(05/12.LGSDRegistration) Lemon Grove School District New Enrollment Form (To be completed by the parent or guardian) FOR OFFICE USE ONLY _________________________ __________________________ __________ _______________ ___________________ School Name Teacher Grade Student Number CSIS Number Enrollment Date _________________ MM/DD/YYYY IEP □ Yes □ No Military □ Yes □ No Mil Housing □ Yes □ No Casino □ Yes □ No DOD □ Yes □ No Transfer INTRA INTER Ver. of Residency □ Yes □ No Due on/before: ______________ Ver. Of Birthdate □ Birth Cert □ Passport Immunizations Date ____________ Source __________ Initials ________ Male Student’s LEGAL Name:_____________________________________________________________ Date of Birth:_____________________ Female (from birth certificate) Last Name First Name Middle Name Mo./Day/Year _______________________________|________________________| (______)__________________________| (______)__________________________ Mother’s/Guardian’s First Name Last Name Home Phone Cell/Work Phone _______________________________|________________________|(_______)__________________________| (______)__________________________ Father’s/Guardian’s First Name Last Name Home Phone Cell/Work Phone ____________________________________________________________________________________________________________________________ Residence Address City State Zip Student lives with: □ Father □ Mother □ Grandparent(s) □ Guardian(s) □ Foster Parent □ Other ________________________ Are there any special custody regulations regarding your child? □ No □ Yes (A copy of custody court order on file at the school is necessary to deny natural parent access.) ____________________________________________________________________________________________________________________________ Mailing Address (if different than home address) City State Zip Name of Last School Attended:________________________________________________________District: ____________________________________ City/State: ____________________________________________Phone: (______)_____________________ Last Grade Attended ___________________ Student’s Birthplace: ___________________________________________ If not born in the U.S., what month/year did your child enter U.S.? _____/_____ City/State /Country Mo./Year What month and year did your child first enroll in a K-8 th grade school in the United States? _______/_______ In California? _______/_______ Has student left the U.S. since then? □ No □ Yes – If Yes, date of most recent U.S enrollment: ___________________ Has student ever been retained? □ No □ Yes – If Yes, what grade level ? _______________ Does student have an IEP? □ No □ Yes HOME LANGUAGE SURVEY The California Education Code requires schools to determine the languages spoken at home by the student. This information is essential in order for schools to provide meaningful instruction for all students. Your cooperation in helping us meet this important requirement is requested. Which language did your son/daughter learn when he/she first began to talk?_______________________________________________________________ What language does your son/daughter most frequently use at home?____________________________________________________________________ What language do you use most frequently to speak to your son/daughter? ________________________________________________________________ Name the language most often spoken by the adults at home:___________________________________________________________________________ PARENT EDUCATION LEVEL The California Department of Education requires that we record the parents’ education level with our testing data. To comply with this requirement, please check the box next to the educational level for each parent. Mother’s Highest Educational Level Father’s Highest Educational Level Not a high school graduate Not a high school graduate High school graduate High school graduate Some college (includes AA degree) Some college (includes AA degree) College graduate College graduate Graduate school/post graduate training Graduate school/post graduate training PLEASE CONTINUE ON TO OTHER SIDE
Transcript
(05/12.LGSDRegistration)
Lemon Grove School District
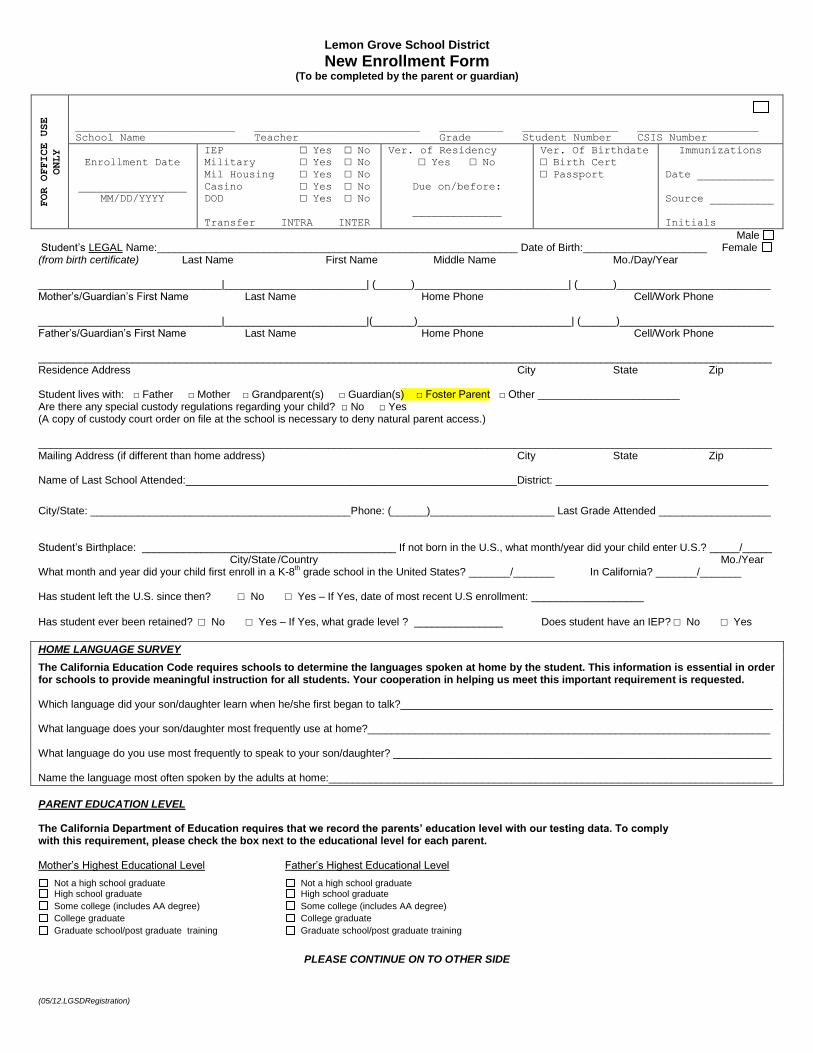
New Enrollment Form (To be completed by the parent or guardian)
School Name Teacher Grade Student Number CSIS Number
Enrollment Date
_________________
MM/DD/YYYY
IEP □ Yes □ No
Military □ Yes □ No
Mil Housing □ Yes □ No
Casino □ Yes □ No
DOD □ Yes □ No
Transfer INTRA INTER
Ver. of Residency
□ Yes □ No
Due on/before:
______________
Ver. Of Birthdate
□ Birth Cert
□ Passport
Immunizations
Date ____________
Source __________
Initials ________
Male Student’s LEGAL Name:_____________________________________________________________ Date of Birth:_____________________ Female (from birth certificate) Last Name First Name Middle Name Mo./Day/Year _______________________________|________________________| (______)__________________________| (______)__________________________ Mother’s/Guardian’s First Name Last Name Home Phone Cell/Work Phone _______________________________|________________________|(_______)__________________________| (______)__________________________ Father’s/Guardian’s First Name Last Name Home Phone Cell/Work Phone ____________________________________________________________________________________________________________________________ Residence Address City State Zip Student lives with: □ Father □ Mother □ Grandparent(s) □ Guardian(s) □ Foster Parent □ Other ________________________ Are there any special custody regulations regarding your child? □ No □ Yes (A copy of custody court order on file at the school is necessary to deny natural parent access.) ____________________________________________________________________________________________________________________________ Mailing Address (if different than home address) City State Zip Name of Last School Attended:________________________________________________________District: ____________________________________
City/State: ____________________________________________Phone: (______)_____________________ Last Grade Attended ___________________ Student’s Birthplace: ___________________________________________ If not born in the U.S., what month/year did your child enter U.S.? _____/_____ City/State /Country Mo./Year What month and year did your child first enroll in a K-8
th grade school in the United States? _______/_______ In California? _______/_______
Has student left the U.S. since then? □ No □ Yes – If Yes, date of most recent U.S enrollment: ___________________
Has student ever been retained? □ No □ Yes – If Yes, what grade level ? _______________ Does student have an IEP? □ No □ Yes
HOME LANGUAGE SURVEY
The California Education Code requires schools to determine the languages spoken at home by the student. This information is essential in order for schools to provide meaningful instruction for all students. Your cooperation in helping us meet this important requirement is requested. Which language did your son/daughter learn when he/she first began to talk?_______________________________________________________________ What language does your son/daughter most frequently use at home?____________________________________________________________________ What language do you use most frequently to speak to your son/daughter? ________________________________________________________________ Name the language most often spoken by the adults at home:___________________________________________________________________________
PARENT EDUCATION LEVEL The California Department of Education requires that we record the parents’ education level with our testing data. To comply with this requirement, please check the box next to the educational level for each parent. Mother’s Highest Educational Level Father’s Highest Educational Level
Not a high school graduate Not a high school graduate High school graduate High school graduate Some college (includes AA degree) Some college (includes AA degree) College graduate College graduate Graduate school/post graduate training
Graduate school/post graduate training
PLEASE CONTINUE ON TO OTHER SIDE
(05/12.LGSDRegistration)
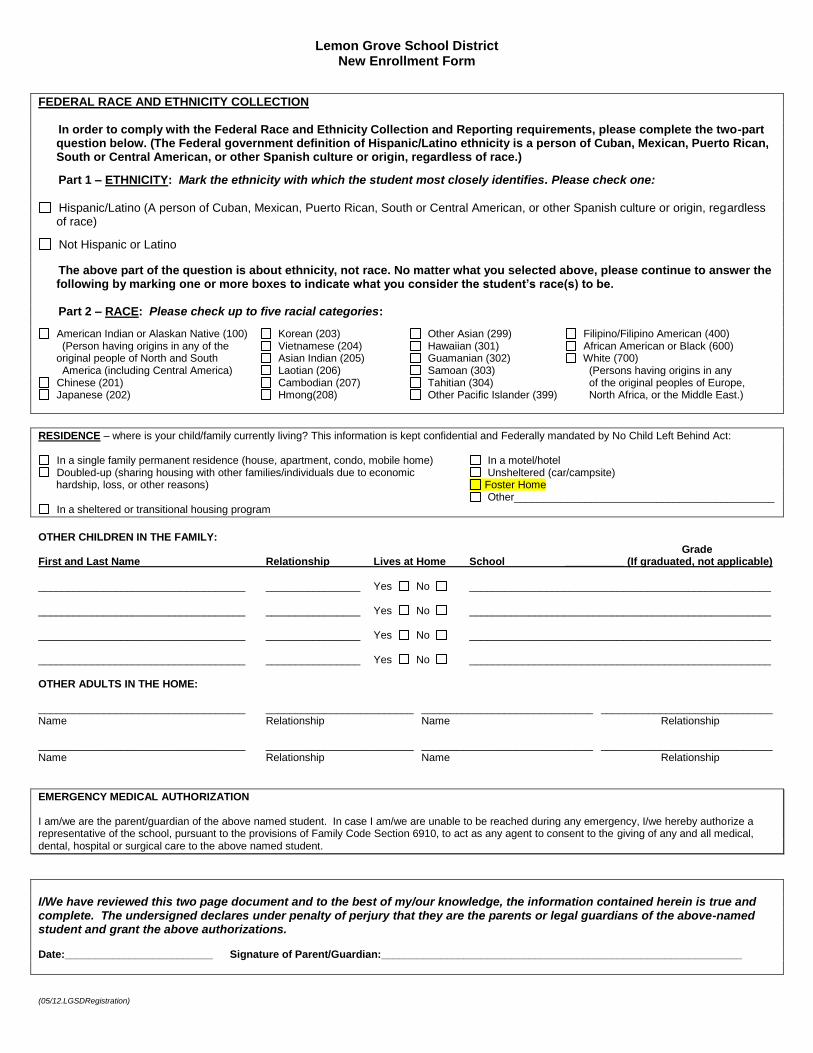
Lemon Grove School District New Enrollment Form
FEDERAL RACE AND ETHNICITY COLLECTION In order to comply with the Federal Race and Ethnicity Collection and Reporting requirements, please complete the two-part
question below. (The Federal government definition of Hispanic/Latino ethnicity is a person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin, regardless of race.)
Part 1 – ETHNICITY: Mark the ethnicity with which the student most closely identifies. Please check one:
Hispanic/Latino (A person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin, regardless of race)
Not Hispanic or Latino
The above part of the question is about ethnicity, not race. No matter what you selected above, please continue to answer the following by marking one or more boxes to indicate what you consider the student’s race(s) to be.
Part 2 – RACE: Please check up to five racial categories:
American Indian or Alaskan Native (100) Korean (203) Other Asian (299) Filipino/Filipino American (400) (Person having origins in any of the Vietnamese (204) Hawaiian (301) African American or Black (600) original people of North and South Asian Indian (205) Guamanian (302) White (700) America (including Central America) Laotian (206) Samoan (303) (Persons having origins in any
Chinese (201) Cambodian (207) Tahitian (304) of the original peoples of Europe, Japanese (202) Hmong(208) Other Pacific Islander (399) North Africa, or the Middle East.)
RESIDENCE – where is your child/family currently living? This information is kept confidential and Federally mandated by No Child Left Behind Act:
In a single family permanent residence (house, apartment, condo, mobile home) In a motel/hotel Doubled-up (sharing housing with other families/individuals due to economic Unsheltered (car/campsite)
hardship, loss, or other reasons) Foster Home Other____________________________________________
In a sheltered or transitional housing program
OTHER CHILDREN IN THE FAMILY: Grade First and Last Name Relationship Lives at Home School __________ (If graduated, not applicable) ___________________________________ ________________ Yes No ___________________________________________________ ___________________________________ ________________ Yes No ___________________________________________________ ___________________________________ ________________ Yes No ___________________________________________________ ___________________________________ ________________ Yes No ___________________________________________________ OTHER ADULTS IN THE HOME: ___________________________________ _________________________ _____________________________ _____________________________ Name Relationship Name Relationship ___________________________________ _________________________ _____________________________ _____________________________ Name Relationship Name Relationship
EMERGENCY MEDICAL AUTHORIZATION I am/we are the parent/guardian of the above named student. In case I am/we are unable to be reached during any emergency, I/we hereby authorize a representative of the school, pursuant to the provisions of Family Code Section 6910, to act as any agent to consent to the giving of any and all medical, dental, hospital or surgical care to the above named student.
I/We have reviewed this two page document and to the best of my/our knowledge, the information contained herein is true and complete. The undersigned declares under penalty of perjury that they are the parents or legal guardians of the above-named student and grant the above authorizations. Date:_________________________ Signature of Parent/Guardian:_____________________________________________________________
(04/12.LGSDAuthDec)
Lemon Grove School District
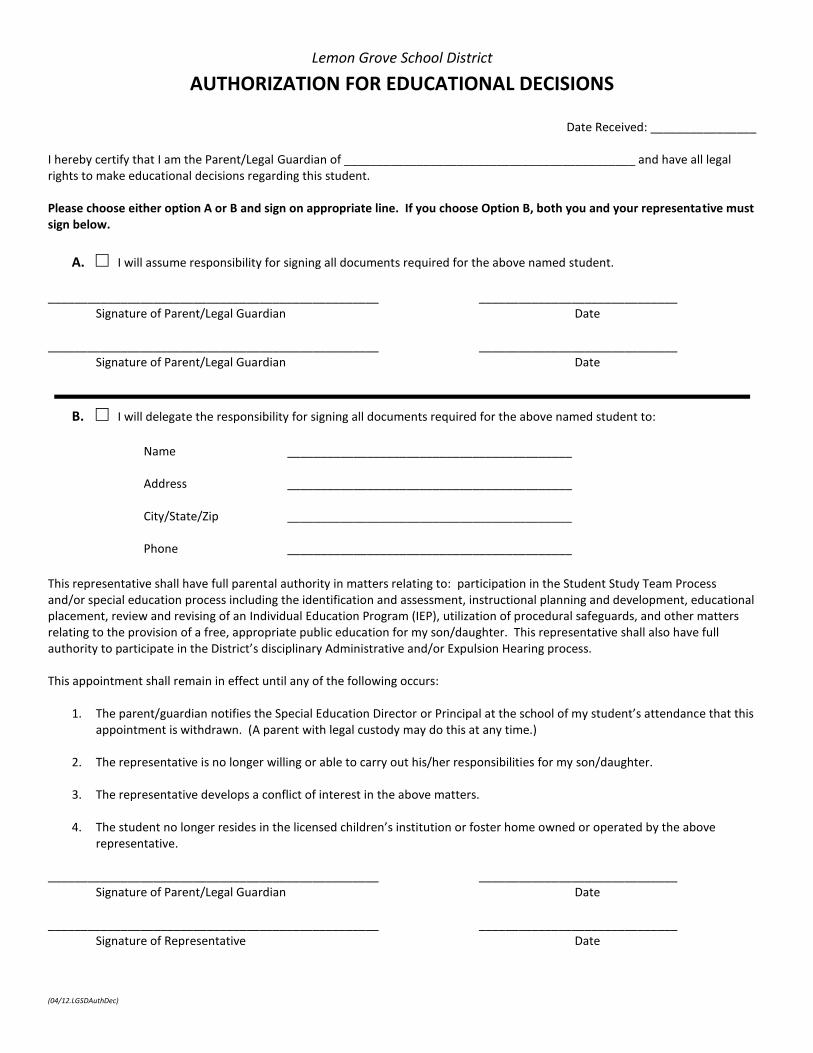
AUTHORIZATION FOR EDUCATIONAL DECISIONS
Date Received: ________________ I hereby certify that I am the Parent/Legal Guardian of ____________________________________________ and have all legal rights to make educational decisions regarding this student. Please choose either option A or B and sign on appropriate line. If you choose Option B, both you and your representative must sign below.
A. □ I will assume responsibility for signing all documents required for the above named student.
Signature of Parent/Legal Guardian Date __________________________________________________ ______________________________
Signature of Parent/Legal Guardian Date
B. □ I will delegate the responsibility for signing all documents required for the above named student to:
Name ___________________________________________ Address ___________________________________________ City/State/Zip ___________________________________________ Phone ___________________________________________
This representative shall have full parental authority in matters relating to: participation in the Student Study Team Process and/or special education process including the identification and assessment, instructional planning and development, educational placement, review and revising of an Individual Education Program (IEP), utilization of procedural safeguards, and other matters relating to the provision of a free, appropriate public education for my son/daughter. This representative shall also have full authority to participate in the District’s disciplinary Administrative and/or Expulsion Hearing process. This appointment shall remain in effect until any of the following occurs:
1. The parent/guardian notifies the Special Education Director or Principal at the school of my student’s attendance that this appointment is withdrawn. (A parent with legal custody may do this at any time.)
2. The representative is no longer willing or able to carry out his/her responsibilities for my son/daughter.
3. The representative develops a conflict of interest in the above matters.
4. The student no longer resides in the licensed children’s institution or foster home owned or operated by the above
Date of last medical examination _______________ Doctor ______________________________________
Date of last dental examination _______________ Doctor ______________________________________
Date of last eye examination _______________ Doctor ______________________________________
If you would like to discuss any health problems of your child with the School Nurse or Health Clerk, please list your name and
daytime phone number:
Name _______________________
Phone_______________________
Signature of Parent/Guardian __________________________________________________ Date _______________________
LEMON GROVE SCHOOL DISTRICT STUDENTS E 5111.1 District Residency
RESIDENCY VERIFICATION AND CHECKLIST Name of Person Completing This Form I am the (please circle one) parent/legal guardian/foster parent/relative. Names of Child/Children I wish to enroll such student(s) in __________________________________________________ (Name of School) I affirm that the student(s) resides at the following street address: Street Address Apt. # City State Zip Code Signature Date FOR OFFICE USE ONLY
The parent/legal guardian/foster parent/relative must present at least TWO (2) of the following
ORIGINAL documents: Property tax payment receipts Rental property contract, lease, or mortgage statement Escrow papers for a new home Utility service contract, statement or payment receipt Pay stub Voter registration Military orders
Correspondence from a government agency If the student is an unaccompanied youth as defined in 42 USC 11434a, a declaration of residency executed by the student If the student is residing in the home of a caregiving adult within district boundaries, an affidavit executed by the caregiving adult in accordance with Family Code 6552
The documents described in the boxes as checked above were presented by the (please circle one) parent/legal guardian/foster parent/relative/emancipated minor verifying the student's residency. The student's registration address matches the address listed on the residency verification document. Verifying School Official ____________________________________ Date _______________
(04/12.LGSDStudentSvcs)
Lemon Grove School District
RECORD OF PREVIOUS STUDENT SERVICE PROGRAMS
Student’s Name: ___________________________________________ Birth Date: _____________Date: ____________ Primary Language: _________________________________________ Grade: ________________ Age: ____________ Name of Previous School: __________________________ Name of Previous District: ___________________________ It is important to us that we are aware of any special services your child may have received or programs he or she participated in at a previous school. Please provide us with the following information to assist us in assigning your child to the most appropriate placement. Please check all of the following that apply to your child:
_____ Gifted and Talented Education (GATE)
_____ English Learner (EL)
_____ Chapter I or Title I
_____ Reading
_____ Math
_____ Additional Support
_____ Reading Lab
_____ Response to Interventions (RTI)
Accommodations and Modifications
_____ Counseling
_____ Section 504 Plan
_____ Resource Specialist Program (RSP)
_____ Specialized Academic Instruction
_____ Specific Learning Disability
_____ Speech and Language Disorder
_____ Other Health Impairment
_____ Intellectual Disability
_____ Orthopedic Impairment
_____ Autism Diagnosis
_____ Visual Impairment
_____ Hearing Impairment
_____ Serious Emotional Disturbance
_____ Adaptive P.E. (APE)/Physical Therapy (PT)
_____ Speech/Language Therapy
_____ My child did not participate in any special programs to support his/her education at his/her previous school.
Has your child ever been tested by a school psychologist to determine the need for special education intervention? _____ If yes, was your child eligible for special education services? _________ Please add any additional information which you think might be helpful in working with your child this school year: __________________________________________________________________________________________________________ __________________________________________________________________________________________________________ __________________________________________________________________________________________________________
Signature of Parent/Guardian _______________________________________________________ Date ______________________