58
Lean In to Medication Safety: A Human Factors Approach VSHP Spring Seminar April 2015 Deb Saine, MS, RPh, FASHP Valley Health System Winchester, VA [email protected]

Lean In to Medication Safety: A Human Factors Approach
VSHP Spring SeminarApril 2015
Deb Saine, MS, RPh, FASHPValley Health System
Winchester, [email protected]
Why Lean In?
• To press into something…
• Make a step forward
• Lean approach▫ Value (customer)▫ Respect (people doing the work)▫ Identify/eliminate defects (waste)

Objectives• Identify three ways humans err.
• List five human factors engineering strategies for error reduction.
• Recognize the hierarchy for effective application of safety strategies.
Overview • Basics of human error
• Systems thinking
• Human factors engineering (HFE) concepts
• HFE and medication safety
• Speaker has no conflicts of interest to disclose.

Definition of Error
•The failure of planned actions to achieve their desired ends, without the intervention of some unforeseeable event.
▫ J. Reason
Reason J. Human Error. Cambridge, UK: Cambridge University Press; 1990.

Preventable Medical Errors…
• Claim the lives of…▫ 400,000 people per year > 1000 people each day
• Persist as the…▫ Third most frequent cause of death in US
• Result in…▫ 10,000 serious complications each day
• Cost US healthcare…▫ $1 trillion per year
Healthcare IT News July 2014
Case Example: Preventing Deadly Vincristine Errors
• Intrathecal vincristine nearly always fatal• First case 1968…. Latest case?• How is vincristine dispensed in your setting?▫ Concentrated dose in syringe▫ Diluted in syringe▫ Diluted in minibag▫ Other/unsure/does not apply

How We Err: Skill – Rule - Knowledge Model
• SKILL - based ▫ “Automatic processing,” routine tasks▫ Routine tasks with occasional checks
▫ SLIP or LAPSE Attention or perception failure Memory failure (e.g. interruption)
How We Err: Skill – Rule - Knowledge Model
• SKILL - based examples:▫ Sound-alike-look-alike med error (slip) dobutamine, dopamine DOBUTamine, DOPamine
▫ Missed a non-automated additive to TPN (slip)▫ Wrong dose ordered/dispensed/administered
(lapse)▫ Forgetting to place auxiliary label on medication
(lapse)
How We Err: Skill – Rule - Knowledge Model
• RULE - based ▫ Intuitive processing▫ Problem encountered, use experience to solve “if this situation, then do this action”

How We Err: Skill – Rule - Knowledge Model
• RULE - based ▫ Rule “mismatch” – good rule, wrong time Tubing a fragile, protein-based medication in error
▫ Use of “bad” rule Procedures incomplete or misunderstood Using injectable syringe to measure oral medication
▫ Rule noncompliance (violation) Shortcuts; cannot follow rule at that time; thrill-
seeking

How We Err: Skill – Rule - Knowledge Model
• KNOWLEDGE - based ▫ Analytical processing▫ New situation, no experience rule to follow
▫ Problem encountered, no experience, create solution Solution incorrect Moving forward without necessary information
Human decisions also influenced by…
• Availability heuristic – facts that come readily vs. information that does not
• Confirmation bias – seek evidence to support the decision reached
• Selectivity – focus on what’s logically important
• Frequency gambling – betting on the condition that occurs most frequently
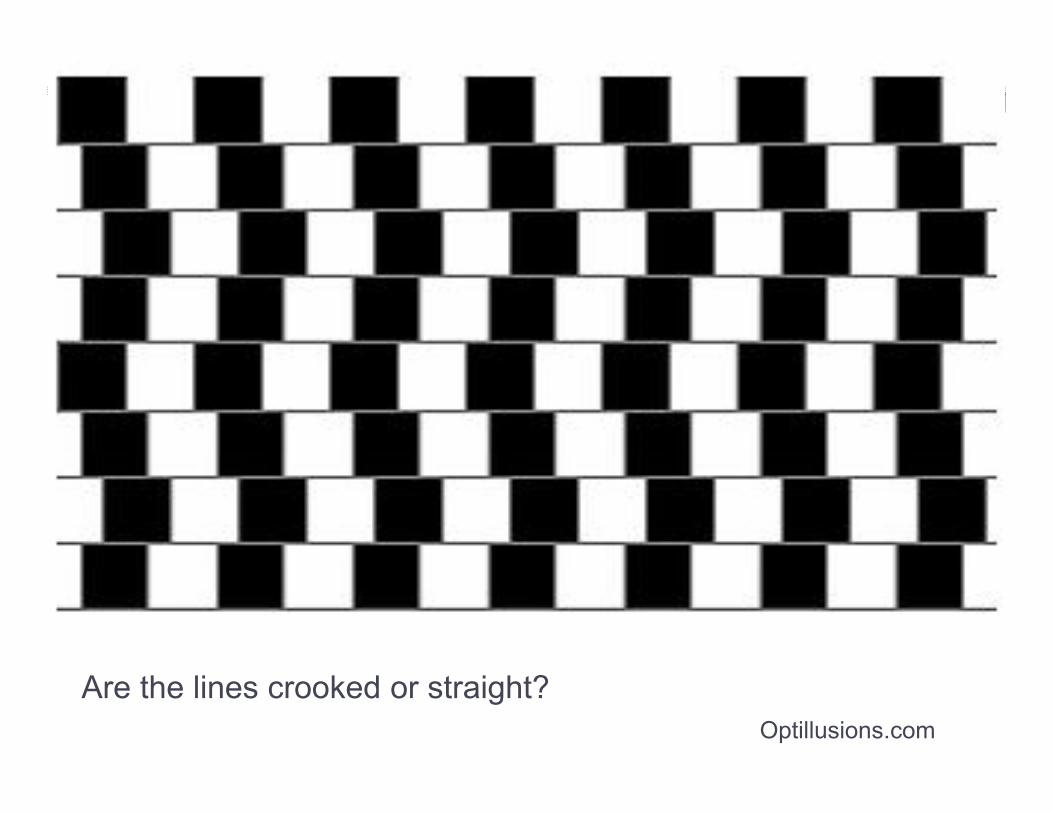
Are the lines crooked or straight?Optillusions.com

Demonstration: Stroop Effect
Row 1
Row 2
Row 3
State the Color of the Text
Red
Red
Red Blue
Blue
BlueYellow
Yellow
Yellow
Green
Green
Green
Row 1
Row 2
Row 3
State the Color of the Text
Red
Red
Red Blue
Blue
BlueYellow
Yellow
Yellow
Green
Green
Green
Row 1
Row 2
Row 3
For further info, see http://faculty.washington.edu/chudler/words.html#seffect
Stroop JR (1935) Studies of Interference in Serial Verbal Reactions. Journal of Experimental Psychology, vol 18, 643-662

System Approach• System: A set of interacting, interrelated, or
independent elements thatwork together in a particularenvironment to perform the functions required to achieve the system’s aim.
Bertalanfy LV. General system theory, Foundations, development, applications. New York: George Braziller, Inc. 1968.

Slices of cheese are defences or safeguards
Holes areweaknesses
A potential hazard or “accident”
SystemFailure
Policies & procedures
Technology, equipment
Staff & teams
Organizational structure & culture
Adapted from J. Reason19
“Swiss Cheese” Model

What is Human Factors Engineering?

What is Human Factors Engineering?
• The science of designing systems, devices, software, and tools to fit human capabilities and limitations
• Using methods to gather unique information on:▫ Hidden needs of the end-user▫ Unexpected interactions between the system and
the end-user
• Taking advantage of knowledge bases about human-system interaction
Adapted from John Gosbee, MD, MSVA National Center for Patient Safety
Premises of HFE
• Technologies/systems must be designed with users in mind
• Physical and cognitive limitations exist and design must accommodate
• Design of all things influences human behavior
• Evaluate during design process
• Uses scientific method
• Systems orientation

Demonstration


Broad Impact of HFE
• Aviation (since 1940’s)• Nuclear Power• Space flight• Computer software and hardware (1970’s)• Consumer products• Railroad, motor vehicles• Health care

Medication Safety

Medication Safety and HFE• Incorporate human factors principles into
design of processes
• Enhance performance and minimize errors
• Make it easy to do the right thing, and hard to do the wrong thing

• “We cannot change the human condition, but we can change the conditions under which humans work.” James Reason
Human error: models and management. BMJ. 200; 320:768-770.

Core Principles: Human Factors Design
• Simplify• Reduce reliance on
memory• Standardize• Error-proof• Make errors visible
• Reduce handoffs• Improve information
access• Automate wisely• Improve communication• Provide adequate training• Manage fatigue

Simplify• Complexity increases the risk of error▫ One step process w/ error rate of 1%▫ 100 steps 67%
• Example: medication formulary
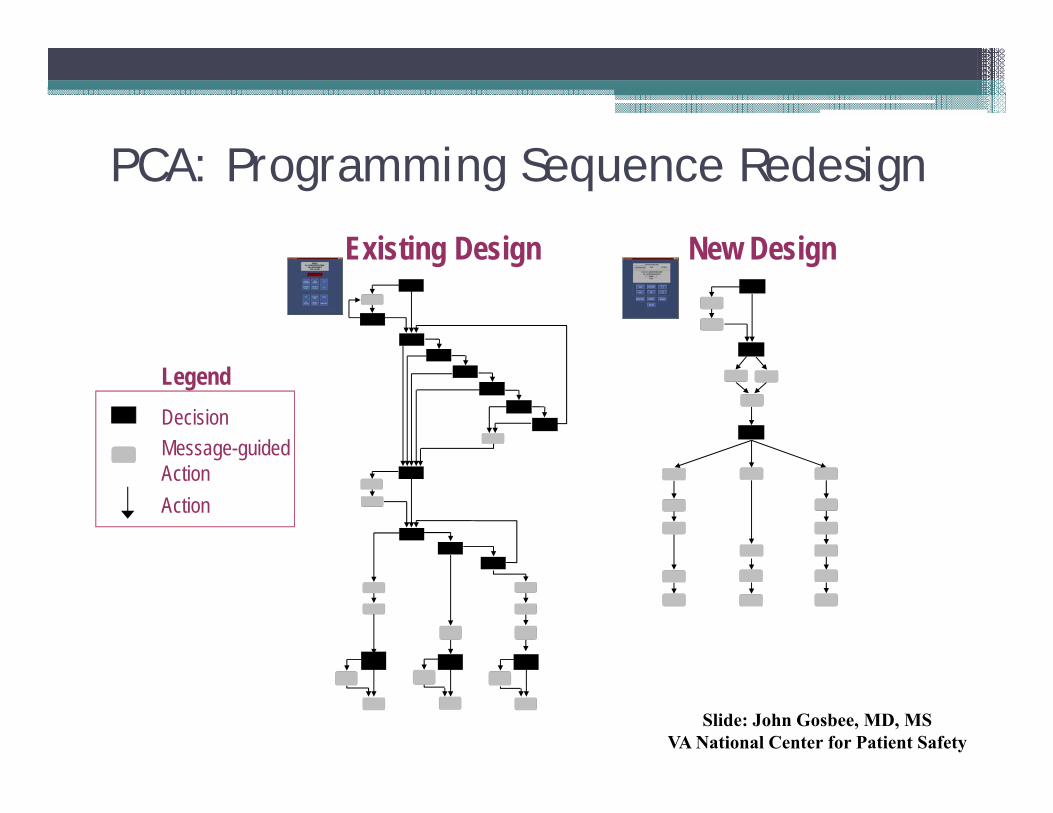
PCA: Programming Sequence Redesign
Existing Design New Design
DecisionMessage-guided ActionAction
Legend
Slide: John Gosbee, MD, MSVA National Center for Patient Safety
Reduce Reliance on Memory• Human mind – limited short term memory• In absence of reminders, probability of human
error of omission is 1%. If steps are embedded within a process, this probability drops by 70%!
• Examples: checklists, protocols, automated reminders

Standardize
• Allows optimization of a process (Lean!)• Limits choices in products, performance of
tasks or procedures• Improves communication: common
understanding• Examples: ▫ standardized IV infusion concentrations▫ script for med history interview▫ standardized format for progress notes


Alteplase Kit, Instructions
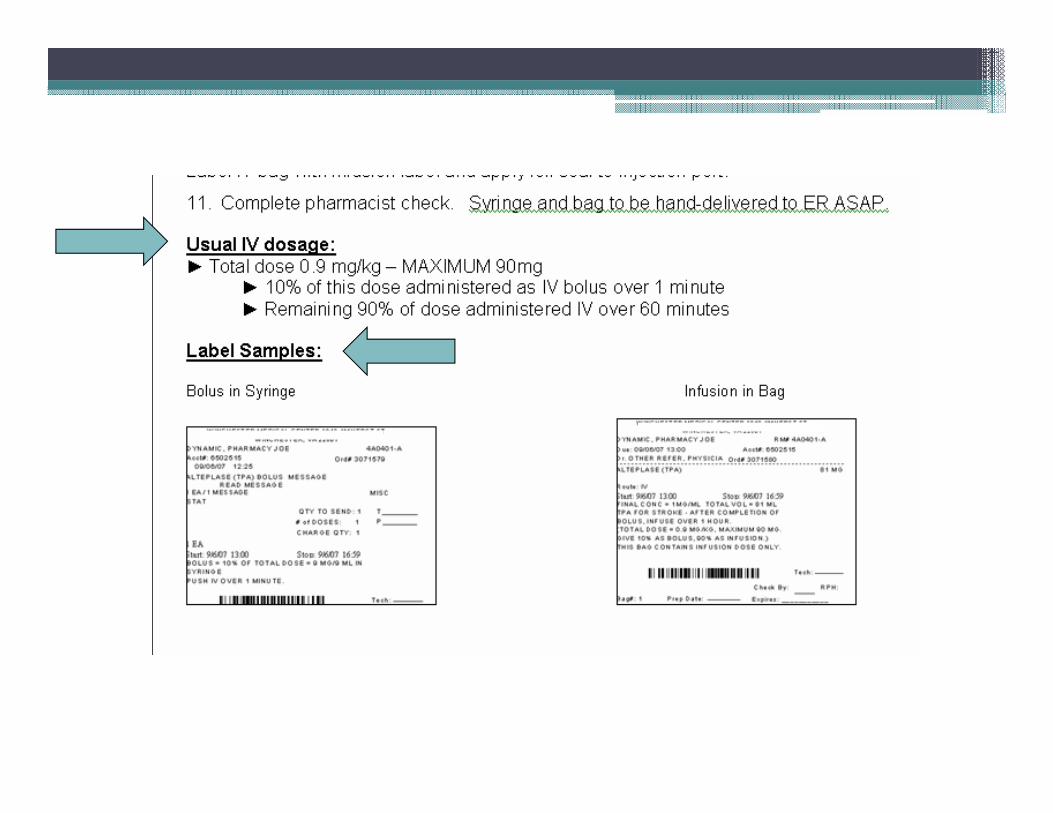

Dispensing Process: Double Check

Improved Checklist

Error-Proof• Designing the process to prevent error or
automate the inspection process to determine if error occurred
• Constraint: physical, procedural, cultural▫ file cabinet drawers, IV pump free flow protection▫ removal of KCl from patient care units, software
will not allow med to be ordered with inappropriate route
▫ not scheduling pharmacists or nurses to work consecutive shifts

Error-Proofing: Constraint
• Before: “380” 380 x 500mg = 190,000 mg
• After: entering “380” will not process order
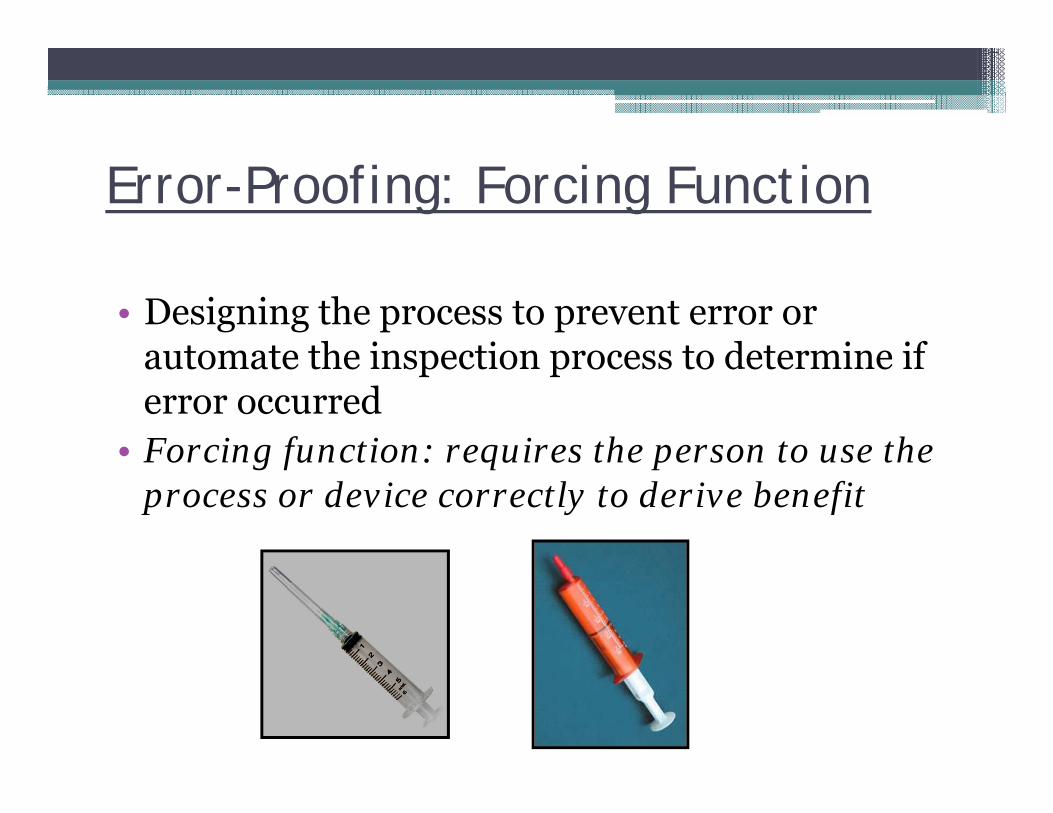
Error-Proofing: Forcing Function
• Designing the process to prevent error or automate the inspection process to determine if error occurred
• Forcing function: requires the person to use the process or device correctly to derive benefit
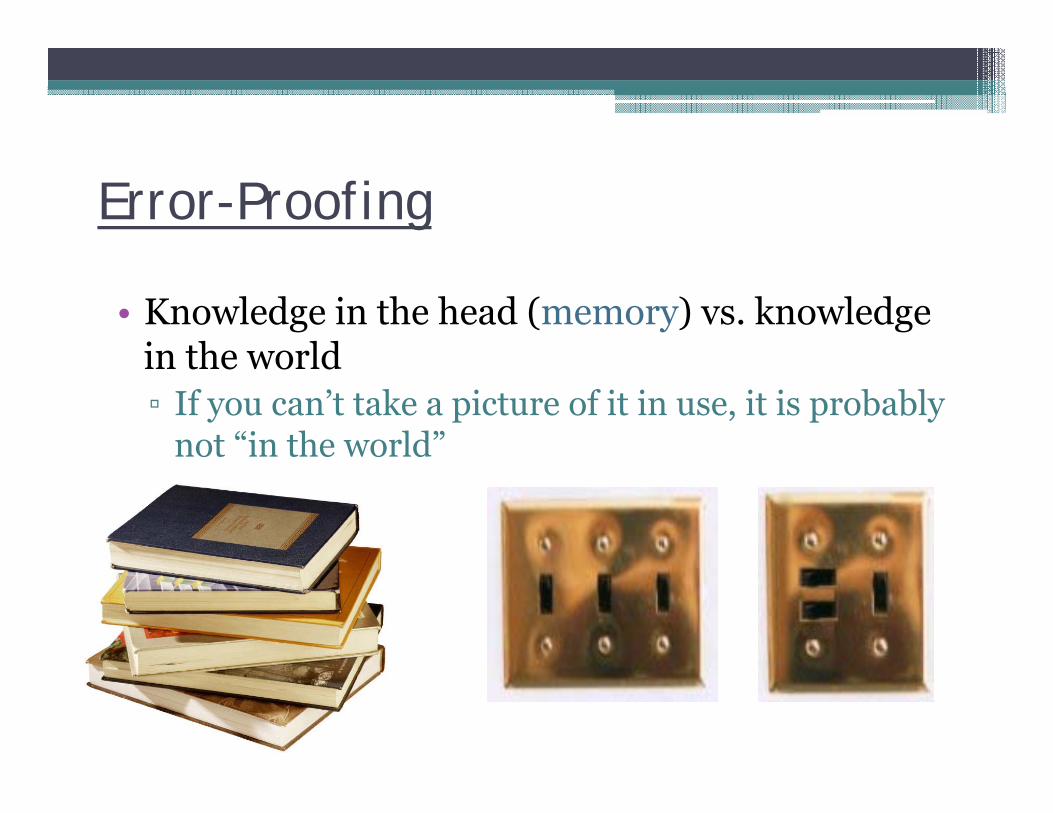
Error-Proofing
• Knowledge in the head (memory) vs. knowledge in the world▫ If you can’t take a picture of it in use, it is probably
not “in the world”

Make Errors Visible
• Use redundancies and safeguards to detect error
• Examples:▫ bar code medication verification▫ independent double check

Code Cart Drawer: Version 1

Code Cart Drawer: Version 5

Applying Design Strategies• Safety Hierarchy:
•Design > Guard
> Warn

Applying Design Strategies
Education/information“Be more careful”Checklists and check systemsStandardization and protocols
Rules and policiesForcing functions and constraintsVisual reminders
Automation and computerization
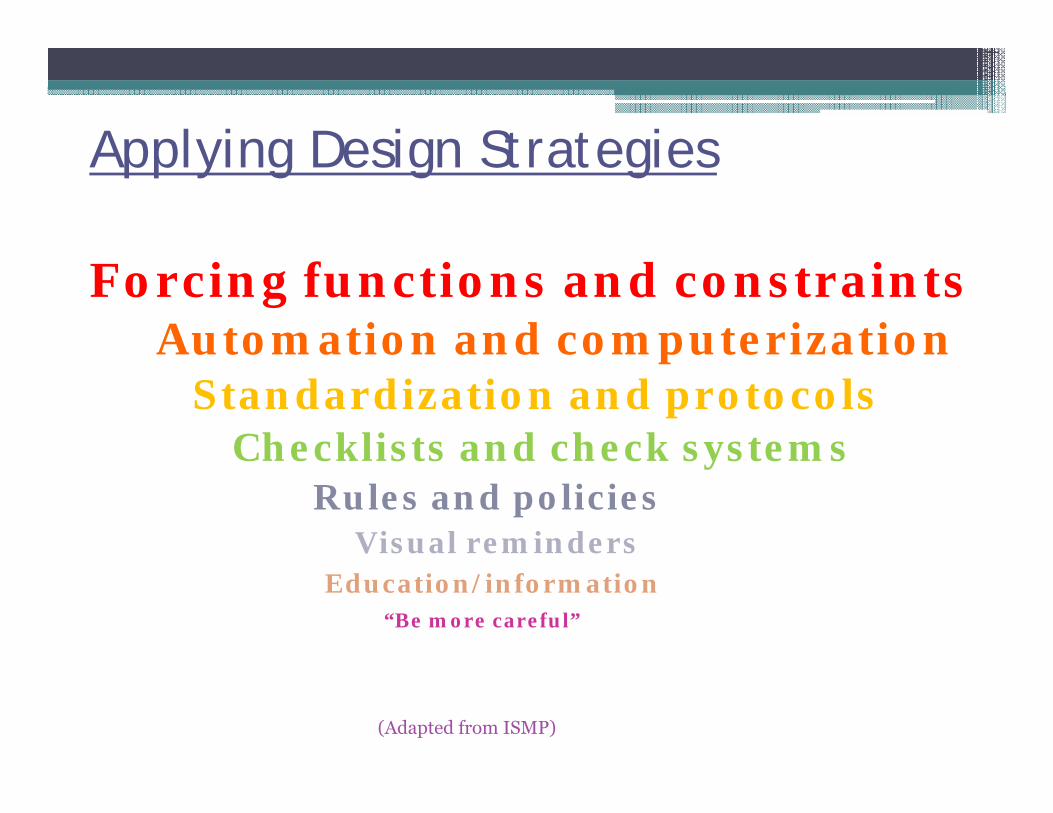
Applying Design Strategies
Forcing functions and constraintsAutomation and computerization
Standardization and protocolsChecklists and check systems
Rules and policiesVisual reminders
Education/information“Be more careful”
(Adapted from ISMP)
Case Example: Vincristine• Which of the following is the strongest strategy
for avoiding intrathecal administration?
▫ A. Warning label “fatal if given intrathecally”▫ B. Double checks by pharmacy and nursing▫ C. Dispense syringe in distinctive packaging (e.g.
double overwrap) with warning labels▫ D. Dispense as dilution in minibag

Death and neurological devastation from intrathecal vinca alkaloids:• Prepared in syringe
120• Prepared in minibag
0
ISMP 2013

Summary: Applying HFE to Your Work Environment
• Review and simplify processes.• Avoid reliance on memory.• Standardize common processes and procedures.• Make errors visible. • Use error-proof design

Concluding Comments
• It has been said that HFE is to patient safety as microbiology is to infection control...
• HFE is about the whole system: think differently!▫ People – Organization – Tasks – Environment
– Technology/Tools• T/F: One goal of HFE is to enhance safety.• T/F: I have learned something new about
human factors and medication safety today.

Assessment Questions• When human factors engineering principles are
applied to medication safety, goals include:A. Make it easy to do the right thing, and hard to do the wrong thing.B. Slow down performanceC. Maximize errorsD. Complex design
Assessment Questions
• Error prevention strategies (core principles of human factors design) include all of the following except:A. Error-proofingB. Increasing reliance on memoryC. StandardizingD. Reducing hand-offs
Assessment Questions• Three modes of human performance which relate to
human error include:A. Memory – violation – risk basedB. Discipline – accountability – compliance basedC. Skill – rule – knowledge basedD. Automation – design – checklist based

…active failures are like mosquitoes. They can be swatted one by one, but they still keep coming. The best remedies are to create more effective defences and to drain the swamps in which they breed. The swamps, in this case, are the ever present latent conditions.▫ James Reason
Human error: models and management. BMJ. 200; 320:768-770

Resources• Grout, J. Mistake-proofing the design of health care processes.
AHRQ Publication No. 07-0020. Rockville, MD. Agency for Healthcare Research and Quality; May 2007.
• Carayon P. Handbook of Human Factors and Ergonomics in Health Care and Patient Safety. Mahwah, NJ; Lawrence Erlbaum Associates Publishers; 2007.
• Larson C, Saine D. Medication Safety Officer’s Handbook. Bethesda, MD; American Society of Health-System Pharmacists; 2013.
• Reason J. Human error: models and management. Br Med J. 2000; 320:768-770.
• Graban M. Lean Hospitals: Improving Quality, Patient Safety and Employee Engagement. 2nd ed. Boca Raton FL, CRC Press; 2012.

Resources• Gregory B, Kaprielian V. Patient Safety Quality Improvement: Anatomy
of an Error. Duke Center for Instructional Technology. Available at http://patientsafetyed.duhs.duke.edu/module_e/module_overview.html Accessed October 6, 2014.
• Porto G. Safety by design: Ten lessons from human factors research. J Healthcare Risk Mng; Fall 2001.
• Green M. Safety hierarchy: Design vs. warning. Available at http://www.visualexpert.com/resources/safetyhierarchy.html. Accessed October 6, 2014.
• Gosbee J. Human factors engineering and patient safety. Qual Saf Health Care; 2002; 11:352-354.
• Scanlon M, Karsh B, Densmore E. Human factors engineering and patient safety. Pediatr Clin N Am; 2006; 53:1105-1119.

















