CONGESTIVE HEART FAILURE CONGESTIVE HEART FAILURE (CHF) NYHA III e.c Coronary (CHF) NYHA III e.c Coronary Artery Disease (OMI Artery Disease (OMI Anteroseptal) Anteroseptal) Supervisor : dr. Pendrik Tandean, SpPD-KKV.FINASIM By : Fathlina C 111 08 212
Transcript
CONGESTIVE HEART FAILURE CONGESTIVE HEART FAILURE
(CHF) NYHA III e.c Coronary (CHF) NYHA III e.c Coronary
Artery Disease (OMI Artery Disease (OMI
Anteroseptal)Anteroseptal)
Supervisor :
dr. Pendrik Tandean, SpPD-KKV.FINASIM
By :FathlinaC 111 08 212
Patient Identity
• Name : Mrs. T• Gender : Female• Age : 68 years old
Anamnesis (1)• Chief Complaint : Shortness of breath
• Shortness of breath has been experienced since 2 years ago and worsened from yesterday. It was experienced while doing minimal activity such as walking to the bathroom and relieved with resting. There is complain of sudden shortness of breath during night time that cause her to be awaken. He also had to use at least 2 pillows to sleep during night time.
Anamnesis (2)• There is also history of chest pain which has been experienced since 2 years ago. Chest pain was felt like being as punch like pain spread to the neck until her arms and last for less than 5 minutes of duration. Chest pain was also relieved by resting.
• There is no complaint of palpitation, fever, cough, nausea, and vomit.
• There is no complaint of urination and defecation.
Past Medical History• There is history of being admitted to the hospital 2 times with the same complaint of shortness of breath.
• There is history of hypertension since 10 years ago but she doesn’t take the drugs regularly.
• She never smoking and consumption alcohol.• There is no history of fever, congenital heart disease, thyroid disease, and diabetes mellitus.
• There is also no family history with cardiovascular disease and thyroid disease.
Risk Factors
• Cigarette smoking (-)• Alcohol consumption(-)• Hypertension(+)• Diabetes Mellitus(-)• Cardiovascular disease (+)• Thyroid disease (-)• History of cardiovascular disease and thyroid disease in family (-)
Physical Examination
General Status:• Severe ill• Nutritional Status: Good • Consciousness: Conscious
Head and Neck Examinations:• Eye : Conjunctiva anemic (-/-), sclera icteric (-/-)• Lip : cyanosis (-)• Neck : No mass, no tenderness, JVP : R + 3 cmH2O
Chest Examination• Inspection : Symmetric left=right • Palpation : No mass, no tenderness, vocal fremitus
left=right• Percussion : Sonor left = right, lung-liver border in ICS
VI right anterior• Auscultation: Breath sound : vesicular Additional sound : Ronchi + +
Wheezing -/- + + + ++ +
Physical Examination
Cardiac Examination•Inspection : Ictus cordis was not visible•Palpation : Ictus cordis was not palpable•Percussion :Right heart border in right parasternal line, left heart border two fingers from left midclavicular line ICS VI.•Auscultation : Heart sound : S I/II regular, no gallop, no additional sound
Physical Examination
Abdominal Examination
• Inspection : flat, following breath movement
• Auscultation : Peristaltic sound (+), normal
• Palpation : No mass, no tenderness, no palpable
liver and spleen
• Percussion : Tympani (+), ascites (-)
Extremities Examination
• Pretibial edema -/-
• Dorsum pedis edema -/-
Physical Examination
Electrocardiography(ECG)Electrocardiography(ECG)
Interpretation:•Rhythm:No sinus•HR/QRS rate:75x/minutes•Regularity: regular•P wave & PR interval: 0,08s and 0,16 s•QRS Complex: 2 small squares(0.08s), Q pathologies in V1,V2, V3. VES (+)•Axis: Normal•ST segment: Normal•T wave: Normal
Conclusion of ECG• Sinus rhythm. • HR 75x/minutes.• Normoaxis.• P wave normal.• Q pathologies in V1, V2, and V3 (OMI Anteroseptal).
• VES (+).• T wave normal
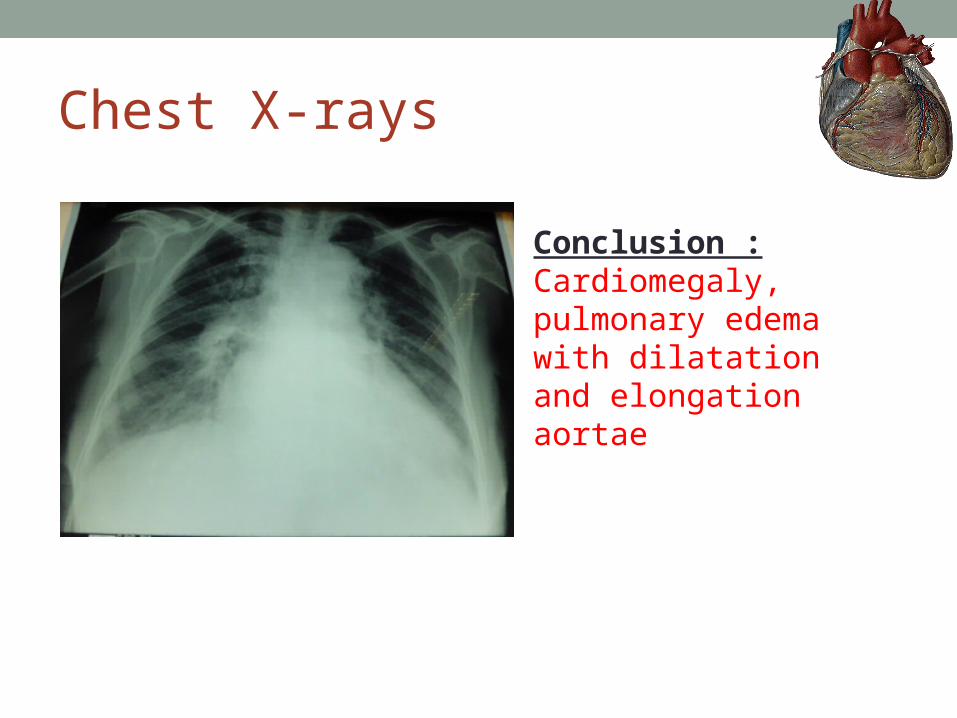
Chest X-rays
Conclusion :Cardiomegaly, pulmonary edema with dilatation and elongation aortae
Coronary Artery Disease• Coronary artery disease is a narrowing of the
small blood vessels that supply blood and oxygen to the heart.
• (CAD) occurs when the arteries that supply blood to the heart muscle (the coronary arteries) become hardened and narrowed due to buildup of a material called plaque (plaque) on their inner walls. This is known as atherosclerosis
• Eventually, blood flow to the heart muscle is reduced, and, because blood carries much-needed oxygen, the heart muscle is not able to receive the amount of oxygen it needs.
Causes Coronary Artery Disease
• Coronary artery disease (CAD) is caused by atherosclerosis (the thickening and hardening of the inside walls of arteries). Some hardening of the arteries occurs normally as a person grows older.
• In atherosclerosis, plaque deposits build up in the arteries. Plaque is made up of fat, cholesterol, calcium, and other substances from the blood. Plaque buildup in the arteries often begins in childhood.
Plaque in the arteries can be:• Hard and stable. Hard plaque causes the artery walls to thicken and harden. This condition is associated more with angina than with a heart attack, but heart attacks frequently occur with hard plaque.
• Soft and unstable. Soft plaque is more likely to break open or to break off from the artery walls and cause blood clots. This can lead to a heart attack.