20
LAST: PREVENTION AND TREATMENT PART A
| Date post: | 21-Dec-2015 |
| Category: |
Documents |
| Upload: | hester-evans |
| View: | 216 times |
| Download: | 0 times |

LAST: PREVENTION AND TREATMENT
PART A

PART A: OVERVIEW
• What are local anesthetics• Classification• MOA• Anesthetic potency• Clearance• Uses• Prolongation of action
PART B: ADVERSE EFFECTS&SYSTEMIC TOXICITY
• Allergic reaction• Local toxicity• Systemic toxicity

What are LA
• Weak bases which produce a transient and reversible loss of sensation (analgesia) in a circumscribed region of the body without loss of consciousness.
• Normally, the process is completely reversible.

Classification
• Local anesthetics - esters or amides.
• Major difference is their potential for producing adverse effects and the mechanisms of their metabolism.
Esters
• Eg: Procaine, Cocaine, tetracaine• The ester linkage is cleaved by plasma
cholinesterase. Short half life( abt 1min).• Amides:• Eg: lidocaine, Marcaine(Bupivacaine),
ropivacaine. Amide linkage is cleaved in the liver. Half life is about 2-3 hrs

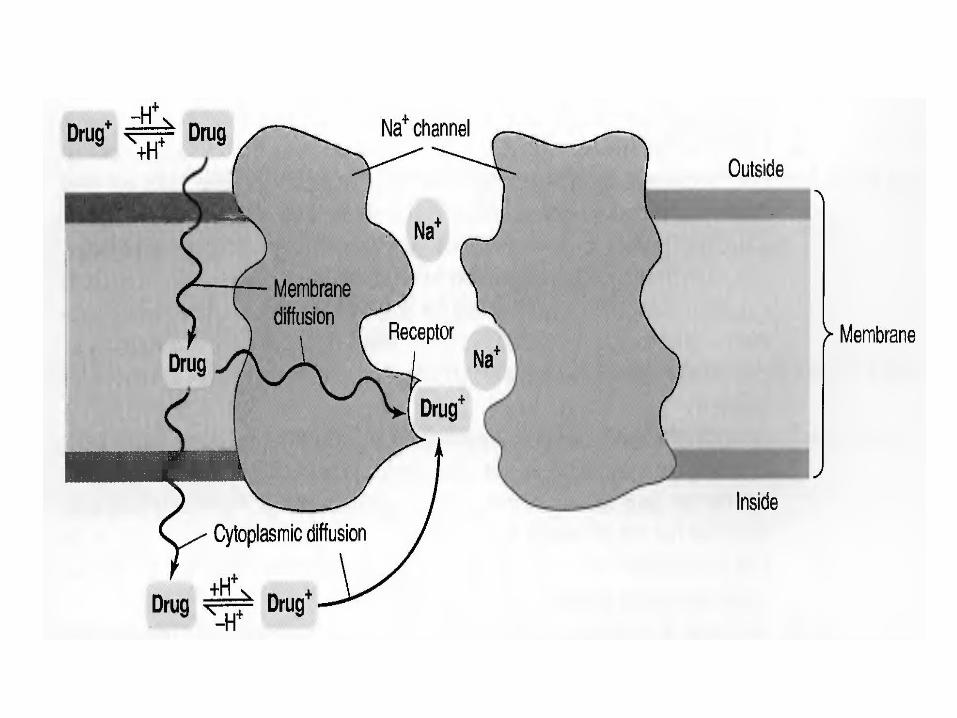
MECHANISM OF ACTION
• LA block nerve conduction by impairing propagation of action potential in axons. Interact directly with Na+ channels and stop Na+ ion influx. May also act on K+ & Ca+ channels.
• LA need to diffuse passively in uncharged state (lipophilic) to reach target-axoplasmic side of Na+ channel.
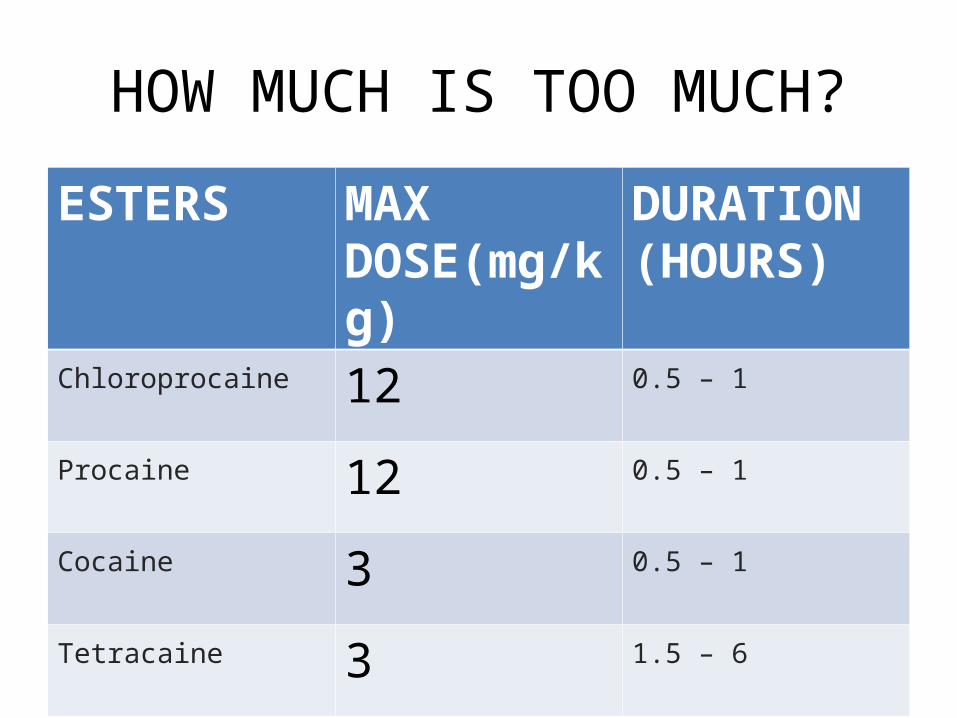
HOW MUCH IS TOO MUCH?
ESTERS MAX DOSE(mg/kg)
DURATION (HOURS)
Chloroprocaine 12 0.5 – 1
Procaine 12 0.5 – 1
Cocaine 3 0.5 – 1
Tetracaine 3 1.5 – 6

Amides Max Dose (mg/kg) Duration (h)
Lidocaine 4.5/(7 with epi) 0.75 – 1.5
Mepivacaine 4.5/(7 with epi) 1– 2
Prilocaine 8 0.5 – 1
Bupivacaine 3 1.5 – 8
Ropivacaine 3 1.5 – 8

ANESTHETIC POTENCY• The more LA is lipophilic the more potent it is
( increased rate of diffusion).• More protein binding prolongs the effect.
Bupivacaine is approximately 95% protein-bound. • Intermediate-duration LAs (lidocaine and
mepivacaine) have a smaller protein-bound fraction (60-70%).
• pH; higher pH speeds action (keeps LA uncharged).
• pKa: lower pKa faster onset.• Concentration; higher conc. =rapid onset (mass
effect).
CLEARANCE
• ESTERShydrolysis via tissue cholinesterase
• AMIDESmetabolism via hepatic enzymes
USES
•Surface anesthesia
•Infiltration anesthesia
•Regional anesthesia

SURFACE ANESTHESIA
• On intact skin –
• eutectic mixture of
Local anesthetics
• (EMLA)
• Slow absorption,
Action up to ½ Hr
INFILTRATION ANESTHESIA
• LA infiltrates locally into tissues to numb the area.
• Purpose of pain free procedures-before injections with large needles, lumbar puncture
REGIONAL ANESTHESIA
• Nerve block
• Intravenous
• Epidural/Extradural
• Intrathecal block/ spinal anaesthesia

NERVE BLOCKS
• Inject a drug around the nerve
• Anaesthetise a region

INTRAVENOUS ANESTHESIA
• 0.5-1% lidocaine without adrenaline
• Bier’s Block

EPIDURAL
• Thoracic, lumbar, sacral
• Act on nerve roots• Less hypotention

SPINAL BLOCK
• Sympathetic nerve block
• hypotension

















