Peripheral Arterial Disease Guidelines: Management of Patients with Lower Extremity PAD A Collaboration of the American College of Cardiology , the American Heart Association, the American Associat ion for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology , Society for Vascular Medicine and Biology, and the PAD Coalition. The PAD Coalition SVMB
Transcript
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Peripheral Arterial Disease Guidelines:Management of Patients with Lower Extremity PAD
A Collaboration of the American College of Cardiology, the American HeartAssociation, the American Association for Vascular Surgery/Society forVascular Surgery, Society for Cardiovascular Angiography and Interventions,Society of Interventional Radiology, Society for Vascular Medicine and
Biology, and the PAD Coalition.
The PAD CoalitionSVMB
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
The First Tool to Establish the PAD Diagnosis:The HPI, ROS, and Phy sic al Exam inat ion
• Individuals with asymptomatic PAD should beidentified in order to offer therapeuticinterventions known to diminish their increasedrisk of myocardial infarction, stroke, and death.
• A history of walking impairment, claudication,and ischemic rest pain is recommended as a
required component of a standard review ofsystems for adults >50 years who haveatherosclerosis risk factors, or for adults >70years.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
A s y m p t o m a t i c : Without obvious symptomaticcomplaint (but usually with a functional impairment).
Class ic Claud icat ion : Lower extremity symptomsconfined to the muscles with a consistent (reproducible)onset with exercise and relief with rest.
“Atypical” leg pain : Lower extremity discomfort that isexertional, but that does not consistently resolve withrest, consistently limit exercise at a reproducibledistance, or meet all “Rose questionnaire” criteria.
This guideline recognizes that:
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
• The ankle-brachial index is 95% sensitive and 99% specific for PAD• Establishes the PAD diagnosis• Identifies a population at high risk of CV ischemic events• “Population at risk” can be clinically & epidemiologically defined:
The Ankle-Brachial Index
Exer t ional l eg s ym ptom s , non- healing w ou nd s, age > 70, age > 50years wi th a h i s to ry o f sm oking o rdiabetes.
• Toe-brachial index (TBI) useful inindividuals with non-compressible pedalpulses
Lijmer JG. Ultrasound Med Biol 1996;22:391-8; Feigelson HS. Am J Epidemiol 1994;140:526-34;
Baker JD. Surgery 1981;89:134-7; Ouriel K. Arch Surg 1982;117:1297-13; Carter SA. J Vasc Surg 2001;33:708-14
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Duplex ultrasound of the extremitiesis useful to diagnose anatomiclocation and degree of stenosis ofperipheral arterial disease.
• Duplex ultrasound is useful toprovide surveillance followingfemoral-popliteal bypass usingvenous conduit (but not prostheticgrafts).
• Duplex ultrasound of the extremitiescan be used to select candidates for:(a) endovascular intervention;(b) surgical bypass, and(c) to select the sites of surgical
anastomosis.
However, the data thatmight support use of
duplex ultrasound toassess long-termpatency of PTA is notrobust.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Duplex ultrasound of the extremities is usefulto diagnose the anatomic location and degree
of stenosis of PAD.
Duplex ultrasound is recommended for routine
surveillance after femoral-popliteal or femoral-tibial-pedal bypass with a venous conduit.minimum surveillance intervals areapproximately 3,6, and 12 months, and thenyearly after graft placement.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Treatment with an HMG coenzyme-A reductase inhibitor(statin) medication is indicated for all patients withperipheral arterial disease to achieve a target LDLcholesterol of less than 100 mg/dl.
Antihypertensive therapy should be administered tohypertensive patients with lower extremity PAD to a goalof less than 140/90 mmHg (non-diabetics) or less than
130/80 mm/Hg (diabetics and individuals with chronicrenal disease) to reduce the risk of myocardial infarction,stroke, congestive heart failure, and cardiovasculardeath.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Antiplatelet therapy is indicated to reduce the risk ofmyocardial infarction, stroke, or vascular death inindividuals with atherosclerotic lower extremity PAD.
Aspirin, in daily doses of 75 to 325 mg, is recommended
as safe and effective antiplatelet therapy to reduce therisk of myocardial infarction, stroke, or vascular death inindividuals with atherosclerotic lower extremity PAD.
Clopidogrel (75 mg per day) is recommended as an
effective alternative antiplatelet therapy to aspirin toreduce the risk of myocardial infarction, stroke, orvascular death in individuals with atherosclerotic lowerextremity PAD.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
A program of supervised exercise training isrecommended as an initial treatmentmodality for patients with intermittent
claudication.
Supervised exercise training should beperformed for a minimum of 30 to 45minutes, in sessions performed at leastthree times per week for a minimum of 12weeks.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
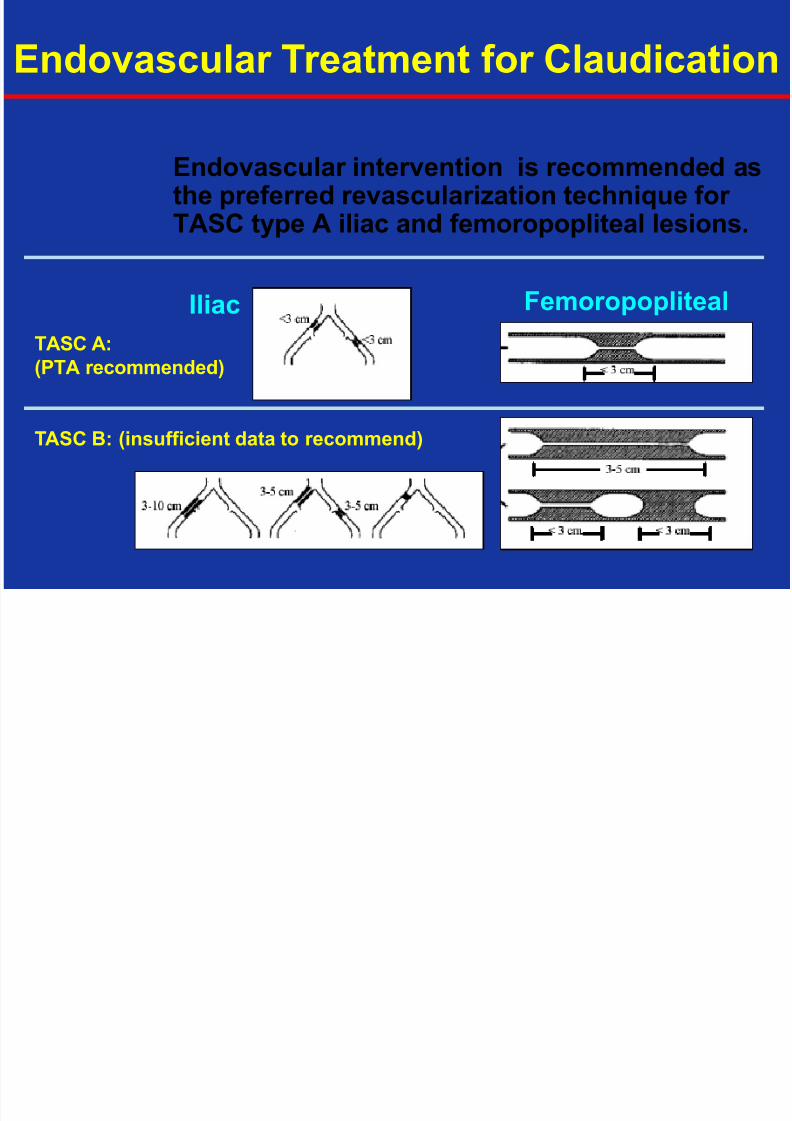
Endovascular procedures are indicated forindividuals with a vocational or lifestyle-limiting disability due to intermittentclaudication when clinical features
suggest a reasonable likelihood ofsymptomatic improvement withendovascular intervention an d …
a. Response to exercise or pharmacologictherapy is inadequate, and/or
b. there is a very favorable risk-benefit ratio(e.g. focal aortoiliac occlusive disease)
Endovascular Treatment for Claudication
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Provisional stent placement is indicated foruse in iliac arteries as salvage therapy forsuboptimal or failed result from balloondilation (e.g. persistent gradient, residualdiameter stenosis >50%, or flow-limitingdissection).
Stenting is effective as primary therapy forcommon iliac artery stenosis andocclusions.
Stenting is effective as primary therapy inexternal iliac artery stenosis andocclusions.
Endovascular Treatment for Claudication:Il iac A rter ies
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Patients who have significant necrosis of theweight-bearing portions of the foot, anuncorrectable flexion contracture, paresis of theextremity, refractory ischemic rest pain, sepsis,or a very limited life expectancy due to co-morbid conditions should be evaluated forprimary amputation.
Surgery is not indicated in patients with severedecrements in limb perfusion in the absence ofclinical symptoms of critical limb ischemia.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Bypasses to the above-knee poplitealartery should be constructed with autogenoussaphenous vein when possible.
Bypasses to the below-knee popliteal arteryshould be constructed with autogenous veinwhen possible.
Prosthetic material can be used effectivelyfor bypasses to the below knee poplitealartery when no autogenous vein from ipsilateralor contralateral leg or arm is available.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad
Femoral-tibial artery bypasses should beconstructed with autogenous vein, includingipsilateral greater saphenous vein, or ifunavailable, other sources of vein from the legor arm.
Composite sequential femoropopliteal-tibialbypass, or bypass to an isolated poplitealarterial segment that has collateral outflow tothe foot, are acceptable methods ofrevascularization and should be consideredwhen no other form of bypass with adequateautogenous conduit is possible.
8/12/2019 Kuliah Vi Blok Hematologi 2009 Arterial Trombosis Pad