EHR IMPACT ON QUALITY PROCESS MEASURES AND POPULATION HEALTH IMPROVEMENTS. Kwame A. Kitson, MD VP of Quality Improvement Institute for Family Health 16 East 16 th St New York, NY 10003 kkitson@ institute2000.org 212-633-0815 www. institute2000.org. Cambridge, Massachussetts - PowerPoint PPT Presentation
Kwame A. Kitson, MD VP of Quality Improvement Institute for Family Health 16 East 16 th St New York, NY 10003 kkitson@ institute2000.org 212-633-0815 www. institute2000.org Cambridge, Massachussetts August 20, 2008 EHR IMPACT ON QUALITY PROCESS MEASURES AND POPULATION HEALTH IMPROVEMENTS
Transcript
Kwame A. Kitson, MD
VP of Quality Improvement
Institute for Family Health
16 East 16th St
New York, NY 10003
kkitson@ institute2000.org
212-633-0815
www. institute2000.orgCambridge, Massachussetts
August 20, 2008
EHR IMPACT ON QUALITY PROCESS
MEASURES AND
POPULATION HEALTH IMPROVEMENTS
IFH AT A GLANCEIFH AT A GLANCE
IFH AT A GLANCEIFH AT A GLANCE
• Geographic area – Manhattan, Bronx, New Paltz, Kingston, Ellenville, Hyde Park, Port Ewen.
• 15 Community Health Centers• 8 Care for The Homeless Primary Care Sites• One School Based Health Center• Two FP Residency Programs• Two Free Clinics for the Uninsured• Two Article 31 Mental Health Sites
IFH AT A GLANCEIFH AT A GLANCESidney Hillman Walton Urban Horizons
Parkchester Mount Hope Westchester
IFH AT A GLANCEIFH AT A GLANCENew Paltz Kingston
Hyde Park Ellenville
Staff and BudgetStaff and Budget• Over 600 staff members:
– family physicians
– family nurse practitioners
– psychiatrists
– social workers
– health educators
– nurses
– practice administrators
– administrative staff
• A budget of approximately 45 million dollars
Electronic Health RecordsElectronic Health Records
• State-of–the-art electronic health records and practice management system across all sites
• Patient-centered care
• MyChart/MyHealth
• Continuous quality improvement/research
OTHER HIT OTHER HIT COLLABORATIVE EFFORTSCOLLABORATIVE EFFORTS
• INVOLVEMENT WITH THREE REGIONAL RHIOS (NYCLIX, BRONX, MID-HUDSON)
• IMMUNIZATION REGISTRY INTERFACE
• LEAD REGISTRY INTERFACE
• VISITING NURSING SERVICE INTERFACE– OUTBOUND REFERRALS IN TESTING.
• RYAN WHITE REPORTING WITH OUTBOUND EMR DATA REPORTING
Research & IRBResearch & IRB
• Clinical and health services research supports our core mission to provide access to superior care for all
• Supports community-based participatory research
• The Institute’s Institutional Review Board (IRB) is a peer-review body responsible for safeguarding the rights of human subjects
Health Information TechnologyHealth Information TechnologyNational Recognition
• Health Information Management System Society – 2006 Physician’s IT Leadership Award
• Health Information Management System Society – 2007 Davies Public Health Award
• CDC Center of Excellence in Public Health Informatics with NYC DOHMH and Columbia University
• NYCDOHMH Syndromic Surveillance
Syndromic SurveillanceSyndromic Surveillance
• How does it work ?– NYCDOMH receives hundreds of thousands of bits of
non-patient identifying data from ER’s, Pharmacies on a nightly basis.
– Data includes temperature data, ICDM’s, CPT codes, chief complaints, pharmaceuticals.
– Data is power analyzed to determine epidemics earlier than would be possible from laboratoory isolates.
– IFH was the first and is still the only ambulatory care site to submit data for this program.
Syndromic SurveillanceSyndromic Surveillance
ELECTRONIC DECISION SUPPORTELECTRONIC DECISION SUPPORT
• What influenced us to aggressively implement Electronic Decision Support Alerts ?- Need for making the most of the artificial
intelligence inherent in the EHR.- Avoid having a “glorified” paper record.- Effective real-time monitoring available via
crystal reporting.
ELECTRONIC DECISION SUPPORTELECTRONIC DECISION SUPPORT
• What were the risks involved with aggressive implementation of Electronic Decision Support Alerts ?
– No previous trailblazer organizations that had done this.– Risk of provider alert fatigue – “too many alerts.” – Multiple journal articles dismissing the idea that
electronic alerts could improve performance.– Risk of providers not reaching optimal levels in other
aspects of EHR documentation.
ELECTRONIC DECISION SUPPORTELECTRONIC DECISION SUPPORT
• What were the factors that led to our aggressive implementation of Electronic Decision Support Alerts ?
– Unanimous buy-in by senior leadership. – Groundwork for cooperation was laid by many years of close
involvement by site medical directors in the CQI process and clinical policy guidelines development.
– Relatively small size of our organization and also the single specialty make-up contributed to being able to quickly make strategic decisions.
– Analysis of Pre-EHR QI Studies revealed that interventions that worked the best were those that facilitated documentation by providers
IFH BEST PRACTICE ALERTSIFH BEST PRACTICE ALERTS
PRIMARILY BASED ON HEDIS CRITERIA
PNEUMOVAX
SEASONAL FLUVAX
BREAST CANCER SCREENING
CERVICAL CANCER SCREENING
LEAD SCREENING
HGBA1C TESTING AND CONTROL
IFH BEST PRACTICE ALERTSIFH BEST PRACTICE ALERTS
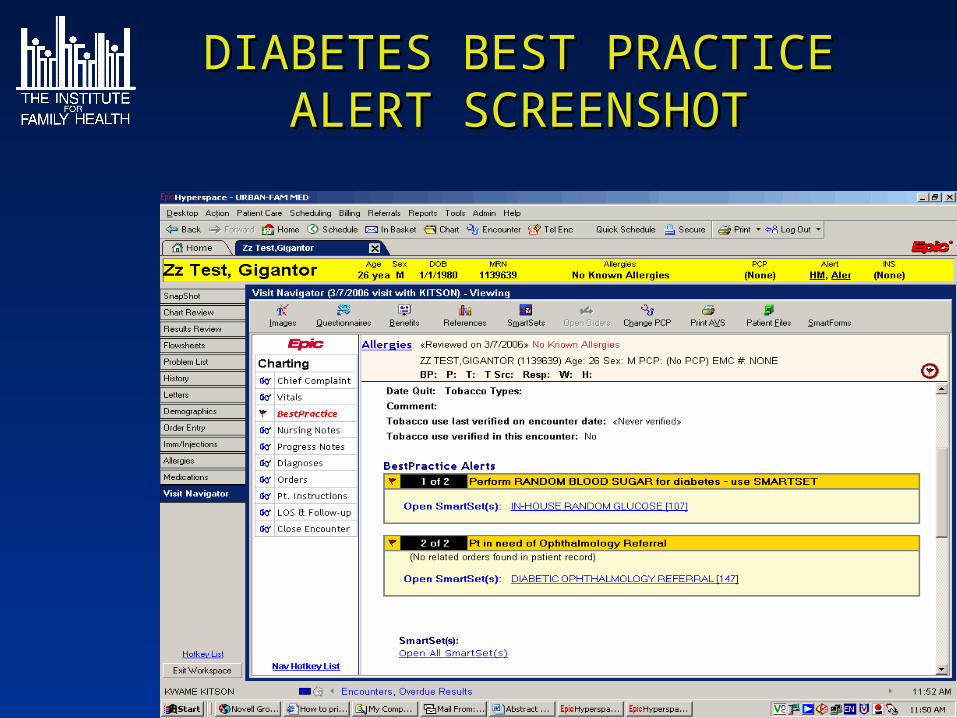
OPHTHALMOLOGY CONSULTS FOR DIABETICS
PEAK FLOW MEASUREMENTS FOR ALL ASTHMATICS
NEPHROLOGY CONSULTS FOR PATIENTS WITH GREATER THAN 1.8 SERUM CREATININE
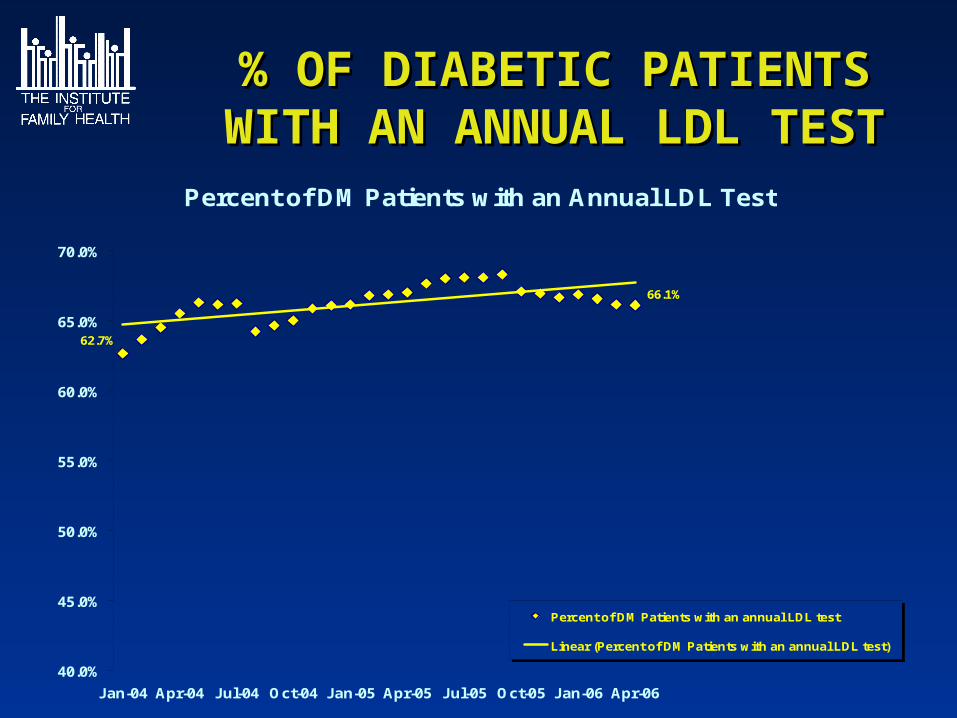
LDL SCREENING
ANNUAL RPR SCREENING IN HIV
DID THEY WORK ?DID THEY WORK ?
Initial concern about the introduction of best practice alerts (BPA’s) replaced by enthusiasm for the improvement seen in multiple clinical areas once initial reports showed improvement.
Keys to Success- Making sure that the BPA’s were accurate in capturing services rendered (e.g. There are dozens of CPT codes utilized for Cervical Cancer screening)
PROVIDER ACCEPTANCE OF PROVIDER ACCEPTANCE OF ELECTRONIC DECISION ELECTRONIC DECISION
SUPPORTSUPPORT
• MORE LIKELY TO ACCEPT ALERTS THAT ARE SIMPLE, LINKED TO EVIDENCE BASED GUIDELINES AND LINK DIRECTLY TO ORDER SETS.
• BREAST CANCER SCREENING, CERVICAL CANCER SCREENING AND COLON CANCER SCREENING ARE THE BPA’S CONSIDERED MOST HELPFUL AT IFH.
PNEUMOVAXPNEUMOVAXPNEUMOVAX GIVEN PER AGE GROUP VISIT
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
BPA INSTALLED 10/2003
LEAD TESTING LEAD TESTING IN TWO YEAR OLDSIN TWO YEAR OLDS
65%79% 82%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
2003 2004 2005
% COMPLIANCE WITH LEAD TESTING
% COMPLIANCEWITH LEADTESTING
37%43%
74%
99%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
April 2003 - July 2004 April 2004 - July 2005 April 2005 - July 2006 April 2006 - July 2007
PPD Screening of HIV PatientsUrban Horizons 15 Month Reports
BPA installed February 2006
N= 183N= 186N= 142N= 140
COLORECTAL CANCER SCREENINGCOLORECTAL CANCER SCREENING
Colorectal Screening IFH Sites 2005 to 2008
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
EAST 13TH ST. FAMILY HLTH CTR
MT. HOPE FAMILY HEALTH CENTER
PARKCHESTER FAMILY HLTH CTR
PHILLIPS FAMILY PRACTICE
SIDNEY HILLMAN FAMILY HLTH CTR
URBAN HORIZONS FAMILY HLTH CTR
WALTON FAMILY HEALTH CTR
BPA FOR COLORECTAL SCREENING INITIATED JAN 2008
All sites listed were fully on the EHR as of Jan 2003
Depression Screening CQIDepression Screening CQI
• Electronic Decision Support• Electronic Best Practice Alerts targeted to intake
nursing personnel to administer initial depression screening utilizing PHQ-2 screening tool. Initial site targeted Was Parkchester (PKFP) in May 2005.
• Positive PHQ-2’s lead to patients filling out PHQ-9’s and then going over the results with their providers.
• PHQ-2 administration is captured via reporting.• PHQ-9 results are loaded into the EHR as
laboratory type results and are then captured via reporting
ResultsResults
• There was a statistically significant increase (p<0.0001, Chi2 = 273.6) in Depression Screening Rate at our initial target site, Parkchester from 22% to 79% within one year.
• All adult patients at Parkchester are currently being screened at a 90% rate.
PARKCHESTER DEPRESSION SCREENING RATE
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PARKCHESTER
NURSING
PERSONNEL SHORTAGE
NURSING SHORTAGE RESOLVED
STEPPED UP VIGILANCE TO BPA ADHERENCE
DEPRESSION SCREENING RATES AT IFH
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
DEPRESSIONSCREENING RATEFOR NON PKFP IFHSITES
DEPRESSIONSCREENING RATEFOR PKFP
ResultsResults
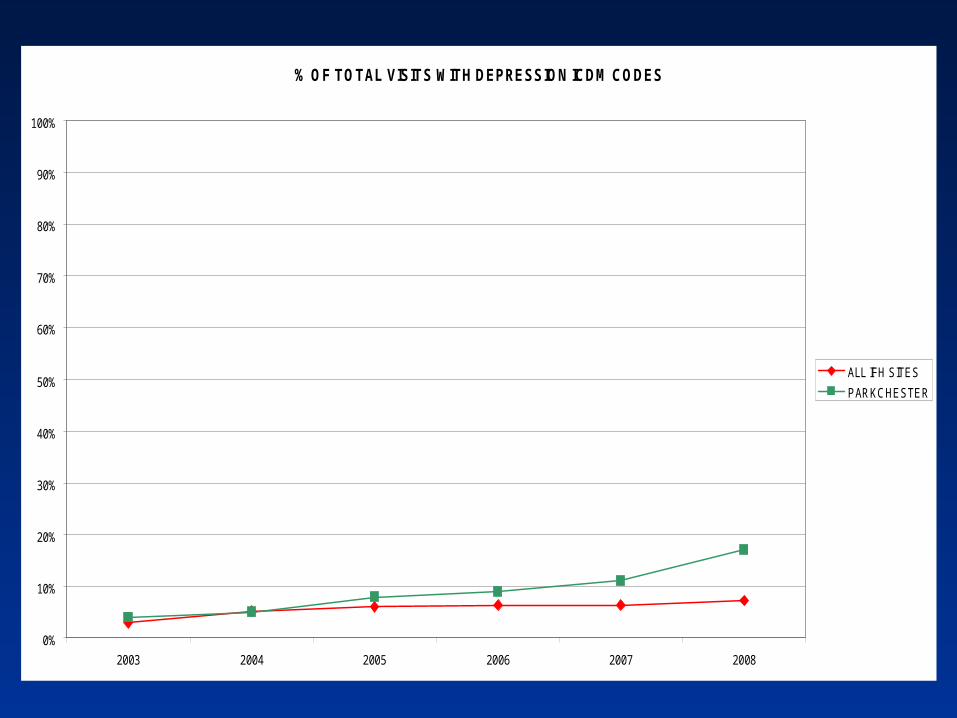
• Increases in screening rates have also led to increases in the number of visits coded for depression at Parkchester.
• There was a statistically significant increase in the % of total visits for adults 19 and over where an ICDM code for depression was used from 4% in 2003 to 17% in the first four months of 2008. (p<0.001).
PARKCHESTER % TOTALS VISITS FOR DEPRESSION
4% 5%
17%
11%9%8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2003 2004 2005 2006 2007 2008
PARKCHESTER% TOTALSVISITS FOR DEPRESSION
% OF TOTAL VISITS WITH DEPRESSION ICDM CODES
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2003 2004 2005 2006 2007 2008
ALL IFH SITES
PARKCHESTER
ResultsResults
• Increased resources for handling patients with depression came through adding on-site social work therapy and psychiatry support.
0
200
400
600
800
1000
1200
1400
2003 2004 2005 2006 2007 2008 PROJ
PARKCHESTER ANNUAL VISITS FOR DEPRESSION
SOCIAL WORKER
PRIMARY CARE PROVIDER
PSYCHIATRIST
ResultsResults
• Increased % of adult (19 and above) PKFP visits involved the ordering of antidepressants.
• Among primary care providers, a statisitcally significant increase from 1.4% to 2.0% has been noted from 2003 to 2007 at PKFP. (P value = 0.002)
• 3.9% of PKFP visits between January and April 2008 involved the ordering of antidepressants.
% OF PARKCHESTER VISITS WHERE AN ANTIDEPRESSANT WAS ORDERED
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
% PCP AND PSYCHVISITS WHERE ANANTIDEPRESSANTWAS ORDERED
% PCP VISITSWHERE ANANTIDEPRESSANTWAS ORDERED
ResultsResults
• Rate of completing full PHQ-9’S at the same visit after a positive PHQ 2 has been identified has improved from 78% in 2003 to 89% in 2008, but is not at the 100% target goal yet.
PARKCHESTER Rate of patients with phq9 done after a positive phq2
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Rate of patients with phq 9 done after a positive phq2
ResultsResults
• The % of patients who went through Depression reassessment and who ended up having PHQ Depression scores < 10 has not changed measurably since 2005.
• An attempt to start Phase II spread amongst all other sites in January 2008 did not fair well. Additional administrative and nursing re-orientation was needed. All sites as of July 1, 2008 are now engaged in phase II spread.
Next StepsNext Steps
• Ensure Phase II Spread is successful via a coordinated administrative and clinical effort.
• Improved 3 month Positive PHQ-9 Reassessment Rate is needed via social work outreach. Low rate of reassessment is linked to timely follow-up.
• Further analysis needed of patients whose PHQ-9 scores fail to improve. Medication Management vs. Access to and Utilization of Mental Health Care.
• More detailed reporting needed to track depression outcomes
DIABETIC ROLLING 12 MONTH DIABETIC ROLLING 12 MONTH AVERAGE REPORTSAVERAGE REPORTS
• Telephonic and Mail Outreach are done to 20,000 plus patients per year.
TYPES OF OUTREACH
• Targeted outreach based on internal reporting data.• Outreach based on mid-year QARR eligible reports• Outreach to patients assigned to our practices that
have never accessed care.• Outreach to patients who are no-shows for their
Major new grant funded CQI outreach effort in 2008 will involve utilizing risk scores for various types of cancer and targeting cancer screening outreach on a risk adjusted basis.
LAST_VISIT_DATE AGE AGE_SCORE LAST_TOBAC tobacco score BMI