Case Report J. St. Marianna Univ. Vol. 7, pp. 21–25, 2016 1 Division of Gastroenterological and General Surgery, St. Marianna University School of Medicine 2 Department of Gastroenterological and General Surgery, St. Marianna University Yokohama City Seibu Hospital 3 Department of Gastroenterological and General Surgery, Kawasaki Municipal Tama Hospital 4 Digestive Disease Center, St. Marianna University School of Medicine Toyoko Hospital Laparoscopic Parastomal Hernia Repair Performed With Two Different Composite Meshes: Report of a Case Ryoji Makizumi 1 , Kuniyasu Horikoshi 2 , Tsukasa Shimamura 3 , Akira Hanai 1 , Satoshi Tsukikawa 1 , Yukihito Kokuba 2 , Nobuyoshi Miyajima 4 , and Takehito Otsubo 1 (Received for Publication: January 25, 2016) Abstract A 69-year-old man presented to us with a large peristomal bulge. He had undergone laparoscopic abdomi‐ noperineal resection with D3 dissection and sigmoid colostomy for lower rectal cancer and 14 months later be‐ gan to notice a bulge in the stoma area. Because of an absence of specific symptoms, continued follow-up was decided upon. However, within 9 months, the bulge had grown so large that it had become difficult for the pa‐ tient to secure the stoma bag in place, so surgery was performed. Abdominal computed tomography revealed the sigmoid colostomy as well as a hernial sac into which intra-abdominal fatty tissue had prolapsed. The sac was cranial to the lifted bowel. Laparoscopic repair was performed. Exploration of the abdominal cavity showed ad‐ herence of the greater omentum, sigmoid mesocolon, and fatty appendages to the abdominal wall around the lifted bowel. Upon adhesiolysis, a 3×3-cm hernial orifice cranial to the lifted sigmoid colon was seen. The ori‐ fice was closed with three sutures of 2–0 absorbable material and repaired with two different Parietex Parasto‐ mal meshes (keyhole style and central band style meshes). The two meshes were fixed so that they overlapped each other. Three cicatricial hernias observed along the midline of the lower abdomen were simultaneously re‐ paired. The operation time was 170 minutes, and the blood loss volume was small. The postoperative course was uneventful. The patient began oral intake on postoperative day 1 and was discharged on postoperative day 4. One year and 6 months have passed since the surgery, and there is no evidence of recurrence. The laparo‐ scopic two-mesh repair is described in detail along with a review of the literature. Key Words Parastomal hernia, laparoscopic surgery, sandwich technique Introduction Parastomal hernia is a common late complica‐ tion of gastrointestinal stoma for which there are var‐ ious repair methods. A procedure for parastomal her‐ nia repair with mesh products designed for use in the peritoneal cavity was recently reported 1–4) . Herein, we report a case of parastomal hernia for which we per‐ formed laparoscopic repair using two different Parie‐ tex Composite meshes. In addition, we review our technique in light of the literature. Case The patient was a 69-year-old man who presen‐ ted to us in December 2012 with a peristomal bulge. He was 177 cm tall, weighed 79 kg, and had a body mass index of 25.2 kg/m 2 . His medical history inclu‐ ded an unrelated surgery for appendicitis, which had left him with a lower midline surgical scar. In Octo‐ ber 2011, however, he had undergone laparoscopic abdominoperineal resection with D3 lymph node dis‐ section and sigmoid colostomy for lower rectal can‐ 21 21
Transcript
Case Report J. St. Marianna Univ.Vol. 7, pp. 21–25, 2016
1 Division of Gastroenterological and General Surgery, St. Marianna University School of Medicine2 Department of Gastroenterological and General Surgery, St. Marianna University Yokohama City Seibu Hospital3 Department of Gastroenterological and General Surgery, Kawasaki Municipal Tama Hospital4 Digestive Disease Center, St. Marianna University School of Medicine Toyoko Hospital
Laparoscopic Parastomal Hernia Repair Performed With
AbstractA 69-year-old man presented to us with a large peristomal bulge. He had undergone laparoscopic abdomi‐
noperineal resection with D3 dissection and sigmoid colostomy for lower rectal cancer and 14 months later be‐gan to notice a bulge in the stoma area. Because of an absence of specific symptoms, continued follow-up wasdecided upon. However, within 9 months, the bulge had grown so large that it had become difficult for the pa‐tient to secure the stoma bag in place, so surgery was performed. Abdominal computed tomography revealed thesigmoid colostomy as well as a hernial sac into which intra-abdominal fatty tissue had prolapsed. The sac wascranial to the lifted bowel. Laparoscopic repair was performed. Exploration of the abdominal cavity showed ad‐herence of the greater omentum, sigmoid mesocolon, and fatty appendages to the abdominal wall around thelifted bowel. Upon adhesiolysis, a 3×3-cm hernial orifice cranial to the lifted sigmoid colon was seen. The ori‐fice was closed with three sutures of 2–0 absorbable material and repaired with two different Parietex Parasto‐mal meshes (keyhole style and central band style meshes). The two meshes were fixed so that they overlappedeach other. Three cicatricial hernias observed along the midline of the lower abdomen were simultaneously re‐paired. The operation time was 170 minutes, and the blood loss volume was small. The postoperative coursewas uneventful. The patient began oral intake on postoperative day 1 and was discharged on postoperative day4. One year and 6 months have passed since the surgery, and there is no evidence of recurrence. The laparo‐scopic two-mesh repair is described in detail along with a review of the literature.
Parastomal hernia is a common late complica‐tion of gastrointestinal stoma for which there are var‐ious repair methods. A procedure for parastomal her‐nia repair with mesh products designed for use in theperitoneal cavity was recently reported1–4). Herein, wereport a case of parastomal hernia for which we per‐formed laparoscopic repair using two different Parie‐tex Composite meshes. In addition, we review ourtechnique in light of the literature.
Case
The patient was a 69-year-old man who presen‐ted to us in December 2012 with a peristomal bulge.He was 177 cm tall, weighed 79 kg, and had a bodymass index of 25.2 kg/m2. His medical history inclu‐ded an unrelated surgery for appendicitis, which hadleft him with a lower midline surgical scar. In Octo‐ber 2011, however, he had undergone laparoscopicabdominoperineal resection with D3 lymph node dis‐section and sigmoid colostomy for lower rectal can‐
21
21
11mm
5mm
5mm
Parastomal hernia
incisional hernias
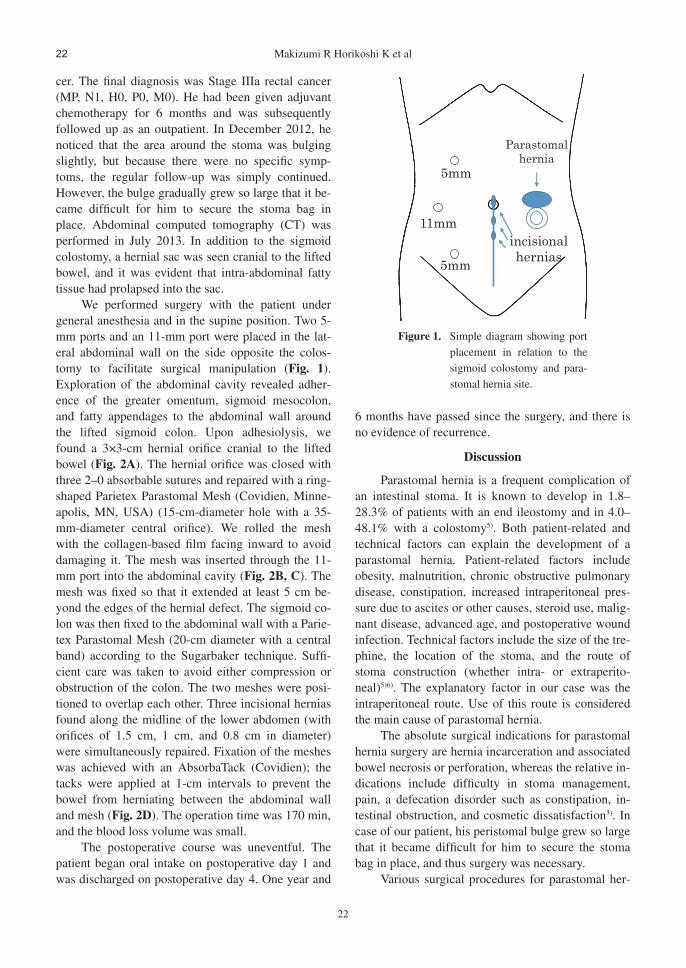
Figure 1. Simple diagram showing port
placement in relation to the
sigmoid colostomy and para‐
stomal hernia site.
cer. The final diagnosis was Stage IIIa rectal cancer(MP, N1, H0, P0, M0). He had been given adjuvantchemotherapy for 6 months and was subsequentlyfollowed up as an outpatient. In December 2012, henoticed that the area around the stoma was bulgingslightly, but because there were no specific symp‐toms, the regular follow-up was simply continued.However, the bulge gradually grew so large that it be‐came difficult for him to secure the stoma bag inplace. Abdominal computed tomography (CT) wasperformed in July 2013. In addition to the sigmoidcolostomy, a hernial sac was seen cranial to the liftedbowel, and it was evident that intra-abdominal fattytissue had prolapsed into the sac.
We performed surgery with the patient undergeneral anesthesia and in the supine position. Two 5-mm ports and an 11-mm port were placed in the lat‐eral abdominal wall on the side opposite the colos‐tomy to facilitate surgical manipulation (Fig. 1).Exploration of the abdominal cavity revealed adher‐ence of the greater omentum, sigmoid mesocolon,and fatty appendages to the abdominal wall aroundthe lifted sigmoid colon. Upon adhesiolysis, wefound a 3×3-cm hernial orifice cranial to the liftedbowel (Fig. 2A). The hernial orifice was closed withthree 2–0 absorbable sutures and repaired with a ring-shaped Parietex Parastomal Mesh (Covidien, Minne‐apolis, MN, USA) (15-cm-diameter hole with a 35-mm-diameter central orifice). We rolled the meshwith the collagen-based film facing inward to avoiddamaging it. The mesh was inserted through the 11-mm port into the abdominal cavity (Fig. 2B, C). Themesh was fixed so that it extended at least 5 cm be‐yond the edges of the hernial defect. The sigmoid co‐lon was then fixed to the abdominal wall with a Parie‐tex Parastomal Mesh (20-cm diameter with a centralband) according to the Sugarbaker technique. Suffi‐cient care was taken to avoid either compression orobstruction of the colon. The two meshes were posi‐tioned to overlap each other. Three incisional herniasfound along the midline of the lower abdomen (withorifices of 1.5 cm, 1 cm, and 0.8 cm in diameter)were simultaneously repaired. Fixation of the mesheswas achieved with an AbsorbaTack (Covidien); thetacks were applied at 1-cm intervals to prevent thebowel from herniating between the abdominal walland mesh (Fig. 2D). The operation time was 170 min,and the blood loss volume was small.
The postoperative course was uneventful. Thepatient began oral intake on postoperative day 1 andwas discharged on postoperative day 4. One year and
6 months have passed since the surgery, and there isno evidence of recurrence.
Discussion
Parastomal hernia is a frequent complication ofan intestinal stoma. It is known to develop in 1.8–28.3% of patients with an end ileostomy and in 4.0–48.1% with a colostomy5). Both patient-related andtechnical factors can explain the development of aparastomal hernia. Patient-related factors includeobesity, malnutrition, chronic obstructive pulmonarydisease, constipation, increased intraperitoneal pres‐sure due to ascites or other causes, steroid use, malig‐nant disease, advanced age, and postoperative woundinfection. Technical factors include the size of the tre‐phine, the location of the stoma, and the route ofstoma construction (whether intra- or extraperito‐neal)5)6). The explanatory factor in our case was theintraperitoneal route. Use of this route is consideredthe main cause of parastomal hernia.
The absolute surgical indications for parastomalhernia surgery are hernia incarceration and associatedbowel necrosis or perforation, whereas the relative in‐dications include difficulty in stoma management,pain, a defecation disorder such as constipation, in‐testinal obstruction, and cosmetic dissatisfaction3). Incase of our patient, his peristomal bulge grew so largethat it became difficult for him to secure the stomabag in place, and thus surgery was necessary.
Various surgical procedures for parastomal her‐
22
Makizumi R Horikoshi K et al22
A B
C D
Figure 2. Intraoperative photographs.
(A) A 3×3-cm fascial defect was revealed after reduction of the stomal prolapse.
(B) The hernial orifice fascia was closed with three sutures of 2–0 absorbable ma‐
terial.
(C) A keyhole style mesh was secured with sutures and tacks.
(D) A center band style mesh was secured with sutures and tacks, and this allowed
for lateralization of the colon going to the stoma.
nia repair have been reported, and the widespread ac‐ceptance and application of laparoscopic surgery inrecent years has resulted in an increasing number ofreports of laparoscopic surgery for repair of this clini‐cal entity. The advantages of laparoscopic surgery areas follows: (1) the hernia can be closely examined,and collateral lesions can also be detected; (2) fascialexposure for mesh placement is unnecessary; (3) thehernial orifice can be fully covered with a mesh; (4)the risk of postoperative infection is reduced; (5)clean surgery can be performed; and (6) because ofthe small incisions, the procedure is applicable evenin obese patients. Disadvantages are reported, how‐ever, and these include (1) the fact that the procedureis very expensive, (2) the fact that the procedure issomewhat complicated in comparison to open sur‐gery, and (3) the fact that the procedure is difficult inpatients with severe adhesions1)3)7–9). A comparativestudy of laparotomy and laparoscopy for parastomalhernia repair showed that the latter results in a shorterhospital stay, a lower incidence of surgical site infec‐tion, and a lower overall risk of morbidity10). At ourhospital, we have aggressively introduced laparo‐scopic surgery for the treatment of parastomal hernia,
and we chose the laparoscopic procedure for the pa‐tient described herein in an effort to achieve a mini‐mally invasive surgery and few or no complications.
Surgical techniques for parastomal hernia repairinclude direct hernia orifice closure with sutures,stoma relocation, and prosthetic mesh placement. Di‐rect hernia orifice closure is the simplest procedurebecause it does not involve stoma relocation, but thesubsequent recurrence rate of 46–100% is signifi‐cantly higher than that following mesh repair5)11).Placement of a prosthetic mesh varies somewhat, de‐pending on the level of the abdominal wall at whichthe mesh will be placed. Although recurrence rateshave not been shown to differ significantly, the rate ishigher with the onlay method than when the mesh isplaced in the preperitoneal position11). Intraperitonealmesh repair can be performed either as laparoscopicor open surgery and by any of three techniques: theSugarbaker technique, the keyhole technique, or thesandwich technique (which combines the formertwo)8–9)12). Results of the keyhole method have beensomewhat disappointing. The reported recurrencerate for the laparoscopic keyhole technique is 44.4%within 6 months of the initial operation13). Muysoms
23
Laparoscopic parastomal hernia repair 23
also reported a disappointing experience and high re‐currence rate with the keyhole technique14).
Results of the Sugarbaker technique have beenmore acceptable. For example, Hansson et al reporteda 6.6% recurrence rate among patients who were fol‐lowed up for a mean of 2 years after laparoscopicSugarbaker technique3), and Mancini et al reported a4% recurrence rate after laparoscopic Sugarbaker re‐pair among patients who were followed up for a me‐dian 19 months (range, 2–38 months)15) . Althoughthe reported recurrence rate for the laparoscopic key‐hole technique is high, that for the laparoscopic sand‐wich technique is low at 2.1%9).
The laparoscopic Sugarbaker technique and themodified Sugarbaker technique are reported to besafe and useful for parastomal hernia repair2)3). Thesandwich technique compensates for the weakness ofthe keyhole technique, and the recurrence rate islower than that seen with the Sugarbaker techniquealone4). Therefore, we chose the Sandwitch techniquein the hope of preventing recurrence.
When the sandwich technique was first devised,the meshes used had no an anti-adhesion barrier. Thisis a major drawback because the bowel, in cases ofparastomal hernia repair, will come into contact withthe mesh. The two meshes we used in our patientwere both designed for parastomal hernia repair, andboth are covered by an absorbable, anti-adhesionfilm. The first one is particularly suited to Sugarbakertechnique, and the second to keyhole technique.
It was for these reasons that we chose to apply aminimally invasive laparoscopic sandwich techniqueusing two different Parietex Composite meshes. TheParietex Composite parastomal meshes we used areprosthetic materials intended specifically for parasto‐mal hernia repair. They are very useful products be‐cause one surface or portion is covered with collagenfilm aimed at reducing adherence to abdominal or‐gans such as the bowel. However, when we use twodifferently styled meshes made of the same compo‐site material, the collagen film surface of the keyholemesh can disturb attachment of the central band stylemesh. There are two important precautions that mustbe taken to prevent herniation between the first meshand second mesh: The second mesh (central bandstyle) must cover the first mesh (keyhole style) in itsentirety as well as the abdominal wall16), and the sec‐ond mesh should be fixed with tacks spaced 1 cmapart around its circumference.
A substantial amount of time has passed sinceour patient’s surgery without any evidence of recur‐
rence, and there were no complications resultingfrom the mesh placement. Our experience in this caseleads us to consider application of the laparoscopicsandwich technique with two different Parietex Com‐posite meshes useful for parastomal hernia repair. Wehope to conduct studies involving a substantial num‐ber of patients to evaluate the safety and utility of thistechnique for parastomal hernia repair. And it will beexpected the development of new mesh for sandwitchtechnique in the future.
Conclusion
We describe a laparoscopic parastomal herniarepair performed with two different Parietex Compo‐site meshes. The good short and long-term outcomesin this case lead us to consider the technique usefulfor parastomal hernia repair.
References
1) Atsumi Y, Sato T, Rino Y, Hasegawa S, Hase‐gawa S, Tamagawa H, Tsuchida K, Oshima T,Yukawa N, Yoshikawa T, Masuda M. A case ofparastomal hernia treated by laparoscopic sur‐gery. Nippon Gekakei Rengou Gakkai Zasshi2013; 38: 927–931 (in Japanese with Englishabstract).
3) Hansson BM, Morales-Conde S, Mussack T,Valdes J, Muysoms FE, Bleichrodt RP. The lap‐aroscopic modified Sugarbaker technique is safeand has a low recurrence rate: a multicenter co‐hort study. Surg Endosc 2013; 27: 494–500.
4) Nakashima M, Nagasue Y, Tanaka E, HayashiK, Yokomizo H, Hirata T. Two cases of laparo‐scopic parastomal hernia repair by sandwichtechnique. J Jpn Soc Endosc Surg 2014; 19:723–729.
6) Pearl RK. Parastomal hernias. World J Surg1989; 13: 569–572.
7) Bittner R, Bingener-Casey J, Dietz U, Fabian M,Ferzli G, Fortelny R, Köckerling F, Kukleta J,LeBlanc K, Lomanto D, Misra M, Morales-Conde S, Ramshaw B, Reinpold W, Rim S,Rohr M, Schrittwieser R, Simon T, SmietanskiM, Stechemesser B, Timoney M, Chowbey P.Guidelines for laparoscopic treatment of ventraland incisional abdominal wall hernias (Interna‐
24
Makizumi R Horikoshi K et al24
tional Endohernia Society [IEHS])-Part III. SurgEndosc 2014; 28: 380–404.
8) Hansson BM, Bleichrodt RP, de Hingh IH. Lap‐aroscopic parastomal hernia repair using a key‐hole technique results in a high recurrence rate.Surg Endosc 2009; 23: 1456–1459.
9) Berger D, Bientzle M. Laparoscopic repair ofparastomal hernias: a single surgeon’s experi‐ence in 66 patients. Dis Colon Rectum 2007; 50:1668–1673.
10) Halabi WJ, Jafari MD, Carmichael JC, NguyenVQ, Mills S, Phelan M, Stamos MJ, Pigazzi A.Laparoscopic versus open repair of parastomalhernias: an ACS-NSQIP analysis of short-termoutcomes. Surg Endosc 2013; 27: 4067–4072.
11) Hansson BM, Slater NJ, van der Velden AS,Groenewoud HM, Buyne OR, de Hingh IH,Bleichrodt RP. Surgical techniques for parasto‐mal hernia repair: a systematic review of the lit‐
erature. Ann Surg 2012; 255: 685–695.12) Sugarbaker PH. Peritoneal approach to pros‐
thetic mesh repair of paraostomy hernias. AnnSurg 1985; 201: 344–346.
13) Safadi B. Laparoscopic repair of parastomal her‐nias. Early results. Surg Endosc 2004; 18: 676–680.
14) Muysoms F. Laparoscopic repair of parastomalhernias with a modified Sugarbaker technique.Acta Chir Belg 2007; 107: 476–480.
15) Mancini GJ, McClusky DA, Khaitan L, et al.Laparoscopic parastomal hernia repair using anonslit mesh technique. Surg Endosc 2007; 21:1487–1491.
16) DeAsis FJ, Lapin B, Gitelis ME, Ujiki MB. Cur‐rent state of laparoscopic parastomal hernia re‐pair: a meta-analysis. World J Gastroenterol2015; 21: 8670–8677.