56
Labour Labour Prof. Mustafa Gawass Prof. Mustafa Gawass FRCOG FRCOG , , FRCPI FRCPI
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | jack-heath |
| View: | 214 times |
| Download: | 0 times |
Labour Labour
Prof. Mustafa Gawass Prof. Mustafa Gawass FRCOGFRCOG, , FRCPIFRCPI
objectivesobjectives
Define labour.Define labour.
Understand the components of labour Understand the components of labour (passage, passenger, power).(passage, passenger, power).
Be able to take a focused history, Be able to take a focused history, examination and anlyse the symptoms and examination and anlyse the symptoms and signs to diagnose labour.signs to diagnose labour.
Describe the stage sand phases of labour.Describe the stage sand phases of labour.
Discuss the mechanism of labour.Discuss the mechanism of labour.
Discuss the management of labour.Discuss the management of labour.

Labour (parturition)Labour (parturition)
It Is the process where by with time regular It Is the process where by with time regular uterine contractions, brings about progressive uterine contractions, brings about progressive affacment and dilatation of the cervix, resulting affacment and dilatation of the cervix, resulting in delivery of the fetus from the uterus and in delivery of the fetus from the uterus and expulsion of the placenta at or beyond 24 (or expulsion of the placenta at or beyond 24 (or 28) completed weeks of pregnancy. 28) completed weeks of pregnancy.
It is a social, psycological and economical event It is a social, psycological and economical event for the couple, family and community.for the couple, family and community.
Cervical dilatationCervical dilatation: The cervix begins : The cervix begins dilating and stretching beyond the normal dilating and stretching beyond the normal dimensions and is measured in dimensions and is measured in centimeters. (0-10cm).centimeters. (0-10cm).
Cervical effacementCervical effacement: softening, : softening, thinning and shortening of the cervix. It is thinning and shortening of the cervix. It is expressed in percentage (0 – 100%)expressed in percentage (0 – 100%)
A 20 year old primigravida comes to maternity unit at A 20 year old primigravida comes to maternity unit at 39 weeks gestation complaining of regular uterine 39 weeks gestation complaining of regular uterine contractions, 3-4/10min. For the past 6 hours. The contractions, 3-4/10min. For the past 6 hours. The contractions are becoming more frequent lasting 45-contractions are becoming more frequent lasting 45-50 sec. she denies any vaginal fluid leakage. The 50 sec. she denies any vaginal fluid leakage. The blood pressure, pulse and temperature are normal. blood pressure, pulse and temperature are normal.
Vaginal examination cephalic, head at s-1,90% Vaginal examination cephalic, head at s-1,90% affaced, 5 cm dilated, soft and anterior. FH=133bpm .affaced, 5 cm dilated, soft and anterior. FH=133bpm .
What is your diagnoses?What is your diagnoses?

1 LNMP 24 W 28 W 37 W 40W 42W
PTL
Term Labour
Labour can occur at:Labour can occur at:
prolongedprolonged
Normal labour:Normal labour:
Spontaneous expulsion, through the Spontaneous expulsion, through the natural passages (birth canal) of a single, natural passages (birth canal) of a single, mature (37-42 completed weeks of mature (37-42 completed weeks of pregnancy) Alive fetus, presenting by pregnancy) Alive fetus, presenting by vertex, within a reasonable time, without vertex, within a reasonable time, without fetal or maternal complications.fetal or maternal complications.

Components of labour:Components of labour:

types of female pelvistypes of female pelvis

passengerspassengers
The following will pass during labour The following will pass during labour (fetus, cord, placenta and membranes). (fetus, cord, placenta and membranes). The most important to pass is the head The most important to pass is the head and shoulder and shoulder

Moulding of the skull:Moulding of the skull:
means obliteration of the suture line between means obliteration of the suture line between the bones and overlapping of the un-united the bones and overlapping of the un-united bones of the fetal skull, and is measured by bones of the fetal skull, and is measured by degree.degree.
Degree Clinical finding
+++
+++
Suture line closed, no overlap Overlap of suture line reducible Overlap of suture line irreducible
As the degree of moulding increase- means there is CPD
Fetal attitudeFetal attitude:: is the relation of the fetal parts is the relation of the fetal parts to each other to each other
1- flexion attitude (common) 1- flexion attitude (common)
2- extension attitude (rare).2- extension attitude (rare).

Clinical course of labourClinical course of labourOnset of labour:Onset of labour: not definitely known – however there not definitely known – however there
are several theories, but none of them is are several theories, but none of them is completely proven. completely proven.
Mechanical theoriesMechanical theories:: - uterine distension - uterine distensionHormonal theories:Hormonal theories: 1.1. Maternal : Maternal : o progesterone withdrawalprogesterone withdrawalo oxytocin stimulationoxytocin stimulationo prostaglandinsprostaglandinso serotoninserotonin2.2. fetal:fetal:o fetal cortisolfetal cortisolo fetal membranes fetal membranes 3.3. Neuronal factors:Neuronal factors:o sympathetic- alpha receptor stimulationsympathetic- alpha receptor stimulation
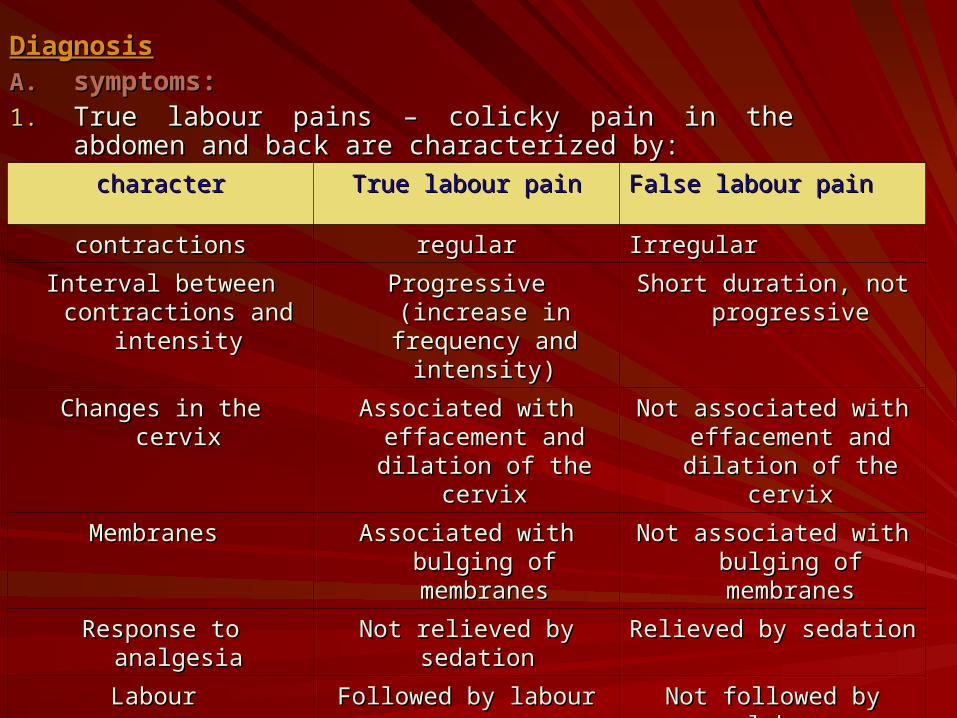
DiagnosisDiagnosisA.A. symptoms:symptoms:1.1. True labour pains – colicky pain in the abdomen and back True labour pains – colicky pain in the abdomen and back
are characterized byare characterized by::
charactercharacter True labour painTrue labour pain False labour painFalse labour pain
contractionscontractions regularregular IrregularIrregular
Interval between Interval between contractions and contractions and
intensityintensity
Progressive (increase Progressive (increase in frequency and in frequency and
intensity)intensity)
Short duration, not Short duration, not progressiveprogressive
Changes in the cervixChanges in the cervix Associated with Associated with effacement and effacement and
dilation of the cervixdilation of the cervix
Not associated with Not associated with effacement and effacement and
dilation of the cervixdilation of the cervix
Membranes Membranes Associated with bulging Associated with bulging of membranesof membranes
Not associated with Not associated with bulging of bulging of
membranesmembranes
Response to analgesiaResponse to analgesia Not relieved by Not relieved by sedation sedation
Relieved by sedationRelieved by sedation
Labour Labour Followed by labourFollowed by labour Not followed by labourNot followed by labour

2.2. Show – blood stained mucous.Show – blood stained mucous.
3.3. SROMSROM
B.B. Signs:Signs:o palpable or recorded uterine contractionpalpable or recorded uterine contractiono effacement and dilation of the cervixeffacement and dilation of the cervixo formation of forewater formation of forewater
STAGES OF LABOUR:STAGES OF LABOUR: I-The First stageI-The First stage:: stage of cervical stage of cervical effacement and dilatationeffacement and dilatationDefinitionDefinition:: the first stage of labour refers to the first stage of labour refers to the period from the onset of true uterine the period from the onset of true uterine contractions to the fully dilation of the cervix, contractions to the fully dilation of the cervix, when the diameter of the cervical os when the diameter of the cervical os measures 10cmmeasures 10cm..
THE ACTIVE STAGE OF LABOUR – WHEN THE CERVIX THE ACTIVE STAGE OF LABOUR – WHEN THE CERVIX IS MORE THAN 3 CM DILATED AND FULLY EFFACEDIS MORE THAN 3 CM DILATED AND FULLY EFFACED

Duration:Duration:o primigravida = 8-12 hprimigravida = 8-12 ho multigravida = 6-8 hmultigravida = 6-8 h
Phases of the first stage:Phases of the first stage: Latent phase: started when the cervix dilatated Latent phase: started when the cervix dilatated
slowly and reached to about 3cm.slowly and reached to about 3cm.A.A. in primigravida = 8hin primigravida = 8hB.B. in multigravida = 4hin multigravida = 4h - Active phase: rapid dilatation of the cervix to - Active phase: rapid dilatation of the cervix to
reach 10cm reach 10cm A.A. in primigravda = 4hin primigravda = 4hB.B. in multigravida =2h in multigravida =2h

The active phase is divided into:The active phase is divided into:1.1. Accelerative phaseAccelerative phase2.2. Slopping phaseSlopping phase3.3. Decelerative:Decelerative:A.A. prolonged active phase prolonged active phase B.B. primary dysfunction: dilation in active primary dysfunction: dilation in active
phase of<1cm/hrphase of<1cm/hrC.C. secondary arrest: active phase dilation secondary arrest: active phase dilation
stops or slow significantly. stops or slow significantly. N.B – in primigravida the cervix dilates from N.B – in primigravida the cervix dilates from
above downwards, in multigravida above downwards, in multigravida dilatation of the internal os, taking up of dilatation of the internal os, taking up of the cervix and dilatation of the external os the cervix and dilatation of the external os occurs simultaneouslyoccurs simultaneously..

Factors affecting cervical dilatation:Factors affecting cervical dilatation:
1.1. Contraction and retraction of the Contraction and retraction of the uterus.uterus.
2.2. The bag of fore-water.The bag of fore-water.
3.3. Absence of membranes.Absence of membranes.
4.4. Fitting of the presenting part to the Fitting of the presenting part to the lower segment and the cervix.lower segment and the cervix.
5.5. Pre-labour changes in the cervix Pre-labour changes in the cervix (eg, softening) (eg, softening)
II-The Second stage of labour:II-The Second stage of labour: stage of stage of delivery of the fetus.delivery of the fetus.Definition:Definition: the second stage of labour refers the second stage of labour refers to the period from complete cervical dilatation to the period from complete cervical dilatation to the birth of the fetus.29-30to the birth of the fetus.29-30Duration:Duration:A.A.in primigravida =1 hin primigravida =1 hB.B.in multigravida = ½ hin multigravida = ½ h however the timing of the second stage is however the timing of the second stage is very different to determine and controversial very different to determine and controversial and can be extended as much as there is and can be extended as much as there is progress in descent and no harm to the progress in descent and no harm to the mother or fetus mother or fetus

The second stage of labour had two The second stage of labour had two phases:phases:
1.1. Passive phase – stage of descent of Passive phase – stage of descent of the presenting part and dilatation of the presenting part and dilatation of the vagina – due to contraction and the vagina – due to contraction and retraction of the uterine muscle.retraction of the uterine muscle.
2.2. Expulsive phase – stage of bearing Expulsive phase – stage of bearing down – due to contraction and down – due to contraction and retraction of the uterine muscle and retraction of the uterine muscle and voluntary efforts by diaphragm and voluntary efforts by diaphragm and abdominal musclesabdominal muscles..

Mechanism of labour in vertex presentation: Definition: The spontaneous adjustments of the fetal position and attitude to affect efficient passage of the fetus through the pelvis, marked by progressive descent until delivery of the fetus.
Delivery of the fetal head:A- Descent: is a continuous movement throughout the process of delivery, however it becomes more rapid in the second stage of labour, it is caused by:o-Uterine contraction and retraction.o-bearing down effort – mainly in the second stage of labour

In normal pelvis, the fetal head enters with In normal pelvis, the fetal head enters with the sagittal suture in the transverse the sagittal suture in the transverse diameter (or occasionally oblique diameter diameter (or occasionally oblique diameter of the brim). If the sagittal suture in of the brim). If the sagittal suture in between the symphysis pubis and sacral between the symphysis pubis and sacral promontory – both parietal bones are felt promontory – both parietal bones are felt vaginally at the same level – the head is vaginally at the same level – the head is said to be (synclitic). In such case the said to be (synclitic). In such case the biparietal diameter (9.5cm) is the diameter biparietal diameter (9.5cm) is the diameter of engagement. However some degree of of engagement. However some degree of lateral inclination of the head over the lateral inclination of the head over the shoulder – (Asynclitism) is present shoulder – (Asynclitism) is present normally as the head enters the pelvic inletnormally as the head enters the pelvic inlet..
*If the sagittal suture lies close to the *If the sagittal suture lies close to the sacrum and the anterior patietal bone sacrum and the anterior patietal bone lies over the inlet (Anterior parietal lies over the inlet (Anterior parietal bone presentation) bone presentation) - Anterior - Anterior asynclitismasynclitism..
**If the sagittal suture lies close to the If the sagittal suture lies close to the symphysis pubis and the posterior symphysis pubis and the posterior parietal bone lies over the inlet parietal bone lies over the inlet (posterior parietal bone presentation) (posterior parietal bone presentation) – posterior asynclitism– posterior asynclitism..

Causes of non-engagement:Causes of non-engagement: Erroneous dates (primigravida)Erroneous dates (primigravida) Extra-uterine:Extra-uterine:A.A. full bladder or loaded rectumfull bladder or loaded rectumB.B. Pelvic tumoursPelvic tumoursC.C. Pendulous abdomen and marked lumbar lordosis.Pendulous abdomen and marked lumbar lordosis.D.D. High angle of inclination of the pelvis.High angle of inclination of the pelvis.E.E. Contracted pelvis.Contracted pelvis. -Uterine:-Uterine:A.A. Poor uterine tone.Poor uterine tone.B.B. Congenital deformities.Congenital deformities.C.C. Fibromyomata.Fibromyomata.D.D. Placenta previa. Placenta previa.

-Fetal:-Fetal:A.A. polyhydramnios.polyhydramnios.B.B. Short umbilical cord(acutal or relative, due Short umbilical cord(acutal or relative, due
to entanglement)to entanglement)C.C. Large baby.Large baby.D.D. Deflexion attitude, and malposition.Deflexion attitude, and malposition.E.E. Multiple pregnancy.Multiple pregnancy.F.F. Hydrocephalus.Hydrocephalus.Engagement – can be assessed by Engagement – can be assessed by
abdominal station in fifths during abdominal station in fifths during antenatal period, and by abdominal and antenatal period, and by abdominal and vaginal stations during labourvaginal stations during labour..

C.C.Increased flexionIncreased flexion:: as the head as the head descends, it meets resistance from the descends, it meets resistance from the pelvic walls and floor and this leads to pelvic walls and floor and this leads to increased flexion of the head. As the increased flexion of the head. As the head flexed it brings the shortest head flexed it brings the shortest longitudinal diameter of the head (sub-longitudinal diameter of the head (sub-occipito-bregmatic – 9.5cm) to pass occipito-bregmatic – 9.5cm) to pass through the birth canal. Flexion is through the birth canal. Flexion is explained by the (two armed lever explained by the (two armed lever theory). theory).

D-Internal rotationD-Internal rotation:: the internal rotation the internal rotation occurs as the head descends through the occurs as the head descends through the pelvic cavity. As the head enters the pelvic pelvic cavity. As the head enters the pelvic inlet in transverse diameter will rotate 3/8 of inlet in transverse diameter will rotate 3/8 of the cycle to pass through the pelvic outlet in the cycle to pass through the pelvic outlet in antero-posterior diameter.antero-posterior diameter.
The rotation is favoured by the slopping The rotation is favoured by the slopping shape of the pelvic floor, angling the leading shape of the pelvic floor, angling the leading point of the head (occiput) in downward and point of the head (occiput) in downward and forward direction, by the effect of the forward direction, by the effect of the contraction and retraction of the uteruscontraction and retraction of the uterus..
E-Crowning, extension and delivery of the fetal E-Crowning, extension and delivery of the fetal head:head:
The combined effect of descent and internal rotation The combined effect of descent and internal rotation bring the presenting diameter to the plane of the bring the presenting diameter to the plane of the pelvic outlet, with the occiput lying under the pubic pelvic outlet, with the occiput lying under the pubic arch and the sinciput at the lower border of the arch and the sinciput at the lower border of the sacrum or coccyx.sacrum or coccyx.
When the widest diameter of the fetal head is When the widest diameter of the fetal head is embraced by the distended vulva, it is said to be embraced by the distended vulva, it is said to be crowned.crowned.
The occiput remains under the pubic arch but the The occiput remains under the pubic arch but the sinciput sweeps forwards as the neck extendssinciput sweeps forwards as the neck extends..

The head is acted upon by:The head is acted upon by:1.1. The downward and forward force of the The downward and forward force of the
uterine contraction and retraction.uterine contraction and retraction.2.2. The upward and forward force offered by The upward and forward force offered by
pelvic floor resistance so the head passes pelvic floor resistance so the head passes forwards i.e. extends vertex, forehead, forwards i.e. extends vertex, forehead, and face come out successively.and face come out successively.
Frequently, especially in primigravida, the Frequently, especially in primigravida, the soft tissues are not able to distend equally soft tissues are not able to distend equally so that tearing of the perineum and so that tearing of the perineum and adjacent tissues may occur unless steps adjacent tissues may occur unless steps are taken to avoid it by making a formal are taken to avoid it by making a formal incision (episiotomy). incision (episiotomy).

F-Restitution and external rotation:F-Restitution and external rotation:
Following delivery of the head the occiput Following delivery of the head the occiput rotates to the lateral position, in the opposite rotates to the lateral position, in the opposite direction of internal rotation to correct the direction of internal rotation to correct the twist of the head on the shoulders produced twist of the head on the shoulders produced by internal rotation. The internal rotation of by internal rotation. The internal rotation of the shoulders inside the pelvis transmitted to the shoulders inside the pelvis transmitted to the delivered head which in turn move one the delivered head which in turn move one eight of a circle outside the pelvis, in the eight of a circle outside the pelvis, in the same direction as that of the restitution, so at same direction as that of the restitution, so at the end the occiput is towards one thigh and the end the occiput is towards one thigh and the face is towards the other thighthe face is towards the other thigh..

Delivery of the shoulder and body:Delivery of the shoulder and body:The widest diameter of the shoulders,( the bi-The widest diameter of the shoulders,( the bi-acromial diameter), pass the pelvic brim at acromial diameter), pass the pelvic brim at the time when the anterior rotation of the the time when the anterior rotation of the head is occurring. Thus the anterior rotation head is occurring. Thus the anterior rotation of the occiput is favourable for both the head of the occiput is favourable for both the head and the shoulders. Similarly external rotation and the shoulders. Similarly external rotation of the head is associated with rotation of the of the head is associated with rotation of the shoulders to bring them into the antero-shoulders to bring them into the antero-posterior diameter of the outlet. With further posterior diameter of the outlet. With further descent, the anterior shoulder delivered first descent, the anterior shoulder delivered first from under the pubic arch, followed by from under the pubic arch, followed by posterior shoulder, during which time lateral posterior shoulder, during which time lateral flexion of the trunk is occurring. The trunk flexion of the trunk is occurring. The trunk and buttocks follow with the same or the next and buttocks follow with the same or the next contractioncontraction..
Even in the course of normal delivery, Even in the course of normal delivery, there are many variations of the there are many variations of the mechanisms, dependent on the mechanisms, dependent on the variation in the size and shape of the variation in the size and shape of the pelvis and of the fetal head.pelvis and of the fetal head.
III-The Third stage of labourIII-The Third stage of labour:: the the stage of expulsion of the placenta and stage of expulsion of the placenta and membranesmembranes..

Duration: up to 30 minutes, however the average length of the third stage of labour is 10 minutes.
Mechanism: the third stage is made of two phases:
1.The first phase: phase of placental separation occurs through the spongiosa layer of the decidua at the time of expulsion of the baby or very soon afterwards. The shearing force responsible for the separation is the contraction and retraction of the uterus, reducing the uterine volume and the area of the placental site, as the fetus is expelled.

2.The second phase: phase of placental expulsion – The separated placenta descends from the upper (active) segment into lower (passive) uterine segment, cervix, and vagina by two mechanisms:
A.-Schultze mechanism:(80%)The placenta delivered as an inverted
umbrella with it’s fetal surface presenting first followed by the membranes with retro-placental haematoma.
B.Mattews – Duncan mechanism: (20%)The placenta delivered side way and it
presents with it’s inferior surface first.

Stage of labour
Definition Duration
Stage I latent phase(affacment)
•Begins from the onset of regular contractions.•Ends with acceleration of cervical dilatation•Prepares cervix for dilatation.
<20 hours in PG<14 hours MG
Stage 1 active phase(dilatation)
•Begins with acceleration of cervical dilatation.•Ends at 10 cm dilatation•Rapid cervical dilatation
<2/hours in PG<1.5/ hrs in MG
Stage 2(descent)
•Begins from 10cm dilatation•Ends with delivery of the baby•Descent of the fetus
<2 hours in PG<1 hours in MGAdd 1 hour in epi
Stage 3(expulsion)
•Begins with delivery of the baby.•Ends with delivery of the placenta•Delivery of the placenta
<30 min.
Management of labourThe management of labour should be commenced during the antenatal period, and the women should be classified as high or low risk pregnancy. The medical or surgical problems should be corrected as in case of (anaemia, hypertension, urinary tract infection), vaccination should be given if necessary, and all investigations should be performed and prepared such as (HIV, HCV, Hbs Ag, blood grouping…….etc).

Also the patient should be advised to attend the antenatal class (parenterful class) and visit the hospital including the labour ward to be familiar to the place and staff. Once labour is commenced and the patient arrived to the admission room the following to be done:

A. -Taking history or reviewing the antenatal file.
1-Last menstrual period – expected date of confinement.
2-Time of onset of labour. 3-Frequency and duration of contraction
(3-4cm/10min). 4-Presence or absence of amniotic fluid
leakage. 5-Presence or absence of show or
vaginal bleeding. 6-Past obstetric history especially mode
of previous delivery, presentation, mode of delivery, and weight of previous children.
7-Past medical or surgical history that may affect labour or delivery, especially diabetes, heart disease, respiratory disease allergies, and any medication.
B-Examination:1. .General: a-pallor, oedema, varicosities, height, and
built. b-Vital signs (BP, P, T) c-Examination of heart, lungs, breast and
other organs if necessary 2. .Abdominal Examination: a-To determine fundal height in cm using
tape measure (to determine gestational age clinically), fetal lie, presentation, engagement in fifths, size of the fetus, amount of liquor, fetal heart rate.
b-The frequency and duration of the contraction.

3. .Vaginal Examination: to assess the following.
a-Cervical dilatation in cm and effacement in %.
b-Length of the cervix.c-Consistency of the cervixd-Position of the cervixe-State of the membranes, amount and colour
of liquor.f-fetal presentation, position and station.g-pelvic architecture.

DO NOT DO VAGINAL EXAMINATION IN CASES OF VAGINAL BLEEDING BEFORE THE PLACENTA PREVIA IS EXCLUDED.
DO STERIL SPECULUM EXAMINATION IF SUSPECTED PLROM, IF THE WOMAN IS NOT IN LABOUR.
If the woman diagnosed as having active labour – to be admitted to labour ward.N.B- active labour means –regular strong and frequent uterine contraction 3-4/10min lasting 45-50 sec, and the cervix is fully effaced and 2.5-3cm dilated.

Arrival to the labour ward:
I-first stage of labour:1-Ensure patient’s privacy by covering her
with sheaths or blankets.2-Reassure and show great sympathy and
interest.3-Record maternal vital signs every hour (BP,
P, T).4-Take blood for grouping and cross match
for high risk patients.5-Monitor:a-high risk patients should have a continuous
electronic fetal heart monitoring.
b-low risk patients should have brief electronic fetal heart monitoring if NORMAL, to be followed by intermittent auscultation:
-first stage every 15min-second stage every 5min6-Limit oral intake to small amount of clear
fluid or frozen pineapple.7-Give all patients in active labour Ranitidine
(Zentac) 150mg orally / 6hourly.8-Nurse the patient in:a-left lateral position for mediated patients.b-sitting or semi-reclining for unmediated
patients.

9-Encourage spontaneous voiding, catheterization may be necessary.
10-Test all urine specimen for proteins, sugar, and acetone.
11-Give IV fluids during labour to avoid dehydration
a-0.9% Nacl or hartmann’s solution at 80-125ml/hr
b-Supplementation with 5% dextrose to prevent ketosis and hypoglycemia.
12-Give analgesia/anesthesia as required.a-Pethidine (50-150mg)IM.b-Diamorphin (5-10mg)IM. Every 3-4 hours.*avoid giving it too early in labour < 3-4cm
cervical dilation or too late when the delivery is expected within 1-2hours.

*if given too late:-inform the pediatrician-give Naloxon (Narcon) 0.02mg IM to the neonate.c-Use Entonox (NO2 50%+O2 50%) by mask if available.d-Use epidural analgesia in selected cases if available such as Breech, Twins, preterm delivery.e-Give anti-emetics such as Metoclopromide (5-10mg)IM if necessary, but should not be routine.13-Do vaginal examination to:a-assess progress of labour every 2-4hrb-or immediately after rupture of membranesc-FHR abnormalities.
14-Recall all the observations in labour in Partogram.15-Consider augmentation with syntocinon if progress of labour is slow (partogram).-1000 ml Hartmann’s solution or normal saline + 10 units syntocinon (pitocin) -Begin the infusion using a pump at 4 milliunits per minute and double the dose every 20 minutes to a maximum of 32 milliunits/min.-Or begin with 15 drops / min and increase the rate by 10 drops every 30 minutes untill adequate contractions.
II-second stage of labour:
Once the patient reach the second stage of labour and have the desire to push down then:
1-Put the patient in lithotomy position or other positions clean the vulva, and perineum with antiseptic solution.
2-Encourage organized pushing down which she is feeling to do so
3. -Monitor the uterine contraction and fetal heart more frequent.
4. -Use syntocinon if progress is slow and no contractions.
5. -When the head appears at the vulva, the perineum is supported during uterine contraction by sterile pad to promote flexion and prevent premature extension of the head by pressing up on the sinciput until crowning occur.
6. -After crowning the head is allowed to be delivered by extension slowly in between the contractions by sliding the perineum over the face.
7. -DO episiotomy if necessary under local anaesthetic ( 10-20 ml) of 1% lignocain, but should not be routine.
8. -Wait for the next contraction to deliver the shoulder and trunks.
9. -Clamp and deliver the cord and baby to be handled to pediatrician.

III-Third stage of labour:The management of third stage is
aimed at:1-Complete delivery of the after birth
(placenta and membranes).2-Prevention of acute inversion of the
uterus.3-prevention of postpartum
haemorrhage

A-Delivery of the placenta and membranes:a-Conservative method: the left hand is placed over the abdomen to detect any change in the level of the fundus or sign of placental separation and decent are detected, the patient is asked to bear down to deliver the placenta spontaneously. Ergometrine 0.5mg or Syntometrine(5 units syntocinon + 0.5mg Ergometrine) to be given intravenouslly.
Signs of separation and decent of the placenta:
1. -The body of the uterus becomes smaller, harder, and globular.
2. -The fundal level rises in the abdomen because the lower segment becomes distended by the placenta.
3. -Suprapubic bulge may appear due to presence of the placenta in the lower segment.
4. -Elongation of the cord out side the vulva.5. -Sudden gush of blood from the vagina.

b-Active methods(prophylaxis against postpartum haemorrhage)
1-Give Methargine 0.5 mg IM or Syntometrine (5units oxytocin+0.5mg Methargine), at the time of the anterior shoulder is free from symphysis pubis or as soon as possible thereafter.
2-Deliver the placenta and membranes by control cord traction by right hand, and the left hand is placed on the suprapubic region, pushing the uterus upwards.
N.B. USE SYNTOCINON RATHER THAN METHARGINE IN CARDIAC AND HYPERTENSIVE CASES.
IV-Post Delivery:1-examine the placenta for their
completeness, anomalies, length, and number of vessels in the cord and record the placental weight.
2-Suture the episiotomy or any laceration.3-Estimate blood loss, count swabs, and take
cord blood for Hb, blood group, Rh, bilirubin, and coomb’s test for Rh negative mother.
4-Check BP, P, T, Lochia and firmness of the uterus before transferring the patient.
5-Continue an infusion of syntocinon through the first hour if necessary.
6-Allow no food during the first hour, sips of water may be taken, encourage nursing.

V-Care of the new born infant:1. -Clearance of the new passages.2. -Determine the Apgar score one and five
minutes- heart rate- respiratory rate- muscle tone- colour- reflex irritability3-Care of the umbilical cord stump4-General assessment of the infant to exclude
any congenital anomalies.5-Identification of weight, estimate the
gestational age, dress it and put a mask to identify it.
6-Protect the baby against cold.
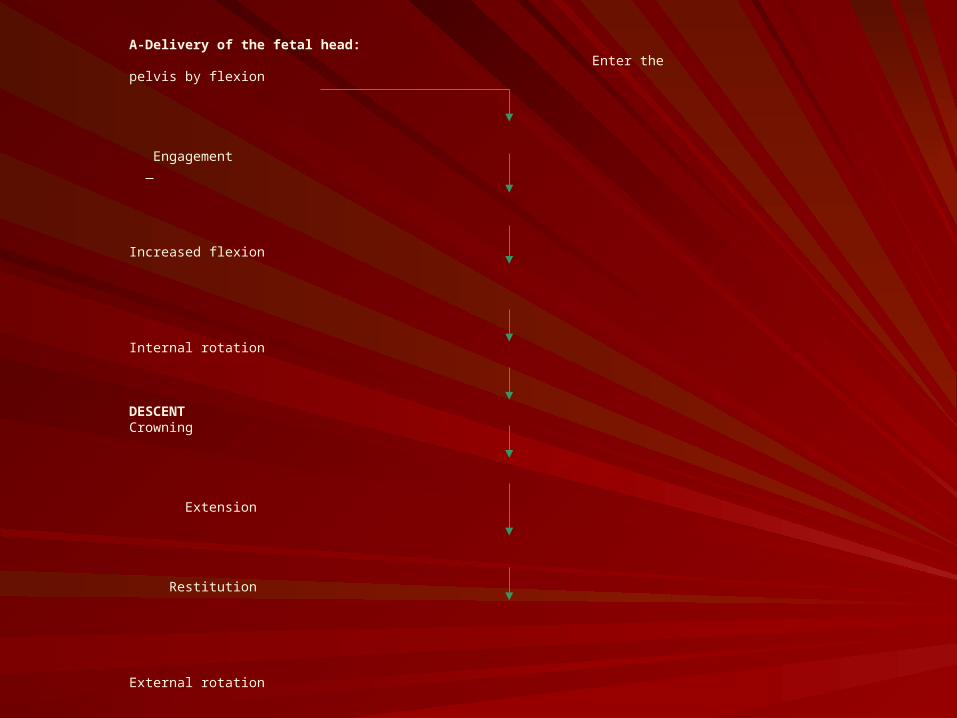
A-Delivery of the fetal head: Enter the pelvis by flexion
Engagement
Increased flexion
Internal rotation
DESCENT Crowning
Extension
Restitution
External rotation
Delivery of the fetal head
B-Delivery of the shoulder and body:

















