This article was downloaded by: [Dalhousie University] On: 30 April 2013, At: 02:11 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Psychoactive Drugs Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/ujpd20 Leaving Methadone Maintenance Treatment: The Role of Personality Traits and Psychic Status Marlene Stenbacka a , Lena Brandt b & Louise Lettholm a a Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden b Department of Medical Epidemiology, Karolinska Institute, Stockholm, Sweden Published online: 07 Sep 2011. To cite this article: Marlene Stenbacka , Lena Brandt & Louise Lettholm (2004): Leaving Methadone Maintenance Treatment: The Role of Personality Traits and Psychic Status, Journal of Psychoactive Drugs, 36:2, 227-234 To link to this article: http://dx.doi.org/10.1080/02791072.2004.10399733 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript
This article was downloaded by: [Dalhousie University]On: 30 April 2013, At: 02:11Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Psychoactive DrugsPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/ujpd20
Leaving Methadone Maintenance Treatment: TheRole of Personality Traits and Psychic StatusMarlene Stenbacka a , Lena Brandt b & Louise Lettholm aa Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Swedenb Department of Medical Epidemiology, Karolinska Institute, Stockholm, SwedenPublished online: 07 Sep 2011.
To cite this article: Marlene Stenbacka , Lena Brandt & Louise Lettholm (2004): Leaving Methadone MaintenanceTreatment: The Role of Personality Traits and Psychic Status, Journal of Psychoactive Drugs, 36:2, 227-234
To link to this article: http://dx.doi.org/10.1080/02791072.2004.10399733
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form toanyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss, actions,claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material.
Marlene Stenbacka, Ph.D.* ; Lena Brandt, B.A. * * & Louise Lettholm, B.Sc. * * *
Abstract-This study investigates personality traits and psychiatric status among 174 methadone patients ( 12 1 men and 53 women) and 387 untreated controls ( 19 1 men and 196 women) in Sweden in 1993 and 1994. The methadone patients were followed up to 1998 with respect to being expelled from treatment. Pretreatment factors, like home background and behavioral factors, were studied in relation to treatment outcome. The methadone patients were interviewed using a structured questionnaire about alcohol and drug use and psychological, social, and behavioral factors. To obtain data about personality traits, the patients were asked to fill in a questionnaire, the Karolinska Scales of Personality (KSP) questionnaire. The male methadone patients had significantly (p < 0.0001 ) higher scores o n somatic anxiety, muscular tension, impulsiveness, and psychasthenia, and significantly lower scores with regard to socialization, social desirability, and inhibited aggression compared with the controls. Compared with the female controls, the female methadone patients differed most significantly (p < 0.000 1 ) in respect of socialization. Low socialization, social desirability, detachment, feelings of guilt, and suspicion were most predictive for later expulsion from treatment. Nearly half of the methadone patients who suffered from human immunodeficiency virus (HIV) infection had difficulties with compliance with the treatment and were later expelled. The results suggest that awareness of personality traits and psychiatric status may be crucial for a better methadone treatment outcome.
Many studies on methadone maintenance treatment in the past decades have described the effect of methadone on different outcome variables, such as opiate abuse, criminality,
tThis study was supported by the Swedish Council for Social Research (project No. 93-0128:1B) and the National Board of Health and Welfare. The authors are grateful to Anders RomelsjO, M.D., Ph.D., for valuable comments on the manuscript. Marlene Stenbacka directed the study and wrote the article. Lena Brandt analyzed the data and participated in the interpretation of the results. Louise Lettholm contributed to the writing and gave valuable comments on the manuscript.
*Project Leader, Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden.
Journal of Psychoactive Drugs 227
inpatient care, and IDV infection (Stenbacka, Leifman & Romelsjt} 2002; Ball & Ross 199 1 ; Ball et al. 1988; Dole, Nyswander & Werner 1968; Dole & Nyswander 1967, 1965).
••Statistician, Department of Medical Epidemiology, Karolinska Institute, Stockholm, Sweden.
•••Chief Psychologist, Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden.
Please address correspondence and reprint requests to Dr. Marlene Stenbacka, Karolinska Institute!, Department of Clinical Neuroscience, Magnus Huss, Karolinska Hospital, M4: 4, S-171 76 Stockholm, Sweden; email : [email protected].
Volume 36 (2), June 2004
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
02:
11 3
0 A
pril
2013
Stenbacka, Brandt & Lettbolm
Methadone treatment was first given after World War II, when it was used in outpatient programs. Today, it is common in most countries where there is heroin misuse (EMCDDA 2000; Murray 1998; Digiusto et al. 1996; Ball & Ross 199 1 ). The criteria for inclusion in a methadone treatment program in Sweden are restrictive, including at least four years of continuous intravenous use of heroin as the primary drug and being at least 20 years of age. In a 1990s survey of drug users who had been in contact with the Social Welfare Department in Stockholm, Sweden, 884 opiate abusers were identified, 220 of whom were in methadone programs and 664 of whom were untreated (Finne 1997). A greater percentage of the methadone patients (34%) than of the untreated opiate users ( 18%) had been treated for psychiatric symptoms. Also, the employment rate was higher among methadone patients than in the untreated group. A total of 23% of the methadone patients and 48% of the untreated opiate abusers were homeless. Human immunodeficiency virus (HIV) infecti0n was more frequent among methadone patients (22%) than among untreated opiate users (5%; Finne 1 997).
Studies on opiate abuse using the American Psychiatric Association's Diagnostic and Statistical Manual of
Mental Disorder, Third Revised Edition (DSM-III; APA 1980), have shown that about 70% of patients meet the criteria for at least one personality disorder other than opiate abuse (Cacciola et al . 1996; Rounsaville, Weissman & Kleber 1992; Kosten, Kosten & Rounsaville 1989; Kosten, Rounsaville & Kleber 1985). The percentage of mood disorders and antisocial personality disorders has been reported to be much higher among substance users than in the general population (Chatham et al. 1 995; Regier, Narrow & Rae 1990). Other studies have shown that several psychiatric diagnoses in substance abusers, especially major depression and antisocial personality disorder, are often associated with high rates of continued substance use and poor psychosocial improvement (Joe, Simpson & Hubbard 1991). Out of 10,000 clients who participated in a Treatment Outcome Prospective Study (TOPS) in the 1980s, 60% reported symptoms of depression in the year before admission (Hubbard et al. 1984). In another TOPS study, of 590 methadone patients recruited from 21 treatment clinics in United States, it was found that relapse to use of opiates was less frequent in patients offered treatment by mental health professionals (Joe, Simpson & Hubbard 1991).
In a study by Rutherford and colleagues ( 1995), a lower percentage of female opiate users (6.5% to 30%) than of male opiate users (40% to 50%) were reported to have antisocial personality disorders. An antisocial personality has often been associated with criminal behavior and drug use, both of which, especially criminality, appear to be less frequent among women. In an earlier study of Swedish methadone patients, criminality and intravenous drug use were more frequent among men than among women during the four years prior to admittance to treatment (Stenbacka
Journal of Psychoactive Drugs 228
Leaving Methadone Maintenance
& Romelsjo 1997), whereas the reduction of both criminality and opiate use during maintenance treatment was equally evident in both sexes (Stenbacka, Leifman & Romelsjo 2003).
How methadone patients with differing severities of psychiatric symptoms and intensities of substance use respond to treatment seems unclear (Alterman, McLellan & Shifman 1993). Alterman and colleagues ( 1993) report that among both alcoholic and drug-dependent patients, those patients with more severe mental problems received more help for medical, alcohol, family/social, and psychiatric problems and therefore had a better treatment outcome than did those with less severe mental symptoms. On the other hand, McLellan and colleagues ( 1983) found that patients who suffered less from psychiatric problems showed greater improvement in response to treatment than did those with more problems, who often did not improve at all. In a 2.5-year follow-up study of opiate users entering methadone treatment, substance use and poor psychiatric functioning were more common among patients who had personality disorders than among those who did not. No differences between the groups was found with regard to employment, family/social, legal, and medical status (Kosten, Kosten & Rounsaville 1989). Nace and Davis (1993) report that in their study, drug users with personality disorders admitted to a substance abuse program reported improvement with respect to drug use but not to either alcohol use or satisfaction with their life situation. Nurco and colleagues ( 1 989) found that persons who were more socially adjusted before starting treatment had a better prognosis for remaining in treatment. Studies on anxiety and depression have shown that the concept of identity in drug users changes dramatically during periods of abstinence (Lilja & Larsson 1996), when they experience uncertainty about the new, drug-free life situation. Avoidance of drug-using friends and places where substance abuse is common often prevents the patients from relapsing to opiates, but often also leads to feelings of loneliness, guilt, and anxiety, and even a depressive mood (Lilja & Larsson 1996).
In this study, the authors analyzed personality traits and self-reported psychiatric status among a group of methadone patients entering treatment in 1993 and 1994 and followed up in 1998 with respect to expulsion from treatment. In the analysis, two questions were addressed: ( 1 ) do methadone patients differ from the general population with regard to personality traits? and (2) do personality traits and self-reported psychiatric status have any predictive value for later expulsion from treatment?
GOALS
The goals of the study were to: ( 1 ) analyze personality traits for a group of 174 metha
done patients compared with a control group representing the general population; and
Volume 36 (2), June 2004
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
02:
11 3
0 A
pril
2013
Stenbacka, Brandt & Lettholm
(2) investigate self-reported psychiatric status and background factors in relation to expulsion from treatment.
MATERIALS AND METHODS
Subjects About half of all opiate users on methadone treatment
from all the four programs in Sweden in 1993-1994 were selected for the interview. Every second person from the list of the patients was chosen for the interview. The selection was performed according to age, gender, and time since start of treatment. One criterion was that patient should have been on methadone treatment for at least six months and were stabilized on their current methadone doses. Otherwise, the patients could suffer from different withdraw! symptoms caused by inappropriate methadone dosage. The mean methadone dosage was 80 to 90 mg/day. Trained interviewers interviewed 205 methadone patients to obtain family background and social and psychological conditions, and each interview took between one and two hours. All interviewers performed test interviews which were videotaped and analyzed by a professional who corrected obvious mistakes. The patients were also asked to fill in the Karolinska Scales of Personality (KSP) questionnaire, which measures personality traits. Thirty-one patients ( 15%) who had not filled in the questionnaires on the majority of the personality traits and psychiatric status were excluded from the study. The study population therefore consisted of 174 ( 121 men and 53 women) out of 205 methadone patients who were in treatment in 1993 and 1 994. Their average age was 37.9 years, and the average age for the men was 39.6 years. The personality traits were compared with those of an untreated control group of 1 9 1 men and 196 women representing the general population. This same group has previously been considered as a normal population and used as a control group in other studies (Gustavsson et al . 2000; Gustavsson 1 997).
Procedure Two sources of information were used: ( 1 ) the inter
views; and (2) the KSP questionnaire. The interviews were performed in 1 993 and 1 994
using a structured questionnaire about home background factors, personality, physical health, and drug and alcohol use. Questions were also asked concerning drug use among parents. The possible answers were "never," "rarely," "sometimes," and "often." The questions about psychiatric status asked whether the subjects suffered from depression, hallucinations, anxiety, suicidal thoughts, concentration problems and difficulties in controlling violence. The reply alternatives were "never," or "yes, during my lifetime," or "during the last three months." The questions were similar to those in the Addiction Severity Index questionnaire (Zanis, McLellan & Corse 1997).
Journal of Psychoactive Drugs 229
Leaving Methadone Maintenance
To obtain information about personality traits, the patients were asked to fill in the KSP questionnaire originally developed by Schalling ( 1978, 1977). The inventory is mainly a test battery initially compiled as a tool useful in research and in finding biological correlates of relevant personality traits. It consists of 135 items grouped into 15 different scales. The subject has to choose one out of four possible levels of agreement: "do not agree at all," "do not agree very well," "agree fairly well," and "agree exactly." The scales have been described in detail elsewhere (Portala et al. 2001 ; Gustavsson et al. 2000; Gustavsson 1997). The 15 scales are:
( 1 ) Socialization: the ability to identify with rules and norms in society;
(2) Impulsiveness: acting immediately; not planning, being impulsive;
(3) Avoidance of monotony: avoiding routine, needing constant change and action (seeking sensation);
(4) Psychic anxiety: worrying, low self-confidence, being sensitive;
(5) Somatic anxiety: suffering from autonomic (physical) disturbances, being restless, panicky;
(6) Muscular tension: feeling tense and stiff, not being relaxed;
(7) Detachment: avoiding involvement with others, being withdrawn;
(8) Psychasthenia: being easily fatigued and uneasy when facing new situations and tasks;
(9) Irritability: being irritable, lacking patience; (10) Verbal aggression: getting into arguments, berat
ing people when annoyed; ( 1 1 ) Indirect aggression: sulking, slamming doors when
angry; ( 1 2) Inhibited aggression: lacking the ability to speak
up and be self-assertive in social situations; ( 13) Guilt: being distressed, being ashamed of own bad
thoughts; ( 14) Suspicion: being suspicious of others; and ( 15) Social desirability: conforming socially; being
friendly, helpful, feeling the need to satisfy others. The validity of the questionnaire has been discussed
elsewhere (Gustavsson et al . 2000; Gustavsson 1 997). Gustavsson (1997) found that the KSP demonstrated stability and construct validity over time. The test-retest and internal consistency reliability has elsewhere been described as satisfactory, except for the aggression scales, which have been termed "not so satisfactory" (Bergman et al. 1983).
The study protocol was approved by the Research Ethics Committee of the Karolinska Institute in Stockholm, Sweden. The methadone patients were then recruited through means of a search of records about expulsion from treatment in the programs up to 1998. Some patients (n = 49) had difficulties in complying with treatment and were consequently expelled from the treatment, mostly due to use of drugs besides methadone or to violation of the rules of
•p < 0.05 **P < 0.01 •••p < 0.001 ••••p < 0.0001 . •••••T-test scores with the probability value (P-value). The T-test i s performed on raw points compared with the control group
according to age distribution and gender.
the program, including manipulation of the dose or urine samples. No patients voluntarily left the treatment.
Analysis of Data The association between personality trait factors and
expulsion from methadone treatment was measured with discriminant analysis and Cox regression analysis. The raw scores of the KSP were transformed into T-scores (x-mean of healthy volunteers/standard deviation (SD) of healthy controls x 10+50). The control group comprised 191 men and 196 women from the general population. Age and sex differences were taken into consideration when using T-scores.
RESULTS
The personality traits among methadone patients compared with the control group are shown in Table 1 . The male methadone patients differed most significantly from the men in the control group by scoring differently in seven out of the 15 personality traits. They had significantly (p < 0.0001 ) higher scores on somatic anxiety, muscular tension, impulsiveness, and psychasthenia and significantly lower scores in socialization, social desirability, and inhibited aggression. The female methadone patients mostly differed in single personality traits (e.g., socialization) from the women in the control group (p < 0.0001 ). Both female and male methadone patients had significantly higher (p < 0.01) scores on suspicious traits than the control group.
Journal of Psychoactive Drugs 230
By 1998, 49 (28%) patients had left the methadone maintenance treatment and four (2%) persons had died during the follow-up period (Table 2). Nearly one-third (27%) of those patients who reported alcohol or substance abuse (illicit drugs, use of sedatives and/or hypnotics, or alcohol use) among their fathers or mothers had unwillingly left treatment, compared with 38% of those who did not report family drug use. Individual problems (running away from home, problems at school, problems with friends) were frequent among the patients. Of the 94% who reported any behavioral problems, 29% were later expelled. Nearly half (43%) of those patients who had experienced separations (came from broken homes) at a young age (thee years or younger) and around one-fourth of those whose parents had separated later (when the patients were four to 15 years old) or whose families had not separated were expelled from the treatment. Sixteen out of 33 ( 48%) HIV-positive patients had difficulties with compliance with treatment. Early experience (less than 1 9 years of age) with illicit drugs was also strongly associated (59%) with being expelled from treatment.
The impact of drug-using behavior during treatment on later expulsion due to misconduct was also analyzed. It was found that nearly half (44%) of those patients who reported no decrease in, or cessation of, substance abuse during the last three months were expelled from treatment, compared with 25% of those who had no problems with discontinuing narcotic use. Cessation of, or reduction in,
TABLE 2 Background and Psychiatric Symptoms Among 174 Methadone Patients
Interviewed in 1993-1994 in Relation to Expulsion from Methadone Treatment
Background Factors Male Female Living condition
Single Married/cohabiting Other
Broken home No three years old or less four to 1 5 years
Drug use in the family* No Yes
Behavioral problems** No Yes
HIV No Yes
Age at first drug use <15 15-19 >20
Psychological Factors Depression
Never Lifetime Last three months
Anxiety Never Lifetime Last three months
Hallucinations Never Lifetime Last three months
Concentration problems Never Lifetime Last three months
Violence problems Never Lifetime Last three months
Suicidal thoughts Never Lifetime Last three months
Total (n=174) Expelled (n=49) N (%)
1 2 1 39 (32) 53 10 ( 19)
9 1 26 (29) 73 2 1 (29)
9 2 (22)
1 1 2 3 0 (27) 23 10 (43) 38 9 (24)
1 3 5 (38) 161 44 (27)
1 1 2 ( 1 8) 163 47 (29)
141 33 (23) 33 16 (48)
82 24 (30) 7 1 20 (29) 1 3 2 ( 1 5)
96 28 (29) 52 15 (29) 25 6 (24)
8 1 25 (31) 57 14 (24) 35 10 (28)
148 43 (29) 1 9 3 ( 16) 2 0
88 24 (28) 30 6 (20) 54 1 8 (33)
148 42 (28) 22 6 (27)
2 0
1 1 1 35 (32) 54 15 (28)
6 2 (33)
Note: The figures do not always add up to 174 in the left column or to 49 in the right column because of missing values. HIV=hurnan immunodeficiency virus.
*This included illicit drugs/hypnotics/sedatives and alcohol use. ••Running away from home, problems at school, and problems with friends
Journal of Psychoactive Drugs 231 Volume 36 (2), June 2004
alcohol abuse was not associated with being expelled from treatment. Very few patients reported alcohol consumption during treatment.
One-third of patients who reported concentration difficulties during the last three months were later expelled from treatment, as were one-third of patients who stated that they had had suicidal thoughts during the last three months. Among those patients (n = 77) who had ever in their lifetime or during the last three months suffered from serious depression, 27% were expelled. Many persons (n = 92) had suffered from anxiety. Of these, 24 (26%) were expelled.
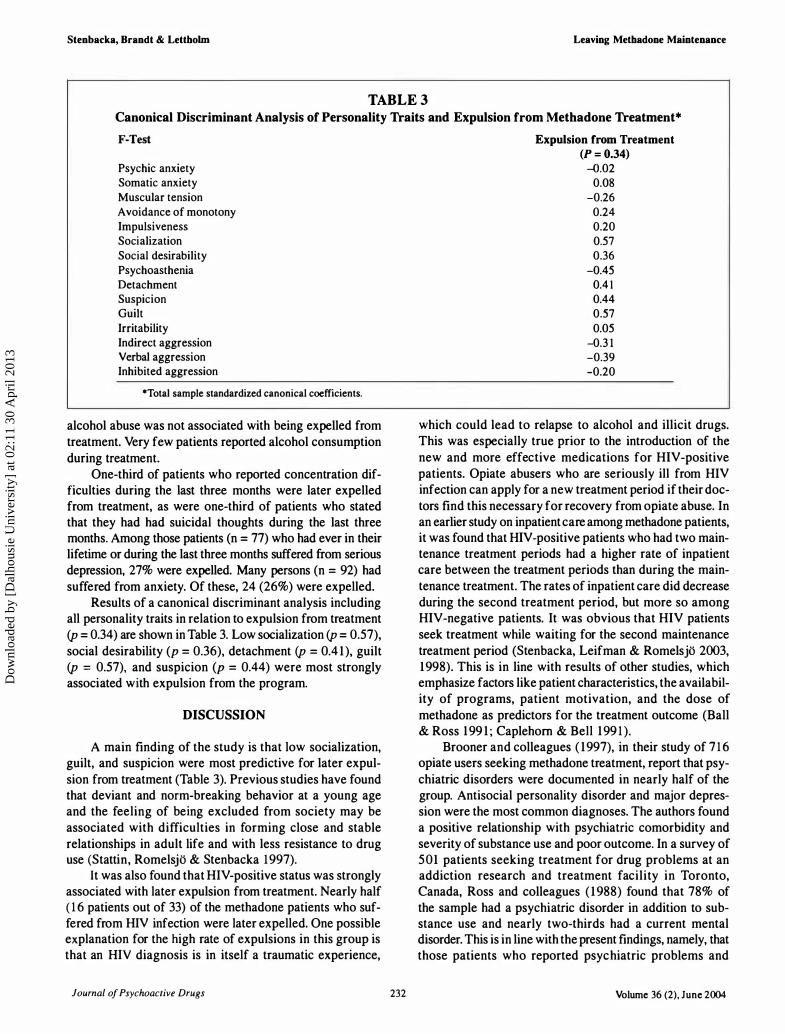
Results of a canonical discriminant analysis including all personality traits in relation to expulsion from treatment (p = 0.34) are shown in Table 3. Low socialization (p = 0.57), social desirability (p = 0.36), detachment (p = 0.4 1), guilt (p = 0.57), and suspicion (p = 0.44) were most strongly associated with expulsion from the program.
DISCUSSION
A main finding of the study is that low socialization, guilt, and suspicion were most predictive for later expulsion from treatment (Table 3). Previous studies have found that deviant and norm-breaking behavior at a young age and the feeling of being excluded from society may be associated with difficulties in forming close and stable relationships in adult life and with less resistance to drug use (Stattin, Romelsjo & Stenbacka 1997).
It was also found that HIV-positive status was strongly associated with later expulsion from treatment. Nearly half ( 1 6 patients out of 33) of the methadone patients who suffered from HIV infection were later expelled. One possible explanation for the high rate of expulsions in this group is that an HIV diagnosis is in itself a traumatic experience,
Journal of Psychoactive Drugs 232
Expulsion from Treatment (P = 0.34)
-0.02 0.08
-0.26 0.24 0.20 0.57 0.36
-0.45 0.4 1 0.44 0.57 0.05
-0.3 1 -0.39 -0.20
which could lead to relapse to alcohol and illicit drugs. This was especially true prior to the introduction of the new and more effective medications for HIV-positive patients. Opiate abusers who are seriously ill from HIV infection can apply for a new treatment period if their doctors find this necessary for recovery from opiate abuse. In an earlier study on inpatient care among methadone patients, it was found that HIV-positive patients who had two maintenance treatment periods had a higher rate of inpatient care between the treatment periods than during the maintenance treatment. The rates of inpatient care did decrease during the second treatment period, but more so among HIV-negative patients. It was obvious that HIV patients seek treatment while waiting for the second maintenance treatment period (Stenbacka, Leifman & Romelsjo 2003, 1998). This is in line with results of other studies, which emphasize factors like patient characteristics, the availability of programs, patient motivation, and the dose of methadone as predictors for the treatment outcome (Ball & Ross 199 1 ; Caplehorn & Bell 199 1 ).
Brooner and colleagues ( 1997), in their study of 7 1 6 opiate users seeking methadone treatment, report that psychiatric disorders were documented in nearly half of the group. Antisocial personality disorder and major depression were the most common diagnoses. The authors found a positive relationship with psychiatric comorbidity and severity of substance use and poor outcome. In a survey of 501 patients seeking treatment for drug problems at an addiction research and treatment facility in Toronto, Canada, Ross and colleagues ( 1 988) found that 78% of the sample had a psychiatric disorder in addition to substance use and nearly two-thirds had a current mental disorder. This is in line with the present findings, namely, that those patients who reported psychiatric problems and
Volume 36 (2), June 2004
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
02:
11 3
0 A
pril
2013
Stenbacka, Brandt & Lettholm
especially suicidal thoughts were often expelled from treatment. However, in a review of 36 studies of integrated treatment of substance abuse and psychiatric illness, it was found that programs which offered integrated treatment of both substance abuse and psychiatric illness had better treatment outcomes than did programs which treated psychiatric illness and substance abuse separately, either in time or with separate teams (Drake et al. 1998, 1997; Meuser, Drake & Wallach 1998).
Another finding was that the methadone patients had significantly higher scores on suspicious traits than the control group, which could lead to problems with cooperation with the staff of the methadone program and less trust in the counselor. One must also assume that many methadone patients, often from adolescence, have lived in criminal gangs or neighborhoods. Outside this community, the patients feel uncomfortable and stigmatized as drug users. This may affect the patients in a negative way in terms of becoming more careful with, and suspicious of, contact with the general population and the authorities. This could negatively affect treatment outcomes and rehabilitation.
The methadone patients in this study had more somatic anxiety, suffered more from muscular tension and psychasthenia, were less socialized, and had a higher tendency to impulsiveness than did the control group from the general population. One possible reason for the differences between methadone patients and the control �;roup is that the patients were not aware of their own feelings due to the effects of the methadone, which may lead to mental fatigue and difficulties in controlling impulsive behavior.
The female methadone patients differed less in personality factors from the control group than did the men. More than one-third of the women were married or cohabiting and they also often took care of the children. A clinical impression is that female methadone patients more often take responsibility for maintaining the social structure of the family, look after the children, manage the family's economy as well as the household, and make things run in a structured way. Another possible explanation, therefore, is that the female methadone patients were less involved in criminal activities and more often sought treatment for their drug use and for infectious and HIV diseases before starting maintenance treatment than the male methadone patients.
Leaving Methadone Maintenance
However, the women did have significantly lower scores in socialization than the control group. In a study by Gunne and colleagues ( 1995), 70% of 105 female heroin users were prostitutes and the rest relied on criminality to fund their own drug use. Other studies have shown that female opiate users do not directly take part in the criminal activities but often help their male counterparts by selling stolen goods, standing guard, acting as a decoy, and so on.
One problem with the study is that methadone may have an effect on the personality factors of the patients. Methadone blocks the effects of heroin and stops the craving for the substance; also, it has a pain-relieving effect. This means that the drug may have a suppressant effect on personality factors, such as muscular tension and psychic anxiety. In Sweden, however, maintenance treatment is very controlled and if patients manipulate the dosage (and sell or buy drugs) they are at risk of being expelled from the treatment. Patients in treatment programs regularly have to give plasma and urine samples for control of other substances as well as methadone.
It must be assumed that opiate abusers who apply for methadone maintenance treatment do so voluntarily and expect improvements in many respects and consequently change their drug-related behavior. Therefore, as previously mentioned, selection of presumably motivated patients who apply for methadone treatment could partly explain the good outcome of maintenance treatment (Strain et al. 1994; Maisto, McKay & Connors 1990; Magura et al. 1987). Most patients who go on treatment have previously been treated for narcomania by detoxification, often several times before the current treatment. Another explanation for the good outcome of the treatment could be that the social welfare authorities recommend methadone treatment to opiate abusers with poor living conditions or poor health status.
So far, studies have focused on medical and biological factors as being most important in relation to treatment of substance use. However, identification of psychological problems is of great value when meeting the patients' needs, especially at the beginning of the treatment period, when the dropout rate seems to be highest (Stenbacka & Romelsjt> 1997). Such identification and, possibly, treatment of psychological problems may be crucial to the patients' improvement as well as to society as a whole.
REFERENCES
Alterman, A.l.; McLellan, T. & Shifman, R.B. 1993. Do substance abuse patients with more psychopathology receive more treatment? Journal of Nervous Mental Diseases 1 8 1 : 576-82.
American Psychiatric Association (APA). 1980. Diagnostic and Statistical Manual of Mental Disorders, Revised Edition. Washington, D.C.: American Psychiatric Association.
Ball, J.C. & Ross, A. 1991 . The Effectiveness of Methadone Maintenance Treatment. New York: Springer Verlag.
Journal of Psychoactive Drugs 233
Ball, J.S.; Lange, W.R.; Meyers, C.P. & Friedman, S.R. 1988. Reducing the risk of AIDS through methadone maintenance treatment. Journal of Health and Social Behaviour 29: 214-26.
Bergman, H.; Bergman, I.; Engelbrektson, K.; Holm, L.; Johannesson, K. & Lindberg, S. 1983. Psykologhandboken. [Manual for Psychologists] Stockholm, Sweden: Magnus Huss Clinic, Karolinska Hospital.
Brooner, R.K.; King, V.L.; Kidorf, M.; Schmidt, C.W. & Biegelow, G.E. 1997. Psychiatric and substance use comorbidity among
Volume 36 (2), June 2004
Dow
nloa
ded
by [
Dal
hous
ie U
nive
rsity
] at
02:
11 3
0 A
pril
2013
Stenbacka, Brandt & Lettbolm
treatment-seeking opioid abusers. Archives of General Psychiatry 54: 7 1 -80.
Cacciola, J.S.; Rutherford, M.J.; Alterman, A.l.; McKay, J.R. & Snider, E.C. 1 996. Personality disorders and treatment outcome in methadone maintenance patients. Journal of Nervous Mental Diseases 1 84: 234-39.
Caplehom, J.R. & Bell, J. 1991. Methadone dosage and retention of patients in maintenance treatment. Medical Journal of Australia 154: 1 95-99.
Chatham, L.R.; Knight, K.; Joe, G.W. & Simpson, D.O. 1995. Suicidality in a sample of methadone maintenance clients. American Journal of Drug and Alcohol Abuse 2 1 : 345-61.
Digiusto, E. ; Seres, V. ; Bibby, A. & Batey, R. 1 996. Concordance between urinalysis results and self-reported drug use by applicants for methadone maintenance in Australia. Addictive Behaviours 2 1 : 3 1 9-29.
Dole, V.P. & Nyswander, M. 1967. Rehabilitation of the street addict. Archives of Environment Health 14 (3): 477-80.
Dole, V.P. & Nyswander, M. 1965. Medical treatment for diacetylmorphine (heroin) addiction. A clinical trial with methadone hydrochlorid. Journal of the American Medical Association 193: 80-84.
Dole, V.P. ; Nyswander, M. & Werner, A. 1968. Successful treatment of 750 criminal addicts. Journal of American Medical Association 206: 2708- 1 1 .
Drake, R.E.; Mercer-McFadden, C.; Meuser, K.T.; McHugo, G.J. & Bond, G.R. 1998. Review of integrated n•ental health and substance treatment for patients with dual disorders. Schizophrenia Bulletin 24 (4): 589-608.
Drake, R.E.; Yovetich, N.A.; Bebout, R.R.; Harris, M. & McHugo, G.J. 1997. Integrated treatment for dually diagnosed homeless adults. Journal of Nervous and Mental Disease 1 85 (5): 298-305.
European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). 2000. Reviewing Current Practice in Drug-Substitution Treatment in the European Union. EMCDDA Insights Series 3. Lisbon: EMCDDA.
Finne, E. 1 997. Statistik Over Missbrukare, HemWsa Och Psykiskt SttJrda I Stockhoklm Ar. Stockholm, Sweden: FoU-rappon.
Gunne, L.M.; Grllnbladh, L. & Ohlund, L.S. 1995. The street life and treatment response of 1 05 heroin-addicted women. In: A. Tagliamonte & I. Maremmani (Eds.) Drug Addiction and Related Clinical Problems. Wien, Austria; New York: Springer Verlag.
Gustavsson, J.P. 1997. Stability and Validity of Self-Reported Personality Traits. Stockholm, Sweden: Karolinska Institute.
Gustavsson, J.P.; Bergman, H.; Edman, G.; Ekselius, L. von Knorring, L. & Linder J. 2000. Swedish Universities Scales of Personality (SSP): Construction, internal consistency and normative data. Acta Psychiatrica Scandinavica 102 (3): 217-25.
Hubbard , R.L.; Rachal, J.V.; Craddock, S.G. & Cavanaugh, E.R. 1984. Treatment outcome prospective study (TOPS ) : Client characteristics and behaviors before, during, and after treatment. In: F.M. Tims & J.P. Ludford (Eds.) Drug Abuse Treatment Evaluation: Strategies, Progress, and Prospects. NIDA Research Monograph No. 5 1 . Rockville, Maryland, National Institute on Drug Abuse.
Joe, G.W.; Simpson, D.O. & Hubbard, R.L. 1991. Unmet service needs in methadone maintenance. International Journal on the Addictions 26: 1-22.
Kosten, T.A.; Kosten, T.R. & Rounsaville, B.J. 1989. Personality disorders in opiate addicts show prognostic specificity. Journal of Substance Abuse Treatment 6: 1 63-68.
Kosten, T.R.; Rounsaville, B.J. & Kleber, H.D. 1985. Ethnic and gender differences among opiate addicts. International Journal of Addiction 20: 1 143-62.
Lilja, J. & Larsson, S. 1996. Drug Communication. How Cognitive Science Can Help the Health Professionals. Kuopio, Finland: University Publications A. Pharmaceutical Science.
Magura, S.; Goldsmith, D.; Casriel , C.; Goldstein, P.J. & Lipton, D.S. 1987. The methadone client's self-reponed drug use. International Journal of Addiction 22: 727-49.
Journal of Psychoactive Drugs 234
Leaving Methadone Maintenance
Maisto, S.A.; McKay, J.R. & Connors, G.J. 1990. Self-reponed issues in substance abuse: State of the an and future directions. Behavioral Assessment 1 2 : 1 1 7-34.
McLellan, A.T.; Luborsky, L.; Woody, G.E.; O'Brien, C.P. & Druley, K.A. 1 983. Predicting response to alcohol and drug abuse treatments. Role of psychiatric severity. Archives of General Psychiatry 40: 620-25.
Meuser, K.T.; Drake, R.E. & Wallach, M.A. 1998. Dual diagnosis: A review of etiological theories. Addictive Behaviors 23 (6): 7 1 7-34.
Murray, J.B. Effectiveness of methadone maintenance for heroin addiction. 1 998. Psychological Reports 83: 295-302.
Nace, E.P. & Davis, C.W. 1993. Treatment outcome in substance-abusing patients with a personality disorder. American Journal of Addiction 2: 26-33.
Nurco, D.N.; Hanlon, T.E.; Kinlock, T.W. & Duszynski, K.R. 1989. The consistency of types of criminal behavior over preaddiction, addiction and nonaddiction status periods. Comprehensive Psychiatry 30: 391-402.
Ponala , K. ; Westmark, K.; Ekselius, L. & Von Knorring, L. 200 1 . Personality traits i n treated Wilson's disease determined b y means on the Karolinska Scales of Personality (KSP). European Psychiatry 16: 362-7.
Regier, D.A.; Narrow, W.E. & Rae, D.S. 1990. The epidemiology of anxiety disorders: The Epidemiologic Catchment Area (ECA) experience. Journal of Psychiatry Research 24 (Supplement 2): 3-14.
Ross, E.R.; Glaser, F.B. & Germanson, T. 1988. The prevalence of psychiatric disorders in patients with alcohol and other drug problems. Archives of General Psychiatry 45: 1023-3 1.
Rounsaville, B.J.; Weissman, M.M. & Kleber, H.D. 1 992. Heterogenity of psychiatric diagnosis in treated opiate addicts. Archives of General Psychiatry 39: 161-66.
Rutherford , M.J.; Alterman, A.l.; Cacciola, J.S. & Snider, E.C. 1995. Gender differences in diagnosing antisocial personality disorder in methadone patients. American Journal of Psychiatry 152: 1 309-1 6.
Schalling, D. 1978. Psychopathy-related personality variables and the psychophysiology of socialization. In: R.D. Hare & D. Schalling (Eds.) Psychopathic Behaviour. Approaches to Research. Chichester, U.K.: John Wiley & Sons.
Schalling, D. 1977. The trait situation interaction and the physiological correlates of behavior. In: D. Magnusson & N. Endler (Eds.) Personality at the Crossroads: Current Issues in Interactional Psychology. Hillsdale, New Jersey: Lawrence Erlbaum Associates.
Stattin, H.; Romelsjll, A. & Stenbacka, M. 1997. Personal resources as modifiers of the risk for future criminality: An analysis of protective factors in relation to 1 8-year-old boys. British Journal of Criminology 37: 198-222.
Stenbacka, M. & Romelsjll, R. 1997. Metadonbehandling i Sverige Beskrivning och Utviirdering. [Methadone Treatment in Sweden Description and Evaluation] Stockholm, Sweden: Socialstyrelsen.
Stenbacka, M.; Leifman, A. & Romelsjll, R. 2003. The impact of methadone treatment on registered convictions and arrests in HIVpositive and HIV-negative men and women with one or more treatment periods. Drug and Alcohol Review 22: 27-34.
Stenbacka, M.; Leifman, A. & Romelsjll, R. 1998. The impact of methadone on consumption of inpatient care and mortality, with special reference to HIV status. Substance Abuse and Misuse 33 ( 14) 28 19-34.
Strain, E. C.; Stitzer, M.L.; Liebson, G.E. & Bigelow, G.E. 1994. Outcome after methadone treatment: Influence of prior treatment factors and current treatment status. Drug and Alcohol Dependence 35: 223-30.
Zanis, D.A.; McLellan, A.T. & Corse, S. 1 997. Is the Addiction Severity Index a reliable and valid assessment instrument among clients with severe and persistent mental illness and substance abuse disorders? Community Mental Health 33: 2 1 3-27.