Lecture 62 Headache Therapeutics Reardon GOALS OF THERAPY: • Treat attacks rapidly & consistently, and prevent recurrence • Restore the pt’s ability to function • Minimize the use of backup and rescue medications • Optimize self-care and reduce subsequent use of resources • Have minimal or no adverse effects • Be cost-effective in overall management APPROACH TO TREATMENT: • Take medications as early as possible when HA pain starts • Select non-oral route of admin for pts whose migraines present early with sig. N&V • Not all agents work in all pts and not all agents work in the same pt all the time • Use a stratified treatment approach • Provide plan for “backup” or “rescue therapy” • Encourage use of headache diary • Guard against medication overuse headache NON-PHARMACOLOGIC MANAGEMENT: • Identify and avoid triggers o Lifestyle consistency: sleep, diet, hydration, caffeine, alcohol, exercise, stress • Application of cold/pressure • Rest/stimulus deprivation • Relaxation training, biofeedback, CBT • Acupuncture, physiotherapy, chiropractic ACUTE MIGRAINE TREATMENT: SIMPLE ANALGESICS (ASA, ACETAMINOPHEN, NSAIDS): Migraines • Reasonable first line choices for treatment of mild-moderate migraine attacks • Not good if pt is vomiting, but could combine with antiemetic • ASA + metoclopramide may be as effective as sumatriptan for mild-mod attacks Tension • First line +/- caffeine Cluster • No role TRIPTANS: Migraines • First line for moderate-severe attacks Tension • Usually no role, may have benefit in patient with co-morbid migraines Cluster • Sumatriptan subcut first line Efficacy • Individual response varies considerably • If pt fails a triptan, they can often be successfully switched to another Admin • Consider subcut/nasal in pts who desire more rapid relief, have nausea, or fast onset of migraine • May be synergy between NSAIDs and triptan • If recurrence, repeat dose Safety re: MI • Caution with CVD, but note no studies show increased risk of MI Drug interactions Triptans • Can’t use within 24h of dihydroergotamine (additive vasoconstriction) • Because PRN, other theoretical interactions unlikely to be clinically significant Frovatriptan, zolmitriptan CYP1A2: cimetidine Eletriptan CYP3A4: fluconazole, ketoconazole, erythromycin, verapamil Serotonin syndrome • Potentially life-threatening condition associated with increased CNS serotonergic activity o Mental status changes, tachycardia, hyperthermia, NVD, hyperreflexia, incoordination o Typically min-hrs after initiation/ dose increase in serotonergic drugs • Selective action on 5HT1B/D = remote possibility o NOTE: routinely in combo with SSRIs/ SNRIs (depression/anxiety meds) • Educate pts – stop triptan & seek medical help if symptoms occur DIHDROERGOTAMINE: Migraines • Mod-severe pain if triptans not an option • Status migrainosus (migraine lasting >72h) Tension • No role Cluster • May be effective (IV) as second-line option Admin • Nasal spray or IV/subcut • Co-admin with antiemetic to reduce nausea Efficacy • DHE IN less effective than sumitriptan IN • Subcut similar to sumatriptan subcut o DHE slower onset but fewer recurrences • Role in treating medication withdrawal HA Drug Interaction • Can’t use within 24h of triptan (additive vasoconstriction) • Avoid use with potent CYP3A4 inhibitors: cimetidine, clarithromycin, erythromycin, efavirenz, ritonavir, itraconazole, ketoconazole ANTIEMETICS: Migraines • PO or IV as adjunct with simple analgesics or migraine specific therapy • IV for aborting migraine (usually hospital) Tension • Limited role • Small, low-quality trials suggest potential role for IV metoclopramide, chlorpromazine to abort headache Cluster • Not part of standard management • May be effective when given IV Oral use • Adjuncts for nausea, increasing gastric motility to facilitate absorption of abortive therapies IV use • Monotherapy for aborting migraines • Dimenhydrinate ineffective for this OPIOIDS: • LAST RESORT • More likely to experience recurrent headache within 7 days MONITORING PARAMETERS: Efficacy Acute attacks • Pain (0-10) at 1h (subcut, IN), 2 h (oral formulations) • Resolution of N,V and other associated symptoms • Resolution of attack Acute med use • Reduced • Under threshold for medication overuse MIDAS score • 50% reduction in frequency and/or severity of HA QOL/fxn • As per individual pt goals Safety • Medication side effects
Transcript
Lecture 62 Headache Therapeutics Reardon
GOALS OF THERAPY:
• Treat attacks rapidly & consistently, and prevent recurrence
• Restore the pt’s ability to function
• Minimize the use of backup and rescue medications
• Optimize self-care and reduce subsequent use of resources
• Have minimal or no adverse effects
• Be cost-effective in overall management
APPROACH TO TREATMENT:
• Take medications as early as possible when HA pain starts
• Select non-oral route of admin for pts whose migraines present early with sig. N&V
• Not all agents work in all pts and not all agents work in the same pt all the time
• Use a stratified treatment approach
• Provide plan for “backup” or “rescue therapy”
• Encourage use of headache diary
• Guard against medication overuse headache
NON-PHARMACOLOGIC MANAGEMENT:
• Identify and avoid triggers o Lifestyle consistency: sleep, diet, hydration, caffeine,
alcohol, exercise, stress
• Application of cold/pressure
• Rest/stimulus deprivation
• Relaxation training, biofeedback, CBT
• Acupuncture, physiotherapy, chiropractic
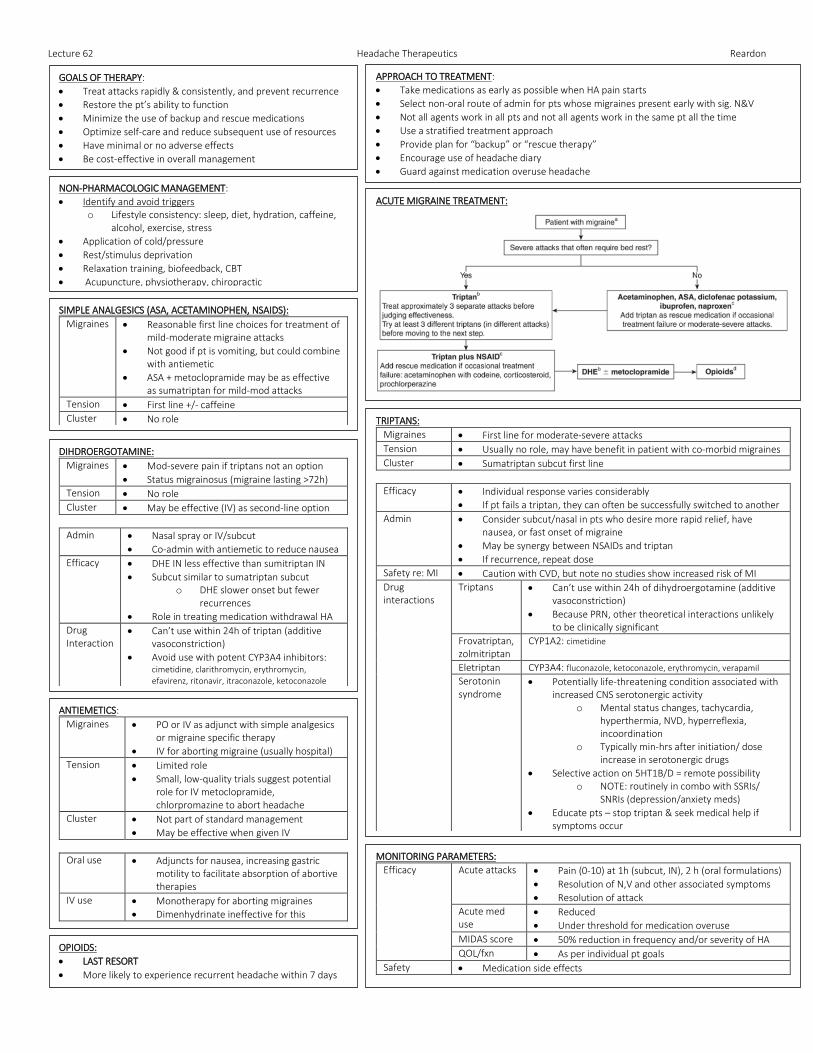
ACUTE MIGRAINE TREATMENT:
SIMPLE ANALGESICS (ASA, ACETAMINOPHEN, NSAIDS):
Migraines • Reasonable first line choices for treatment of mild-moderate migraine attacks
• Not good if pt is vomiting, but could combine with antiemetic
• ASA + metoclopramide may be as effective as sumatriptan for mild-mod attacks
Tension • First line +/- caffeine
Cluster • No role
TRIPTANS:
Migraines • First line for moderate-severe attacks
Tension • Usually no role, may have benefit in patient with co-morbid migraines
• Potentially life-threatening condition associated with increased CNS serotonergic activity
o Mental status changes, tachycardia, hyperthermia, NVD, hyperreflexia, incoordination
o Typically min-hrs after initiation/ dose increase in serotonergic drugs
• Selective action on 5HT1B/D = remote possibility o NOTE: routinely in combo with SSRIs/
SNRIs (depression/anxiety meds)
• Educate pts – stop triptan & seek medical help if symptoms occur
DIHDROERGOTAMINE:
Migraines • Mod-severe pain if triptans not an option
• Status migrainosus (migraine lasting >72h)
Tension • No role
Cluster • May be effective (IV) as second-line option
Admin • Nasal spray or IV/subcut
• Co-admin with antiemetic to reduce nausea
Efficacy • DHE IN less effective than sumitriptan IN
• Subcut similar to sumatriptan subcut o DHE slower onset but fewer
recurrences
• Role in treating medication withdrawal HA
Drug Interaction
• Can’t use within 24h of triptan (additive vasoconstriction)
• Avoid use with potent CYP3A4 inhibitors: cimetidine, clarithromycin, erythromycin, efavirenz, ritonavir, itraconazole, ketoconazole
ANTIEMETICS:
Migraines • PO or IV as adjunct with simple analgesics or migraine specific therapy
• IV for aborting migraine (usually hospital)
Tension • Limited role
• Small, low-quality trials suggest potential role for IV metoclopramide, chlorpromazine to abort headache
Cluster • Not part of standard management
• May be effective when given IV
Oral use • Adjuncts for nausea, increasing gastric motility to facilitate absorption of abortive therapies
IV use • Monotherapy for aborting migraines
• Dimenhydrinate ineffective for this
OPIOIDS:
• LAST RESORT
• More likely to experience recurrent headache within 7 days
MONITORING PARAMETERS:
Efficacy Acute attacks • Pain (0-10) at 1h (subcut, IN), 2 h (oral formulations)
• Resolution of N,V and other associated symptoms
• Resolution of attack
Acute med use
• Reduced
• Under threshold for medication overuse
MIDAS score • 50% reduction in frequency and/or severity of HA
QOL/fxn • As per individual pt goals
Safety • Medication side effects
Lecture 62 Headache Therapeutics Reardon
MEDICATION OVERUSE HEADACHE:
DIAGNOSIS: A. Headache occurring on ≥ 15 days per month in a patient with
a pre-existing headache disorder B. Regular overuse for >3 months of one or more drugs that can
be taken for acute and/or symptomatic treatment of headache
• Triptans 10-14 HA days/month
• Opioids: 8 days/month
• Barbiturates: 5 days/month
• Simple analgesics >14 days/month (protective if <10d/m) C. Not better accounted for by another diagnosis Suggested that highest risk if with opioids, butalbital compounds and ASA/acetaminophen/caffeine combos
MANAGEMENT:
• Stop offending agent o Taper if opioids or barbiturate o May stop cold turkey if triptans/simple analgesics
• Manage withdrawal according to agent o Bridge with NSAID or prednisone
• Educate pts that HA likely will get worse before getting better
• Start appropriate prophylaxis
HOSPITAL ADMISSION FOR MIGRAINE:
• Treatment of severe nausea, vomiting and subsequent dehydration
• Treatment of severe, refractory migraine pain (status migrainosus)
• Detoxification from overuse of combo analgesics, ergots or opioids
PREVENTION:
INDICATIONS:
• Contraindication/failure acute abortive therapy
• Use of abortive medication > twice per week
• Risk of medication overuse headache
• Frequent or long-lasting migraine headaches
• Significant disability or diminished QOL despite appropriate acute treatment
• Menstrual migraines
APPROACH TO TREATMENT:
• Optimize non-pharmacologic interventions
• Choice depends on co-morbidities, patient-specific factors
• Preventive medications are considered effective if the frequency and/or monthly headache days and/or severity of attacks are reduced by ≥ 50%
• Titrate meds over a few weeks o Start low and titrate up to minimize side effects o Allow 4-8 weeks for benefit once at target dose
▪ Adequate trial is 2-3 months at reasonable dose
• Reasonable to leave on prophylactic therapy for 6-12 months, then consider slowly tapering off with monitoring for worsening headaches
PREVENTIVE MEDICATIONS:
BBs • Propranolol > placebo
CCBs • Flunarizine, verapamil o Old studies, gaps in reporting o Weak, conflicting data
• Verapamil = CYP3A4 inhibition
TCAs • Amitriptyline o First line option based on decades of clinical
experience (limitations of available data) o Non-inferior vs. topiramate
• Nortriptyline may be considered due to lower risk of anticholinergic SEs, however not studied for migraine
Anti-convulsants
• Sodium valproate, divalproex sodium, gabapentin
• Topiramate caused paresthesia o Potential for oral contraceptive failure (unlikely at
• Severe nausea: metoclopramide or prochlorperazine
Prophylaxis • Propranolol, magnesium
Lactation Acute • Acetaminophen 1st line
• Ibuprofen NSAID of choice
• Antiemetics = safe
• Sumatriptan if migraines refractory
Prophylaxis • Propanol, magnesium (1st line)
• Divalproex/valproic acid = compatible
Lecture 62 Headache Therapeutics Reardon
OTHER HEADACHES:
Peri-menopausal /hormonal
• Migraines typically worsen initially (erratic menstrual cycles, disturbed sleep)
• With menopause, migraines may improve
• Acute treatment remains standard
• Hormone replacement may be considered for prevention depending on risk:benefit analysis (but no evidence)
Post-traumatic HA
• HA developing within 7 days of injury or after regaining consciousness post injury
• Mixed headache types: migraine, tension, other features
• Paucity of data to guide treatment; often treat as primary headache type based on clinical features o Standard acute treatment o Prophylaxis determined case by case











![ClaPD (Clarithromycin/[Biaxin®], Pomalidomide ...static9.light-kr.com/documents/Mark - ASH 2012 - Clarithromycin...SPEAKER: Tomer Mark MD, MSc ... PD 10 (10) IMWG, ... • The addition](https://static.documents.pub/doc/80x56/5aaaed457f8b9a95188eb76b/clapd-clarithromycinbiaxin-pomalidomide-ash-2012-clarithromycinspeaker.jpg)






