49
Medical Microbiology Immunopathology of Infectious Disease! Allen H. P ensick, Ph. D., Profes sor of Microbiology Department of Microbiology, St. George’s , , Lecture 3, Fall 2012 1

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 1/49
Medical Microbiology Immunopathology of Infectious Disease!
Allen H. Pensick, Ph. D., Professor of Microbiology Department of Microbiology, St. George’s
, ,
Lecture 3, Fall 2012
1

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 2/49
Study Hints• Keep up with reading assignments
• Attendance of Lecture or other Class activities are required.• Text: Murrary
•
• Questions will be taken at lecture but also encourage you toend questions by email to me. [email protected] with aco to cflemin s u.edu
• Study Chapter 11 Murray: Review Immunology Notesand terminology. (Ch. 12 in 6th edition)
•
• Pre Schedule appointments by calling Ms Ann MarieGeorge, or Ms Carolyn Fleming at 444-4357
•
• Sonic Foundry may not have all of the material recorded
2

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 3/49
Lecture and Study Objectives
• Explain the contribution role of the immune response in the
pathogenesis of some of the infectious diseases.
• Apply the basic concepts of the immune response as they relate to
to immune mediation of disease.
• List and describe key features of immune disorders.
• List and describe the major classes of hypersensitivity disorders.
•
immunodeficiency diseases and describe the pathogenesis of
associated diseases process.
•immune system.
• Explain the role of antigen or antibody complexes and the role they
. .
3

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 4/49
• It is important to understand the basic concepts of
Immunology and the biology of microbial
dynamics that exists between the host and the
microorganism during an infection.
• It is possible for things to go wrong during this
interactive process in which case pathology may
arise either due to failure of the immune system or
that which is mediated by the immune system.
4

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 5/49
Overview of Immunology • “ ,
physical events surrounding immune phenomena”! Simplystated, “It is The ability to tell Self Vs non self, all else istechnical detail”. Self Reco nition is an absoluterequirement for the Immune System to be successful.
• Dysfunctional immune systems can lead to disease andDeath!
– genetic aberrations of immune system – infections that destroy the immune system (e.g. HIV)
–
– senescence
– Genetics, Genomics and Immuno-genomics
• Specific Immune system has dual nature, *Humoral and CellMediated System.
5
•development of pathology.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 6/49
Immunopathology and *Infectious Disease
• Immunopathology is a branch of medicine is asubspeciality of Clinical Pathology which consists of
analysis of body fluids for detection of immune
system diseases.
• wo ma or v s ons o pa o ogy – Clinical Pathology
– .
– The role of infectious disease organisms in the
the study of the pathology of an organism , a tissue
or or an s stem or disease with res ect to the
immune system and its responses.6

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 7/49
Immunology and Its Relevance to Medicine.
• Immunopathology is a subdivision of ClinicalPathology that deals with immune responses
that are associated with disease or a pathogenic
process.
– n o ogy, re ers o amage cause o an organ smby its own immune response, as a result of an
infection.
– In its broadest sense, we can view the failure of the
immune system to respond to a disease in an
of disease.
– Recall the immune system is made up of the specific
7
and non specific divisions that interact as the immune
system.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 8/49
What are the defense mechanisms of
e mmune sys em•
called innate immunity.
• Second Line of Defense: Chemical barriers
protective cells and fluids, and in *inflammatory
response also called innate immunity.
– Inflammasone as inflammation promoter and
regulator.
• r ne o e ense: ap ve mmune
response to invaders called Specific Immunity
.
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 9/49
What are Features of Acquired Immune
Response?•
• Adaptive
•
• Has Memory
• Appropriate (respond to the invader at hand).
• -and repertoire of Ag found in the genes of the
9
.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 10/49
Recall the Dual Nature of the
n egra e mmune ys em c ema cFailure in the innate
immunopathology
Invaders must breach
The innate barriers
And be immunogenic
The host must be
Immunocompetent
To Evoke an
10
Immune Response response
Chart from Immunology: Benjamini 2nd edition

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 11/49
Immune Response-Cooperative Effector
ec an sms u y e• Complement
– ass ca a way
• IgM &IgG
– – Opsonization
– Alternative Pro erdin Pathwa
– IgM & IgG with Complement
– Lectin Pathway
• Phagocytosis enhanced by opsonins
• Increased aggressive behavior of Cellular Immunity
11

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 12/49
Complement System Acitivation (pp. 117-119 Murray) Study Slide p106 6th ed.
IgM, IgG
Mannose Binding Protein binds to
non reduced mannose, fucose
and glucosamine working to
ac va e comp emen roug
convertase
C3a-C5aÆ Inflammation
C3bÆOpsonization
Complement levels In
circulation can be used
as a diagnostic feature
of disease process.
Activated by Bacterial Cell Surfaces, componenst e.g.
Endotoxin, Microbial Polysacharrides, Aggregated IgA
12
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 13/49

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 14/49

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 15/49
What goes wrong? Why does the immune system fail to
detect non-self in microbial populations? Microbial
Pathogenesis?(Ch.19 chart 19.5; Ch. 18-p185 in 6th ed.)
• Microbial o ulations also have strate ies!
– Concealment
– Antigenic variations
– Immunosuppression
– Mimicry
– Molecular Mimicry
– Tolerization
– Gaps in host’s immune repertoire
– Up-seting the balance between antibody and
15
an responses

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 16/49
What goes wrong and why does the immune system
fail to detect non-self in microbial o ulations
Microbial Pathogenesis? (Ch.19 chart 19.5)• Microbial populations also have a strategies!
– Temporary immunosuppression by someviruses
– – Some microbes interfere with cell signalingbetween immune cells with cytotoxic T-cells,or with host responses
– Some microbes interfere with local expression
16

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 17/49
Fig 18.5 p. 187 Mur. 6th Edition
17
Figure 19-5 Bacterial mechanisms for escaping phagocytic clearance. Selected examples of bacteria that use the indicated
antiphagocytic mechanisms are given.
Downloaded from: StudentConsult (on 6 January 2006 03:46 AM)© 2005 Elsevier

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 18/49
Exotoxins As Super Antigens• -,
or gram-negative bacteria and include cytolytic enzymesand receptor-binding proteins that alter a function or kill thecell.
• Superantigens, a special group of toxins (Figure 18.3p185 6th ed). that activate T cells by binding simultaneouslyto a T-cell receptor and a major histocompatibility complex
c ass mo ecu e on anot er ce w t out requ r ngantigen.
• This nonspecific means of activating T cells can trigger life-rea en ng au o mmune- e responses y s mu a ng e
release of large amounts of interleukins, such as IL-1 andIL-2.
• u uthe activated T cells causing the loss of specific T-cellclones and their immune responses.
18
.aureus, staphylococcal enterotoxins, and the erythrogenic
toxin A or C of S. pyogenes.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 19/49
Immune Disease and Disorders; Study Slide
• Immune Disorders – Hypersensitivity
• Immunodeficiency
• Immunosuppression
– Autoimmune Disease
– Immunodeficiency
– a rogen c or organ c
• Inappropriate response
enetic or ex osure
– – Inappropriate
Response
• Failure to clear the
infectious disease agent
– Failure to Clear in the
Infectious Disease
pers s en n ec ons
.
– Failure to recognize
“self”
19

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 20/49
Immunodeficiency: Study Slide
• mmuno e c ency may
result from – genetic deficiencies
• Immunodeficiencynaturally occurs inneonates and pregnant
– starvation
– drug-inducedimmunosuppression
women.
• Deficiencies in specificprotective responses put
(e.g., steroid treatment,cancer chemotherapy
– chemotherapeutic
serious disease becauseof the infectious agents
suppress on o ssuegraft rejection)
– cancer (especially of
by that response (Murry,Table 14-8 6th 12.9 p 143).
• "natural ex eriments“mmune ce s – or disease (e.g., AIDS)
that illustrate theimportance of specificresponses in controlling
20
spec c n ec ons
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 21/49
Immunopathology and Infectious Disease
• Refers to damage to host cells by the effector systems of the immune response resulting from microbially-induced
specific and non specific immune responses.
• Immune response can be protective under some conditions,
.
– lack of an immune response (hypo)
– excessive/unlimited/uncontrolledÆ dama e h er
– Inflammasones
• Probably significant contributor and integral component of
observed signs & symptoms for many infections
21
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 22/49
Acute Phase Proteins: C-Reactive
Protein• CRP is Acute phase protein produced by liver during
n amma ory response.
• Rise is due to a rise in the plasma concentrationof IL-6, which is produced in macrophages,
- .
• C-reactive protein blood test
– Low risk < 1 mg/L
– High risk> 3 mg/L
• Patients with elevated basal levels of CRP are at anincreased risk for diabetes, hypertension or cardiovascular disease
• Exercise, lose weight, stop smoking, flaxseed,
aspirin, niacin,, statins, clean teeth
• Metabolic Syndrome (Syndrome X)
22
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 23/49
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 24/49

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 25/49
Immune Disorders;;Classification: Murray Ch. 14, p152-154
6th edition 12.7 139
Coombs Classification!
25

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 26/49
Murrary Murray Ch. 14,p.1536th ed. 12.1 p 139
Fig.l 14-11. Type Iimmediate
Requires the presence of
IgE (reaginic) Ab which
binds to the Fc rece tors
on the mast cells andBecomes a cell surface
receptor for Antigens.
This process can cause
Anaphylactic reactions
which can Life
rea en ng. e.g.reactions to Bee or Wasp
Venom).
26
Downloaded from: StudentConsult (on 6 January 2006 02:32 AM)© 2005 Elsevier

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 27/49
Type II Hypersensitivity
Fig. 14-12 Type II
6th Fig 12.12 p 140
hypersensitivity:
mediatedby antibody and
.
Complement activation
promotes direct cell
damage through the
complement cascade andby the activation
of effector cells.
Exam les are
Goodpasture's
syndrome, the response
to Rh factor in newborns,
an au o mmuneendocrinopathies. ADCC,
Antibody-dependent
cellular c totoxicit ; I ,
27
Downloaded from: StudentConsult (on 6 January 2006 02:32 AM)© 2005 Elsevier
immunoglobulin.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 28/49
-6th Fig 12-13).
hypersensitivity: immunecomplex deposition.
Immune com lexes can be
trapped in the kidney and
elsewhere in the body, can
activate complement, and
can cause other damagingresponses. Examples are
serum sickness, nephritis
assoc a e w c ron c
hepatitis B infection, and
Arthus reaction.
28
Downloaded from: StudentConsult (on 6 January 2006 03:00 AM)© 2005 Elsevier

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 29/49
Review Key Concept: Primary and
Microbial Invaders6th fig 10.5 p 106
Figure 12-7 Time course of immune responses. The primaryresponse occurs after a lag period. The immunoglobulin (Ig) M
29
.response (anamestic response ) reaches a higher titer, lastslonger, and consists predominantly of IgG.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 30/49
Antigen/Antibody Precipitatation
Rx: ptimal Proportions•
antigen and antibody must be such that each
antibody molecule can find a binding site on the
antigen at which time precipitation occurs• Antigen Excess can occur early in antibody
production making soluble antigen antibody
comlexes.
• nt o y xcess can orm so ua e ant gens.
• Deposits in the tissue can result in immune
comp ex sease;.30

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 31/49
• Nephrotic Syndrome,Renal Biopsy – IF WithAnti-IgG
•
granular. This patterncorresponds to the
deposition.
• It is the immune
stained.
31

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 32/49
Fig. 14-14 Type IV
Delayed-type
hypersensitivity (DTH)mediated by CD4 T cells
. n s case,
chemically modified self-
proteins are processed
cells, which release
cytokines (including
- -
γ]) that promote
inflammation. Other
exam les of DTH are the
6th Fig. 12.14 p 141
tuberculin response
(purified protein derivative
test)and reaction to
32
:
Downloaded from: StudentConsult (on 6 January 2006 03:00 AM)
© 2005 Elsevier
metals such as nickel.
APC, TCR, T-cell
receptor.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 33/49
Fig. 14-15 Contact and
6th Fig. 12. 15 p 143
tuberculin
hypersensitivityresponses. These type
responses are
cell mediated but differ
in the site of cell
symptoms. Contact
hypersensitivity occurs
leads to the formation of
blisters; tuberculin-type
h ersensitivit occursin the dermis and is
characterized by
swelling.
33Downloaded from: StudentConsult (on 6 January 2006 03:00 AM)
© 2005 Elsevier

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 34/49
Fig. 14-14 Type IV
Delayed-type
hypersensitivity (DTH)mediated by CD4 T cells
. n s case,
chemically modified self-
proteins are processed
cells, which release
cytokines (including
- -
γ]) that promote
inflammation. Other
exam les of DTH are thetuberculin response
(purified protein derivative
test)and reaction to
34
:
Downloaded from: StudentConsult (on 6 January 2006 03:00 AM)
© 2005 Elsevier
metals such as nickel.
APC, TCR, T-cell
receptor.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 35/49
Delayed Hypersensitivity pp. 154
•
6th fig 12.8 p 141
35
that is maximal 48 to 72 hours after injection and is indicative of prior exposure toMycobacterium tuberculosis
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 36/49
Murray Table 14.8 Infections Associated with
Defects in the Immune Res onse
6th
Table 12.9 p 142•
– Induction by physical means (e.g. burns, trauma)
– Granulocyte and monocyte defects in movement,
phagocytosis or killing or decreased numbers of cells(neutropenia)
–
– T-cells (Di George Syndrome; X-Linked IMD)
– - ’ – Combined Immunodeficiency (T and and B Cell)
pathogens.
36

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 37/49
Autoimmune Disease
• Persons are Tolerized to
self-antigens whichprevents autoimmune
lack of tolerization to specificantigens. – Autoimmune reactions result
.
• Deregulation of theimmune response may beinitiated by cross-reactivity
rom e presence oautoantibodies, activated T cells,and hypersensitivity reactions.
• People with certain MHC antigens
with microbial antigens(e.g., group Astreptococcal infection,
are at higher risk for autoimmuneresponses (e.g., HLA-B27 [humanleukocyte antigen], juvenilerheumatoid arthritis, ankylosing,
• Polyclonal activation of lymphocytes induced bytumors or infection e. .,
spondylitis).
– Responses are associated withinflammatory TH1-type
res onses.malaria, Epstein-Barr virusinfection)
– Multiple sclerosis, aninflammatory response directedagainst myelin basic protein,
37
responses to one or moreviruses, such as Human
herpesvirus 6 or measles.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 38/49
S stemic lu us er thematosus (SLE)
• chronic inflammatory
– may affect many organsystems skin, joints andinternal organs.
– e sease may e m or severe and life-threatening for most only a mild disease
– African-Americans and Asians
affected.
– Estimated 500,000 Americanhave been diagnosed with the
– 90% have Discoid rash rather the generalized SLE
38

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 39/49
Pediatric Autoimmune Neuropsychiatric
Disorders (PANDA)•
• Describes children who have obsessive
com ulsive disorder OCD and/or tic disorders
such as Tourette’s Syndrome.
• Symptoms worsen following strep. Infections
such as “strep throat” and Scarlet Fever.
• Mechanism at present: It is thought to be
similar to that of Rheumatic Fever know as
Syndenham’s Chorea or St. Vitus dance.
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 40/49

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 41/49
Hereditary Complement Deficiences(6th ed. P 143)
• Deficiencies of C1q, C1r, C1s, C4, and C2 areassociated with defects in activation of the classiccomplement pathway. – reater susce tibilit to o enic us- roducin sta h lococcal
and streptococcal infections (Figure 14-16). – These bacteria escape detection by T cells.
– A deficiency of C3 leads to a defect in activation of both theclassic and the alternative pathways, which also results in ahigher incidence of pyogenic infections.
– Defects of the properdin factors impair activation of the
– Deficiencies of C5 through C9 are associated with defectivecell killing with increased susceptibility to disseminated neisserial
41
.

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 42/49
Figure 14-16 Consequences of deficiencies
in the complement pathways6th ed Fig 12-16 p 143
. -
of deficiencies in the
complement pathways.
Factor B binds to C3b on
cell surfaces, and the
plasma serine protease D
cleaves and activates
-
alternative pathway.Factors FI and FH limit the
inappropriate activation
of complement. FH binds to
C3b and prevents
activation and is a cofactor
for FI. FI is a serine
6th ed. P 143
protease that cleaves
C3b and C4b. C1 inh,
C1 inhibitor; SLE,
42Downloaded from: StudentConsult (on 6 January 2006 03:00 AM)
© 2005 Elsevier
sys em c upus
erythematosus.
7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 43/49
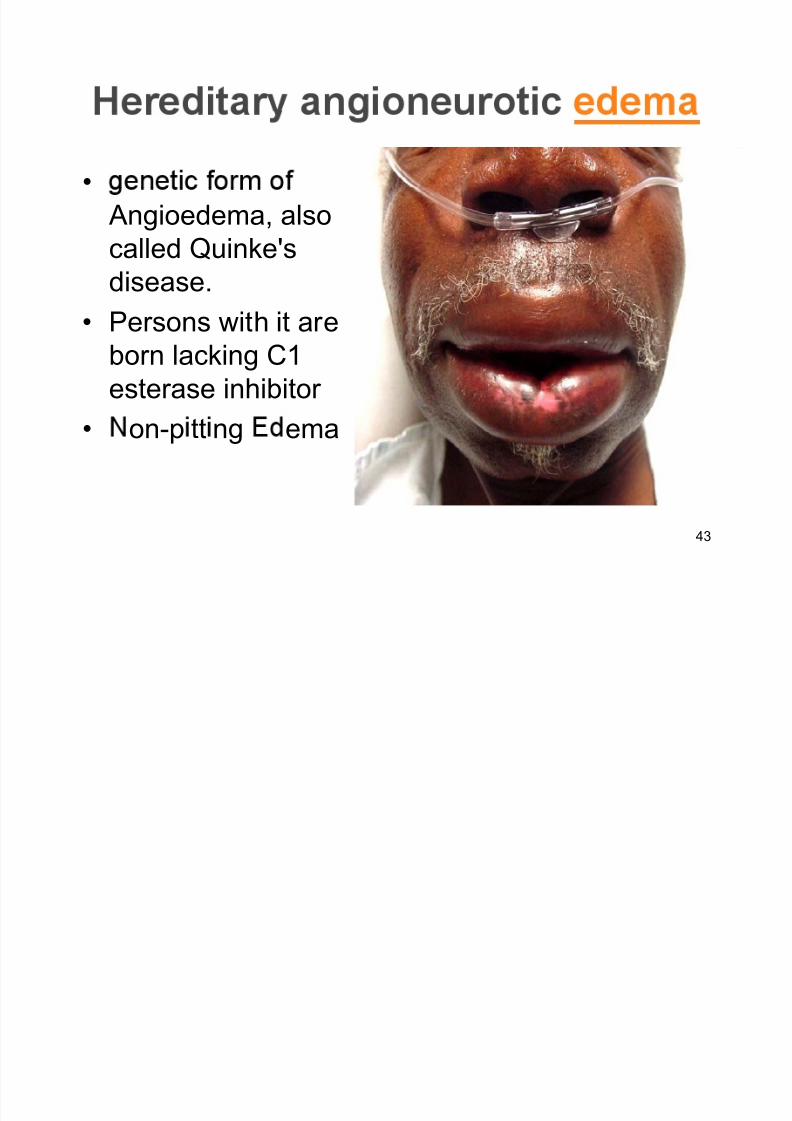
•
Angioedema, also
called Quinke's
disease.• Persons with it are
born lacking C1
esterase inhibitor
• on-p tt ng ema
43

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 44/49
Immunosuppression
• Immunosuppressive therapy is important for reducing
excessive inflammatory or immune responses of macrophages and T cells or for preventing the rejectiono ssue ransp an s y ce s. – Anti-inflammatory treatments primarily target the production
and action of TNF, IL12, and IL-1.
–
may be toxic to T cells. Soluble forms of the TNF receptor andantibody to TNF can be used to block the binding of TNF andprevent its action.
– inhibits the action or causes the lysis of T cells.
– Cyclosporin, tacrolimus and rapamycin prevent the activationof T cells. Anti-CD3 and anti-CD25 prevent activation of T cellsto prevent a response.
– Antibody Administration to costimulatory molecules such asB7 or CD40 ligand at the time of transplant can block proper T-cell activation and romote aner rather than res onsiveness.
44

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 45/49
Defective PhagocytesMurrary Page 156 (6th p 144 Fig 12-17)
• People with defective phagocytes are more susceptible to bacterial.
14-17 ).
• Chronic Granulomatous Disease in children who have diminishedlevels of cytochrome b and fail to form superoxide anions.
– Defective Oxygen-Dependent Killing. – Children have an impaired ability to oxidize NADPH and destroybacteria through the oxidative pathway. In patients with
• -immature n the bone marrow. – neutrophils from these patients can phagocytose bacteria but have
greatly diminished ability to kill them.
organisms – lack the filtration mechanism of spleen macrophages. Other deficiencies
are shown in See Murray Figure 14-17 . (Review Next Slide)
45

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 46/49
Fig. 14-17 Consequences of phagocyte
dysfunction Murrary Page 156
More Susceptible
To Bacterial Dis.
- - -
46
. . ,
phosphate dehydrogenase; Lad, leukocyte adhesion deficiency.
Downloaded from: StudentConsult (on 6 January 2006 03:00 AM)
© 2005 Elsevier

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 47/49
Creutzfeld-Jakob-Spongiform Enephalopathy
(Prion Disease) H&E Immune Failure?
47

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 48/49
• CBC Complete Blood • Agar Geloun
• ELISA;Enzyme LinkedImmunoassay and the
mmuno us on es
• Radial Immunodiffusion
• Hemagglutination
; nzymeImmunoassay
• Immunodiffusion
Inhibitition (HAI)• Hemagglutination
• Com lement Fixation• Immuno-electrophoresis
• Fluorescence ActivatedCell Sorting (Flow
Test
• Cellulose AcetateElectro horesis
y ome ry• Coombs, Direct and
Indirect
• Rh and other blood factor tests
48

7/27/2019 Lecture 03 Immunopathology 1pp Slides
http://slidepdf.com/reader/full/lecture-03-immunopathology-1pp-slides 49/49
Double Dimension Agar Gel
mmuno us on: Murray Chapter 18
• Gel Diffusion used for examination of .
• Clarified agar gel is used as a matrix for combining diffusion withprecipitation. The reactants simply
• Reactants diffuse to each other andppt.l at the equivalence points.
• Line of precipitation
49

















