Legionnaires’ Disease Pneumonia: Histopathologic Features and Comparison with Microbial and Chemical Pneumonias*
GARY L. LATTIMER, M .D.,f RAYMOND A. RACHMAN, M.D.,*and M ICHAEL SCARLATO, M .D.f
t Infectious Diseases Section and \ Department o f Pathology, Allentown and Sacred Heart Hospital Center,
Allentown, PA 18105
ABSTRACT
The histopathologic findings in lung tissue are reported from five cases of P h ilade lph ia L egionnaires’ D isease and the results are com pared to pneumonias caused by other microbial and chemical agents. Histopathology of lung tissue was similar in all cases, despite the fact that death occurred betw een the fourth and 14th day of clinical illness. The inflammatory response was almost totally lim ited to the lower respiratory tract and prim arily involved respiratory bronchioles, alveolar ducts and alveoli. Major bronchial branches and pulmonary interstices showed little or no involvement. There was considerable variation in the extent and nature of the consolidation, but the overall reaction pattern was highly characteristic of diffuse alveolar damage. Most involved areas showed intra-alveolar, fibrinocellular mononuclear cell predom inant exudates, associated with pneumocytic hyperplasia and slough. These findings plus the presence of erythroleucophago- cytosis by macrophages and paucity of polymorphonuclear leucocytes are commonly associated with psittacine pneumonia, and much less so with classic patterns of bacterial, viral, fungal or rickettsial pneumonias. O f the toxic inhalants, nickel carbonyl, phosgene, nitrous oxide, cadmium oxide and some halogenated hydrocarbons have been associated with this tissue reaction pattern. Bacteria were notably absent in lung tissue stained by methods used to demonstrate the Legionnaires’ Disease agent.
Introduction
An u n u su a lly se v ere p n eu m o n ia , Legionnaires’ Disease (LD), resulting in 182 cases and 29 deaths, occurred in Philadelphia during July and August of 1976.4 A fter five m onths o f in tensive
Send request for reprints to: Gary L. Lattimer, M .D ., A llentow n and Sacred Heart H osp ital C enter,1200 S. Cedar Crest Blvd., A llentown, PA 18105.
epidem iologic and laboratory investigation , the C e n te r for D isease C ontro l (CDC) reported the isolation of a Gram- negative bacterium from lung tissue of disease victims and identified it as the putative agent by dem onstrating immuno- fluorescent antibodies in serum of patients surviving the illness.5 Findings in the lungs of 14 autopsied victims were in itia lly repo rted as non-specific and probably produced by a toxic substance.22
Most show ed areas of extensive pneumonitis w ith some areas of m ild in terstitial reaction. Special stains revealed no fungi, bacteria or other microorganisms except in one case w ith d issem inated c an d id ias is .4 M ore recen tly , the p u lmonary tissue reaction pattern was described as “ sim ilar to those associated w ith a lobar pneum on ia ,” w ith acute fibrinopurulent pneum onia in 21 cases and diffuse alveolar disease in 13 cases.3 In 19 of 26 LD victims, bacilli were readily dem onstrated in lung tissue by the D ieterle silver-impregnation m ethod and found inconsistently with conventional h is to p a th o lo g ic sta ins for m icro organisms.3
T he e p id e m io lo g ic fea tu re s and clinical findings of progressive atypical pneum onia associated with fever and relative bradycardia, with apparent response to tetracycline therapy, suggest the clinical diagnosis of a zoonosis, particularly p sittacosis . 15F u rth e rm o re , our in itia l
study of lung tissue did not reveal changes seen in acute bacterial pneumonia.910 In stead, the present authors found a fibrino- cellular, m ononuclear cell predominant, in tra -aveo lar exudative process m ore commonly described in psittacosis,14 but also seen in toxic, viral, fungal and mycop lasm a p n eu m o n ia . To com pare, in further details, the histopathologic features of these clinically similar entities, tissue sections w ere studied from five fatal LD cases and from two fatal cases of psittacosis and our findings were compared with those seen in other microbial or toxic pneumonias.
M aterial and M ethods
In table I are given the sex, age, days of clinical illness at the tim e of death, underlying disease process, antibiotic therapy and summary of the gross description of the lung noted at the time of autopsy. All cases were listed as LD victims by the
TABLE I
Clinical Data with Gross Pulmonary Pathology
Age, Day ofYr/ Illness Cause of Underlying Antibiotic Autopsy Findings
Patient Sex At Death Death Disease Therapy Gross Description of Lung
(500 cc).Diffuse severe edema and patchy pneumonia all lobes.
Penicillin Diffuse bilateral pneumonia, edema and Cephalothin congestion all lobes.
♦Arteriosclerotic cardiovascular disease
LEGIONNAIRES’ PNEUM ONIA HISTOPATHOLOGY 355
P e n n sy lv a n ia S tate D e p a rtm en t of Health,23 were over 40 years of age, had significant underly ing disease and expired betw een the fourth and 14th day after the clinical illness was noted. The im m ediate cause of death was ascribed to respiratory failure (4 cases) and cardiac failure (1 case).
Formalin-fixed, paraffin em bedded tissue specim ens from lung (5 cases), liver and spleen (4 cases) were stained by the haematoxylin and eosin, periodic acid- Shiff, G ridley’s reticulin, Verhoeff-Van Gieson, Peris’ prussian blue and phospho- tungstic acid-hematoxylin methods. To compare staining characteristics of microbial agents, sequential sections of lung tissue specim ens w ere stained by the Brown-Brenn, Giemsa, D ieterle silver- impregnation m ethods27 and direct fluorescent antibody (FA) technique.6 Lung t is su e s in cases 1 and 5 w ere also examined with an electron microscope. F inally , haem atoxylin and eosin and Giemsa stained lung tissue slides from fatal cases of human psittacosis infected with the Epizootic Bovine Abortion1 and Borg2 strains of Chlamydia psittaci were com pared directly to LD victim specimens. Control tissue for the Dieterle stain and specific conjugate for fluorescent staining was kindly supplied by the CDC.
ResultsThe histopathology of lung tissue was
similar in all five cases regardless of the day of illness prior to death. The inflammatory response was almost totally limited to the lower respiratory tract and involved respiratory bronchioles, alveolar ducts and alveoli. The bronchial branches often had light chronic inflammatory infil- tra tes w ith in th e ir w alls, co n s is tin g mainly of lymphocytes, but destruction of the mucosa was rare or absent even in those w ith lum enal cellu lar exudates. There was considerable variation in the extent and nature of the consolidation, often within the same lobule. Two distinc
tive patterns of involvement were recognized. D ense consolidation, ex tending into uninvolved area by direct alveolar spread, was most commonly seen (figure 1).
In other sections, dilated alveolar ducts, some filled w ith exudates, were found scattered throughout normal appearing lung (figure 2). Septal and in terstitial areas were congested with red blood cells b u t contained few inflamm atory cells. Those alveoli located at the periphery of th e inflam m atory reac tio n c o n ta in ed few er num bers of inflam m atory cells; however, the components of the exudative response were similar to those found in central dense areas of inflammation. Hypertrophied alveolar lining cells, many of which were desquam ating in cohesive sheets, were frequently found at the margin of the inflammatory response (figure 3). The contents of the alveolar exudate commonly varied from field to field. Most involved alveoli contained a fibrinocel- lular exudate composed of large, occasionally vacuolated m ononuclear cells, red blood cells, polym orphonuclear cells, lymphocytes and alveolar epithelial cells in various proportions (figure 4). Erythro- phagocytosis and leukophagocytosis by macrophages was frequently encountered (figure 5). The polymorphonuclear leucocyte content varied, bu t they were in the main fewer in num ber than the mononuclear cells. Fibrin, where present, was in the form of intra-alveolar m eshwork with entrapped cells, not splayed on the septa as a hyaline m em brane (figure 5). Interstitial fibrosis, or organizing oblitera- tive alveolitis, was not seen. Pulmonary arterial and venous throm bi or em boli were absent.
H epatic and sp len ic tissue show ed m arked acu te congestion . T h e re was moderate hepatic steatosis and moderate Kupffer ce ll hypertrophy . O ccasional hepatic Kupffer cells and macrophages in the splenic red pulp showed erythrocytic and leucocytic phagocytosis. There were small numbers of immunoblasts and ma-
3 5 6 LATTIMER, RACHMAN AND SCARLATO
F ig u r e 1. (Top) Margin of consolidated alveoli and normal lung. Note the lack of inflammatory response in the small bronchus (arrowhead). Hematoxylin and eosin stain, magnification x 125.
F ig u r e 2. (Bottom). Scattered area of intra-alveolar exudates of varying densities, not associated with dense consolidation. Hematoxylin and eosin stain, magnification x 125.
l e g i o n n a i r e s ’ p n e u m o n i a h i s t o p a t h o l o g y 357
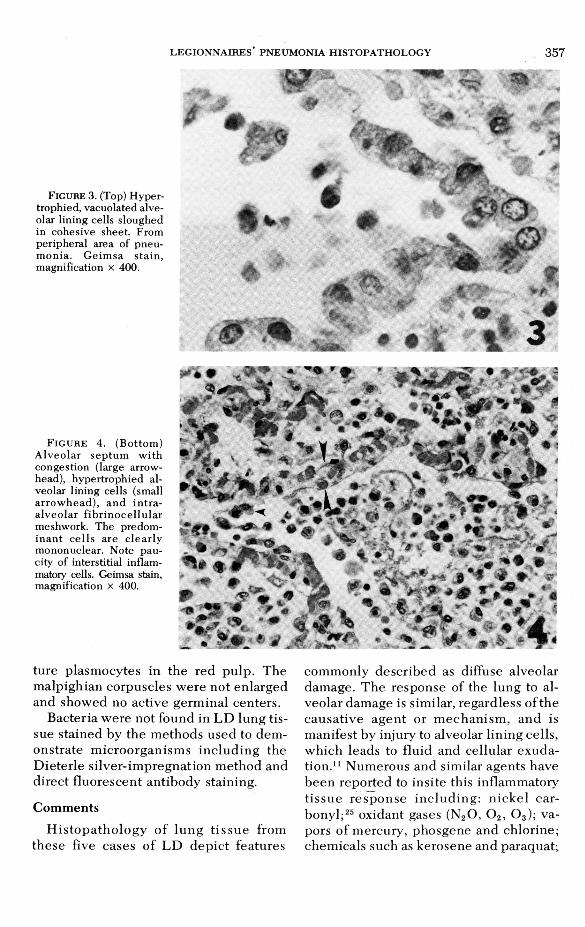
FIGURE 3. (Top) H ypertrophied, vacuolated alveolar lining cells sloughed in cohesive sheet. From peripheral area of pneum onia. G eim sa sta in , magnification x 400.
I» .#
WÊk
04 ÉL» ‘
Ü
%" r
• • i ,1 3
F i g u r e 4. (B ottom ) A lveo lar sep tum w ith congestion (large arrowhead), hypertrophied alveolar lining cells (small arrow head ), and in tra - alveo lar fib rin o ce llu la r meshwork. The predom in an t c e lls are c lea rly mononuclear. Note paucity of interstitial inflammatory cells. Geimsa stain, magnification x 400.
ture plasmocytes in the red pulp . The m alpighian corpuscles were not enlarged and showed no active germinal centers.
Bacteria were not found in L D lung tissue stained by the m ethods used to dem onstrate m icroorganism s inc lud ing the Dieterle s ilver-im pregnation m ethod and direct fluorescent antibody staining.
Com ments
H is to p a th o lo g y o f lu n g t i s su e from these five cases of L D dep ic t features
com m only described as diffuse alveolar damage. T he response of the lung to alveolar damage is similar, regardless o f the causative agen t or m echan ism , and is manifest by injury to alveolar lining cells, which leads to fluid and cellular exudation.11 N um erous and similar agents have b een reported to insite this inflammatory t is su e re sp o n se in c lu d in g : n icke l ca rbony l;25 oxidant gases (NzO, 0 2, 0 3); vapors of mercury, phosgene and chlorine; chemicals such as kerosene and paraquat;
358 LATTIMER, RACHMAN AND SCARLATO
W
%
»
F i g u r e 5 . H igh po w ered view show ing fibrinocellular, m ononuclear exudate, and erythro- leukophagocytosis by m acrophages (arrowhead). Geimsa stain, magnification x 1000.
and a group o f clinical diseases associated with the adult respiratory distress syndrome.11 O f the infectious agents known to cause this h is topathologic response, only influenza and feline calicivirus have been described com pletely.12 O ur cases were not exposed to any of these agents, except case 4 w ho received high concentrations of 0 2 while receiving artificial ventilation.
A n u m b e r o f o u tb r e a k s o f h u m a n chlam ydial infections o f the psittacine ty p e 17,19 as w ell as experim ental disease in prim ates21 has been reported, which allows comparison to be made with the histopathology of these five cases of LD. A review of these pub lished reports and
V * c
' A t ' l• a
? *
Q># L : <K * - 7
M k |
/ » .
4
f t
% •
j l m m
mm5
direct comparison to lung tissue from two cases of psittacosis1,2 reveal the following similarities: (1) marked variability in the d eg ree an d characteristic of the intra- alveolar process, often w ith in the same lobu le ; (2) m o n onuc lea r cell p redom i- nence; (3) s loughed hypertrophied alveolar l in in g ce lls , red b lood cells , m acrophages and m ononuclear cells in varied p r o p o r t io n s e m b e d d e d in a f ib r in meshwork; (4) virtual absence of significan t in te rs t i t ia l in f lam m atory ce l lu la r ex u d a te ; (5) th e p re s e n c e of e ry th ro- leukophagocytosis by macrophages; (6) little or no involvem ent of the larger bronchi or bronchio les; and (7) absence of clearly identifiable organisms with standard staining techniques.
M ononuc lea r cells and m acrophages are the p rédom inen t cells found within alveoli d u r in g th e re so lu t ion s tage of com m on bacterial pneum onias, bu t are uncom m only found during the acute stage except in certain zoonoses owing to rickettsial or bacterial agents.24 Although the patchy consolidation and m ononuc lea r intra-alveolar exudates are characteristic of rickettsial pneum onias, interstitial in volvement, bronchial epithelial necrosis and perivascular cuffing usually described in th is e n t i t y 2,18 w e re n o t o b se rv e d . T h e m a rk e d in te r s t i t i a l a n d a lv e o la r septal infiltrates and the bronchial ep ithelia l necrosis typically seen in viral p n eu m o n ias8 w ere also not found. O f the bacterial agents, tularemia, plague, an thrax and brucellosis are associated with m o n o n u c le a r in t ra -a lv eo la r ex u d a te s . H ow ever, areas of necrosis, vasculitis, b ro n c h ia l in f la m m a to ry re a c t io n an d iden tif iab le m icroorganism s with s tandard staining techn iques are histologic features characteristically associated with these bacterial pa thogens24 and w ere not observed in our cases of LD.
Inhalan t toxins exert their effect in the respiratory tract d epend ing upon their solubility in water. Vapors of hydrochloric acid, hydrofluoric acid, formaldehyde and
l e g i o n n a i r e s ’ p n e u m o n i a h i s t o p a t h o l o g y 359
ammonia are highly soluble and affect the mucous membranes of the nose, throat and upper respiratory tract. In contrast, phosgene nitrous oxide, cadmium oxide, nickel carbonyl fumes and some hallo- genated hydrocarbons are less soluble and cause severe injury to the respiratory b ronchio les and alveolar lin ing cells, w h ile sp a rin g th e u p p e r re sp ira to ry tract.7,25,26 Clinical symptoms produced by the less soluble agents are often delayed for hours to days.7,26 T he histopathologic sim ilarities b e tw een some toxic and infectious pneum onias were noted by W internitz30 while studying the pathology of phosgene poisoning. At the same time, he called attention to the high incidence of secondary infection complicating injuries caused by inhalation of toxic gases.30
Diffuse alveolar damage is the active stage of an inflammatory response, the morphogenesis of which depends upon the nature of the inciting agent and duration of exposure. Resolution may occur without residual damage or progress to pulmonary interstitial or alveolar fibrosis, atelectasis or em physem a.11
Although the natural history of patients with LD pneum onia has not been determined, pulmonary function studies performed on LD survivors two years after the outbreak showed abnormalities in the diffusion capacity. Also, the clinical findings of shortness of breath and recurrent bronchitis suggest perm anent lung damage may follow the resolution of Legionnaires’ Disease pneum onia.16 Additional follow-up studies will be necessary to determ ine if long-term sequela develop.
Although our findings are similar to those reported by the CDC,3 we differ in regards to some histopathologic characteristics and in our failure to identify the organisms by special stains. O f 26 autop- sied cases, the CDC reports finding an acute fibrinopurulent pneum onia in 21 cases and diffuse alveolar disease in 13 cases. The significance of the diffuse al
veolar damage has not been explained,3 but its presence is often associated with lung injury owing to viral pneum onias, oxidant gases, chem ical toxins, shock, pancreatitis and several drugs,11 and much less frequently with infection by bacte r ia .24 T hat b ac te ria w ere found by the D ieterle silver-im pregnation stain in areas o f c lassic f ib r in o p u ru le n t pneum onia but not in areas of acute diffuse alveolar damage suggest the tissue action patterns may be due to separate agents. This combination of tissue reaction patterns has been described in cases of pneum onia secondary to influenza or toxic gases complicated by secondary infection owing to bacteria.30,31
Although highly sensitive, the D ieterle m ethod cannot be used to identify specifically the LD bacteria because it stains o ther bacteria, chrom atin, hem osiderin phagocytic granules, form alin pigm ent and melanin in a non-specific fashion.27 A method of direct fluorescent antibody (FA) staining of deparaffinized lung tissue sections has been described,6 which should allow for a more specific bacteriologic diagnosis in tissue sections. However, in a previous report, the CDC failed to identify the agent in 30 lung tissue specim ens from five LD victims using pooled convalescent serum conjugated with fluorescein isothiocyanate (FITC) or radioactive iodine.20 Using FITC direct FA conjugate prepared from hyperim m une sera from goats or Legionnaires’ Disease survivors, we failed to demonstrate organisms by the direct FA test in lung tissue sections or tissue scrapings from these five cases.
Also, in contrast to the CDC report, we found only the reaction pattern of diffuse a lv eo lar dam age w ith in tra -a lv eo la r m ononuclear predom inant cellular exud ate , m acrophages, and p ro m in e n t erythrophagocytosis. There was a paucity of polymorphonuclear leukocytes in all five cases and bacteria were not found on special stains, includ ing the D ie te rle silver impregnation and direct fluorescent
360 LATTIMER, RACHMAN AND SCARLATO
antibody methods. Our lung tissue samples were taken from patients who expired at different time intervals during the acute illness and the exudative process was florid in all cases. Furtherm ore, we studied areas located at the periphery of the inflammatory reaction usually considered the area of most recent involvement, as w ell as the central dense areas of inflammation. Perhaps tissue specim ens from these five cases were not from similar areas of lung involvement, when com pared to the CD C’s samples, as we found ne ither a f ib rinopu ru len t reaction nor organisms.
Histopathologic findings in lung tissue of LD victims from other outbreaks or sporatic cases of Legionnaires’ Disease vary considerably. Report findings in clude: exudative bronchopneum onia;13 ulcerative bronchitis with focal necrosis of bronchial epithelial cells;28 interstitial pneum onitis w ith edem atous alveolar septa, infiltrated with polymorphonuclear leukocytes and macrophages; necrosis, microabscesses, interstitial fibrosis and coagulation necrosis.29 These findings were also not seen in these five cases from the Philadelphia epidem ic.
It seems clear that some of the histopathologic findings in LD pneum onia may be due to secondary infection, the results of therapy or underlying disease. Final definition of the pulmonary histo- pathology m ust await studies in primates infected with aerosolized LD agent, as performed by McGavran when studying the histopathology of psittacosis.21
Ackno wledgmentsWe are indebted to Drs. Anthony E. Mass and
Rosario M aniglia, Camp Hill, Pennsylvania, Dr. G ene T. Fries, Williamsport, Pennsylvania and Dr. Jules Foldes, Hazleton, Pennsylvania for providing c lin ic a l in fo rm ation an d tis su e sp ec im en s on Legionnaires’ D isease victims, and to Dr. Oscar Rambo, San Francisco, California and Dr. Chapman Binford, W ashington, D. C. for supplying tissue specim ens and slides of human psittacosis.
References1. B a r n e s , M. G . and B r a i n e r e d , H.:
Pneumonitis with alveolar-capillary block in a cattle rancher exposed to epizootic bovine abortion. N. Eng. J. Med. 271:981-985, 1964.
2. B in f o r d , C. H. and H a u s e r , C. H.: An epidemic of severe pneumonitis in the Bayou region of Louisiana, pathologic observation: Report of an autopsy of two cases and brief comparative note on psittacosis and Q-fever. Public Health Rep. 59:1363-1373, 1944.
3. B la c k m a n , J. A., H ic k l in , M. D., and C h a n d l e r , F. W.: Legionnaires’ Disease: Pathological and historical aspects of a ‘N ew ’ disease. Arch. Path. Lab. Med. 102:337-343, 1978.
4. C e n t e r f o r D i s e a s e C o n t r o l : Follow- up—Respiratory D isease—Philadelphia. Morbidity and Mortality Weekly Report. 25:270- 276, 1976.
5. C e n t e r f o r D is e a s e C o n t r o l : Follow-up on Respiratory Illness— Philadelphia. Morbidity and Mortality Weekly Report. 26:9-11, 1977.
6. CHERRY, W. B.: Legionnaires: The Disease, the Bacteria and Methodology. Center for Disease Control Laboratory Manual, U. S. Department of Health, Education and Welfare, 1978, p. 100.
7. G l e a s o n , M. G o s s e l in , R., and H o d g e , H.: Clinical Toxicology of Commercial Products. Baltimore, Williams and Wilkins, p. 256, 1968.
8. H e r s , J. F., Ma s u r e l n , N. M u l d e r , J.: Bacteriology and histopathology of the respiratory tract and lungs in fatal Asian influenza. Lancet 1:1141-1143, 1958.
9. Ka s s , E. H.: Legionnaires’ disease (editorial). N. Eng. J. Med. 297:1229-1230, 1977.
10. Ka s s , E. H.: Legionnaires’ disease (letter). N. Eng. J. Med. 298:852, 1978.
11. Ka t z e n s t e i n , A. A., B l o o r , C. M., and L e ib o w , A. A.: Diffuse alveolar damage—The role of oxygen, shock and related factors. Amer. J. Path. 85:210-228, 1976.
12. L a n g l o s s , J. M., H o o v e r , E. A., and Ka h , D.E.: Diffuse alveolar damage in cats induced by nitrogen dioxide or feline calicivirus. Amer. J. Path. 89:637-644, 1977.
13. L a t t im e r , G. L., M c C r o n e , C., and G a lg o n , J.: Diagnosis o f Legionnaires’ disease from transtracheal aspirate by direct fluorescent antibody staining and isolation of the bacterium. N. Eng. J. Med. 299:1172-1173, 1978.
14. La t t im e r , G . L., Ra c h m a n , R. A., and Sc a r - LATO, M.: Legionnaires’ disease (letter). N. Eng. J. Med. 298:852, 1978.
15. L a t t im e r , G . L. and R h o d e s , L . V.: Legionnaires’ disease: Clinical findings and one-year followup. J. Amer. Med. Assoc. 240:1169-1171, 1978.
16. L a t t im e r . G. L., Rh o d e s , L. V., Sa l v e n t i , J. S., G a l g o n , J. P., St o n e b r a k e r , V., Bo l e y , S. L., and H a a s , G.: The Philadelphia epidemic of Legionnaires’ disease: Clinical, pulmonary and serologic findings two years later. Ann. Int. Med. 90:522-526, 1979.
l e g i o n n a i r e s ’ p n e u m o n i a h i s t o p a t h o l o g y 361
17. L i l l i e , R. D.: T he pathology of psittacosis in man. Nat. Inst. H ealth Bull. 161 :l-4 6 , 1933.
18. L i l l i e , R. D., P e r r in , T. L., and A r m s t r o n g , C.: An institutional outbreak of pneum onitis.III. Histopathology in man and rhesus monkey in pneum onitis due to virus of “Q” fever. Pub. H ealth Rep. 56:149-155, 1941.
19. M a c L a c h la n , W. W., P e r m a r , H. H., R o g e r s , C. A.: Psittacosis: A clinical and pathology report of three cases. Ann. Intern. Med. 4:260- 276, 1930.
20. M cD a d e , J. E., S h ep a rd , C. C., F r a s e r , D . W., T sai, T. F., R edus, M. A., and D o w d le , W. R.: Laboratory investigation team: Legionnaires’ disease, isolation ofabacterium and demonstration of its role in other respiratory disease. N. Eng. J. Med. 297:1197-1203. Supplementary material, Naps D ocum ent 03184, p. 4 -5 , 1977.
21. M cG a v ra n , M. H., B e a rd , C. W., B e r e n d t , R.F., and NAKAMURA, R. M.: The pathogenesis of psittacosis; Serial studies of rhesus monkeys exposed to small particle aerosol o f the Borg strain. Am. J. Path. 40:653-670 , 1962.
22. Pa th o lo g y o f “Leg io n n a ir es’ D ise a se ” : Memorandum from Director o f Pathology D iv ision and Staff Pathologist, Toxicology Branch, CDC to Director for D isease Control, Atlanta, GA, Septem ber 17, 1976.
23. Pen n sy l v a n ia American Leg io n Ne w s : vol.19, # 9 , p. 7, Sept. 30, 1976.
24. SPENCER, H.: Pathology o f the Lung. 3rd ed ition, P h iladelph ia , Saunders, pp. 151-171,1977.
25. S u n d e r m a n , F. W il l ia m : Perspectives on Legionnaires’ disease in relation to acute nickel carbonyl poisoning, The H enry M. Scharf Lecture on C urrent Affairs. Ann. Clin. Lab. Sci. 7:187-200, 1977.
26. U n d e r h i l l , F. P.: The Lethal War Gases. Yale University Press, New Haven, pp. 1-21, 1920.
27. V a n O r d e n , A. E. and G r e e r , P. W.: Modification of the D ieterle spirochete stain. J. Histo. Technol. 1 :51-53, 1977.
28. W e s t l e y , M. E., Y e s n e r , R., and P ie r s o n , D. J.: Legionnaires’ disease: C linical and histopathologic features of a sporatic case. Chest 74:220-222, 1978.
29. W in n , W. C ., G a v in , F. L„ P e r l , D . P ., K e l l e r , J. L., A n d r e s , T. L., B r o w n , T. M ., C o f f i n , C. M ., S e n s e c q u a , J. E„ R om a n , L. N ., an d C r a i g h e a d , J. E .: T h e p a th o lo g y o f L eg io n n a ires’ D ise a se . Arch. Path. Lab. M ed. 102:344-350, 1978.
30. W i n t e r n i t z , M. C.: T he Pathology of War Gases. Yale University Press, pp. 35-66, 1920.
31. W i n t e r n i t z , M. C„ W a so n , I., and M c N a m a r a , F.: The Pathology o f Influenza. Yale University Press, pp. 40-43, 1920.