Ankle Arthritis & Fusion: Open, Mini, Arthroscopic Selene G. Parekh, MD, MBA Associate Professor of Surgery Partner, North Carolina Orthopaedic Clinic Department of Orthopaedic Surgery Adjunct Faculty Fuqua Business School Duke University Durham, NC 919.471.9622 http://seleneparekhmd.com Twitter: @seleneparekhmd
Transcript
Ankle Arthritis & Fusion:Open, Mini, Arthroscopic
Selene G. Parekh, MD, MBAAssociate Professor of Surgery
Partner, North Carolina Orthopaedic ClinicDepartment of Orthopaedic Surgery
Adjunct Faculty Fuqua Business SchoolDuke University
Ankle Arthritis• Ankle is more commonly injured than any other joint in
the body
• Subject to more WB force per cm2 than any other joint
• Prevalence of ankle arthritis is 9 x’s lower than at the hip or knee
• Trauma is the most common cause• Ankle sprains, ankle fx, pilon fx …
Indications
• Arthrosis
• Pain
• Deformity
• Failed TAR
• Charcot ankle
• Degenerative Arthritis• Rheumatoid Arthritis• Post Traumatic/ Acquired Deformity• Instability from Paralytic Disorders• Neuropathic Joint• Failed Total Ankle Replacement
Goals
• To create a painless, stable, plantigrade foot
Surgical Considerations
• Minimal periosteal stripping
• Rigid internal fixation• Screws• Plates
• External fixation
• Attention to alignment and position• Plantigrade foot• 5-7 deg valgus• Neutral to 5 degrees DF• Rotation equal to other side• Posterior displacement: anterior-anterior
Preoperative Planning
• R/O subtalar DJD• May require CT scan
• May need combined fusion of both joints
Preoperative Planning
• R/O AVN talus• May require MRI
• May require bone graft
• May require tibio-calcaneal fusion
Preoperative Planning
• R/O fixed equinus
• Achilles contracture• TAL• Gastroc recession
• Anterior osteophytes• Excision of osteophytes• +/- tendoachilles lengthening
Preoperative Planning
• Varus or Valgus deformity• Plafond fracture• Talar collapse
• Bone grafting
• Osteotomy
Problems
• Nonunion rate – 0 – 40%
• Initial pain relief can be elusive
• Functional limitations• Uneven surfaces>stairs>objects from floor=driving
• Shoe modifications• SACH heel/rocker-bottom sole
• Adjacent joint degeneration• 50% arthroses within 7 yrs
Concepts
• Technical considerations– In-situ fusion
• Usually no deformity
– Deformity-correcting fusion
Concepts
• Soft tissue considerations– Avoid placing tension on skin edges
– Utilize full-thickness flaps
– Cognizant of cutaneous nerves
Surgical Principles
• Create broad, congruent cancellous surfaces• Remove all cartilage• Feather and penetrate into subchondral bone
• Use bone graft or substitutes to fill defects
• Stabilize w/ rigid fixation
• Appropriate alignment to create a plantigrade foot
Complications
• Infections– Careful soft tissue handling, removal of devitalized
tissue, prevention of hematoma
• Nerve disruption/entrapment
• Nonunion– Prepare joint, adequate fixation
• Malalignment
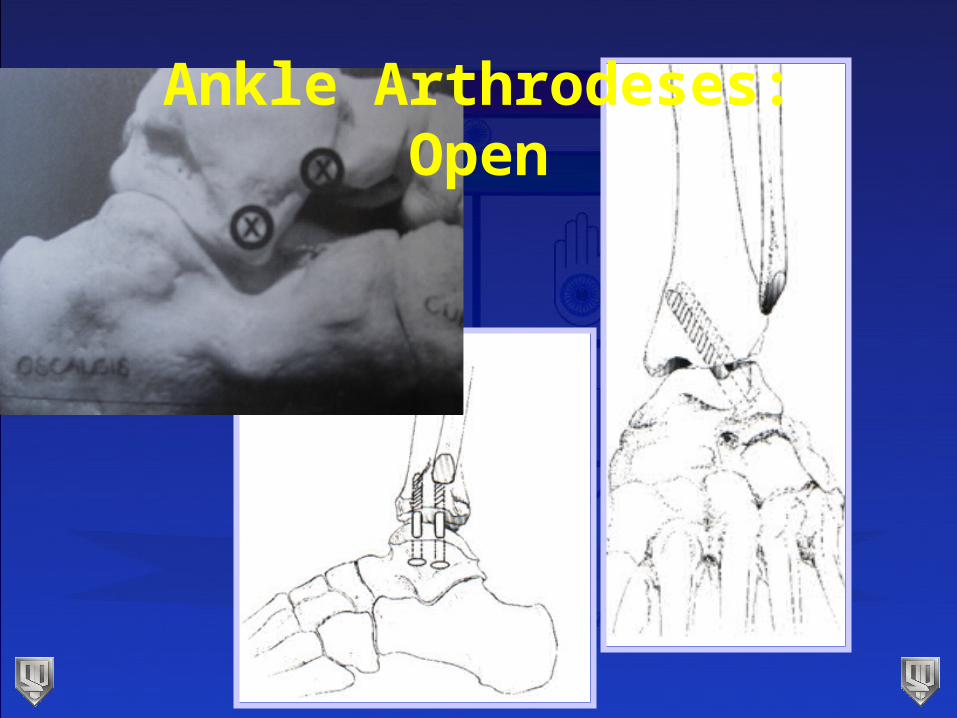
Ankle Arthrodeses
• Open
• Mini-open
• Arthroscopic-assisted
Ankle Fusions - Open
• Advantages• Easier visualization
• Ability to address deformity
• Better opposition of joint surfaces
• Disadvantages• More soft tissue dissection
Open
• Lateral/Transfibular approach• Never a TAR candidate
• Posterior• Poor anterior or lateral skin
• Anterior• All others
Open: Lateral
• Position: supine• Incision
• 10cm prox to tip of fibula base of 4th MT
• Structure at risk• Anterior branch sural n.• Peroneals
Open: Lateral
• Full thickness flaps• Periosteum of fibula stripped anteriorly and
posteriorly• Protect peroneals
Open: Lateral
• Fibular osteotomy 2cm proximal to level of joint• Proximal-lateral• Distal-medial