Left Atrial Segmentation from 3D Respiratory- and ECG-gated Magnetic Resonance Angiography Rashed Karim 1(B ) , Henry Chubb 1 , Wieland Staab 3 , Shadman Aziz 1 , R. James Housden 1 , Mark O’Neill 1,2 , Reza Razavi 1,2 , and Kawal Rhode 1 1 Department of Biomedical Engineering, King’s College London, London, UK [email protected]2 Department of Cardiology, Guy’s and St. Thomas’ NHS Foundation Trust, London, UK 3 Department of Cardiology and Pneumology, University of G¨ottingen, G¨ottingen,Germany Abstract. Magnetic resonance angiography (MRA) scans provide excel- lent chamber and venous anatomy. However, they have traditionally been acquired in breath-hold and are not cardiac-gated. This has made it diffi- cult to use them in conjunction with late gadolinium enhancement (LGE) scans for reconstructing fibrosis/scar on 3D left atrium (LA) anatomy. This work proposes an image processing algorithm for segmenting the LA from a novel MRA sequence which is both ECG-gated and respiratory- gated allowing reliable 3D reconstructions with LGE. The algorithm implements image partitioning using discrete Morse theory on digital images. It is evaluated in the context of creating 3D reconstructions of scar/fibrosis with LGE. Keywords: Image segmentation · Delayed-enhancement MRI · Mag- netic resonance angiography · Left atrium 1 Introduction Cardiac magnetic resonance (CMR) has evolved in the last two decade as a tech- nique for non-invasive assessment of cardiac anatomy and function. The focus has primarily been on the ventricles. Recent advancements in CMR techniques have made it possible to investigate the atria. There has been increasing inter- est to image the left atrium (LA) to derive biomarkers that are relevant to the management of atrial fibrillation. One such biomarker is fibrosis/scar pre- and post- ablation therapy. The gold standard method is to use late gadolinium enhancement (LGE) imaging. In this imaging sequence, the wash-out kinetics of the contrast agent within the fibrosis/scar regions allows it be imaged. Accurate assessment of left atrial myocardial fibrosis/scar size and anatomy with LGE is challenging. The 3D reconstructions of fibrosis/scar on LA anatomy can be obtained for this purpose. A shape-based segmentation of c Springer International Publishing Switzerland 2015 H. van Assen et al. (Eds.): FIMH 2015, LNCS 9126, pp. 155–163, 2015. DOI: 10.1007/978-3-319-20309-6 18
Transcript
Left Atrial Segmentation from 3D Respiratory-and ECG-gated Magnetic Resonance
Angiography
Rashed Karim1(B), Henry Chubb1, Wieland Staab3, Shadman Aziz1,R. James Housden1, Mark O’Neill1,2, Reza Razavi1,2, and Kawal Rhode1
1 Department of Biomedical Engineering, King’s College London, London, [email protected]
2 Department of Cardiology, Guy’s and St. Thomas’ NHS Foundation Trust,London, UK
3 Department of Cardiology and Pneumology, University of Gottingen,Gottingen, Germany
Abstract. Magnetic resonance angiography (MRA) scans provide excel-lent chamber and venous anatomy. However, they have traditionally beenacquired in breath-hold and are not cardiac-gated. This has made it diffi-cult to use them in conjunction with late gadolinium enhancement (LGE)scans for reconstructing fibrosis/scar on 3D left atrium (LA) anatomy.This work proposes an image processing algorithm for segmenting the LAfrom a novel MRA sequence which is both ECG-gated and respiratory-gated allowing reliable 3D reconstructions with LGE. The algorithmimplements image partitioning using discrete Morse theory on digitalimages. It is evaluated in the context of creating 3D reconstructions ofscar/fibrosis with LGE.
Cardiac magnetic resonance (CMR) has evolved in the last two decade as a tech-nique for non-invasive assessment of cardiac anatomy and function. The focushas primarily been on the ventricles. Recent advancements in CMR techniqueshave made it possible to investigate the atria. There has been increasing inter-est to image the left atrium (LA) to derive biomarkers that are relevant to themanagement of atrial fibrillation. One such biomarker is fibrosis/scar pre- andpost- ablation therapy. The gold standard method is to use late gadoliniumenhancement (LGE) imaging. In this imaging sequence, the wash-out kinetics ofthe contrast agent within the fibrosis/scar regions allows it be imaged.
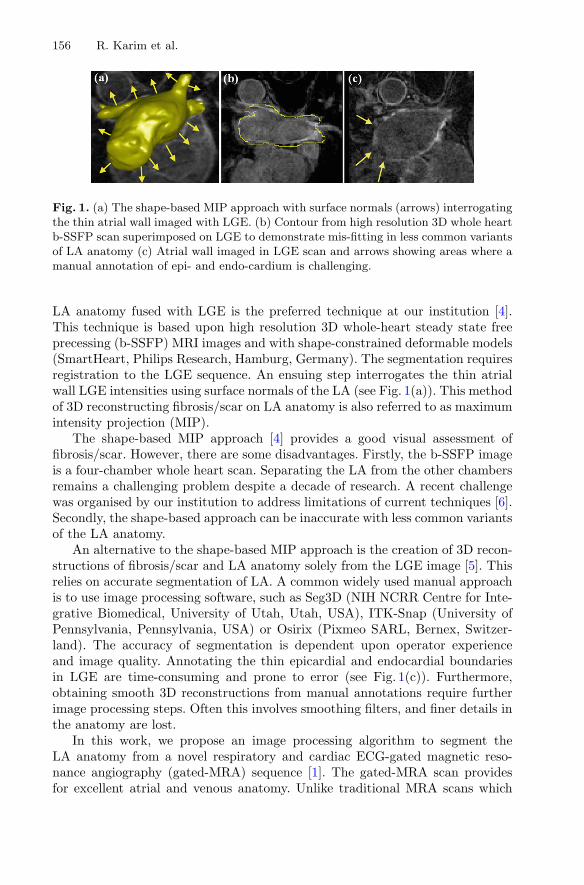
Fig. 1. (a) The shape-based MIP approach with surface normals (arrows) interrogatingthe thin atrial wall imaged with LGE. (b) Contour from high resolution 3D whole heartb-SSFP scan superimposed on LGE to demonstrate mis-fitting in less common variantsof LA anatomy (c) Atrial wall imaged in LGE scan and arrows showing areas where amanual annotation of epi- and endo-cardium is challenging.
LA anatomy fused with LGE is the preferred technique at our institution [4].This technique is based upon high resolution 3D whole-heart steady state freeprecessing (b-SSFP) MRI images and with shape-constrained deformable models(SmartHeart, Philips Research, Hamburg, Germany). The segmentation requiresregistration to the LGE sequence. An ensuing step interrogates the thin atrialwall LGE intensities using surface normals of the LA (see Fig. 1(a)). This methodof 3D reconstructing fibrosis/scar on LA anatomy is also referred to as maximumintensity projection (MIP).
The shape-based MIP approach [4] provides a good visual assessment offibrosis/scar. However, there are some disadvantages. Firstly, the b-SSFP imageis a four-chamber whole heart scan. Separating the LA from the other chambersremains a challenging problem despite a decade of research. A recent challengewas organised by our institution to address limitations of current techniques [6].Secondly, the shape-based approach can be inaccurate with less common variantsof the LA anatomy.
An alternative to the shape-based MIP approach is the creation of 3D recon-structions of fibrosis/scar and LA anatomy solely from the LGE image [5]. Thisrelies on accurate segmentation of LA. A common widely used manual approachis to use image processing software, such as Seg3D (NIH NCRR Centre for Inte-grative Biomedical, University of Utah, Utah, USA), ITK-Snap (University ofPennsylvania, Pennsylvania, USA) or Osirix (Pixmeo SARL, Bernex, Switzer-land). The accuracy of segmentation is dependent upon operator experienceand image quality. Annotating the thin epicardial and endocardial boundariesin LGE are time-consuming and prone to error (see Fig. 1(c)). Furthermore,obtaining smooth 3D reconstructions from manual annotations require furtherimage processing steps. Often this involves smoothing filters, and finer details inthe anatomy are lost.
In this work, we propose an image processing algorithm to segment theLA anatomy from a novel respiratory and cardiac ECG-gated magnetic reso-nance angiography (gated-MRA) sequence [1]. The gated-MRA scan providesfor excellent atrial and venous anatomy. Unlike traditional MRA scans which
Left Atrial Segmentation from Gated-MRA 157
Fig. 2. A flow diagram showing the steps in the proposed algorithm.
are not cardiac-gated and acquired in breath-hold, they require registration tothe LGE image sequence. With cardiac ECG-gating, both the gated-MRA andLGE images can be acquired in the same cardiac cycle, requiring no registration.With the proposed technique, the 3D reconstructions of fibrosis/scar and LA canbe obtained with greater reliability than previous mentioned works.
2 Methods
2.1 Image Acquisition
All patients in this study (n = 7) were scanned on a commercial 1.5T IngeniaMRI scanner (Philips Healthcare, The Netherlands). Electrocardiographic elec-trodes were positioned for optimal gating before the study. A free breathing,contrast enhanced MRA using an ECG triggered, respiratory gated, inversionrecovery prepared, 3D image sequence was acquired. The acquisition was started90 s after initiation of an intravenous infusion of Gadolinium (Gadovist, Bayer,Germany) at a rate of 0.3 ml/s. The reconstructed image pixel resolution was:1 × 1 × 2 mm and typically 50 slices to cover the whole of the LA. A standard3D LGE sequence was also performed using the same gating parameters. Thereconstructed image pixel resolution was: 0.6 × 0.6 × 2 mm and 45–50 slices.
2.2 Algorithm
The steps involved in the proposed algorithm are shown as a flow diagram inFig. 2. The algorithm exploits Morse partitions of the image. In Morse theory,the topology of sub-level sets of real-valued functions is connected to its criticalpoints. In binary images, real-valued functions can be derived from the distancetransformation, and the sub-level set consists of all voxels x where f(x) ≤ c. Theproposed algorithm partitions and thus segments the LA by exploiting the basins
158 R. Karim et al.
surrounding the local maxima of f(x). This is closely related to the watershedtransform. In this work, the topology was defined by considering all voxels to beconnected to its immediate neighbours (i.e. 26-neighbourhood or cubical com-plex). The algorithm was comprised of three steps: (1) Otsu region growing,(2) Morse partitioning, and (3) partition selection. Each step is herewithdescribed in detail.
In the Otsu region growing step, a connected region was obtained from auser-selected seed point and region of interest (ROI). The threshold in the Otsustep was computed on the gated-MRA image; it is the optimal intensity whichpartitions the image into two tissue classes. This was ideal in gated-MRA wherethere is a high contrast between blood and surrounding structures. The Otsustep generated a well-connected binary mask containing the LA and surroundingchambers.
In the Morse partitioning step illustrated in Fig. 3, the distance transformf(x) for the Otsu binary region was computed, where for every voxel x, f isthe real-valued distance to the closest zero voxel. The local maxima of f wascomputed in an ensuing step. Basins surround each local maximum point in f.These basins are defined as voxels from which a path to the maxima exists. Thispath is the gradient flow φ(x, t) of f, where:
φ(x, 0) = x
∂
∂tφ(x, t) = ∇f(φ(x, t))
Each basin is a Morse partition B surrounding a critical point (i.e. local maxi-mum) p:
Bp = {x| limt→∞ φ(x, t) = p}
In the context of gated-MRA, the hollow LA chamber comprised of several localmaxima on the distance transformation, yielding several such basins. The LA wasgenerally connected to the aorta, coronaries and pulmonary artery due to partialvoluming. Due to the nature of the distance transform and Morse partitions,rarely partitions spanned across chambers. For example, a partition spanningacross the LA and aorta. It was this special feature of the algorithm that enabledthe LA to be separated from its surrounding structures. However, a final partitionselection step was necessary.
In the final partition selection step, the user selects the partitions (or basins)that should be included in the LA. The final segmentation is then computedfrom this selection.
2.3 Evaluation
The focus of this work was to obtain LA anatomy for quantifying fibrosis/scarin LGE. A time-consuming rigorous manual segmentation of the LA from LGEimages generally gives the most reliable 3D reconstruction of LGE scar on LA
Left Atrial Segmentation from Gated-MRA 159
Fig. 3. (Left) A schematic showing how Morse partitions are computed from the dis-tance transform f(x) of the binary image. (Right) Morse parititions labelled on a 3Dreconstruction of the LA.
anatomy. To evaluate the algorithm, segmentations were thus compared to LAanatomy obtained manually from LGE images. These manual segmentationswere obtained from an observer with experience in LA anatomy. The observeranalysed each corresponding LGE image, starting from the base of the LA, iden-tifying the location of the mitral valve region, and working upwards to the roof.In each slice, the atrial wall boundary was annotated by selecting several pointsalong the boundary and drawing a polygonal contour. The atrial wall contourwas interpolated in regions where it was not visibly clear. Segmentations fromthe algorithm were also manually corrected, when necessary. However, the orig-inal segmentations obtained from the algorithm, without the manual correctionstep, were evaluated separately.
Segmentations were compared using two different techniques. The similaritybetween segmentations from the algorithm and manual method was quantifiedwith a Dice similarity metric, separately computed on the LA boundary andinner chamber. A second technique evaluated smoothness of the segmentations.Smoothness was obtained by quantifying the disparity in the directions of the3D LA surface normals. Measuring disparity of surface normals within a neigh-bourhood, as opposed to surface curvature, is more important. This is due to themethod for creating 3D reconstructions of fibrosis/scar on LA anatomy, whichrelies on smooth surface normals interrogating the atrial wall in the LGE image.Furthermore, evaluating smoothness allows us to investigate the hypothesis thatmanual annotation of the LA on a slice-by-slice basis yields non-smooth surfaces,often difficult to recover using smoothing filters.
3 Results
Results from the algorithm in some selected cases can be seen in Fig. 4. Thesimilarity between segmentations obtained from the algorithm (on gated-MRA)and manual annotation (on LGE) were compared with the Dice similarity metric.As the Dice metric on digital images is computed voxel-wise, it can be biased tolarge voxel volumes that differ mostly on the boundary. To eliminate this bias,
160 R. Karim et al.
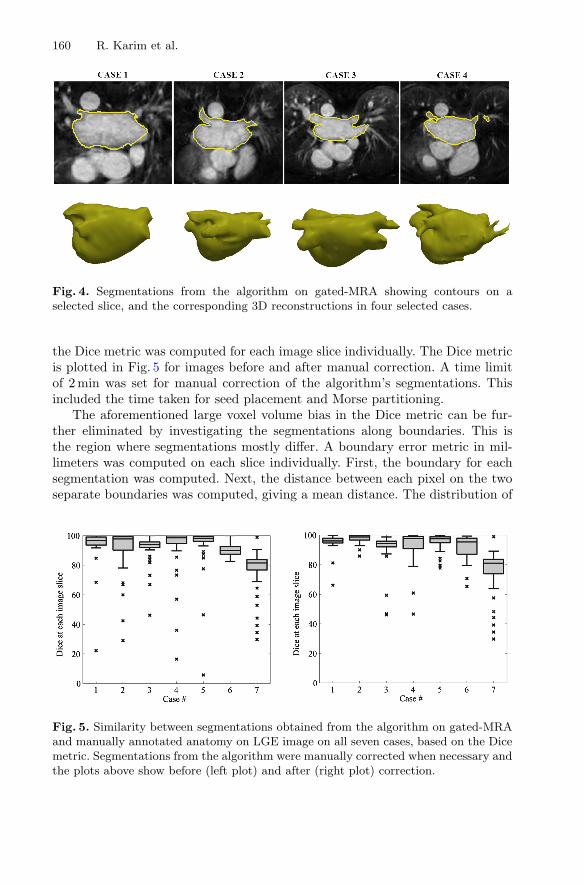
Fig. 4. Segmentations from the algorithm on gated-MRA showing contours on aselected slice, and the corresponding 3D reconstructions in four selected cases.
the Dice metric was computed for each image slice individually. The Dice metricis plotted in Fig. 5 for images before and after manual correction. A time limitof 2 min was set for manual correction of the algorithm’s segmentations. Thisincluded the time taken for seed placement and Morse partitioning.
The aforementioned large voxel volume bias in the Dice metric can be fur-ther eliminated by investigating the segmentations along boundaries. This isthe region where segmentations mostly differ. A boundary error metric in mil-limeters was computed on each slice individually. First, the boundary for eachsegmentation was computed. Next, the distance between each pixel on the twoseparate boundaries was computed, giving a mean distance. The distribution of
Fig. 5. Similarity between segmentations obtained from the algorithm on gated-MRAand manually annotated anatomy on LGE image on all seven cases, based on the Dicemetric. Segmentations from the algorithm were manually corrected when necessary andthe plots above show before (left plot) and after (right plot) correction.
Left Atrial Segmentation from Gated-MRA 161
Fig. 6. The mean difference (in mm) along the boundary of the segmentations obtainedfrom the algorithm on gated-MRA and manually annotated anatomy on LGE imageon all seven cases. Segmentations from the algorithm were manually corrected whennecessary and the plots above show before (left plot) and after (right plot) correction.(1 pixel ∼ 2 mm based on the image resolution)
this distance in each individual case is plotted in Fig. 6 for segmentations beforeand after manual correction.
The smoothness of the 3D reconstructions obtained both from algorithmand manual annotation was evaluated. The surface normal at every point wasinvestigated by measuring the angular difference from other surface normals inits neighbourhood. The standard deviation of these angle-difference distributionswere plotted and is shown for some example cases in Fig. 7. Finally, the total
Fig. 7. Three cases where the smoothness of 3D reconstructed surfaces of manuallyannotated (left column) and algorithm segmentations (right column) are plotted. Thesmoothness is based on the distribution of angle differences between surface normalvectors in a neighbourhood.
162 R. Karim et al.
time taken to run the algorithm, interact and manually correct the segmenta-tions was measured as 3.2 ± 1.4 min. In comparison, manual annotations took23.4 ± 2.4 min.
4 Discussion and Conclusion
Accurate assessment of left atrial myocardial fibrosis/scar size and anatomy ischallenging. Shape-based segmentation of LA from high resolution whole-heartb-SSFP is a preferred technique at our institution [4]. Manual annotation of theLA directly from LGE images is also a well-known technique [5]. Both thesemethods have limitations. The proposed algorithm segments LA from a novelrespiratory and ECG-gated MRA sequence. This enables 3D reconstructions offibrosis/scar on LA anatomy with greater accuracy and reliability. Segmentationof LA from MRA images using distance transformations is not novel, and this hasbeen investigated in earlier works [2,3]. The proposed work implements distancetransform image partitioning with Morse theory and evaluates it in the contextof LGE fibrosis/scar quantification.
Results demonstrated good similarity with manual annotations of the LAon LGE images. The analysis of smoothness is important in the context of 3Dreconstructions of LGE-imaged fibrosis/scar. In the analysis, regions with highlyvariable surface normals (in terms of their direction) were identified. Results havedemonstrated that these high curvature regions are more dense in annotatedsegmentations. This is since annotations are performed on the single axial view,which is typically the LGE acquisition orientation. The algorithm’s segmentationachieved greater smoothness due to its 3D image processing pipeline.
The presented work has several limitations. The algorithm requires manualselection of partitions and an automation may be possible. Also, the algorithmwas not validated with other existing MRA segmentation algorithms and thusit may be difficult to assess the quality of the results.
References
1. Groarke, J.D., Waller, A.H., et al.: Feasibility study of electrocardiographic and res-piratory gated, gadolinium enhanced magnetic resonance angiography of pulmonaryveins and the impact of heart rate and rhythm on study quality. J. Cardiovasc. Magn.Reson. 16(1), 43 (2014)
2. John, M., Rahn, N.: Automatic left atrium segmentation by cutting the blood poolat narrowings. In: Duncan, J.S., Gerig, G. (eds.) MICCAI 2005. LNCS, vol. 3750,pp. 798–805. Springer, Heidelberg (2005)
3. Karim, R., Juli, C., et al.: Automatic segmentation of left atrial geometry fromcontrast-enhanced magnetic resonance images using a probabilistic atlas. In:Camara, O., Pop, M., Rhode, K., Sermesant, M., Smith, N., Young, A. (eds.) STA-COM 2010. LNCS, vol. 6364, pp. 134–143. Springer, Heidelberg (2010)
4. Knowles, B., Caulfield, D., Cooklin, M., Rinaldi, C., Gill, J., Bostock, J., Razavi, R.,Schaeffter, T., Rhode, K.: 3-D visualization of acute RF ablation lesions using MRIfor the simultaneous determination of the patterns of necrosis and edema. IEEETrans. Biomed. Eng. 57(6), 1467–1475 (2010)
Left Atrial Segmentation from Gated-MRA 163
5. Oakes, R., Badger, T., et al.: Detection and quantification of left atrial structuralremodeling with delayed-enhancement magnetic resonance imaging in patients withatrial fibrillation. Circulation 119(13), 1758–1767 (2009)
6. Tobon-Gomez, C., Peters, J., et al.: Left atrial segmentation challenge: a uni-fied benchmarking framework. In: Camara, O., Mansi, T., Pop, M., Rhode, K.,Sermesant, M., Young, A. (eds.) STACOM 2013. LNCS, vol. 8330, pp. 1–13.Springer, Heidelberg (2014)