19
LAB #5 – LOWER EXTREMITY Range of Motion Case Study #2 Tyler Hyvarinen (0308368) Kelly Heikkila (0305975) Allison Pruys (0310660)
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | kasey-halbrooks |
| View: | 213 times |
| Download: | 0 times |
LAB #5 – LOWER EXTREMITYRange of Motion Case Study #2
Tyler Hyvarinen (0308368)
Kelly Heikkila (0305975)
Allison Pruys (0310660)
CASE STUDY 28 year old student Complete tear of ACL, MCL & Lateral Meniscus Healthy and active and has completed 3 weeks of
treatment Has partial flexion and is partially weight bearing with
use of crutches The meniscus tear has partially healed and MCL is still
weak and needs strengthening
GOAL: Develop full range of motion and establish weight
bearing function

Functional Assessment Exercises
Stair assessmentChair exercise

Functional Assessment – Test #1
Procedure: The patient will ascend and descend a set
of stairs (minimum of three steps)
Normal Range: Note that normal Range of Motion for the
knee is from 0° of extension to 135° of flexion.
The maximum knee flexion needed for this movement is between 83° and 105° to ascend and 86° to 107° to descend the stairs.
Contraindications & Substitution/Trick Movements:
Although there are movements occurring at the ankle and hip joints, the knee joint undergoes the largest range.
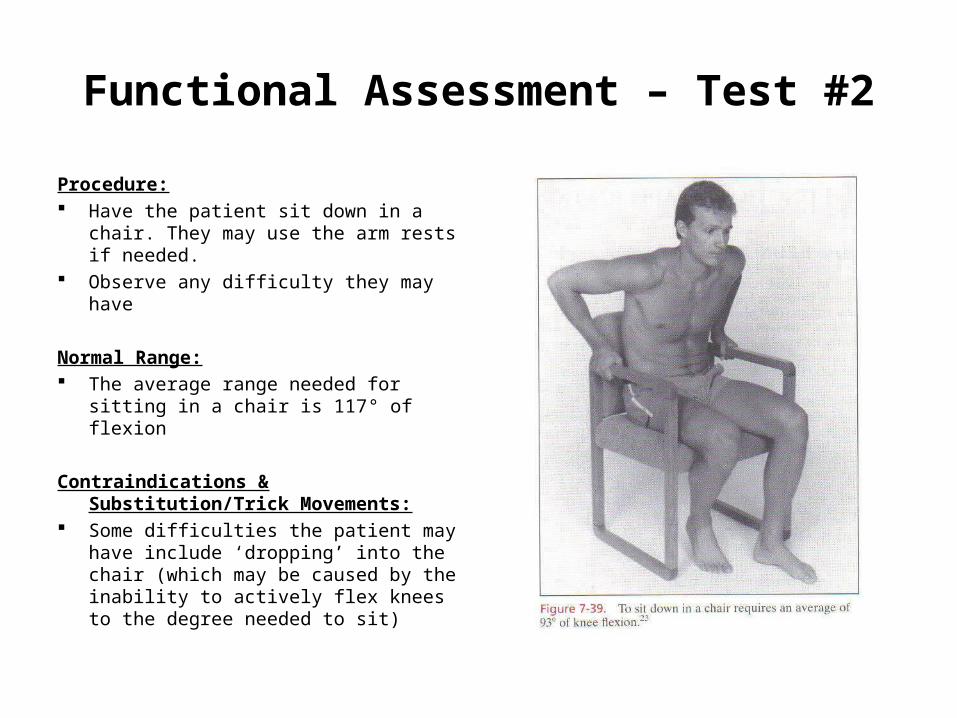
Functional Assessment – Test #2
Procedure: Have the patient sit down in a chair.
They may use the arm rests if needed. Observe any difficulty they may have
Normal Range: The average range needed for sitting
in a chair is 117° of flexion
Contraindications & Substitution/Trick Movements:
Some difficulties the patient may have include ‘dropping’ into the chair (which may be caused by the inability to actively flex knees to the degree needed to sit)

Active Range of Motion Assessments (AROM)
Knee flexionKnee extension

AROM Assessment – Knee FlexionProcedure: The patient is lying in a prone position with a pillow under the abdomen. The
knee is in extension, the tibia is in a neutral position and the foot is over the end of the table.
A pelvic strap is applied to stabilize the hips around the gluteal muscles and the therapist stabilizes the thigh with his/her hand over the distal hamstrings
The patient flexes his/her knee through full range of motion. AROM is visually assessed or measured using a universal goniometer.
Contraindications & Substitution/Trick Movements: The rectus femoris may limit the range of knee flexion in the prone position Substitution movements may occur at the sartorius (producing hip flexion
and external rotation) and the gracilis (producing hip abduction)
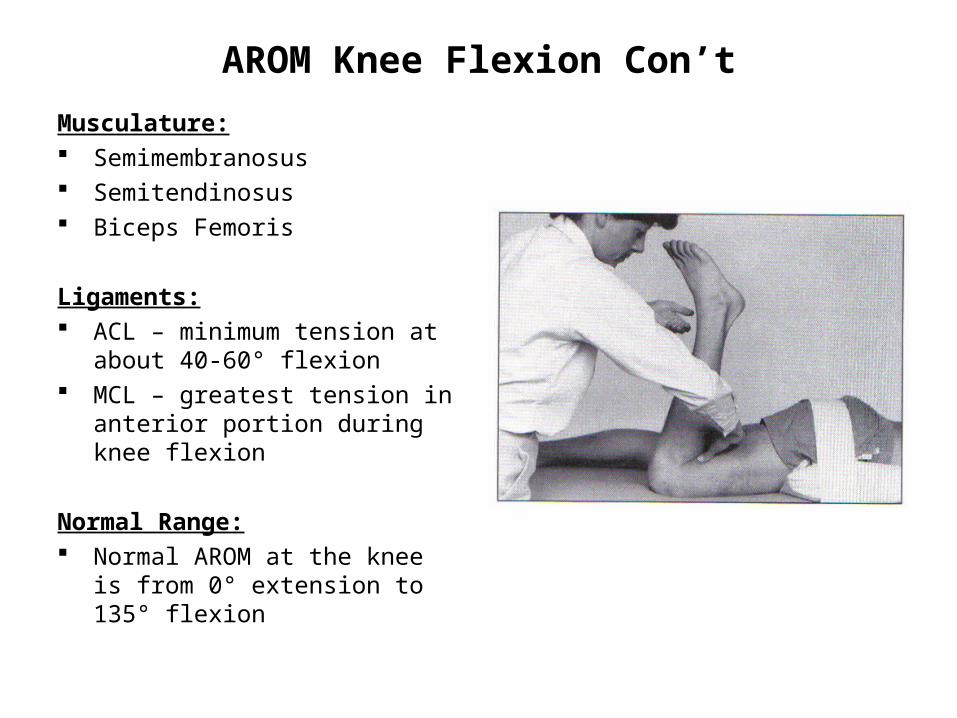
AROM Knee Flexion Con’t
Musculature: Semimembranosus Semitendinosus Biceps Femoris
Ligaments: ACL – minimum tension at about
40-60° flexion MCL – greatest tension in anterior
portion during knee flexion
Normal Range: Normal AROM at the knee is from
0° extension to 135° flexion
AROM Assessment – Knee ExtensionProcedure: Patient is instructed to sit on a table, with legs suspended, grasping the
edge of the table for support. The non-test foot should be supported on a stool.
The therapist explains, demonstrates or passively moves the limb though knee extension then instructs the patient to straighten the knee as far as possible.
The patient is instructed to maintain the thigh in the start position or the therapist may stabilize the thigh with his/her hand.
The patient performs knee extension. The knee is extended as far as possible through the range of motion. AROM is visually assessed or measured with a universal goniometer.
Contraindications & Substitution/Trick Movements: Tight hamstrings may restrict knee extension in this position. As a trick/substitution movement, the patient may lean back to posteriorly tilt
the pelvis and extend the hip joint.
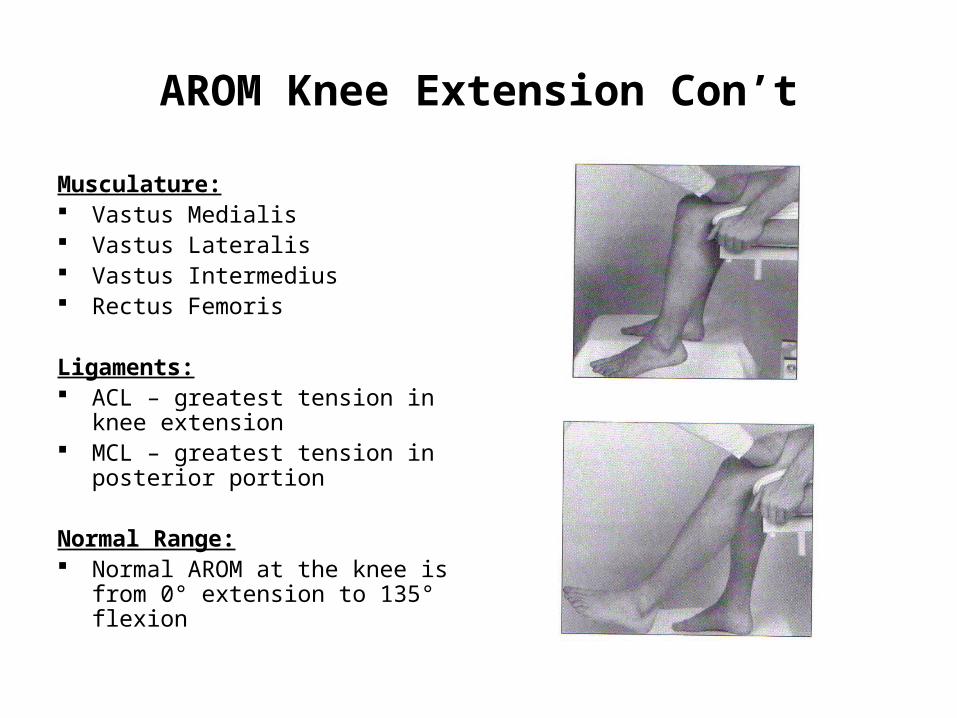
AROM Knee Extension Con’t
Musculature: Vastus Medialis Vastus Lateralis Vastus Intermedius Rectus Femoris
Ligaments: ACL – greatest tension in knee
extension MCL – greatest tension in
posterior portion
Normal Range: Normal AROM at the knee is from
0° extension to 135° flexion
Passive Range of Motion Assessments (PROM)
Knee flexion/extensionMeasurement of muscle length (rectus femoris)Tibial rotationKnee flexion
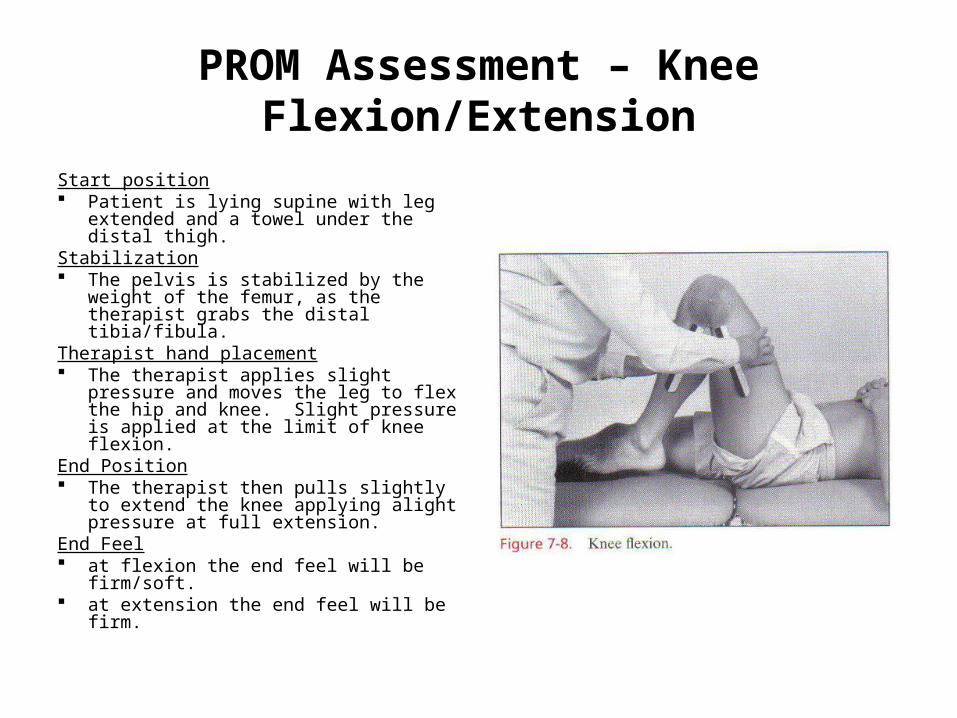
PROM Assessment – Knee Flexion/Extension
Start position Patient is lying supine with leg
extended and a towel under the distal thigh.
Stabilization The pelvis is stabilized by the weight of
the femur, as the therapist grabs the distal tibia/fibula.
Therapist hand placement The therapist applies slight pressure
and moves the leg to flex the hip and knee. Slight pressure is applied at the limit of knee flexion.
End Position The therapist then pulls slightly to
extend the knee applying alight pressure at full extension.
End Feel at flexion the end feel will be firm/soft. at extension the end feel will be firm.

PROM Knee Flexion/Extension Con’t
Measurement: The axis of the goniometer is
placed over the lateral epicondyle of the femur
The stationary arm is placed parallel to the longitudinal axis of the femur, pointing toward the greater trochanter
The moveable arm is placed parallel to the longitudinal axis of the fibula, pointing toward the lateral malleolus
Measurements are taken at point of maximum flexion and at point of maximal hyperextension (0-10 degrees)

PROM Assessment – Measurement Of Muscle Length (Rectus Femoris)
Start Position: The patient is prone. A towel is placed under the thigh to eliminate pressure
on the patella. The leg is in the anatomical position with the knee in extension (0°)
Stabilization: The therapist stabilizes the femur End Position: The lower leg is moved in a posterior direction so that the heel
approximates the buttock to the limit of knee flexion. Passive insufficiency of rectus femoris may restrict the range of knee flexion when the patient is prone
End Feel: Rectus femoris on stretch – firm end feelSubstitution/Trick Movement: The patient anteriorly tilts the pelvis and flexes the hip to place the rectus
femoris on slack and thus allow increased knee flexion.
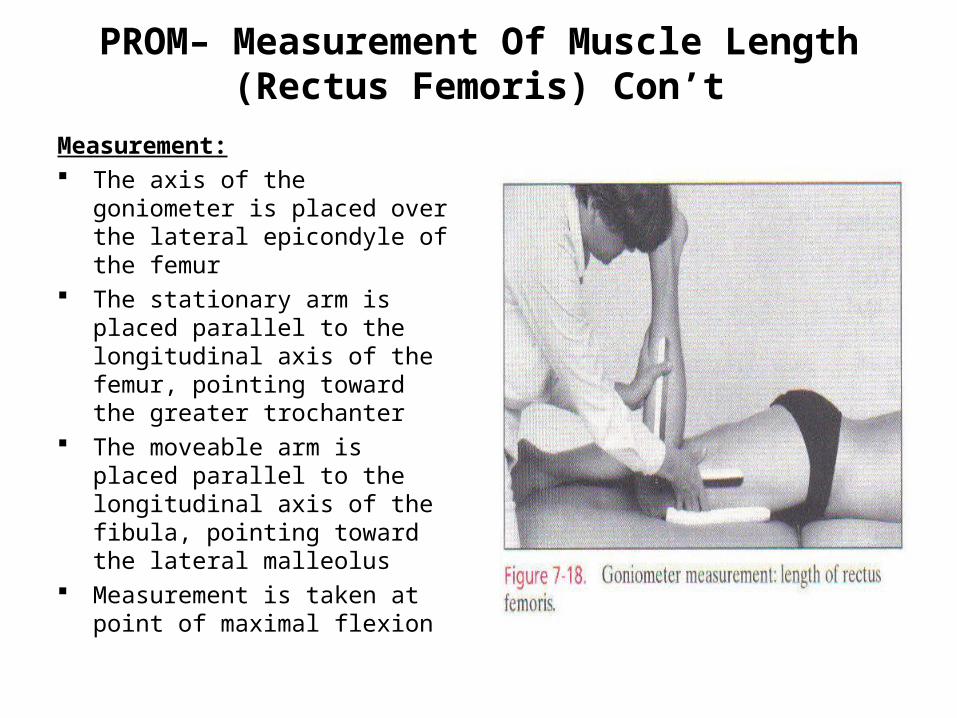
PROM– Measurement Of Muscle Length (Rectus Femoris) Con’t
Measurement: The axis of the goniometer is
placed over the lateral epicondyle of the femur
The stationary arm is placed parallel to the longitudinal axis of the femur, pointing toward the greater trochanter
The moveable arm is placed parallel to the longitudinal axis of the fibula, pointing toward the lateral malleolus
Measurement is taken at point of maximal flexion
PROM Assessment – Tibial Rotation
Start Position: The patient is sitting with the knee 90° flexion, hanging over the side of the
table. A towel is placed under the distal thigh to maintain the thigh in a horizontal position.
Stabilization: The therapist stabilizes the femur
End Position: The tibia starts in full internal rotation and is then rotated by the therapist to
the full available range for external rotation. The total range is the tibia is recorded as excessive, normal or restricted (average is 58°).
End Feel: Internal rotation and external rotation – firm.
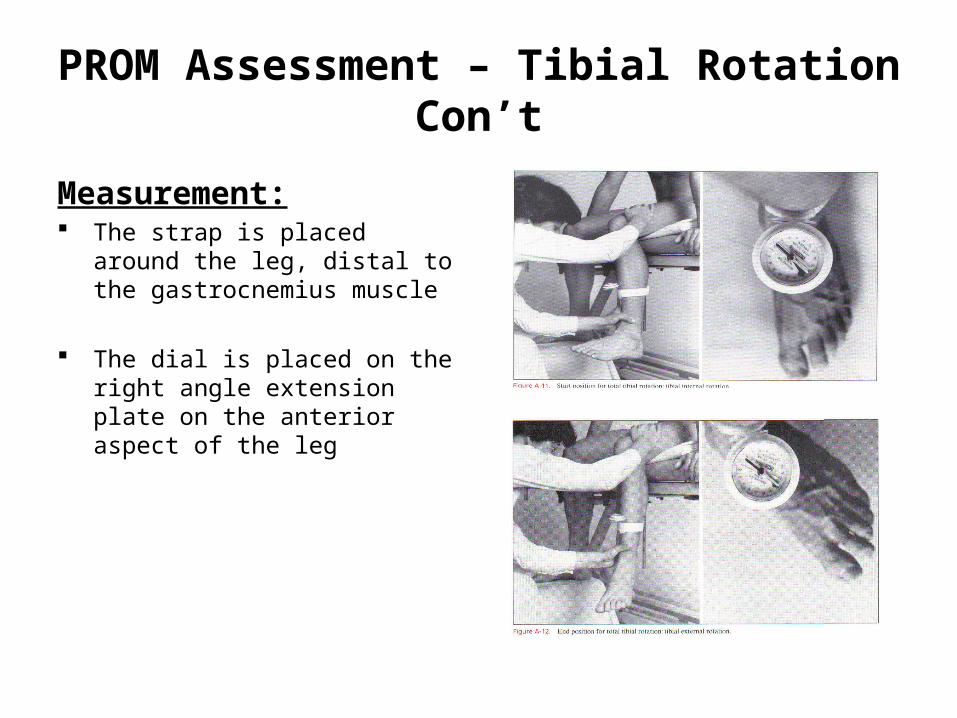
PROM Assessment – Tibial Rotation Con’t
Measurement: The strap is placed around the leg,
distal to the gastrocnemius muscle
The dial is placed on the right angle extension plate on the anterior aspect of the leg

PROM (against gravity) – Knee Flexion
Start position Patient is lying in the prone position with a pillow under the abdomen. The knee is in extension with the tibia in the neutral position, and the foot is
over the end of the table.
Stabilization A strap is placed around the pelvis, the therapist stabilizes the thigh.
Movement The patient flexes the knee through the full rang of motion.
Trick Movements Sartorius – Producing hip flexion and external rotation. Gracilis – Producing hip adduction.
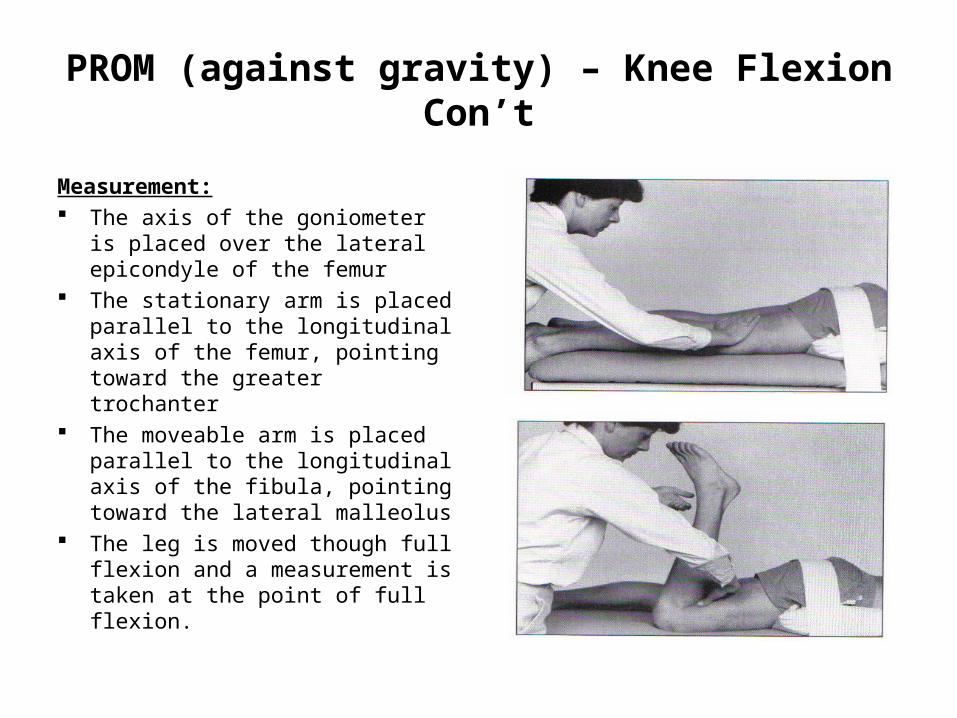
PROM (against gravity) – Knee Flexion Con’t
Measurement: The axis of the goniometer is
placed over the lateral epicondyle of the femur
The stationary arm is placed parallel to the longitudinal axis of the femur, pointing toward the greater trochanter
The moveable arm is placed parallel to the longitudinal axis of the fibula, pointing toward the lateral malleolus
The leg is moved though full flexion and a measurement is taken at the point of full flexion.

















