Page 1
8/6/2019 Koletzko Allergy Prevention Singapore 2011
http://slidepdf.com/reader/full/koletzko-allergy-prevention-singapore-2011 1/8
1
Preventing allergy by nutritional intervention
Sibylle Koletzko
Dr. von HaunerschesKinderspital,
Ludwig-Maximilians-
University Munich
Objectives
● Epidemiology of allergy and the hygiene hypothesis
● Possible allergy prevention by nutritional intervention
● Maternal diet during pregnancy and breast-feeding
● Breast-feeding
● Soy formula
● Hydrolysed formula (the GINI-study)
● Supplementary feeding
The prevalence of the differentallergic diseases in relation to age
0 ½ 1 3 7 15
Age (years)
P r e v a l e n c e
foodallergy
atopicdermatitis
asthma
allergic rhinitis
Rising prevalence in the 70ies-90ies of allergicdiseases in children living in middle Europe
von Mutius
Atopy and exercise-induced bronchospasmin Ghana: 1993-2003
0
2
4
6
8
10
12
14
16
Atopy EIB
%1993
2003
P<0.001
P=0.004
EOD Addo Yobo & A Custovic, 2006
Page 2
8/6/2019 Koletzko Allergy Prevention Singapore 2011
http://slidepdf.com/reader/full/koletzko-allergy-prevention-singapore-2011 2/8
2
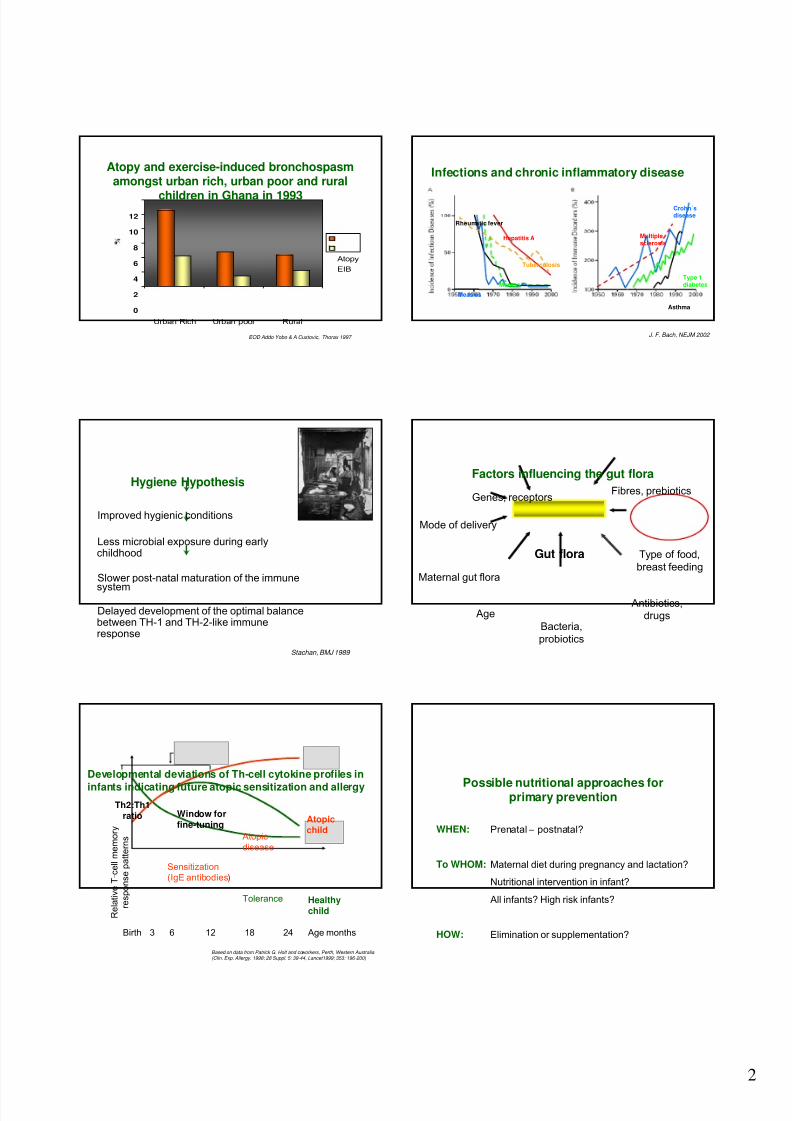
Atopy and exercise-induced bronchospasmamongst urban rich, urban poor and rural
children in Ghana in 1993
0
2
4
6
8
10
12
Urban Rich Urban poor Rural
Atopy
EIB
EOD Addo Yobo & A Custovic, Thorax 1997
Infections and chronic inflammatory disease
Hepatitis A
Measles
Rheumatic fever
Tuberculosis
Mumps
Crohn´sdisease
Multiplesclerosis
Type 1diabetes
Asthma
J. F. Bach, NEJM 2002
Hygiene Hypothesis
Improved hygienic conditions
Less microbial exposure during earlychildhood
Slower post-natal maturation of the immune
system
Delayed development of the optimal balancebetween TH-1 and TH-2-like immuneresponse
Stachan, BMJ 1989
Type of food,
breast feeding
Age
Bacteria,
probiotics
Antibiotics,drugs
Gut flora
Fibres, prebiotics
Maternal gut flora
Mode of delivery
Genes, receptors
Factors influencing the gut flora
Developmental deviations of Th-cell cytokine profiles in
infants indicating future atopic sensitization and allergy
Based on data from Patrick G. Holt and coworkers, Perth, Western Australia (Clin. Exp. Allergy. 1998; 28 Suppl. 5: 39-44, Lancet1999; 353: 196-200)
Sensitization(IgE antibodies)
Tolerance
Atopic
disease
Atopicchild
Healthychild
Age monthsBirth 3 6 12 18 24
Th2:Th1ratio
R e l a t i v e T - c e l l m e m o r y
r e s p o n s e p a t t e r n s
Window forfine-tuning
Possible nutritional approaches forprimary prevention
WHEN: Prenatal – postnatal?
To WHOM: Maternal diet during pregnancy and lactation?
Nutritional intervention in infant?
All infants? High risk infants?
HOW: Elimination or supplementation?
Page 3
8/6/2019 Koletzko Allergy Prevention Singapore 2011
http://slidepdf.com/reader/full/koletzko-allergy-prevention-singapore-2011 3/8
3
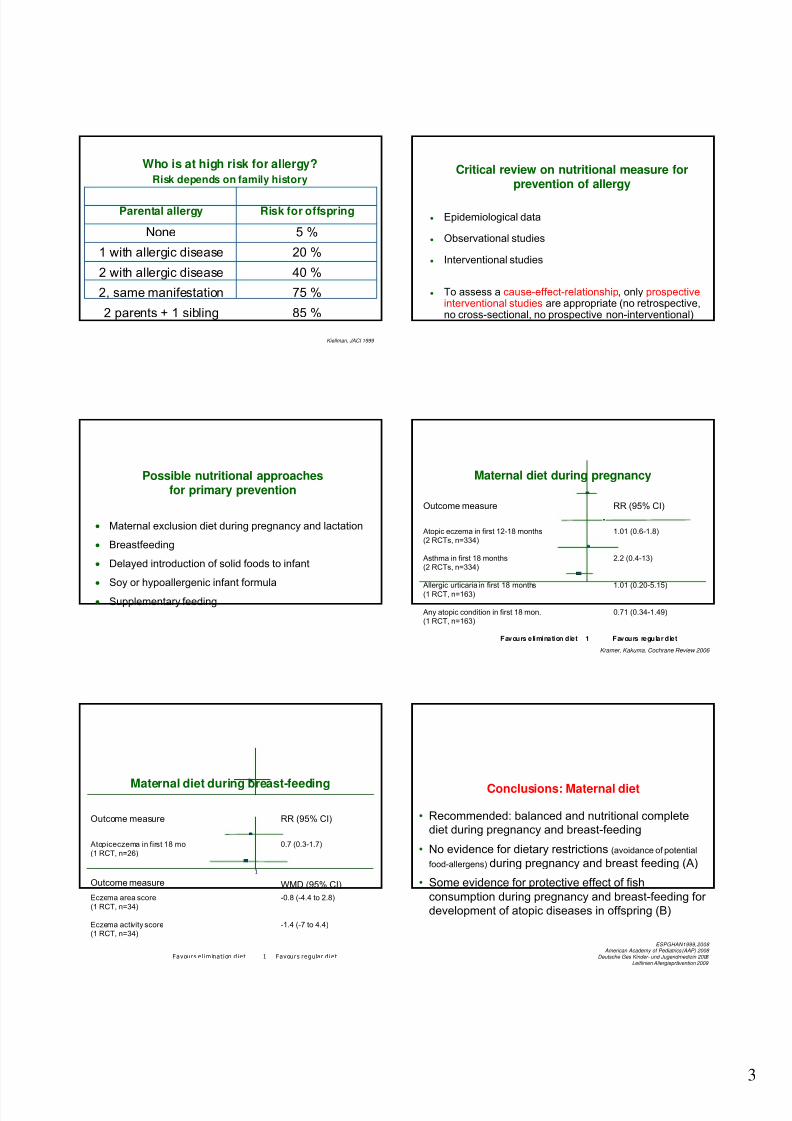
Who is at high risk for allergy?
Risk depends on family history
85 %2 parents + 1 sibling
75 %2, same manifestation
40 %2 with allergic disease
20 %1 with allergic disease
5 %None
Risk for offspringParental allergy
Kiellman, JACI 1999
Critical review on nutritional measure forprevention of allergy
• Epidemiological data
• Observational studies
• Interventional studies
• To assess a cause-effect-relationship, only prospectiveinterventional studies are appropriate (no retrospective,no cross-sectional, no prospective non-interventional)
• Maternal exclusion diet during pregnancy and lactation
• Breastfeeding
• Delayed introduction of solid foods to infant
• Soy or hypoallergenic infant formula
• Supplementary feeding
Possible nutritional approachesfor primary prevention
Maternal diet during pregnancy
0.71 (0.34-1.49)Any atopic condition in first 18 mon.(1 RCT, n=163)
1.01 (0.20-5.15)Allergic urticaria in first 18 months
(1 RCT, n=163)
2.2 (0.4-13)Asthma in first 18 months(2 RCTs, n=334)
1.01 (0.6-1.8)Atopic eczema in first 12-18 months(2 RCTs, n=334)
RR (95% CI)Outcome measure
Kramer, Kakuma. Cochrane Review 2006
Favours elimination diet 1 Favours regular diet
-1.4 (-7 to 4.4)Eczema activity score(1 RCT, n=34)
-0.8 (-4.4 to 2.8)Eczema area score
(1 RCT, n=34)
WMD (95% CI)Outcome measure
0.7 (0.3-1.7)Atopiceczema in first 18 mo
(1 RCT, n=26)
RR (95% CI)Outcome measure
Favours e l im inat ion d ie t 1 Favours regu lar d ie t
1
Maternal diet during breast-feeding Conclusions: Maternal diet
• Recommended: balanced and nutritional complete
diet during pregnancy and breast-feeding
• No evidence for dietary restrictions (avoidance of potential
food-allergens) during pregnancy and breast feeding (A)
• Some evidence for protective effect of fish
consumption during pregnancy and breast-feeding for
development of atopic diseases in offspring (B)
ESPGHAN1999, 2008 American Academy of Pediatrics (AAP) 2008
Deutsche Ges Kinder- und Jugendmedizin 2008 Leitlinien Allergieprävention 2009
Page 4
8/6/2019 Koletzko Allergy Prevention Singapore 2011
http://slidepdf.com/reader/full/koletzko-allergy-prevention-singapore-2011 4/8
4
Does breast-feeding reduces the risk for allergy?
• Very conflicting data whether any, prolonged or
exclusive breast-feeding reduces the risk for
allergic diseases.
• Evidence mostly from observational studies,
(reverse causality is likely)
Breast-feeding: no protection against asthmaUS Agency for Healthcare Research and Quality, 2007
??
Exclusive breast-feeding for at least 3 months doesNOT reduce the risk for later atopic dermatitis
Conclusion: Breastfeeding
• There are many good reasons to promote
breastfeeding during the first half year of life.
• The available knowledge does not support the
evidence that prolonged or exclusive
breastfeeding reduces the risk for atopic
dermatitis, asthma or allergic rhinitis.
Formulae for infants
Intact Protein Partial ly hydrolyzed Extensively hydrolyzed Amino acid formula
Allergenicity
WheyCasein
Cow’s milk formulaSoy formulaGoat’s milk formula
HA-formulaWheyCasein
For treatment of cow’s milk allergy
• „Feeding with a soy formula cannot be
recommended for prevention of allergy or
food intolerance …“
Osborn DA, Sinn J. Soy formula for prevention of allergy and food intolerance in
infants.Cochrane Database Syst Rev. 2006 Oct 18;(4):CD003741
Soy formula:no benefit for allergy prevention
Page 5
8/6/2019 Koletzko Allergy Prevention Singapore 2011
http://slidepdf.com/reader/full/koletzko-allergy-prevention-singapore-2011 5/8
5
Depending on the degree of enzymatic hydrolysis,
ultraheating and ultrafiltration classified as
partially hydrolysed formula (pHF) (18% >6000 Dalton)
extensively hydrolysed formula (eHF) (0.5-2% >6000 Dalton)
and
depending on the protein source
whey or casein hydrolysate
Hypoallergenic protein hydrolysates Hydrolysed formulae: Major questions
• Are hydrolysed cow‘s milk based formulae able to reducethe incidence of allergic diseases?
• Short- or long-term effect?
• Is the starting protein (whey/casein) and/ or the degreeof hydrolysation important for the effect?
• Is the effect dependent on the family history for atopy?
• Does nutrition in early life have any influence on the
particular type of allergic manifestation?
German Infant Nutritional Intervention study
Objective of the studyTo investigate the allergy preventive effect of three different
hydrolysed formulas compared with a regular cow’s milk based
formula in the first three years of life in children at risk of allergic
diseases.
The study is supported by the German Federal Ministryfor Education, Science, Research and Technology, grant no 01EE 9401-4
Recruitment and study design
5991 healthyterm neonatesborn 1995-1998
Pos. familyhistoryof allergy Pos. family history, but refusal
Neg. family history of allergy
Intervention group: n=2252breastmilk +/- 4 study formulae
Non-Intervention group: n=3739breastmilk +/- free formula
•Formula used for intervention
Hydrolysates:
Partially hydrolysed whey formula pHF-W
NAN HA®Extensively hydrolysed whey formula eHF-W
Nutrilon pepti®Extensively hydrolysed casein formula eHF-C
Nutramigencompared with
Regular cow‘s milk based formula CMF
Blinded formulas of the GINI study,
4 letters for each kind of formula
Feeding recommendations in theintervention group
• Breastfeeding for at least 4, better 6 months.
• Feeding the randomised study formula as only supplement
for breastfeeding during intervention period of 4 months
• No solids within the first 4 months.
• Thereafter, only one new solid food per week.
• No potentially allergenic foods as whole cow‘s milk and
diary products, hens‘s egg, fish, nuts, and citrus during the
first year of life.
Page 6
8/6/2019 Koletzko Allergy Prevention Singapore 2011
http://slidepdf.com/reader/full/koletzko-allergy-prevention-singapore-2011 6/8
6
Feeding characteristics in intervention group:Distribution of study formula and human milk
excl. study formula
study formula +human milk
excl. human milk
0
20
40
60
80
100
CMF
n=453
pHF-W
n=455
eHF-W
n=456
eHF-C
n=446
%
n= 1810
Non-intervention, pos. family historyNon-intervention, neg. family history
HR 1.9 (95% CI 1.5-2.4)
Intervention, pos. family history
Adjusted cumulative incidence of physician diagnosedatopic dermatitis in fully breast-fed infants with positiveand negative family history of atopy
v. Berg et al. Clin & Experimental Allergy 2009
Significant different characteristics between fullybreastfed & partly or non-breastfed children in theintervention & non-intervention group
0
10
20
30
40
50
60
70
80
U r b a
n a r
e a
S c h o
o l > 1 0
P e t k
e e p i
n g
M a t e
r n a l
s m o k
i n
S o l i d
s < 4 m
o
E g g , C P M
fully BF Int mixed/no BF Int fully BF Non-Int mixed/no BF Non-Int
J Pediatr 2004;104:602-7
*
*
*
*
* *
* *
*
*
* *
* p<0.05
%
*p < 0.05 forpHF-W and eHF-Cvs CMF
*
*
*
*
**
Cumulative incidence of atopic dermatitisin the 4 intervention groups (per protocol analysis)
v. Berg, Koletzkoet al. J ACI 2003;111:533-40
0
5
10
15
20
25
birth first second third year
CMF pHF-W
eHF-W eHF-C
Adjusted cum. Incidenz von Arztdiagnose
N=402
N=889 p h y s i c i a n d i a g n o s e d e c z e m a [ a d j . % ]
age [years]1 2 3 4 5 6
6
0
7
0
8
0
9
0
10
0
15
0
20
0
25
0
30
0
35
0
40
00
NI:
NI:NI pos. family history
NI neg. family history
NI pos. family history
NI neg. family history
HR 2.1 (95% CI 1.6-2.7)
Adj. cumulative incidence of physician diagnosed atopic dermatitis
in formula-fed infants with pos. and neg. family history for atopy
NI = non-intervention, formula freely chosen by mother
v. Berg et al. Clin & Experimental Allergy 2009
Adjusted cum. Incidenz von Arztdiagnose
I non compliant, HR 2.7 (95% CI 1.9-3.9)
I CMF, HR 2.6 (95% CI 2.0-3.5)
NI FH+, HR 2.1 (95% CI 1.6-2.7)
NI FH-,
NI non-InterventionI =Intervention
N=402
N=889 p h y s i c i a n d i a g n o s e d e c z e m a [ a d j . % ]
age [years]1 2 3 4 5 6
6
0
7
0
8
0
9
0
10
0
15
0
20
0
25
0
30
0
35
0
40
00
NI:
NI:
N=224
N=118
I: CMF
I: non-compliant
Adj. cumulative incidence of physician diagnosed atopic dermatitis
in formula-fed infants with pos. and neg. family history for atopy
NI = non-intervention, formula freely chosen by mother
Pos. familiy history
Neg. family history
v. Berg et al. Clin & Experimental Allergy 2009
Page 7
8/6/2019 Koletzko Allergy Prevention Singapore 2011
http://slidepdf.com/reader/full/koletzko-allergy-prevention-singapore-2011 7/8
7
Adjusted cum. Incidenz von Arztdiagnose
I non compliant, HR 2.7 (95% CI 1.9-3.9)I CMF, HR 2.6 (95% CI 2.0-3.5)
I eHF-W, HR 1.9 (95% CI 1.4-2.6)
I pHF-W, HR 1.6 (95% CI 1.2-2.3)
I eHF-C, HR 1.3 (95% CI 0.9-1.9)
NI FH+ fb-, HR 2.1 (95% CI 1.6-2.7)
NI FH-fb-, 1.0
NI = non-Intervention
I =Intervention
N=224
N=180
N=211
N=118
N=204
N=402
N=889 p h y s i c i a n d i a g n o s e d e c z e m a [ a d j .
% ]
age [years]
6
0
7
0
8
0
9
0
10
0
15
0
20
0
25
0
30
0
35
0
40
00
NI:
I: CMF
I: eHF-C
I: eHF-W
I: non-compliant
I: pHF-W
NI:
1 2 3 4 5 6
Adj. cumulative incidence of physician diagnosed atopic dermatitisin formula-fed infants with pos. and neg. family history for atopy
Pos. familiy history
Neg. family history
v. Berg et al. Clin & Experimental Allergy 2009
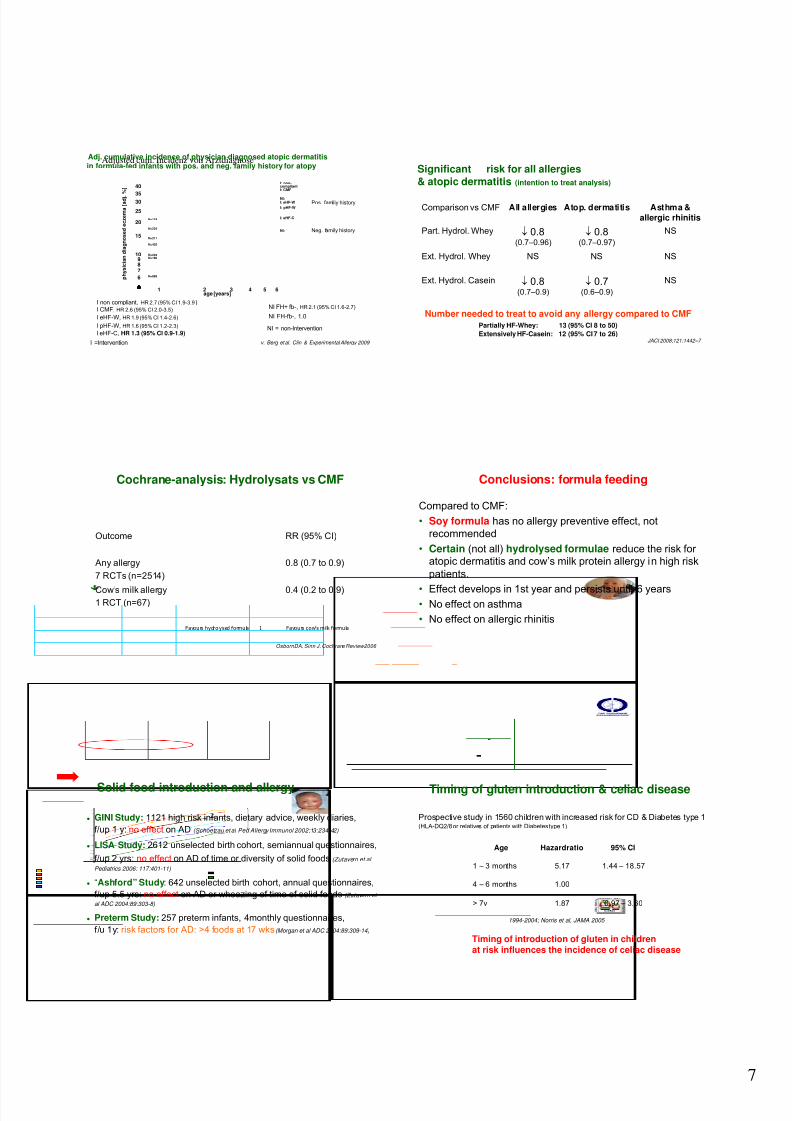
Comparison vs CMF All allergies Atop. dermatitis Asthma &allergic rhinitis
Part. Hydrol. Whey ↓ 0.8(0.7–0.96)
↓ 0.8(0.7–0.97)
NS
Ext. Hydrol. Whey NS NS NS
Ext. Hydrol. Casein ↓ 0.8(0.7–0.9)
↓ 0.7(0.6–0.9)
NS
JACI 2008;121:1442–7
Number needed to treat to avoid any allergy compared to CMFPartially HF-Whey: 13 (95% CI 8 to 50)
Extensively HF-Casein: 12 (95% CI 7 to 26)
Significant risk for all allergies& atopic dermatitis (intention to treat analysis)
Cochrane-analysis: Hydrolysats vs CMF
0.4 (0.2 to 0.9)Cow’s milk allergy1 RCT (n=67)
0.8 (0.7 to 0.9)Any allergy
7 RCTs (n=2514)
RR (95% CI)Outcome
Favours hydrolysed formula 1 Favours cow’s milk formula
OsbornDA, Sinn J. Cochrane Review2006
Conclusions: formula feeding
Compared to CMF:
• Soy formula has no allergy preventive effect, not
recommended
• Certain (not all) hydrolysed formulae reduce the risk for atopic dermatitis and cow’s milk protein allergy in high risk
patients.
• Effect develops in 1st year and persists until 6 years• No effect on asthma
• No effect on allergic rhinitis
Solid food introduction and allergy
• GINI Study: 1121 high risk infants, dietary advice, weekly diaries,
f/up 1 y: no effect on AD (Schoetzau et al Ped Allergy Immunol 2002;13:234-42)
• LISA Study: 2612 unselected birth cohort, semiannual questionnaires,
f/up 2 yrs: no effect on AD of time or diversity of solid foods(Zutavern et al
Pediatrics 2006: 117:401-11)
• “Ashford” Study: 642 unselected birth cohort, annual questionnaires,
f/up 5.5 yrs: no effect on AD or wheezing of time of solid foods(Zutavern et
al ADC 2004:89:303-8)
• Preterm Study: 257 preterm infants, 4monthly questionnaires,
f/u 1y: risk factors for AD: >4 foods at 17 wks(Morgan et al ADC 2004:89:309-14)
Prospective study in 1560 children with increased risk for CD & Diabetes type 1(HLA-DQ2/8 or relatives of patients with Diabetes type 1)
1994-2004; Norris et al, JAMA 2005
1.004 – 6 months
0.97 – 3.601.87> 7v
1.44 – 18.575.171 – 3 months
95% CIHazardratioAge
Timing of introduction of gluten in childrenat risk influences the incidence of celiac disease
Timing of gluten introduction & celiac disease
Page 8
8/6/2019 Koletzko Allergy Prevention Singapore 2011
http://slidepdf.com/reader/full/koletzko-allergy-prevention-singapore-2011 8/8
8
Introduction of gluten while still breast-feeding
risk for celiac disease
Akobenget al. ArchDis Child2006;91:39-43
Do we have a window of opportunity ?
Months 0 – 4 5 – 6 5 – 12
?
For countries/populations with high hygiene:
Solid foods should be introduced in the 5th and 6th
months of age, regardless of the familial risk of allergy
and breast-feeding or formula-feeding
„ Prevent CD“Prevention of Celiac Disease with Nutritional Intervention
1000 high risk infants for CD (family hx, DQ2/DQ8 pos)RCTwith gluten during months 5&6 vs. placebo)
Conclusions: Solid food introduction
• Very early solid food introduction (< 3 – 4 months of life) with a
high variety of different foods may increase the risk of
allergic diseases (eczema).
• Delaying the introduction of solids food beyond the 6th
months of life has no protective effect or may be even
increase the risk for allergy.
• This also applies to allergenic foods like hen‘s egg, cow‘smilk, fish, wheat.
Summary
● Increased incidence of allergies in countries/populations with
high hygiene (western life-style)
● Nutrition in early life plays a role for tolerance induction
● NO allergy preventive effect with maternal diet during
pregnancy and breast-feeding
● Certain hydrolysed formulae (not soy formula) reduce the risk
for atopic dermatitis & CMPA in high risk patients compared to
CMF. No effect on asthma and allergic rhinitis
● Too early (<3months) and too late (>>6 months)introduction of
solids (wheat) increases the risk for atopic dermatitis (celiac
disease) in high risk infants
● Remember: breast is best
Thank you
for your kind attention!