1 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018 SH CP 171 Learning Disabilities Services CPA Standard Operating Procedure Version: 6 Summary: This Standard Operating Procedure (SOP) defines Trust expectations and requirements for Learning Disability Services providing care planning and Care Programme Approach (CPA) in line with National CPA Standards. Keywords: Care Plan, Care Programme Approach (CPA), Care System, Care Coordinator, CPA Training. Target Audience: All staff in SHFT Learning Disabilities services. Next Review Date: February 2021 Approved & Ratified by: Learning Disabilities QSM / Mortality Meeting Date of meeting: 15 November 2017 Date issued: January 2018 Author: Diane Statham, Kimberly Ashwin, Celia Scott-Molloy, Tara Reffell, Alistair Upton Director: Mark Morgan, Director of Operations
Transcript
1 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
SH CP 171
Learning Disabilities Services CPA Standard Operating Procedure
Version: 6
Summary: This Standard Operating Procedure (SOP) defines Trust expectations and
requirements for Learning Disability Services providing care planning and Care
Programme Approach (CPA) in line with National CPA Standards.
Keywords: Care Plan, Care Programme Approach (CPA), Care
System, Care Coordinator, CPA Training.
Target Audience: All staff in SHFT Learning Disabilities services.
7. When discharging from LD Health team ............................................................................................ 8
8. Recording CPA review on RiO when other robust care planning review processes are in place ........ 8
9. Core functions and requirements of the Care Coordinator ................................................................. 9
10. Recording: Good Practice and Practicalities .................................................................................... 11
11. The CPA care plan .......................................................................................................................... 11
12. The CPA review ............................................................................................................................... 12
13. Training and Development ............................................................................................................... 12
14. Process for monitoring and compliance ........................................................................................... 12
Appendix 1 – Practicalities of CPA Review meetings .............................................................................. 13
Appendix 2 - Service User Standards for CPA review meetings ............................................................. 15
4 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
Learning Disabilities Services CPA Standard Operating Procedure
1. Introduction
This SOP provides guidance on how National CPA standards can be applied within Southern
Health NHS Foundation Trust (SHFT) LD services.
This SOP should be used as a guide and staff are reminded to apply clinical judgement and
autonomy in the pursuit of best practice. Any deviation from guidance in this SOP must be
clearly documented in the clinical record to evidence the reasoning for the deviation. It is the
clinician’s responsibility to refer to standards within their own professional groups.
The standards within this SOP have been drawn primarily from National CPA standards within
the Department of Health (2008) Refocusing the Care Programme Approach: Policy and
Positive Practice Guidance and the Care Co-ordination Association (formerly the CPAA) New
Edition Care Standards Handbook.
This SOP is written with reference to the SHFT SH CP 82 Care Planning Policy version 3 which
covers the policy and requirements for the Trust.
2. Care Programme Approach or Standard Care Planning Process
The standard care planning process applies to all service user referrals into SHFT LD Services
with the primary care planning principle that all service users will have a MDT Care Plan that
provides evidence of ongoing needs and involvement of professions within the MDT. It is the
aspiration of LD services to include Service Users in the care planning process and to provide
an accessible plan to promote service user understanding.
Whether on full CPA or standard care planning clinical work should always include assessment
and review.
Care Quality Commission (CQC) detail the need to evidence that care plans are meaningful.
They assess quality of care plans against the following criteria;
be up to date
reflect the person’s own assessment of their situation and priorities
be written in simple personally meaningful language
be created in partnership with the service user
have clearly identified actions
service users have a copy of their care plan
5 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
During the episode of care a decision guided by the level of complexity that an individual
presents with and the degree of intervention required can be made on when to use CPA.
6 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
3. Values and principles
The person is at the centre of planning
The role of families and carers is actively supported
Emphasis is placed on the service user’s strengths with the aim of ownership of their care
and promoting recovery
CPA must ensure that in delivering care consideration is given to potential inequalities and
diversity issues e.g. issues of age, religious belief, sexual orientation in service users or
their carers
All documents should be as accessible to the service user as possible
The CPA reviews can be completed in a variety of ways, and should be adapted to meet
the needs of the service user and delivery of care. The CPA review does not have to take
the form of a meeting but should include the views of all relevant parties
Information will be shared, but confidentially respected
The CPA/Care planning is an ongoing process, not just a review meeting
4. Criteria for CPA
Service users must have a degree of clinical complexity and/or risk which requires multiagency
collaboration. Staff should use clinical judgement as part of the MDT process when considering
whether to apply CPA.
Further guidance on the characteristics for CPA can be found in the Department of Health
(2008) Refocusing the Care Programme Approach: Policy and Positive Practice Guidance.
5. Characteristics to consider when deciding if support of CPA needed
The following characteristics are from the DOH 2008 Refocusing the Care Programme
Approach document. These statements act as a guide when considering to apply the CPA
process.
High degree of clinical complexity related to LD Service Clinical Areas of practice.
In addition to the refocussing document/guidance CPA as a framework must be
considered for the following factors, exploitation, mental capacity, vulnerability:
Hate/ Mate crime or discrimination
Physical / emotional abuse
Cognitive impairment affecting ability to self-care or care for others
Child protection issues
Deprivation of Liberties
Current or significant history of severe distress/instability or disengagement
7 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
Presence of non-physical co-morbidity e.g. substance/alcohol/prescription drugs misuse,
learning disability.
Multiple service provision from different agencies, including: housing, physical care,
employment, criminal justice, voluntary agencies.
Current/ recently detained under the Mental Health Act or referred to crisis/home
treatment team.
At point of significant transition or transfer of care and support
Significant reliance on carer(s) or has own significant caring responsibilities.
Experiencing disadvantage or difficulty as a result of:
Parenting responsibilities
Physical health problems/disability
Unsettled accommodation/housing issues
Employment issues when mentally ill.
Significant impairment of function due to mental illness
Discrimination (e.g. immigration status; race/cultural issues; language difficulties;
religious practices); sexuality or gender issues.
6. Who should be CPA Coordinator?
Factors to consider in deciding who should be CPA Coordinator include:
Capacity to carry out requirements of CPA and level of involvement of professionals
Member of staff who knows the services user and can work with them to include them
in the CPA process
Consideration of any particularly demanding issues which would benefit from a senior
member of the team being CPA coordinator.
Registered staff that have the appropriate level of experience and deemed competent
by their line manager.
Psychiatrists should not routinely take on the role of Care Coordinator.
6.1 Care Coordinator
The decision about who will be Care Coordinator will be reached through an MDT discussion
with consideration given to members of staff that are most familiar with the service user’s
needs. The care coordinator must be a qualified member of staff.
Change of Care Coordinator should be mutually agreed by professionals. It is best practice to
allocate the professional that knows the person the best as a care coordinator.
An alternative member of staff should take over the role if a care coordinator is off for any period
of time.
8 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
If a Care Coordinator finishes clinical work, discussion needs to take place about whether
person remains on CPA and who should be the Care Coordinator.
6.2 Intensive Support Teams, Community Forensic Teams and Hampshire Adult Mental Health in-patient services
CPA coordination should be carried out by a member of the Community LD team only if the LD
team are currently providing intervention for a related need.
Where the Community LD team, Intensive Support Teams and/or Community Forensic Services
are currently providing intervention discussion should take place to ensure the most suitable
service takes on care coordination duties.
Where required there should be a member of the Community Team to transition care on
completion of other services work.
6.3 LD Inpatient services
CPA coordination is led by in-patient team.
7. When discharging from LD Health team
On completion of Health Team involvement any remaining issues that require ongoing
coordination will need to be managed via processes within other agencies. This may take the
form of ongoing social needs reviews coordinated by Adult services.
Steps should be taken to ensure that the services user and associated services are clear when
the CPA process is complete.
When service user is on CPA with an external service this needs to be documented within the
clinical record e.g. risk summary and care plans. SHFT will receive the minutes as a participant
which must be uploaded as correspondence.
8. Recording CPA review on RiO when other robust care planning review processes are in place
CPA is a process of systematic care planning. If care planning is also part of another
comprehensive review process, such as MAPPA or Child Protection, which takes precedence
over Southern Health Trust it is acceptable with MDT agreement to ‘piggy back’ the information
from the other review onto OpenRiO as long as other requirements are met. These include
giving service user a copy of their care plan, involving the service user in the process and
coordinating the actions in a systematic way. Clinicians should use clinical judgement and
record their decisions within the OpenRiO CPA review form and with agreement from the MDT.
9 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
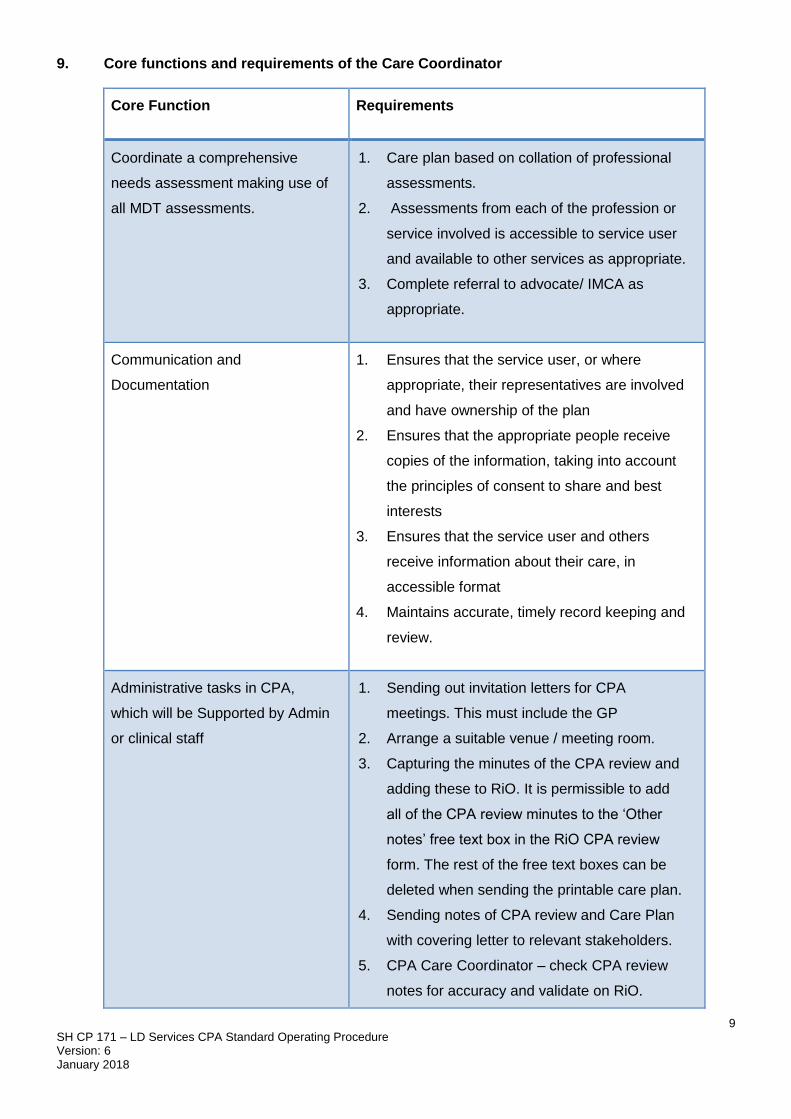
9. Core functions and requirements of the Care Coordinator
Core Function Requirements
Coordinate a comprehensive
needs assessment making use of
all MDT assessments.
1. Care plan based on collation of professional
assessments.
2. Assessments from each of the profession or
service involved is accessible to service user
and available to other services as appropriate.
3. Complete referral to advocate/ IMCA as
appropriate.
Communication and
Documentation
1. Ensures that the service user, or where
appropriate, their representatives are involved
and have ownership of the plan
2. Ensures that the appropriate people receive
copies of the information, taking into account
the principles of consent to share and best
interests
3. Ensures that the service user and others
receive information about their care, in
accessible format
4. Maintains accurate, timely record keeping and
review.
Administrative tasks in CPA,
which will be Supported by Admin
or clinical staff
1. Sending out invitation letters for CPA
meetings. This must include the GP
2. Arrange a suitable venue / meeting room.
3. Capturing the minutes of the CPA review and
adding these to RiO. It is permissible to add
all of the CPA review minutes to the ‘Other
notes’ free text box in the RiO CPA review
form. The rest of the free text boxes can be
deleted when sending the printable care plan.
4. Sending notes of CPA review and Care Plan
with covering letter to relevant stakeholders.
5. CPA Care Coordinator – check CPA review
notes for accuracy and validate on RiO.
10 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
6. Consideration should be given to asking Team
Managers or senior professionals within the
team to chair CPA meetings if they are
predicted to be complex.
7. At clinical discretion put a copy of last CPA
review in secondary record (shred previous
copy).
Risk Assessment and
Management
1. Facilitate completion of an MDT risk
assessment and ensure the management plan
is documented in the clinical record.
2. Consider safety of children that the service
user is in regular contact with.
3. Consider any Safeguarding Adults issues
4. Review and address risk issues at all
meetings as a MDT.
Crisis Planning and Management 1. Complete the crisis plan, contingency plan
and relapse prevention plan
2. Review at all meetings to ensure accuracy
3. Send out with CPA review minutes.
Assessing and responding to
carer’s needs
1. Involve carers in assessment and care
planning;
2. Ask carers if they want a ‘Carer’s Assessment’
from Adult Services if appropriate.
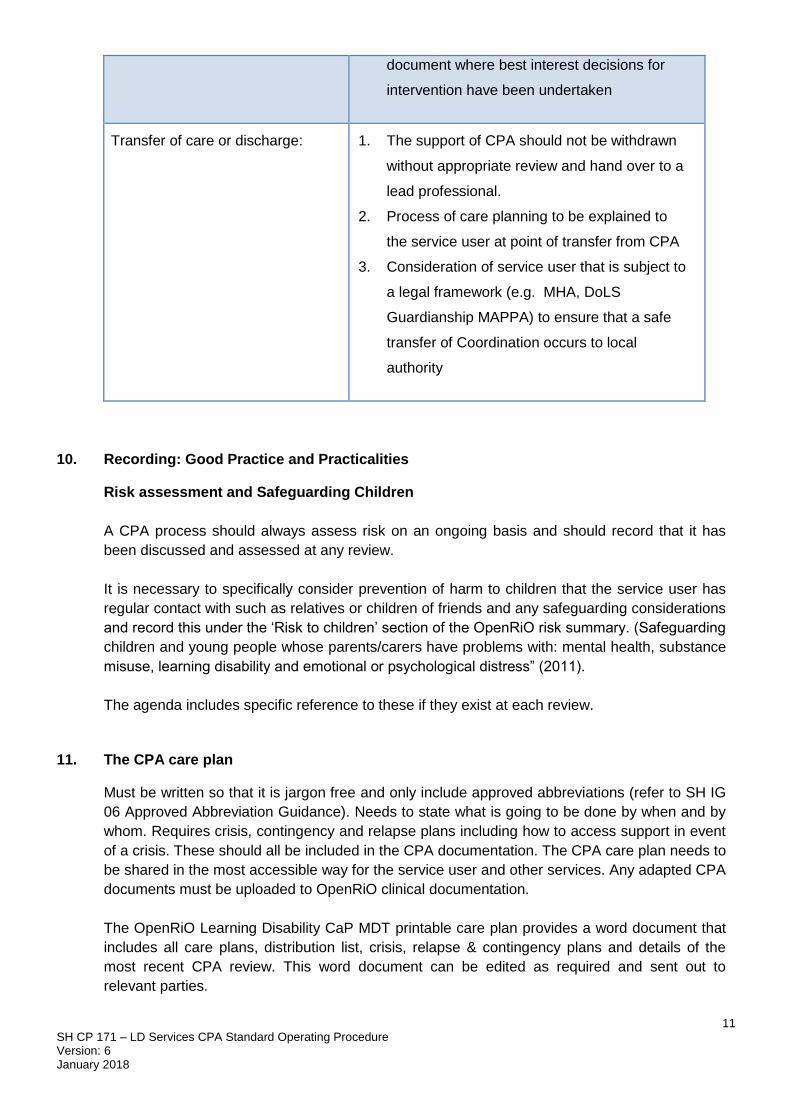
Care Planning and Review: 1. Ensure the care planning happens
2. Review the MDT care plan when needed
rather than on a fixed time schedule. At least
every 6 months
3. Review does not have to be a specific
meeting but should include the service user
4. Ensure care plans have outcomes that are
agreed with the service user or their
representative
5. Include service user in the review or
11 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
document where best interest decisions for
intervention have been undertaken
Transfer of care or discharge: 1. The support of CPA should not be withdrawn
without appropriate review and hand over to a
lead professional.
2. Process of care planning to be explained to
the service user at point of transfer from CPA
3. Consideration of service user that is subject to
a legal framework (e.g. MHA, DoLS
Guardianship MAPPA) to ensure that a safe
transfer of Coordination occurs to local
authority
10. Recording: Good Practice and Practicalities
Risk assessment and Safeguarding Children
A CPA process should always assess risk on an ongoing basis and should record that it has
been discussed and assessed at any review.
It is necessary to specifically consider prevention of harm to children that the service user has
regular contact with such as relatives or children of friends and any safeguarding considerations
and record this under the ‘Risk to children’ section of the OpenRiO risk summary. (Safeguarding
children and young people whose parents/carers have problems with: mental health, substance
misuse, learning disability and emotional or psychological distress” (2011).
The agenda includes specific reference to these if they exist at each review.
11. The CPA care plan
Must be written so that it is jargon free and only include approved abbreviations (refer to SH IG
06 Approved Abbreviation Guidance). Needs to state what is going to be done by when and by
whom. Requires crisis, contingency and relapse plans including how to access support in event
of a crisis. These should all be included in the CPA documentation. The CPA care plan needs to
be shared in the most accessible way for the service user and other services. Any adapted CPA
documents must be uploaded to OpenRiO clinical documentation.
The OpenRiO Learning Disability CaP MDT printable care plan provides a word document that
includes all care plans, distribution list, crisis, relapse & contingency plans and details of the
most recent CPA review. This word document can be edited as required and sent out to
relevant parties.
12 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
12. The CPA review
The policy explicitly states that the review is the process and not always a meeting.
Refer to appendix 1 for details of topics that need to be covered during the CPA review.
Outcomes: Each care plan should have its own outcomes agreed with the service user. These
should be Specific, Measurable, Achievable, Realistic and Timely (SMART). The care coordinator
should facilitate the review process in seeing whether these outcomes have been met.
13. Training and Development
LEAD
The courses available on LEAD website should be completed as appropriate. There is specific E-
learning about how to document CPA.
In House training
Each Team should have a CPA Champion who can deliver bespoke training to teams and
contribute to induction process including preceptorship. The CPA Champion can delegate this as
needed.
14. Process for monitoring and compliance
Learning will come from a number of sources such as audit, complaints, IMAs, CIRs, Staff
investigations, themed reviews. County Governance meetings will monitor this process and
respond to issues as required. These groups report to the Learning Disability Divisional Quality
and Safety group.
13 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
Appendix 1 – Practicalities of CPA Review meetings
Role of Care Coordinator
1. Schedule review (at least every 6 months, or more frequently according to need). Where
appropriate schedule a meeting.
2. Invite appropriate people, arrange minute taker if necessary, chair the meeting or agree an
appropriate chair.
3. Ensure service user is involved. Plan in advance how the service user will be involved, document
the reasons if not involved.
4. Ensure minutes and risk assessments are entered into RiO.
5. Ensure MDT care-plan is adjusted after the review.
6. At clinical discretion put the CPA minutes are in secondary record and shred previous minutes.
7. Ensure copies sent to relevant people, including service user.
Framework for CPA Review Agenda
(This can be modified to form an agenda)
Welcome
Introductions
Examples of Introductory script in CPA meetings
First CPA meeting
“Thank you for coming to this meeting. I am [job title] and I am chairing this meeting.
The aim of the meeting today is to discuss XXXX’s needs, to listen to each other and plan the best ways to support XXXX. Let’s start with some introductions (go round for everyone to introduce themselves).”
Further CPA Review meetings
“Thank you for coming to this meeting. I am [job title] and I am chairing this meeting.
The aim of the meeting today is to discuss XXXX’s needs, to listen to each other and review the CPA care plan to see what is working and what may need changing.”
If new people at meeting say: “Let’s start with some introductions (go round for everyone to introduce themselves).”
Set time expectations.
If necessary, explanation of why service user not present. Document.
Explanation of reason for meeting and format
Formalities – correct GP details? Correct address? Correct contact details
14 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
Service User Strengths – Record in What is going well? Rio section
Structured clinical areas that should to be covered:
- Review actions from previous meeting
- Housing/Accommodation
- Support
- Occupation incl. Activities, Employment and training
- Leisure Opportunities
- Physical, Psychological & Psychiatric Health
- Treatment/Interventions
- Friendship and family
- People to help
- Finances
- Spiritual needs
- Wishes/Aspirations
Risk assessment
- What are current risks?
- Any change to risk information?
- How will risks be managed?
- Any risks relating to children? [record in RiO]
- Any additional safeguarding issues?
Carers’ needs – any issues not already been covered? Do they need individual carer’s
assessment? If so, inform them how this will occur (e.g. who will make referral etc)
Complete/update Crisis, Contingency and Relapse plans
Remind different professionals to update their individual care plans as necessary
Is the current care planning level correct?
- Does it still require multi-professional/agency coordination or can they be
discharged to Standard Care?
Schedule next meeting
15 SH CP 171 – LD Services CPA Standard Operating Procedure Version: 6 January 2018
Appendix 2 - Service User Standards for CPA review meetings
The Following standards were devised by service user representatives from all Service User
groups in Hampshire. To create these standards the service users looked at what a CPA review
meeting is and role played good and bad CPA reviews.
Service User involved
Planning meeting with Service User
Have the right people at the meeting
Know who is coming to the meeting and be involved in deciding
An agenda with pictures and send it to Service Users in advance