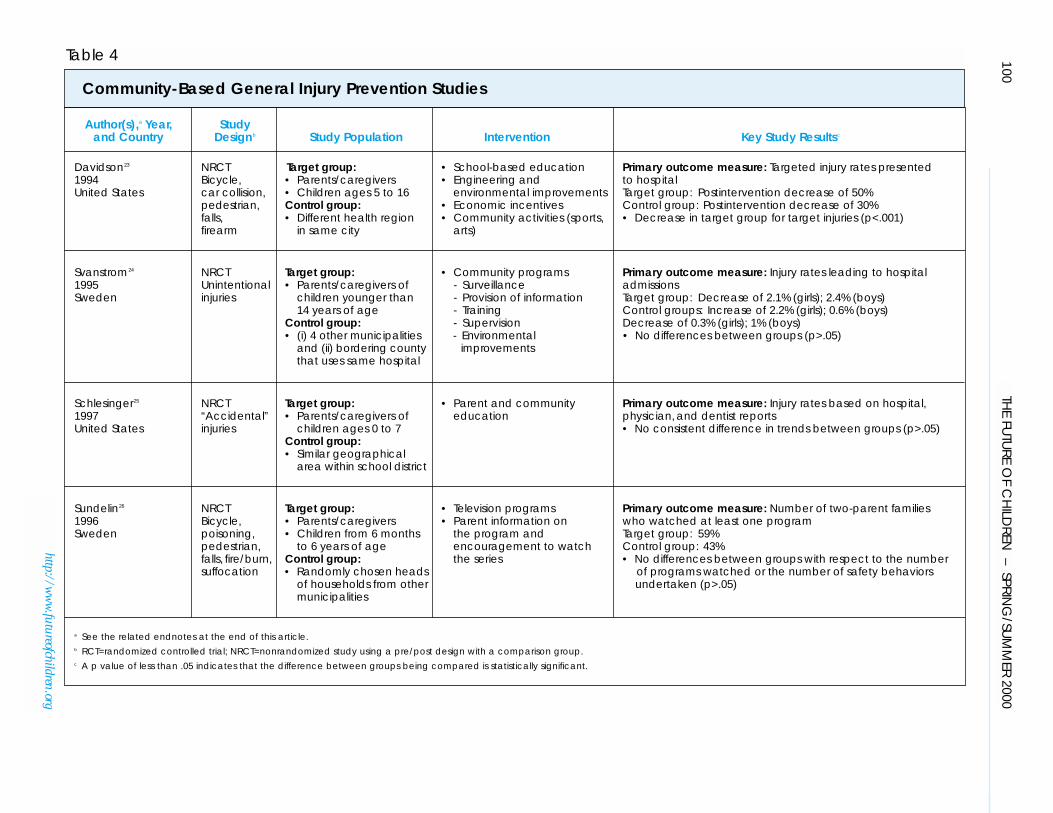
General Safety CampaignsThis article has discussed community-basedstudies, each focused on a specific type ofinjury. However, a major strength of thecommunity-based approach is the opportu-nity to target more than one type of injurywithin a community. Four nonrandomizedcommunity-based trials were found thatused general safety campaigns to target mul-tiple child-injury problems (see Table 4).23–26
Three of these used changes in injury ratesas a measure of program effectiveness,though only one trial reported statisticallysignificant decreases in injury rates associ-ated with the intervention.23 General safetycampaigns differ from other community-based interventions in that they tend to belong term and adapted over time to meetcommunity needs. The success of theseinterventions largely relies on input fromcommunity members and community own-ership of program activities.
The Safe Kids/Healthy NeighborhoodsCoalition illustrates how a successfulcommunity-based intervention grows andchanges within a community.23 This pro-gram, implemented in the Harlem neigh-borhood of New York City, was aimed atreducing a variety of childhood injuriesresulting from outdoor activities. The initia-tive was started because parents and educa-tors in central Harlem requested a programin playground safety from health profes-sionals. Surveys of playgrounds revealedthat they were being used by drug dealersand were in poor repair, and that childrenusing playgrounds had little adult supervi-sion. The Harlem Hospital Injury Preven-tion Program, in collaboration with a varietyof community groups and city agencies,started the Safe Kids/Healthy Neighbor-hoods Coalition with the following goals:(1) to renovate central Harlem play-grounds; (2) to involve children and adoles-cents in safe, supervised activities that teachuseful skills; (3) to provide injury and vio-lence prevention education; and (4) to pro-vide safety equipment (for example, bicyclehelmets) at reasonable cost. During the firstthree years of the program, 26 organiza-tions participated in the coalition, anddifferent programs and activities weredeveloped.
The effectiveness of this community-based coalition was evaluated by examining
changes in injury rates in the targeted agegroup (5- to 16-year-olds) for injuries tar-geted by the campaign (for example, allinjuries related to vehicles, outdoor falls,assaults, and guns) over nine years (1983 to1991). These rates were compared withchanges in the rates of nontargeted injuries(that is, poisoning, burns, and so on) andchanges in injury rates in a comparison com-munity (the suburb of Washington Heights)during the same time period.
Targeted injuries were reduced by anestimated 44% during the interventionperiod, with no significant decrease for non-targeted injuries; this decrease was noted
mainly in the targeted age group. Unexpect-edly, a 30% decline in severe injuries amongschool-age children also was observed inWashington Heights. However, the declinein Washington Heights occurred in both tar-geted (motor vehicle injuries only) and non-targeted categories. Whether this reductionin motor vehicle injuries observed in thecomparison community occurred indepen-dently of the intervention, or whether theeffect of the Safe Kids/Healthy Neighbor-hoods Coalition “spilled over” into Washing-ton Heights, could not be ascertained.Notwithstanding this concurrent change inthe control community, the authors con-cluded that the specific decrease in targetedinjuries within the targeted age group incentral Harlem demonstrated a positiveeffect of the intervention.
A second general injury prevention cam-paign, the Lidkoping Accident PreventionProgramme (LAPP), was associated with amodest, though not significant, rate decreasein injuries leading to hospital admission.24
Nonetheless, the comprehensiveness of the
99Community-Based Injury Prevention Interventions
http://www.futureofchildren.org
General safety campaigns differ from othercommunity-based interventions in that theytend to be long term and adapted over timeto meet community needs. The success ofthese interventions largely relies on inputfrom community members and communityownership of program activities.
100TH
E FUTU
RE OF C
HILD
REN – SPRIN
G/SU
MM
ER 2000
http://ww
w.futureofchildren.org
Author(s),a Year, Studyand Country Designb Study Population Intervention Key Study Resultsc
Davidson23 NRCT Target group: • School-based education Primary outcome measure: Targeted injury rates presented1994 Bicycle, • Parents/caregivers • Engineering and to hospitalUnited States car collision, • Children ages 5 to 16 environmental improvements Target group: Postintervention decrease of 50%
pedestrian, Control group: • Economic incentives Control group: Postintervention decrease of 30%falls, • Different health region • Community activities (sports, • Decrease in target group for target injuries (p<.001)firearm in same city arts)
Svanstrom24 NRCT Target group: • Community programs Primary outcome measure: Injury rates leading to hospital1995 Unintentional • Parents/caregivers of - Surveillance admissionsSweden injuries children younger than - Provision of information Target group: Decrease of 2.1% (girls); 2.4% (boys)
14 years of age - Training Control groups: Increase of 2.2% (girls); 0.6% (boys)Control group: - Supervision Decrease of 0.3% (girls); 1% (boys)• (i) 4 other municipalities - Environmental • No differences between groups (p>.05)
and (ii) bordering county improvementsthat uses same hospital
Schlesinger25 NRCT Target group: • Parent and community Primary outcome measure: Injury rates based on hospital,1997 “Accidental” • Parents/caregivers of education physician, and dentist reportsUnited States injuries children ages 0 to 7 • No consistent difference in trends between groups (p>.05)
Control group:• Similar geographical
area within school district
Sundelin26 NRCT Target group: • Television programs Primary outcome measure: Number of two-parent families1996 Bicycle, • Parents/caregivers • Parent information on who watched at least one programSweden poisoning, • Children from 6 months the program and Target group: 59%
pedestrian, to 6 years of age encouragement to watch Control group: 43%falls, fire/burn, Control group: the series • No differences between groups with respect to the numbersuffocation • Randomly chosen heads of programs watched or the number of safety behaviors
of households from other undertaken (p>.05)municipalities
a See the related endnotes at the end of this article.b RCT=randomized controlled trial; NRCT=nonrandomized study using a pre/post design with a comparison group.c A p value of less than .05 indicates that the difference between groups being compared is statistically significant.
strategies used and the collaborative approachadopted illustrate critical components ofpromising general safety campaigns.
LAPP was developed by a communityhealth unit in an effort to plan and coordi-nate health and safety in Lidkoping,Sweden. The program included five ele-ments: (1) surveillance of inpatient and out-patient injuries; (2) information, such astelephone hotlines and bicycle safety cam-paigns; (3) training of coaches, child carestaff, and parents in first aid or other injuryprevention areas; (4) supervision, includingmunicipal safety; and (5) environmentalimprovements, such as improving gym floorsto decrease slipping injuries. Key to this cam-paign was the involvement of representativesfrom existing community organizations,municipal administrations, welfare services,and the Red Cross, as well as communityprofessionals such as engineers, nurses,teachers, and police.
The impact of LAPP was evaluated bymeasuring decreases in rates of injuriesleading to hospital admissions over nineyears (1983 to 1991). During this time,there was an average annual decrease inhospital admissions in the interventiongroup of 2.4% for boys and 2.1% for girls,without a similar decrease in neighboringcomparison municipalities. These differ-ences were not significant, and manymethodological limitations were associatedwith the intervention, such as changes inrecording procedures at the hospitals andinconsistent implementation during theearly years of the program.
In summary, findings from generalcommunity-based safety campaigns aremixed at best. Only the Safe Kids/HealthyNeighborhoods Coalition has reportedstatistically significant decreases in targetedinjuries, and even in this study it is question-able whether the decrease in injury rates canbe wholly attributed to the intervention.Nonetheless, general safety campaigns thatadopt a broad array of strategies and garnersupport from numerous community con-stituencies are promising.
Future general safety campaigns shouldrely on these strategies and employ rigor-ous study designs to evaluate programimpact. RCTs may not be possible since the
success of these broad-based programslikely depends on an impetus for changethat comes from community constituen-cies, as with the Safe Kids/Healthy Neigh-borhoods Coalition. Thus, randomlyassigning a community to receive the inter-vention, whether or not the communityexpresses a desire for change, may diminishprogram success. Nevertheless, carefulselection of a comparison community thatis similar to the intervention communitywith respect to characteristics associatedwith the injury outcomes of interest, butdistant enough in proximity to avoid “spillover” effects, is critical. Evaluation of gen-eral safety campaigns also requires carefullystandardized data coding that is narrowenough to capture the different compo-nents of the program, yet broad enough toensure that data collection is manageable.Finally, more sophisticated data analysesare required so that possible confounds,such as variations in time, are statisticallycontrolled.
PHOTO OMITTED
102 THE FUTURE OF CHILDREN – SPRING/SUMMER 2000
http://www.futureofchildren.org
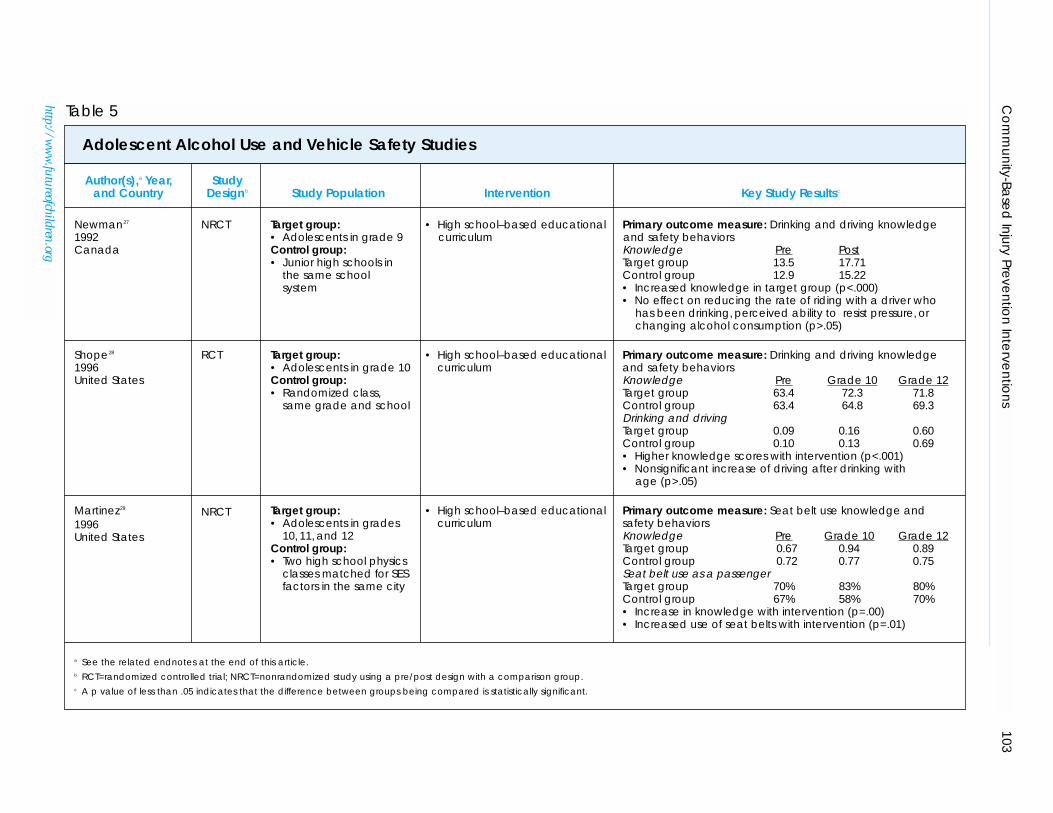
Programs Targeting AdolescentAlcohol Use and Vehicle SafetyMotor vehicle collisions are a major cause ofdeath and disability in youths, with alcoholplaying an important role in many instances(see the article by Grossman in this journalissue).54 Although interventions are neededto alter unsafe adolescent driving behaviors,risk-oriented behaviors common amongteenagers make this a difficult challenge.Peer pressure also is a powerful motivatoramong adolescents, and individual behaviorchange often is predicated on behaviorchange in one’s peer group.
This review identified three community-based programs aimed at decreasing alcoholmisuse and reckless driving amongteenagers (see Table 5).27–29 All three pro-grams were delivered as part of a high school
educational curriculum; only one was anRCT.28 While all programs reported that theintervention increased knowledge of therisks of consuming alcohol and operating amotor vehicle, only one trial found a changein behavior (self-reported increased seat beltuse when riding as a passenger) associatedwith the intervention.29 Because the linkbetween knowledge, attitudes, and subse-quent behaviors is tenuous at best,37 inter-ventions that affect the first two domains,but do not influence behavior change,should be viewed with caution.
Newman and colleagues developed aninnovative program, “Resisting Pressures toDrink and Drive,” designed to teach ninth-grade students the physiological effects ofalcohol, myths about alcohol use, and skillsto resist peer pressure to drink.27 Studentsfrom nine schools were assigned to eitherthe “Resisting Pressures to Drink and Drive”intervention group or to a control groupthat received the traditional alcohol educa-tion program. Increases in students’ knowl-edge associated with the intervention wereobserved after the first year of the program.
The intervention was not successful, how-ever, at changing behaviors (that is, reduc-ing the rate of riding with a driver who hasbeen drinking), changing teenagers’ per-ceived ability to resist peer pressure, orreducing alcohol consumption. In fact,both alcohol consumption and the numberof occurrences of riding with a driver whohad been drinking increased over time inboth groups.
A second school-based curriculum wasaimed at preventing alcohol use among10th grade students in nine Michigan highschools by preparing them to cope effec-tively with peer pressures to misuse alco-hol.28 Classes within each school wererandomly assigned to either the interven-tion or control groups, with the interven-tion delivered by trained teachers duringfive sessions. A significant increase inknowledge about alcohol, its physiologicaleffects, and resisting pressure to drink wasobserved in the intervention group follow-ing the intervention and again in 12thgrade, with no change among controls.However, despite this sustained gain inknowledge, self-reported alcohol misuseand driving a motor vehicle after drinkingstill increased over time among students inboth groups.
A similar program aimed at improvingvehicle safety included a weeklong moduleon injury control and crash safety informa-tion in a high school physics course.29 Theintervention covered forms of energy, injuryprevention, car safety features, types ofvehicular collisions, seat belts, and g forces,as well as hands-on activities. At baseline, thegroups were similar in terms of knowledge,self-reported seat belt use, speeding, anddriving under the influence of alcohol. Twoyears following the intervention, however,knowledge, reported seat belt use whenriding as a passenger, and intention ofalways wearing a seat belt were significantlyhigher in the intervention group. Despitethe positive behavioral change reflected inseat belt use—which increased from 70% to80% in the intervention group, but only67% to 70% among controls—this study suf-fered from notable limitations. Theseincluded differential dropout of risk takers(that is, teenagers most inclined to drivefast, drive after drinking one to two alco-holic beverages, and not wear a seat belt)
Although interventions are needed to alter unsafe adolescent driving behaviors,risk-oriented behaviors common amongteenagers make this a difficult challenge.
103C
om
mun
ity-Base
d In
jury Preve
ntio
n In
terve
ntio
ns
http://ww
w.futureofchildren.org
Author(s),a Year, Studyand Country Designb Study Population Intervention Key Study Resultsc
Newman27 NRCT Target group: • High school–based educational Primary outcome measure: Drinking and driving knowledge1992 • Adolescents in grade 9 curriculum and safety behaviorsCanada Control group: Knowledge Pre Post
• Junior high schools in Target group 13.5 17.71the same school Control group 12.9 15.22system • Increased knowledge in target group (p<.000)
• No effect on reducing the rate of riding with a driver whohas been drinking, perceived ability to resist pressure, orchanging alcohol consumption (p>.05)
Shope28 RCT Target group: • High school–based educational Primary outcome measure: Drinking and driving knowledge1996 • Adolescents in grade 10 curriculum and safety behaviorsUnited States Control group: Knowledge Pre Grade 10 Grade 12
• Randomized class, Target group 63.4 72.3 71.8same grade and school Control group 63.4 64.8 69.3
Drinking and drivingTarget group 0.09 0.16 0.60Control group 0.10 0.13 0.69• Higher knowledge scores with intervention (p<.001)• Nonsignificant increase of driving after drinking with
age (p>.05)
Martinez29 NRCT Target group: • High school–based educational Primary outcome measure: Seat belt use knowledge and 1996 • Adolescents in grades curriculum safety behaviorsUnited States 10, 11, and 12 Knowledge Pre Grade 10 Grade 12
Control group: Target group 0.67 0.94 0.89• Two high school physics Control group 0.72 0.77 0.75
classes matched for SES Seat belt use as a passengerfactors in the same city Target group 70% 83% 80%
Control group 67% 58% 70%• Increase in knowledge with intervention (p=.00)• Increased use of seat belts with intervention (p=.01)
a See the related endnotes at the end of this article.b RCT=randomized controlled trial; NRCT=nonrandomized study using a pre/post design with a comparison group.c A p value of less than .05 indicates that the difference between groups being compared is statistically significant.
Table 5
Adolescent Alcohol Use and Vehicle Safety Studies
104 THE FUTURE OF CHILDREN – SPRING/SUMMER 2000
http://www.futureofchildren.org
between follow-up assessments, and scoreson drinking and driving attitudinal ques-tions that left little room for improvement.
In summary, alcohol use among adoles-cents is a difficult behavior to modify, andcommunity-based programs aimed atreducing the likelihood that adolescentswill drive or ride with a driver under theinfluence of alcohol have been unsuccess-ful. In fact, results from these studies showthat adolescent alcohol consumption actu-ally increases with age, and increasedknowledge regarding alcohol misuse nega-tively correlates with subsequent alcohol-related behavior.
The failure of these studies to influenceadolescent behavior may reflect interventionsthat were poorly designed for this age group.
Because modeling peer group behaviors is soimportant for teenagers, future community-based strategies should appeal to the ability ofpeer groups to facilitate changes in normativebehavior. Differences within teenage peergroups also should be examined to deter-mine whether certain groups are moreamenable to change following differentstrategic interventions. It may be that differ-ent strategies need to be implemented for dif-ferent peer groups to maximize programsuccess. Teenagers who are involved in sports,for example, may respond most favorably tointerventions that focus on the potentialdetrimental effects of alcohol on athletic per-formance. Alternatively, educating youngwomen about the high caloric content ofalcoholic beverages may have the greatestimpact on their drinking behaviors. Becauseteenagers are in a unique developmentalstage, in which they are testing boundaries,interventions also may be more successful ifthey provide additional rewards and incen-tives for adopting well-defined vehicle safetybehaviors. Finally, future interventions shouldexplore more innovative and less pedagogical
approaches to promote adolescent safetybehaviors. Given the increased use of com-puter technology by youths, for example,Internet-based interventions should be testedas a potential venue for influencing adoles-cent safety behaviors.
Even if the effectiveness of community-based strategies can be improved by morecarefully designed and executed interven-tions, programs that rely on educationalstrategies to alter adolescent behaviors arelikely to be more successful when combinedwith regulatory or legislative approachessuch as graduated licensure (see the articleby Schieber, Gilchrist, and Sleet in this jour-nal issue). A recent systematic review of grad-uated licensure found that this approach islikely to reduce motor vehicle crashes andcrash-related injuries involving teenagers,although few evaluations of graduatedlicensing systems have been conducted.55
ConclusionsCommunity-based interventions have beensuccessful in some areas of childhood injuryprevention. Specifically, the increased use ofbicycle helmets and motor vehicle safetyseats among children has been associatedwith effective community-based programs.For other injury areas—including childpedestrian safety, adolescent alcohol useand vehicle safety, and general safetycampaigns—the benefit of community-based strategies is less evident. Lack of suc-cess in these areas may be attributed topoorly designed and implemented pro-grams, inadequate research methodology,or the inherent inability of community-based strategies to alter safety practices orreduce injury outcomes. For some safetybehaviors and target populations, such asmotor vehicle restraint use among adoles-cents, well-designed programs that includemultiple strategies and are grounded in anaccepted theory of behavior change simplyhave not been tested in community set-tings. For other areas, such as pedestriansafety among young children, there is evi-dence that community-based educationalinterventions alone are insufficient to con-sistently alter young children’s behaviorin traffic situations. Community-basedapproaches focused on engineering modi-fications to increase road safety may bemore effective, but have not been rigor-ously evaluated.
Community-based programs aimed atreducing the likelihood that adolescentswill drive or ride with a driver under theinfluence of alcohol have been unsuccessful.
Future community-based interventionsshould adopt the key elements commonamong the successful programs in this sys-tematic review. Education remains an impor-tant component of community-based injuryprevention efforts. All too often, though,education is viewed in only one dimension:the didactic presentation of information toaffect knowledge. The key assumption—thatchanges in knowledge automatically resultin changes in behavior—is not supported byresearch. Instead, changes in knowledgemust be accompanied by improved skill,changes in social norms, a supportive envi-ronment, and reinforcement that encour-ages behavior change. These aims may bedifficult to achieve in community programs,especially given the limited time of mostinterventions.
In addition to education, effective pro-grams use a broad array of other strategiesand rely on existing community organiza-tions and infrastructure, such as schools, themedia, and/or sponsorship by privateindustry (that is, to reduce costs of safetydevices). The selection of strategies shouldbe based on previous evidence identifyingfactors most amenable to change. Finally,messages should be tailored to address asmany community groups as possible withinthe target audience.
Perhaps the most important challenge indesigning community-based interventions isthe use of scientific evaluation. Recent evi-dence has established that nonrandomizeddesigns yield an overestimation of benefitcompared with randomized designs,56 andmany community interventions fail toemploy randomization, even when thisapproach is feasible.1 Randomization can beachieved by randomly assigning groups ofindividuals (for example, schools) or entirecommunities to control or intervention con-ditions. Cluster randomization, a techniquethat allows for randomization of communi-ties, should be used more frequently.57 It isonly when such rigorous designs are usedthat society will be able to determine wherebest to invest resources in community-basedinterventions.
The community-based approach toinjury prevention fits in well with the publichealth priority of improving the health ofpopulation groups. For communities to
maximize the potential benefit of thisapproach, they must become active partici-pants in injury prevention efforts. Manystudies included in this systematic reviewindicate that community organizationshave shown the commitment, the desire,and the ability to share the burden andresponsibility for reducing childhood unin-tentional injuries. In consultation withcommunity leaders and organizations,future studies should continue to test theeffect of well-designed community-basedapproaches aimed at improving safetybehaviors and reducing injuries amongchildren and youths.
The authors wish to extend their gratitude toJessie McGowan for the development of theirsearch strategy.
PHOTO OMITTED
106 THE FUTURE OF CHILDREN – SPRING/SUMMER 2000
http://www.futureofchildren.org
Methods Used for the Systematic Reviews
The search strategy was designed in conjunction with a research librarian to iden-tify studies that examined the effectiveness of a community-based injury controlintervention in decreasing injury rates or increasing behaviors that decrease injuryrates in children and adolescents. A filter (that is, a series of subject-related key-words used to extract potentially relevant articles from computerized databases) fordefining “community” was developed, tested, and included in the search strategies.Upon examining the results of the injury searches, it was apparent that not allpotentially relevant articles were being identified. Two additional search strategieswere developed, both including the community filter. As the age range varies foreach database, we accounted for this by using text words to specify ages in additionto numerical ages.
Databases Searched
Eight electronic databases were searched for studies published in any language.The databases included MEDLINE (1966–98), EMBASE (1974–98), Psychinfo(1967–98), Current Contents (wk1–wk25), HealthSTAR (1975–98), Sportdiscus(1949–98), CINAHL (1982–98), and The Cochrane Database of Systematic Reviews(CDSR) (1998, Issue 2). Separate searches of each database were conducted forthe following injury categories: (a) bicycle, walk, and motor vehicle; (b) gun,drown, and choke; (c) fall, burn, and electrocution; (d) poisoning and cuts; (e)sports and amputation. Detailed search strategies are available from the corre-sponding author. When references were retrieved by more than one database, pri-ority in downloading was given to MEDLINE. The journal Injury Prevention fromMarch 1995 to 1998 was searched by hand and four potentially relevant studieswere identified. A fifth article was identified through an article found inMEDLINE. Two additional articles were selected based on expert opinion. How-ever, due to time constraints, reference lists from relevant reviews were not exam-ined for potential studies.
Once the search process was complete, two members of the research teamscreened each citation and available abstract in the database. For all databases, letters,comments, editorials, or articles on sunburn, abuse, and other intentional injurieswere excluded. All references to injury in children or adolescents and those that useda study design that included a control group were tagged as potentially relevant. Arti-cles were reviewed and assessed using eligibility criteria established by the team.
Inclusion/Exclusion Criteria
A study was included if: (1) it included a control group that did not receive theintervention; (2) the target population was between 0 and 19 years of age (if agreater age range was examined, separate data analysis had to be conducted forthe 0 to 19 age group); (3) it examined the effectiveness of a community-basedintervention based in a setting such as a recreational center, school, or day-carecenter and involved any intervention between an individual-based approach anda state or nationwide one; and (4) it reported injury rates or change in an injury-reducing behavior. Three members of the team independently reviewed allpotentially relevant articles to determine the eligibility of each document. All dis-agreements were resolved by consensus.
Data Extraction
Pertinent information was extracted from each article by one member of the teamusing a Data Extraction Form (available upon request). To interpret the study, weattempted to extract the primary outcome of interest, the intervention used, and
1. Smith, P., Moffatt, M., Gelskey, S., et al. Are community health interventions evaluated appro-priately? A review of six journals. Journal of Clinical Epidemiology (1997) 50:137–46.
2. Morris, B.P., and Trimble, N.E. Promotion of bicycle helmet use among schoolchildren: Arandomized clinical trial. Canadian Journal of Public Health (1991) 82:92–94.
3. Towner, P., and Marvel, M.K. A school-based intervention to increase the use of bicycle hel-mets. Family Medicine (1992) 24:156–58.
4. Cote, T.R., Sacks, J.J., Lambert-Huber, D.A., et al. Bicycle helmet use among Maryland chil-dren: Effect of legislation and education. Pediatrics (1992) 89:1216–20.
5. Dannenberg, A.L., Gielen, A.C., Beilenson, P.L., and Wilson, M.H. Bicycle helmet laws andeducational campaigns: An evaluation of strategies to increase children’s helmet use. AmericanJournal of Public Health (1994) 83:667–74.
6. DiGuiseppi, C.G., Rivara, F.P., Koepsell, T.D., and Polissar, L. Bicycle helmet use by children.Evaluation of a community-wide helmet campaign. Journal of the American Medical Association(1989) 262:2256–61.
7. Parkin, P.C., Spence, L.J., Hu, X., et al. Evaluation of a promotional strategy to increase bicy-cle helmet use by children. Pediatrics (1993) 91:772–77.
8. Parkin, P.C., Hu, X., Spence, L.J., et al. Evaluation of a subsidy program to increase bicyclehelmet use by children of low-income families. Pediatrics (1995) 96:283–87.
9. Farley, C., Haddad, S., and Brown, B. The effects of a four-year program promoting bicyclehelmet use among children in Quebec. American Journal of Public Health (1996) 86:46–51.
relevant data about the results. The primary outcome reports the effectiveness ofthe intervention and is used to determine which sample size to report for thisstudy. If the primary outcome was unclear, the outcome which seemed to be the“most important” to eliminate bias was chosen. For example, if helmet ownershipand helmet use were both outcomes, helmet use was selected. In cases where atti-tude, behavior, and knowledge were all examined, behavior was selected.
Following data extraction, quality assessment was conducted for each ran-domized controlled trial (RCT) and nonrandomized controlled trial (NRCT)using the Jadad Scale, a validated instrument designed to assess methodologicalquality.1 Quality is scored between 0 and 5, with 5 being the highest score/quality.Three members of the team calibrated themselves on the instrument, and twoindependently completed quality assessments of each relevant study. Disagree-ments were resolved by consensus.
Results
A total of 1,236 citations were identified, of which 349 were duplicates, resulting in887 articles. The initial screen identified 158 potentially relevant articles. Two arti-cles were reviews, one was a meta-analysis, and the remaining 155 articles containedoriginal data. Of the 155 articles that were potentially relevant, 28 were included inthe review; 4 were not discussed further in this review, because they addressed othertypes of injury prevention (such as gun-playing); 5 were excluded and are discussedin the article by DiGuiseppi and Roberts in this journal issue; 5 were unavailablethrough the library; 2 were in French; and 111 did not meet the eligibility criteria.More than half of the excluded articles did not contain a control and/or did notuse a community-based intervention. Of the 28 studies discussed, 6 were RCTs and22 were NRCTs.
1 Jadad, A.R., Moore, R.A., Carroll, D., et al. Assessing the quality of reports of randomized clinical trials: Is blinding necessary?Controlled Clinical Trials (1996) 17:1–12.
Appendix (continued)
108 THE FUTURE OF CHILDREN – SPRING/SUMMER 2000
http://www.futureofchildren.org
10. Liller, K.D., Smorynski, A., McDermott, R.J., et al. The MORE HEALTH Bicycle Safety Project.Journal of School Health (1995) 65:87–90.
11. Moore, D.W., and Adair, V. Effects of a school-based education programme on safety helmetusage by 11- to 13-year-old cyclists. Educational Psychology (1990) 10:73–78.
12. Ekman, R., Schelp, L., Welander, G., and Svanstrom, L. Can a combination of local, regionaland national information substantially increase bicycle-helmet wearing and reduce injuries?Experiences from Sweden. Accident Analysis and Prevention (1997) 29:321–28.
13. Tenn, L., and Dewis, M.E. An evaluation of a Canadian peer-driven injury prevention pro-gramme for high-risk adolescents. Journal of Advanced Nursing (1996) 23:329–37.
14. Chang, A., Dillman, A.S., Leonard, E., and English, P. Teaching car passenger safety topreschool children. Pediatrics (1985) 76:425–28.
15. Hazinski, M.F., Eddy, V.A., and Morris, J.A.J. Children’s traffic safety program: Influence ofearly elementary school safety education on family seat belt use. Journal of Trauma (1995)39:1063–68.
16. Bowman, J.A., Sanson-Fisher, R.W., and Webb, G.R. Interventions in preschools to increasethe use of safety restraints by preschool children. Pediatrics (1987) 79:103–9.
17. Stuy, M., Green, M., and Doll, J. Child care centers: A community resource for injury preven-tion. Journal of Developmental and Behavioral Pediatrics (1993) 14:224–29.
18. Neuwelt, E.A., Coe, M.F., Wilkinson, A.M., and Avolio, A.E. Oregon Head and Spinal CordInjury Prevention Program and evaluation. Neurosurgery (1989) 24:453–58.
19. West, R., Sammons, P., and West, A. Effects of a traffic club on road safety knowledge and self-reported behaviour of young children and their parents. Accident Analysis and Prevention(1993) 25:609–18.
20. Rothengatter, T. A behavioural approach to improving traffic behaviour of young children.Ergonomics (1984) 27:147–60.
21. Renaud, L., and Suissa, S. Evaluation of the efficacy of simulation games in traffic safety edu-cation of kindergarten children. American Journal of Public Health (1989) 307–9.
22. Nishioka, N., Ieda, S., Takahashi, H., et al. An experimental study on the safety behavior ofchildren in a dashing-out situation: Effects of verbal instructions and traffic conditions onsafety behavior. IATSS Research (1991) 15:39–45.
23. Davidson, L.L., Durkin, M.S., Kuhn, L., et al. The impact of the Safe Kids/Healthy Neighbor-hoods Injury Prevention Program in Harlem, 1988 through 1991. American Journal of PublicHealth (1994) 84:580–86.
24. Svanstrom, L. The Lidkoping Accident Prevention Programme: A community approach topreventing childhood injuries in Sweden. Injury Prevention (1995) 1:169–72.
25. Schlesinger, E.R., Dickson, D.G., Westaby, J., et al. A controlled study of health education inaccident prevention: The Rockland County Child Injury Project. Injury Prevention (1997)3:218–23.
26. Sundelin, C., Rasmussen, F., Berfenstam, R., and Troedsson, K. Information through televi-sion: Does it promote child safety? Injury Prevention (1996) 2:36–40.
27. Newman, I.M., Anderson, C.S., and Farrell, K.A. Role rehearsal and efficacy: Two 15-monthevaluations of a ninth-grade alcohol education program. Journal of Drug Education (1992)22:55–67.
28. Shope, J.T., Copeland, L.A., Maharg, R., and Dielman, T.E. Effectiveness of a high school alco-hol misuse prevention program. Alcoholism: Clinical and Experimental Research (1996) 20:791–98.
29. Martinez, R., Levine, D.W., Martin, R., and Altman, D.G. Effect of integration of injury con-trol information into a high school physics course. Annals of Emergency Medicine (1996)27:216–24.
30. Hardy, M.S., Armstrong, F.D., Martin, B.L., and Strawn, K.N. A firearm safety program forchildren: They just can’t say no. Developmental and Behavioral Pediatrics (1996) 17:216–21.
31. Bixler, B., and Jones, R.L. High-school football injuries: Effects of a post-halftime warm-upand stretching routine. Family Practice Research Journal (1992) 12:131–40.
32. Van Schagen, I.N., and Brookhuis, K.A. Training young cyclists to cope with dynamic trafficsituations. Accident Analysis and Prevention (1994) 26:223–30.
33. Thomas, K.A., Hassanein, R.S., and Christophersen, E.R. Evaluation of group well-child carefor improving burn prevention practices in the home. Pediatrics (1984) 74:879–82.
34. Becker, M.H., and Mainman, L.A. Sociobehavioral determinants of compliance with healthand medical care recommendations. Medical Care (1975) 13:10–21.
35. Haggerty, R.J. Changing lifestyles to improve health. Preventive Medicine (1977) 6:289.
36. Green, L.W. Community health. St. Louis, MO: Times Mirror/Mosby College Publishing, 1990,pp. 81–102.
37. Pless, I.B., and Arsenault, L. The role of health education in the prevention of injuries to chil-dren. Journal of Social Issues (1987) 43:87–103.
38. Thompson, R.S., Rivara, F.P., and Thompson, D.C. A case-control study on the effectiveness ofbicycle safety helmets. New England Journal of Medicine (1989) 320:1361–67.
39. Thompson, D.C., Rivara, F.P., and Thompson, R.S. Effectiveness of bicycle safety helmets inpreventing head injuries: A case-control study. Journal of the American Medical Association (1996)276:1968–73.
40. Maimaris, C., Summers, C.L., Browning, C., and Palmer, C.R. Injury patterns in cyclists attend-ing an accident and emergency department: A comparison of helmet wearers and non-wearers.British Medical Journal (1994) 308:1537–40.
41. Thomas, S., Acton, C., Nixon, J., et al. Effectiveness of bicycle helmets in preventing headinjury in children. British Medical Journal (1994) 308:173–76.
42. McDermott, F.T., Lane, J.C., Brazenore, G.A., and Debney, E.A. The effectiveness of bicyclisthelmets: A study of 1,701 casualties. Journal of Trauma (1993) 34:834–45.
43. Spaite, D.M., Murphy, M., Criss, E.A., et al. A prospective analysis of injury severity among hel-meted and nonhelmeted bicyclists involved in collisions with motor vehicles. Journal of Trauma(1991) 31:1510–16.
44. Harborview Injury Prevention and Research Center, Seattle, WA. Personal correspondencewith Dr. Frederick Rivara, director, January 1999.
45. MacKay, M., Reid, D.C., Moher, D., and Klassen, T. Final report to Health Canada: Systematicreview of the relationship between childhood injury and socioeconomic status. No. H5301-7-CY07.Ontario, Canada: Child and Youth Injury Prevention Centre, 1999.
46. National Transportation Safety Board. The performance and use of child restraint systems, seatbelts,volume 1: Analysis. Washington, DC: NTSB, 1999.
47. U.S. Department of Transportation, National Highway Traffic Safety Administration. Children—Traffic safety facts. Washington, DC: DOT, NHTSA, 1996.
48. Decina, L.E., and Knoebel, K.Y. Child safety seat misuse patterns in four states. Accident Analy-sis and Prevention (1997) 29:129–32.
49. Wright, M., Rivara, F.P., and Ferse, D. Evaluation of the Think First head and spinal cordinjury prevention program. Injury Prevention (1995) 1:81–85.
50. Sandels, S. Young children in traffic. British Journal of Educational Psychology (1970) 40:111–16.
51. Engel, U., and Thomsen, L.K. Safety effects of speed reducing measures in Danish residentialareas. Accident Analysis and Prevention (1992) 24:17–28.
52. Van Houten, R., and Malenfant, L. The influence of signs prompting motorists to yield beforemarked crosswalks on motor vehicle-pedestrian conflicts at crosswalks with flashing amber.Accident Analysis and Prevention (1992) 24:217–25.
53. Vis, A.A., Dijkstra, A., and Slop, M. Safety effects of 30 Km/H zones in the Netherlands. Accident Analysis and Prevention (1992) 24:75–86.
54. U.S. Department of Transportation, National Highway Traffic Safety Administration. Trafficsafety facts 1996. Washington, DC: DOT, NHTSA, 1997.
55. Foss, R.D., and Evenson, K.R. Effectiveness of graduated driver licensing in reducing motorvehicle crashes. American Journal of Preventive Medicine (1999) 16:47–56.
56. Kunz, R., and Oxman, A.D. The unpredictability paradox: Review of empirical comparisonsof randomised and non-randomised clinical trials. British Medical Journal (1998) 317:1185–90.
57. Donner, A., and Birkett, N. Randomization by cluster: Sample size requirements and analysis.American Journal of Epidemiology (1981) 114:906–14.