62
La gestione dei Parkinsonismi nell’Anziano Fulvio Lauretani, MD Unità Operativa di Geriatria e Laboratorio di Prevenzione della Disabilità Azienda Ospedaliero-Universitaria di Parma

La gestione dei Parkinsonismi
nell’Anziano
Fulvio Lauretani, MD
Unità Operativa di Geriatria e
Laboratorio di Prevenzione della Disabilità
Azienda Ospedaliero-Universitaria di Parma

Età (anni)
Incid
en
za / 100 0
00
Marttila, R. et al. Eur. J. Neurol. 3, 187, 1996
Incidenza della Malattia di Parkinson

Prevalence of parkinsonian signs and associated mortality
in a community population of older people
Follow-up (years)
Pro
ba
bil
ity o
f S
urv
iva
l No Parkinsonism
Parkinsonism
0 8
1
0
Bennett DA, et al. N Engl J Med 1996;334:71-6

I Segni Neurologici Minori ed il
Rischio di Caduta nell’Anziano
Neurological examination findings to
predict limitations in mobility and falls
in older persons without a history of
neurological disease
Ferrucci L, Bandinelli S, Cavazzini C, Lauretani
F, Corsi A, Bartali B, Cherubini A, Launer L,
Guralnik JM
Am J Med 2004; 116: 807-15

La diagnosi di Parkinsonismo,
può essere fatta al letto del malato
(secondo i Criteri della British Brain Bank)
Step 1
Bradicinesia
Più almeno uno tra i seguenti criteri:
Rigidità plastica
Tremore a riposo
Instabilità posturale
Definizione di Bradicinesia nell’anziano:
- Prova Prono-Supinazione: < 20 prove in venti secondi
- Prova “Finger Tapping”: < 30 prove in venti secondi
Jankovic J, JNNP 2008;79:368-376
Ferrucci L, Bandinelli S, Cavazzini C, Lauretani F et al., AJM 2004; 116: 807-815

Braak’s Stage 1-2
Aspecific non-motor
symptoms:
-Hyposmia
-Costipation
-Depression
-Articular pain
-Fatigue
-Orthostatic Hypotension
Specific motor
symptoms:
-Bradikinesia
(plus at least):
-Rigidity
-Tremor
-Postural Instability
Aspecific non-motor
symptoms, specific in the
geriatric setting
-Memory Impairment
-Sleep Disorder
-Acute Delirium
-Nocturia
-Dysphagia with pneumonia
Frail “in situ”: mean 3-6 years Frail: mean 10 years Disability: mean 7 years
2 yr > 1 yr
Premotor Phase
Braak’s Stage 3-4 Braak’s Stage 5-6
Clinically Evident (PD) With Complications (PD-D)
Diagnosis
Lauretani F, et al. Arch Gerontol Geriatr 2012 ;54: 242-6

Pre-frail elderly:
Sub-clinical phase
Frail:
Clinically evident with
specific motor symptoms
Disable:
Clinically complex:
motor and non-motor symptoms
Pathologically Clinically Geriatric point of view
Braak’s stage Symptoms Transitional phases
1-2 • Premotor • Pre-frail
3-4 • Motor • Frail
5-6 • With Cognitive decline • Disable
Il ruolo del Geriatra:
deve rendere possibile
Lauretani F et al. J Am Geriatr Soc 2010; 58: 982-4


Logopedista
Fisiatra
Dietista
Psichiatra
Neurologo Neurologo
Geriatra
Dietista
Fisiatra
Logopedista
Approccio interdisciplinare per la gestione della Malattia di Parkinson in base all’età di insorgenza
Giovani Anziani
Regista
Scenografo

Es. Arena di Verona “a nudo”
Es. Trasformazione dell’Arena di Verona
dall’Arte Scenografica

Commentary
Fulvio Lauretani, Nigerian Medical Journal 2013 (in press)
Parkinson’s disease (PD) in the Elderly and the Comprehensive Geriatric Assessment (CGA)
• This is as the geriatricians "endoscopy" or "angiography" that provides an underlying aetiology of functional ill-health and overall plan of management, especially in these patients. • PD appear a typical neurological disease where the CGA could be applied for targeting approach with advantages not only for improving walking ability and mobility limitation, but also for reducing complications such as pneumonia dysphagia-related, deep vein thromboembolism and delirium.

Lees A. The bare essentials: Parkinson's disease. Pract Neurol 2010;10:240-6
Terapia: Tipi e dosaggio dei farmaci antiparkinson
( Stalevo )

Glass PG, Lees AJ, et al. J Neurol Neurosurg Psychiatry 2012; 83: 1027-9

Domanda:
E’ realmente l’età anagrafica il
fattore principale
per orientare la terapia con Levodopa o
Dopaminoagonisti
nell’Anziano Parkinsoniano?

Cosa condiziona la gestione dei sintomi motori della
Malattia di Parkinson nell’età avanzata?
SINTOMI
MOTORI
SINTOMI
COGNITIVI
e
PSICOTICI
Il bilanciamento tra i sintomi motori e quelli cognitivi del paziente

via
nigro-striatale
Dopamina e sintomi motori e sintomi psicotici
a. Sistema Nigrostriatale:
controlla i movimenti (ove sono presenti i
recettori dopaminergici D1 e D2)
b. Sistema Mesolimbico e della
Corteccia pre-frontale:
coinvolto nei sintomi
psicotici (es. deliri, allucinazioni)
(ove sono presenti i
recettori dopaminergici D3 e D4)

Maetzler W, Liepelt I, Berg D. Lancet Neurol 2009; 8:1158-71
Progression of cognitive decline in Parkinson’s disease

Hilker, R. et al. Neurology 2005;65:1716-1722
Regions with significantly decreased cortical MP4A binding vs controls in the Parkinson
disease (first row) and the Parkinson disease with dementia group (second row)
Acetilcolina e riduzione delle funzioni cognitive:
= aree cerebrali deficitarie di acetilcolina
Cholinesterase inhibitors for dementia with Lewy bodies,
Parkinson's disease dementia and cognitive impairment
in Parkinson's disease.
Conclusions:
The currently available evidence supports the use of cholinesterase
inhibitors in patients with Parkinson’s disease-Dementia (PDD),
with a positive impact on global assessment, cognitive function,
behavioural disturbance and activities of daily living rating scales.
The effect in DLB remains unclear. There is no current
disaggregated evidence to support their use in CIND-PD.
Rolinski M, Fox C, et al. Cochrane Database Syst Rev. 2012; 3: CD006504

Rivastigmina e Cadute nella M. di Parkinson ?
Conclusions: Unlike nigrostriatal dopaminergic denervation, cholinergic
hypofunction is associated with fall status in Parkinson disease (PD).
Thalamic AChE activity in part represents cholinergic output of the
pedunculopontine nucleus (PPN), a key node for gait control. Our results are
consistent with other data indicating that PPN degeneration is a major factor leading to impaired postural control and gait dysfunction in PD.
Bohnen NI, et al. NEUROLOGY 2009;73:1670-1676
Cadute Deficit
Dopaminergico ?
Deficit
Colinergico ?

Dopamina
Confusione mentale nell’anziano parkinsoniano e bilanciamento tra dopamina ed acetilcolina
Lauretani F, Maggio M, et al. Chapter 7 – Treatment of Parkinson’s Disease and Parkinsonism in the elderly (pp.165-178) Authors / Editors: Chiyo Yoshida and Ami Ito; Pub. Date: 2012
Acetilcolina
Somministrazione
continua
Somministrazione
pulsatile

Olanow CW, Obeso JA, Stocchi F. (2006) Drug Insight: continuous dopaminergic stimulation in the
treatment of Parkinson's disease. Nat Clin Pract Neurol 2: 382–392
Effect of intraintestinal levodopa infusion on motor
complications in Parkinson's disease

Domanda:
E’ possibile ipotizzare che la somministrazione
di farmaci che permettono una stimolazione
dopaminergica continua produca un minor
rischio di sviluppare complicanze
neuropsichiatriche così come accade per quelle
motorie?
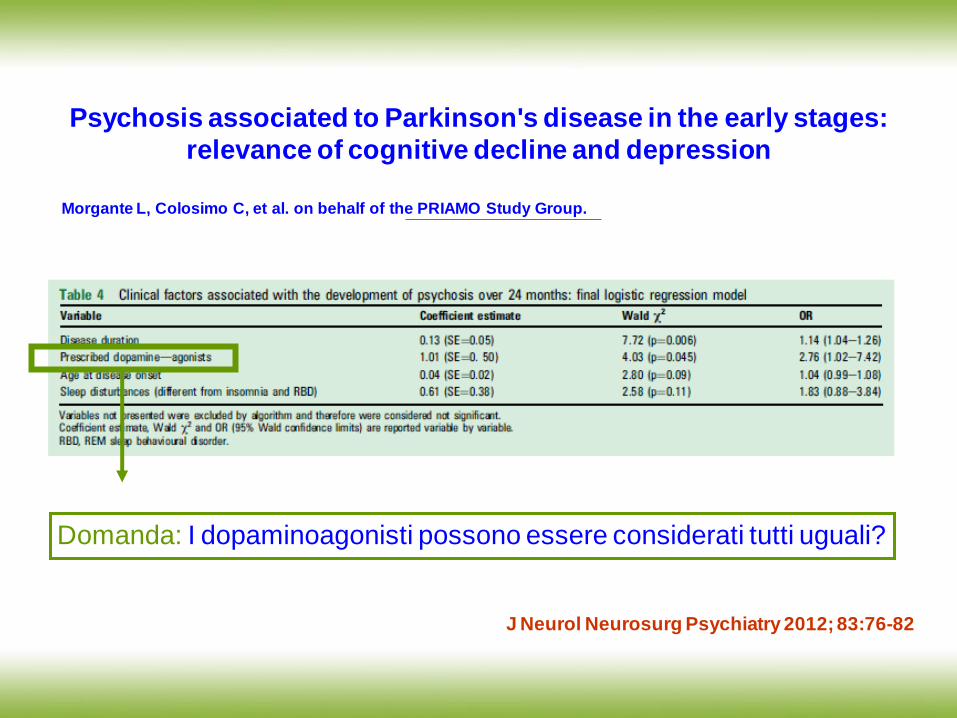
Psychosis associated to Parkinson's disease in the early stages:
relevance of cognitive decline and depression
Morgante L, Colosimo C, et al. on behalf of the PRIAMO Study Group.
Domanda: I dopaminoagonisti possono essere considerati tutti uguali?
J Neurol Neurosurg Psychiatry 2012; 83:76-82

Olanow, C. W. et al. Neurology 2009;72:S1-S136
The scientific and clinical basis for the treatment of Parkinson disease

CLEOPATRA-PD STUDY
Lancet Neurol 2007; 6: 513-20


Fasano A, Guidubaldi A, De Nigris F, Bentivoglio AR. J Am Geriatr Soc 2011; 59:2386-7
Safety and efficacy of rotigotine in individuals with Parkinson's disease aged 75 and older

CONFRONTO TRA ROTIGOTINA E
LEVODOPA NELL’ANZIANO CON
MALATTIA DI PARKINSON
Fulvio Lauretani, Gian Paolo Ceda,
Augusto Scaglioni, Anna Nardelli
Marcello Maggio
UO Geriatria, Azienda Ospedaliero-
Universitaria di Parma
Clinica Geriatrica, Università di Parma
UO Neurologia, Ospedale di Vaio,
ASL di Parma

Neuropsychiatric safety of continuous dopaminergic therapy versus standard levodopa in older parkinsonian patients:
a pilot randomized study
Results: 60 consecutive newly diagnosed drug-naïve PD patients (mean age = 80.5 ± 9.2
years; mean MMSE: 25.8 ± 3.0) were evaluated. 30 patients were treated with rotigotine (6 mg/daily) and 30 patients were treated with levodopa (250 mg/daily). UPDRS part III was significantly lower in both groups after treatment (from 26.4 to 18.3 (rotigotine group) and from 26.3 to 17.3 (levodopa group), but comparable between groups. Acute delirium and/ or psychosis were observed in two cases (5%) of patients treated with rotigotine and in three cases (10 %) of those treated with levodopa (difference evaluated by ANOVA showed no significance between groups, p=NS), after 6 months of follow-up.
Fulvio Lauretani, Gian Paolo Ceda, et al. 2012 (submitted)

Le conclusioni dello studio pilota sono state:
• I Dopaminoagonisti che producono una
stimolazione dopaminergica continua possono
essere utilizzati con sicurezza nell’anziano con
Parkinson
• Se questi risultati saranno confermati da studi
con adeguato sample size, potranno essere
riviste anche le linee guida per il trattamento
della malattia di Parkinson nell’anziano

La Gestione dei Sintomi Psicotici nella Malattia di Parkinson
SINTOMI
non
MOTORI
- depressione, apatia, ansietà
- deficit dell’attenzione - demenza - confusione
- delirio - allucinazioni
COGNITIVI e
NEUROPSICHIATRICI
Chaudhuri et al.
Curr Neurol Neurosci Rep 2005;5:275-83

Risk of Mortality Among Individual Antipsychotics in Patients With Dementia
Helen C. Kales, M.D.; Am J Psychiatry 2012;169:71-79

Seeman P, Tallerico T. Am J Psychiatry. 1999;156: 876-84
Antipsicotici ed effetti extrapiramidalici

La Gestione della Complicanze Internistiche nella Malattia di Parkinson
SINTOMI
non
MOTORI
- es. MALATTIA
TROMBOEMBOLICA
- es. DISFAGIA e POLMONITE
DA INALAZIONE
COMPLICANZE
INTERNISTICHE
Chaudhuri et al.
Curr Neurol Neurosci Rep 2005;5:275-83

Lauretani F, Maggio M, Giordano A, Ceda GP, Nardelli A. Aging 2013 (in press)
• We performed an observational study on patients, aged 65 and older, who were admitted
to the Geriatric Unit of University Hospital of Parma
• 66 in the year 2010 and 58 patients in the year 2011 were admitted with diagnosis of
Parkinsonism (6.0% of the total amount of patients admitted to our Hospital)
• All these patients presented a H&Y stage of 4 or 5. Mean age + SD of the patients was
80 + 12 years
• 20.9% were affected by VTE
• None of these patients were on low molecular weight heparin or other treatments aimed
to preventing VTE
TVP e Parkinsonismi nell’Anziano

Lauretani F, Maggio M, Giordano A, Nardelli A, Ceda GP. Aging 2012 (submitted)
• We performed an observational study on patients, aged 65 and older, who were admitted
to the Geriatric Unit of University Hospital of Parma.
• 6.0% of the total amount of patients admitted to our Hospital were affected of
parkinsonism
• Nearly 80% of patients showed respiratory failure, and almost all of these patients
presented dysphagia
• None of patient’s caregivers were informed on the presence of dysphagia
Disfagia e Parkinsonismi nell’Anziano

Il Giudizio Universale by
Michelangelo

Necessità di creare la Scuola in Geriatria per la cura dell’anziano con Parkinson
La Scuola di Atene by Raffaello

Ringraziamenti:
Prof. Gian Paolo Ceda
Prof. Marcello Maggio
Dr.ssa Anna Nardelli
Dott.ssa Livia Ruffini
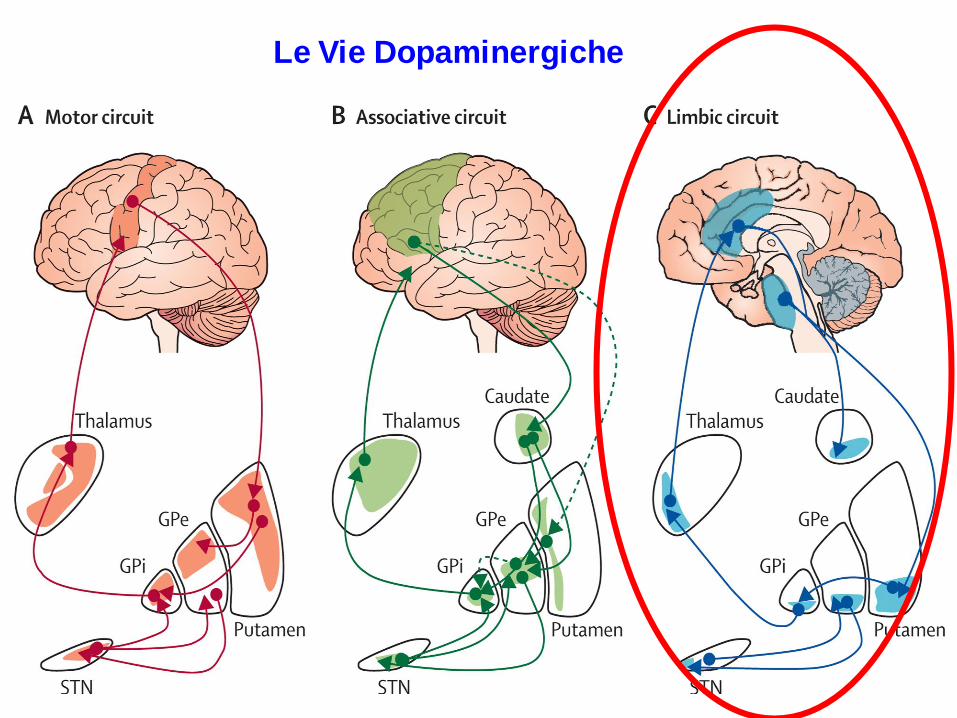
Le Vie Dopaminergiche

J Neurol Neurosurg Psychiatry 2012; 83: 1155-1161

L-DOPA Dopamine Agonists
-Punding -DDS*
-Gambling -Pathological Shopping
-Hypersexuality -Overeating
Disadvantages:
Psychosis Hallucinatios
Confusion Compulsivity
Disadvantages:
Psychosis Hallucinatios
ICDs**
* DDS=Dopamine Disregulation Syndrome
** ICDs= Impulse Control Disorders Lauretani F, Maggio M, et al. Chapter 7 – Treatment of Parkinson’s Disease and Parkinsonism in the
elderly (pp.165-178) Authors / Editors: Chiyo Yoshida and Ami Ito Pub. Date: 2012

The Sydney multicenter study of Parkinson's disease: The inevitability of
dementia at 20 years
Hely MA et al. Mov Disord 2008; 23: 837-44.

Dopaminergic deficits Dysexecutive syndrome
Cholinergic deficits Impairment of memory
Noradrenergic deficits Impairment of attention
Serotoninergic deficits Depressive symptoms
Le funzioni dei neurotrasmettitori nella Malattia di Parkinson
Calabresi P, Picconi B, Parnetti L, Di Filippo M. Lancet Neurol 2006; 5:974-83

IMPATTO DELL’INTRODUZIONE DELLA SPECT CEREBRALE CON DatSCAN™ PER
LA DIAGNOSI DIFFERENZIALE DEI PARKINSONISMI E SULLA LORO
GESTIONE CLINICA NEL PAZIENTE ANZIANO
TESI DI:
Chiara Guareschi
RELATORE:
Prof. Marcello Maggio
TUTORE:
Dott. Fulvio Lauretani
IMPATTO DELL’INTRODUZIONE DELLA SPECT
CEREBRALE CON DatSCAN™ SULLA DIAGNOSI DIFFERENZIALE DEI PARKINSONISMI E SULLA
LORO GESTIONE CLINICA NEL PAZIENTE ANZIANO
Lauretani F, et al. EJN (submitted)

DAT-SPECT
Qualitative Analysis Quantitative Analysis
Male: 88 years

SPECT CON [₁₂₃I]-FP-CIT
NORMALE
PATOLOGICO

ANALISI SEMIQUANTITATIVA
NORMALE
PATOLOGICO
Basal Ganglia v.2

OBIETTIVI DELLO STUDIO
• Valutare il ruolo della SPECT con [123I]-FP-CIT nella diagnosi di Parkinsonismo nei soggetti anziani
• Identificare i fattori associati ad un ridotto up-take di [123I]- FP-CIT
• Proporre un nuovo algoritmo diagnostico nell’uso della SPECT nei soggetti anziani con Parkinsonismo indefinito

MATERIALI E METODI
• Tutti i soggetti di età superiore a 65 anni con diagnosi di Parkinsonismo che hanno eseguito un esame SPECT tra Gennaio 2009 e Maggio 2012
• Sono state prese in considerazione più informazioni:
SESSO ED ETÀ DEI PAZIENTI
MOTIVAZIONE DELLA RICHIESTA DELLA SPECT
SEGNI E SINTOMI CLINICI CHE ERANO PRESENTI AL MOMENTO DELL’ESAME
STATO NEUROPSICOLOGICO DEL SOGGETTO
EVENTUALE ASSUNZIONE DI FARMACI ANTIDOPAMINERGICI
PRESENZA DI REPERTI TAC e\o RMN
TEMPO TRASCORSO TRA LA RICHIESTA DELLA SPECT E L’ESORDIO DEI SINTOMI

CARATTERISTICHE GENERALI DELLA POPOLAZIONE IN STUDIO (267 pazienti)
Media ± DS
Età (anni) 73 ± 5.08
Tempo intercorso tra l’esecuzione della SPECT e la comparsa dei sintomi (mesi) 29.52 ± 41.72
N° pz (%)
Sesso (maschi) 147 (55.06%)
SPECT CON DAT:
- Esame normale 78 (30.08%)
- Compromissione monolaterale del sist. nigro-striatale 59 (23.03%)
- Compromissione bilaterale del sist. nigro-striatale 116 (45.08%)
SEGNI EXTRA-PIRAMIDALI RIPORTATI:
- Bradicinesia 103 (38.06%)
- Tremore a riposo 127 (47.57%)
- Rigidità plastica 29 (10.08%)
- Criteri della British Brain Bank rispettati 65 (24.03%)
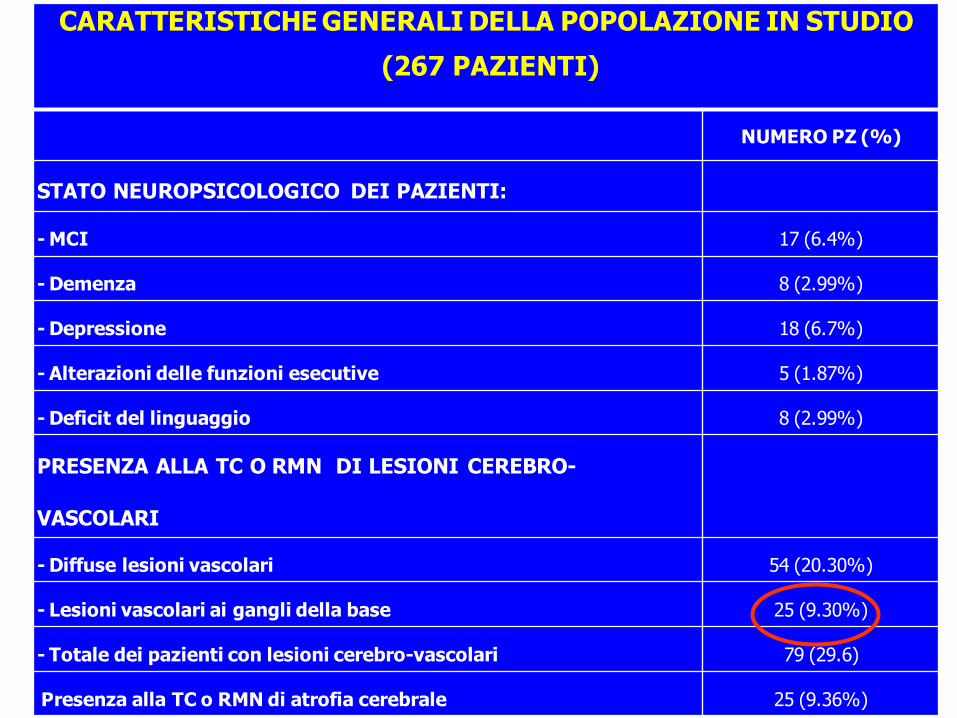
CARATTERISTICHE GENERALI DELLA POPOLAZIONE IN STUDIO
(267 PAZIENTI)
NUMERO PZ (%)
STATO NEUROPSICOLOGICO DEI PAZIENTI:
- MCI 17 (6.4%)
- Demenza 8 (2.99%)
- Depressione 18 (6.7%)
- Alterazioni delle funzioni esecutive 5 (1.87%)
- Deficit del linguaggio 8 (2.99%)
PRESENZA ALLA TC O RMN DI LESIONI CEREBRO-
VASCOLARI
- Diffuse lesioni vascolari 54 (20.30%)
- Lesioni vascolari ai gangli della base 25 (9.30%)
- Totale dei pazienti con lesioni cerebro-vascolari 79 (29.6)
Presenza alla TC o RMN di atrofia cerebrale 25 (9.36%)

Caratteristiche della popolazione in studio stratificate
secondo il risultato dell’esame SPECT
SPECT
NORMALE
(N,%)
SPECT
PATOLOGICA
(N,%)
P P aggiustata
per età e sesso
Sindrome
Extrapiramidale Aspecifica
60 (41.0%) 86 (58.9%) 0.10 0.15
Criteri della British
Brain Bank 12 (18.5%) 53 (81.5%) 0.001 0.003
Bradicinesia 24 (23.3%) 79 (76.7%) 0.002 0.004
Tremore a riposo 49 (38.6%) 78 (61.4%) 0.17 0.14
Rigidità Plastica 5 (17.2%) 24 (82.8%) 0.003 0.004

Analisi di regressione multipla per testare l'associazione dei segni che meglio si correlano con
SPECT patologica
Beta SE P
Bradicinesia 0.17 0.05 0.003
Lesioni cerebro-vascolari a TC o RM 0.19 0.06 0.002
Età -0.01 0.005 0.02
Sesso -0.095 0.056 0.09

E.S.
not specified Atypical
Parkinsonism
Re-evaluation
Iatrogenic
Parkinsonism
LDB
E. S. with
specified symptoms
Motivation for prescription of SPECT with DATscan
0
20
40
60
80
100
Perc
en
tag
e (%
)
Abnormal
DAT scan
Normal
DAT scan

ALGORITMO DIAGNOSTICO
Sospetto Tremore
Essenziale
TRIAL CON
L-DOPA
ASSENZA DI RISPOSTA
ALLA L-DOPA
Dovrebbe essere considerata la
diagnosi di Tremore EssenzialeB
RISPOSTA CRONICA
ALLA L-DOPA
Dovrebbe essere presa in
considerazione la diagnosi di MP

ALGORITMO DIAGNOSTICO
Dopo 3 mesi dalla sospensione dei farmaci
Entro un mese dall’esordio
DEMENZA A CORPI DI
LEWY
SPECT
PATOLOGICA
Può essere confermata una diagnosi di
Demenza a corpi di Lewy
NORMALE
Bisognerebbe considerare i criteri per la malattia di Alzheimer

ALGORITMO DIAGNOSTICO

CONCLUSIONI
• Utilizzare questo studio come traccia al fine di individuare un algoritmo diagnostico condiviso su tutto il territorio
• Migliorare la comunicazione tra il clinico e i
medici di Medicina Nucleare, ad esempio riportando sulla richiesta dell’esame SPECT dati come:
Presenza di sintomi tipici del parkinsonismo Presenza di disturbi cognitivi
Utilizzo di farmaci anti-dopaminergici

The orexin neurons promote wakefulness and modulate reward pathways
Thomas E Scammell & Clifford B Saper. Nature Medicine 13, 126 - 128 (2007)


















