69
Lens diseases Wen Xu Eye Center, 2nd Affiliated Hospital Zhejiang University
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | gyles-thomas |
| View: | 216 times |
| Download: | 0 times |
Lens diseases
Wen XuEye Center, 2nd Affiliated Hospital
Zhejiang University

The most common cause of painless, progressive loss of vision today is
Cataract
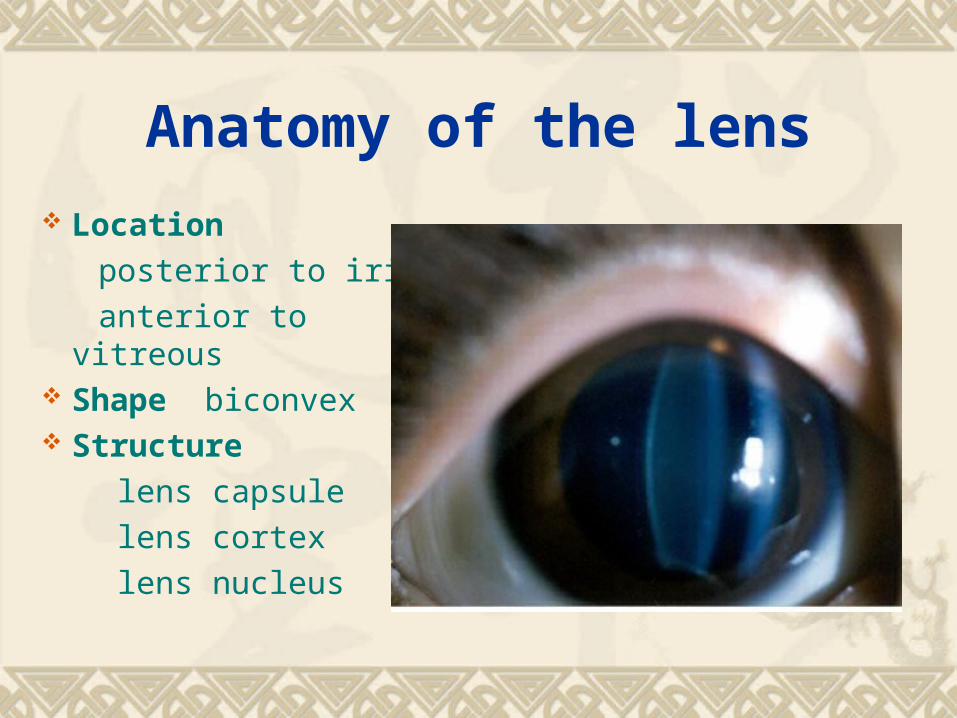
Anatomy of the lens
Location
posterior to iris
anterior to vitreous Shape biconvex Structure
lens capsule
lens cortex
lens nucleus
Physiology of the lens
No vessel, nerve and transparent.
Derive nutrients from the aqueous humor
Significant refractive medium
Accommodative function
No immediate relation with adjacent tissues
Complex metabolism
Simple disorders: transparency and location change
Cataract
Definition: opacification of the lens epidemiology:
clinical cataract
corrected vision<0.5
Cataract
Mechanism:
many factors lens capsular damage
osmosis increase,loss of protective screen,metabolic disorders protein degeneration, cell apoptosis lens opacify cataract
Cataract Classification: by cause: congenital, senile(age-related), complicated,
metabolitic, drug-induced, toxic, traumatic, secondary
by age:congenital, acquired
by location: cortical, nuclear, subcapsular
by shape: dot-like, coronary, lamellar
by degree: immature, intumescent, mature, hypermature
CataractSymptoms: decreased vision: most obvious and important
decreased contrast sensitity
refractive error: myopia,astigmatism
monocular diplopia or multiple vision
glare: scattered light rays
poor color discrimination:blue spectrum
Cataract
Signs: The lens is best examined with the pupil
dilated. A magnified view of the lens can be obtained with a slit-lamp or by using the direct ophthalmoscope with a high plus (10+) setting

Cataract
Grade’s standards of nuclear hardness:
Ⅰ transparent,no nucleus,soft
Ⅱ yellow-white or yellow,soft
Ⅲ dark yellow,moderate hard
Ⅳ brown or amber, hard
Ⅴ brown or black,extremely hard
(I) Age-related cataractDescription: the most common type, most patients are beyond
their 50’s. The incidence goes up with aging. It is the
first rank of ophthalmic diseases leading to blindness
Risk factors: Many factors are involved include age, occupation,
sex, ultraviolet radiation, diabetes, hypertension,
positive family history, nutritious condition
(i) Cortical Cataract
The most common typeFour stages:
(1) incipient stage
(2) intumescent stage or immature stage
(3) mature stage
(4) hypermature stage
1. incipient stageFeatures: a 、 cuneiform( 楔形 ['kjunɪə,fɔrm]) opacity
b 、 lamellar seperate
c 、 vacuole
d 、 cracks
e 、 no vision damage
Tests: a 、 slit-lamp b 、 transillumination

2. intumescent stage or immature stage
Features: a 、 more serious opacity b 、 larger volume and more shallow anterior chamber c 、 iris shadow d 、 obvious vision decrease e 、 myopia
Tests: a 、 slit-lamp b 、 oblique illumination
Matter needs attention: angle-closure glaucoma


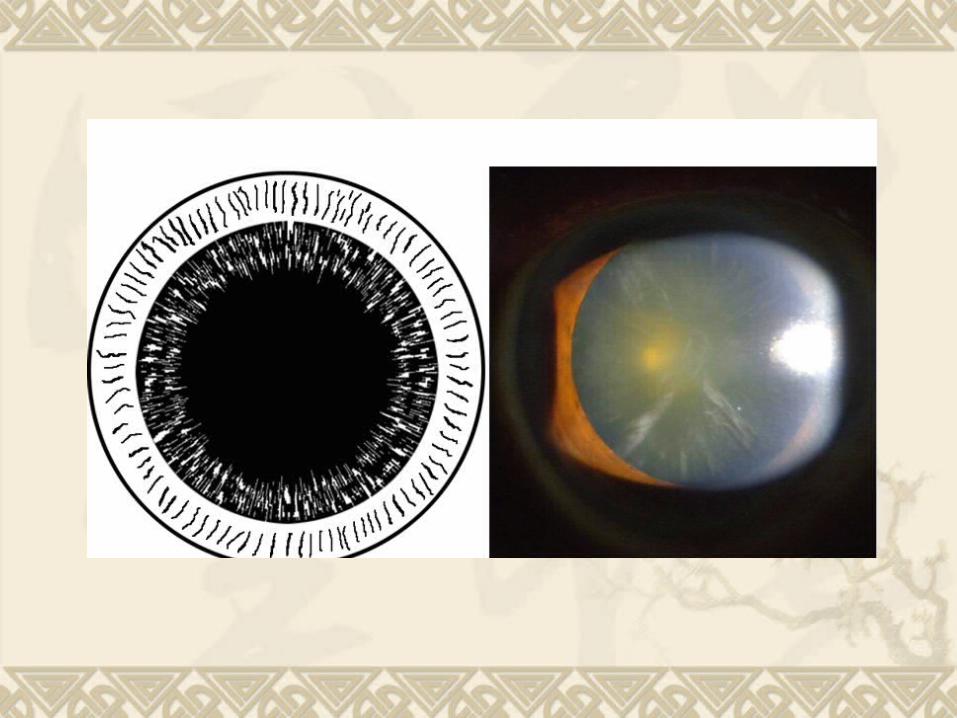
3. mature stage
Features: a 、 complete opacity, milky white, iris shadow
disappear
b 、 volumn and anterior chamber regain normal
c 、 vision: LP or HM before the eye
Tests: a 、 slit-lamp
b 、 flashlight

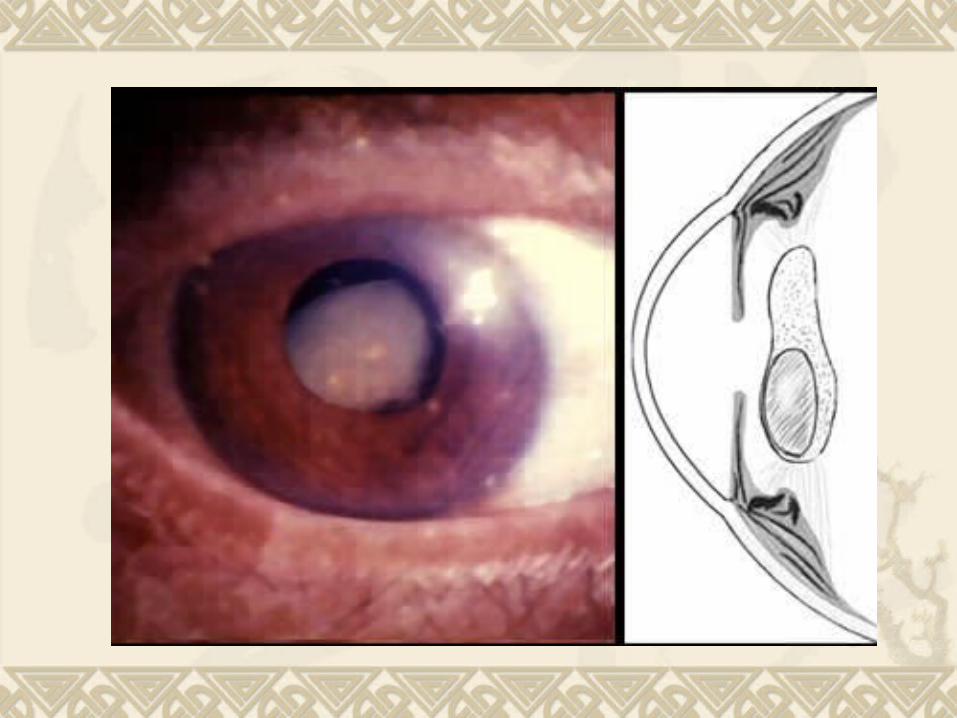
4. hypermature stage
Features: a 、 smaller volumn,wrinkled lens capsule,claybank
and fallen nucleus (Morgagnian cataract) ,superior
of anterior chamber deepens while inferior is the
opposite,ridodonesis.
b 、 laceration of lens capsule,lens luxation.
c 、 phacoanaphylactic uveitis,phacolytic glaucoma
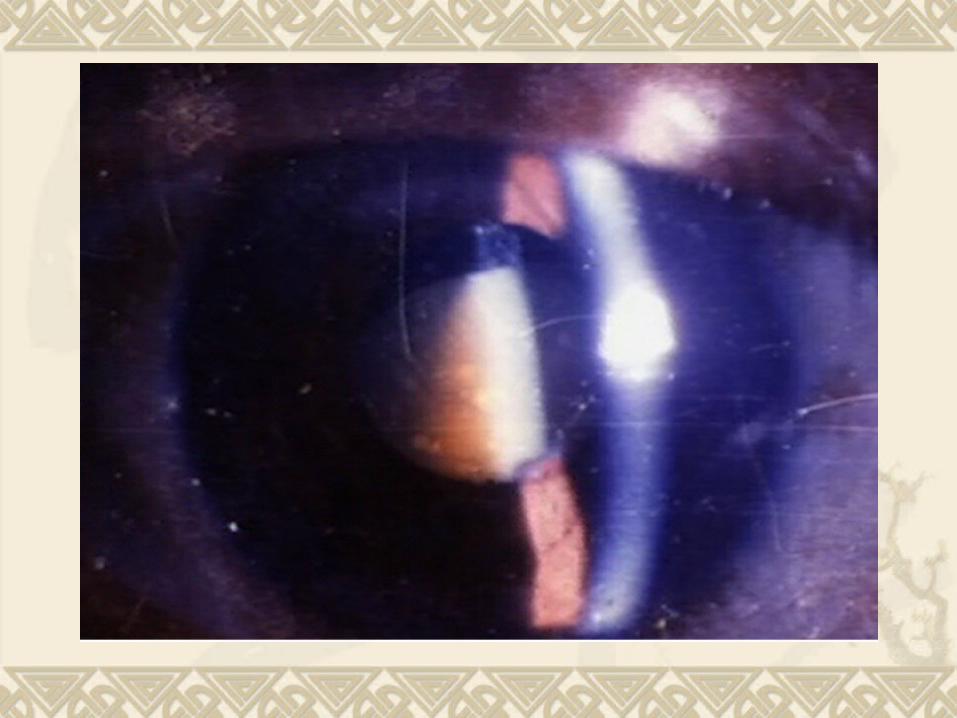
(ii) Nuclear Cataract
Features: a 、 start earlier,generally on 40’s,slowly
progressive, not likely to be mature.
b 、 nuclear opacity: start by embryonic nucleus.
c 、 vision: no vision damage early on, myopia
Tests: slit-lamp 、 transillumination 、 oblique illumination

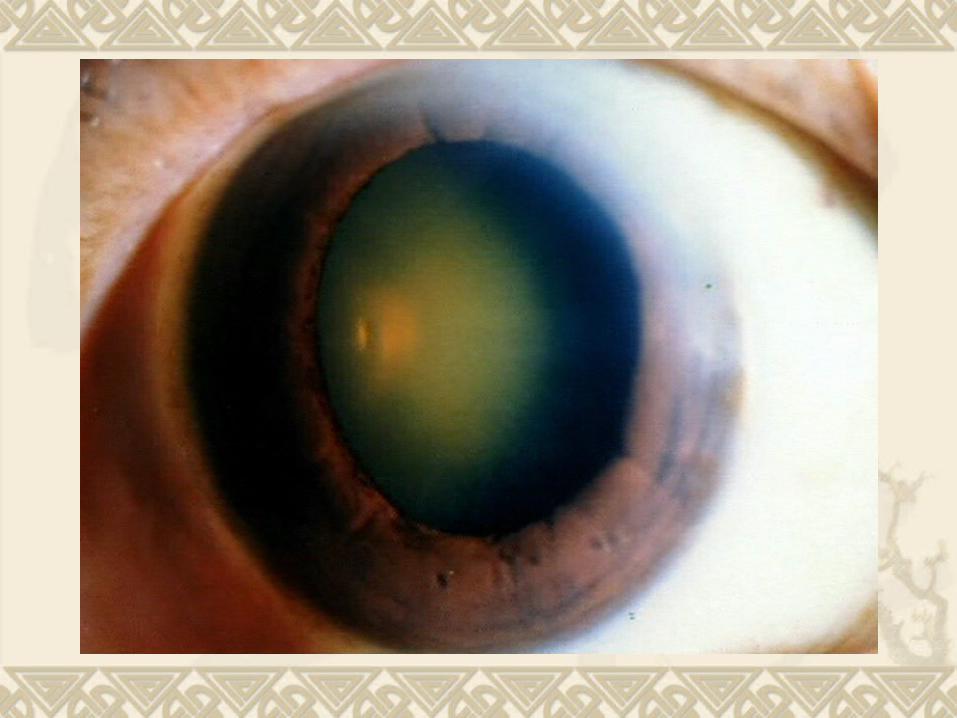
(iii) Subcapsular Cataract
Features: a 、 start earlier
b 、 posterior subcapsular cataract: cause
obvious vision defect early on
c 、 cupuliform( 杯状 ) opacity of posterior pole

(II) Congenital CataractFeatures: present at birth or appear shortly thereafter; unilateral or bilateral;
may be alone or associated with other ocular or systemic
congenital abnomalities
Etiology:
(1) hereditary factors(chromosome,gene)
(2) environmental factors (matrix disease) when pregnance <3 m:
virus infection; drugs,metabolic diseases
(3) undetermined causes
Classification
According to location, form and degree anterior polar cataract
posterior polar cataract
perinuclear cataract
coronary cataract
punctate cataract
total cataract
membrane cataract
nuclear cataract

Congenital cataract
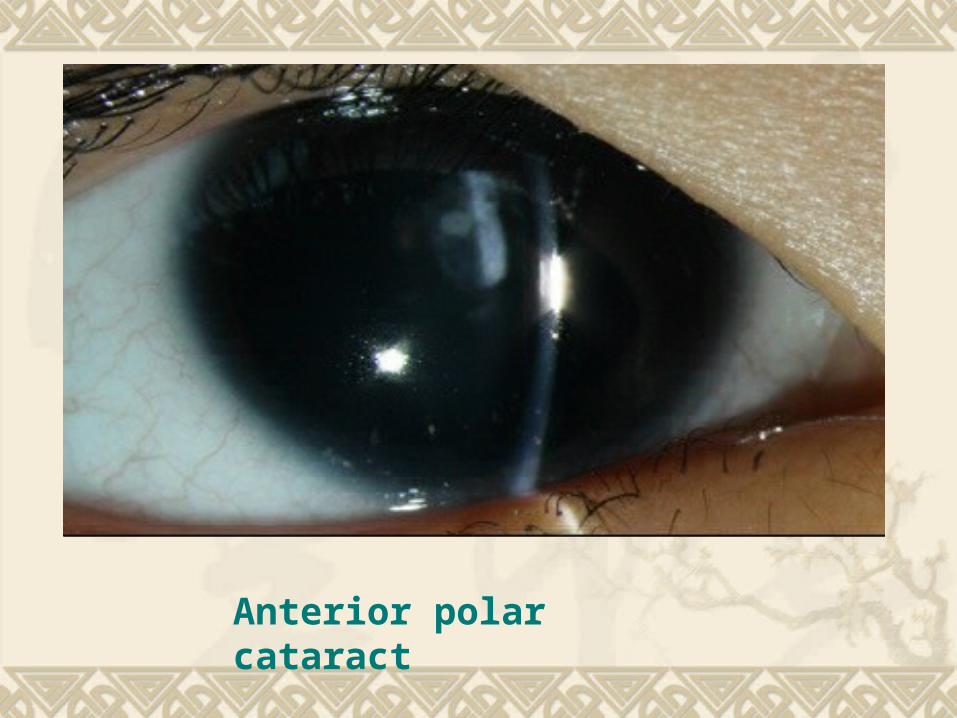
Anterior polar cataract

Posterior polar cataract
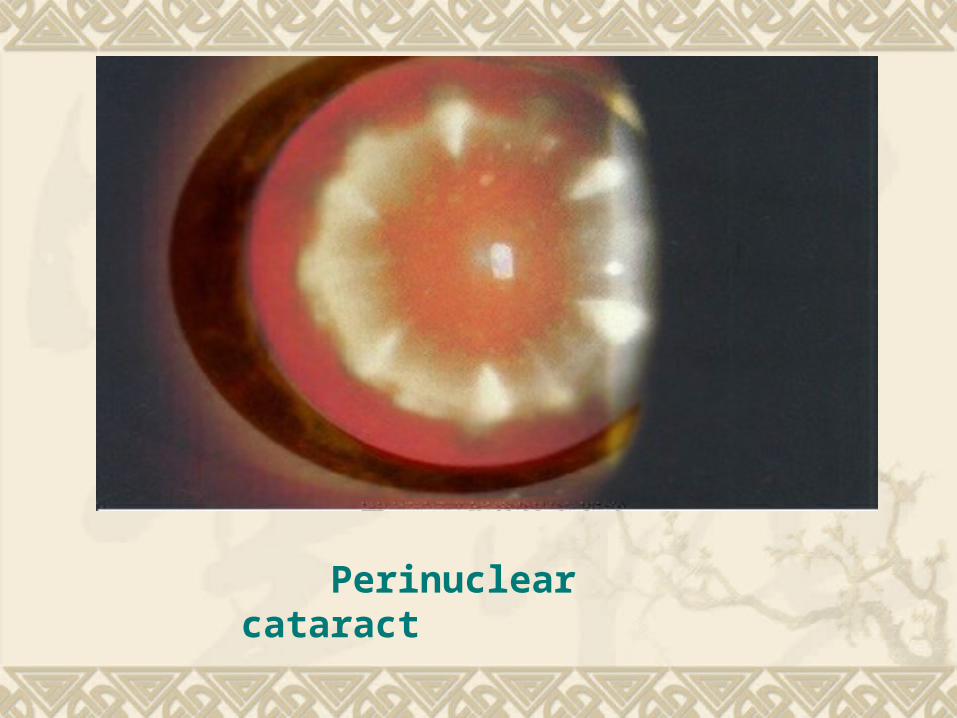
Perinuclear cataract
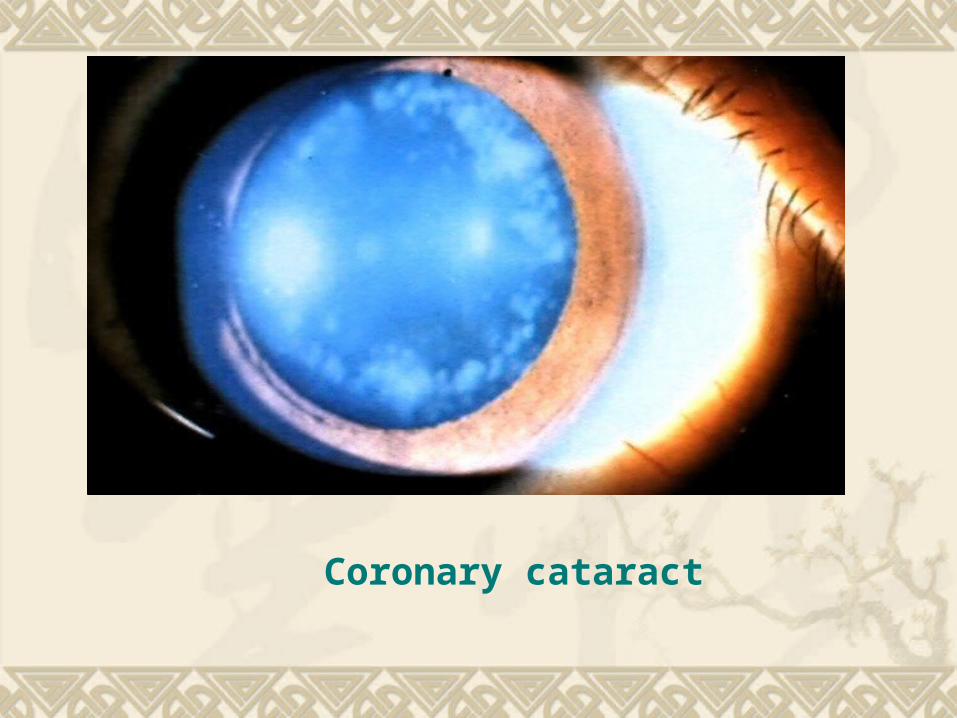
Coronary cataract

Punctate cataract
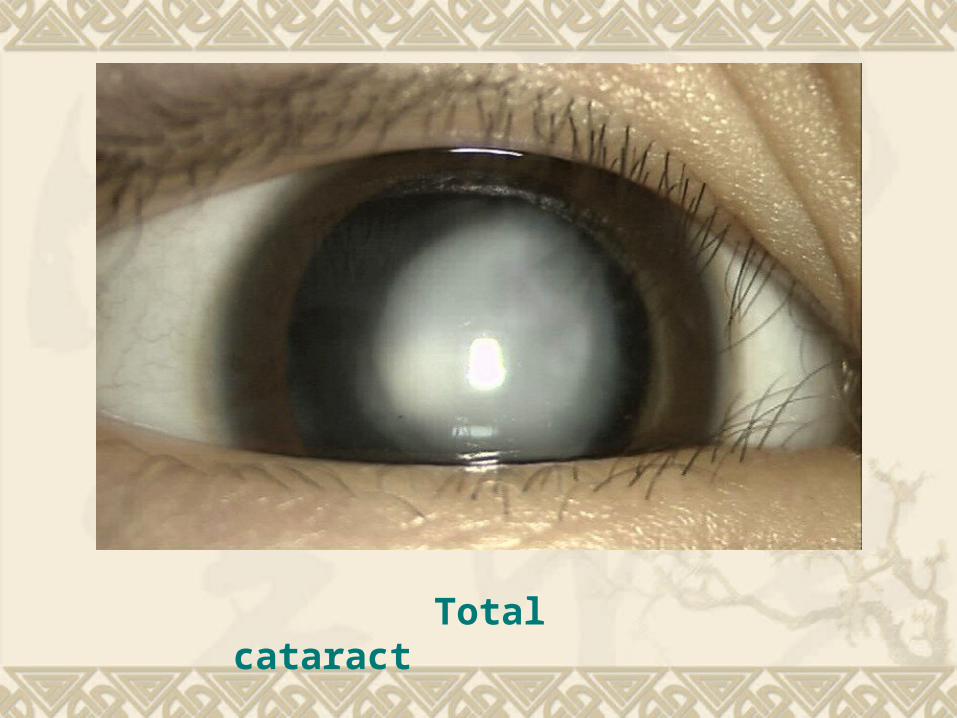
Total cataract
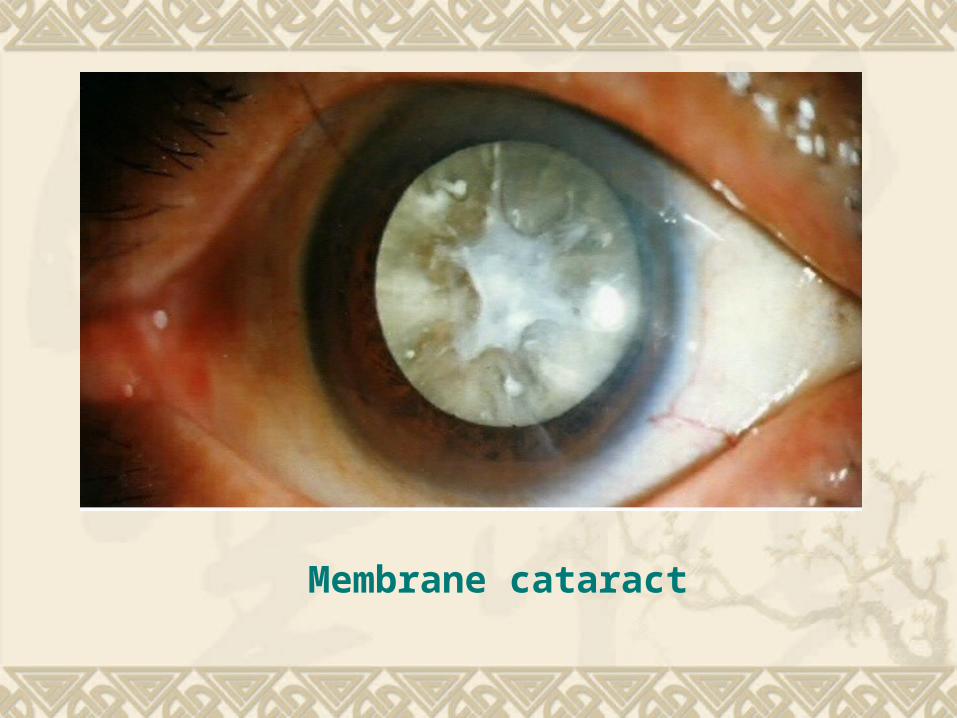
Membrane cataract
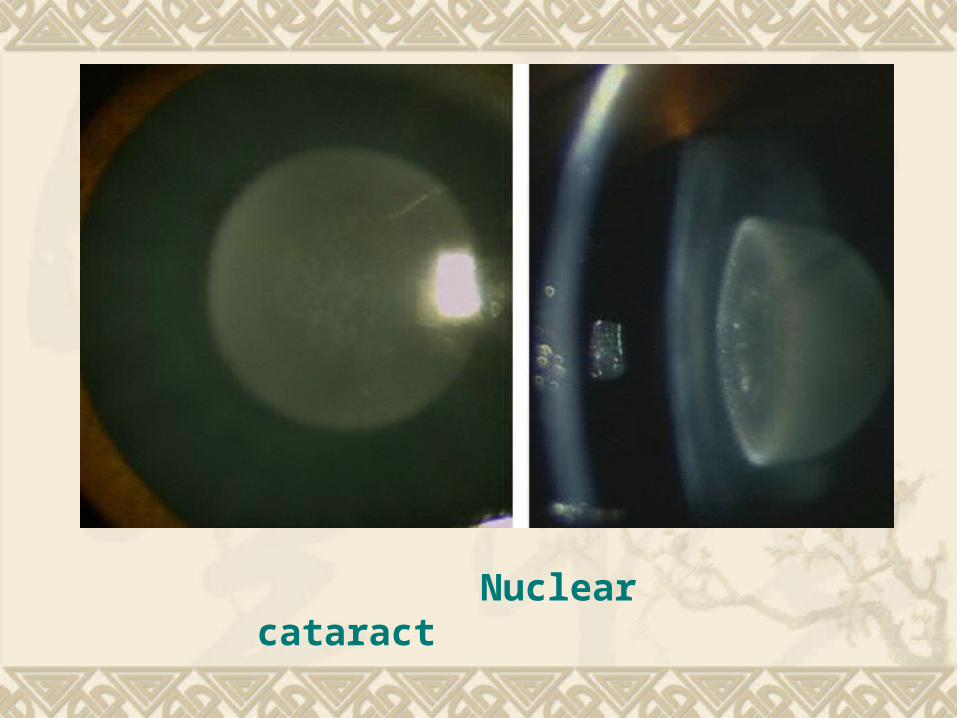
Nuclear cataract
(III) complicated cataractFeatures:
ocular inflammation or degenerative disorders→
nutritious or metabolic defect → lens opacity
Common causes:
corneal ulcer, glaucoma, uveitis,retinal
detachment, retinitis pigmentosa, intraocular
tumor,high myopia, etc.
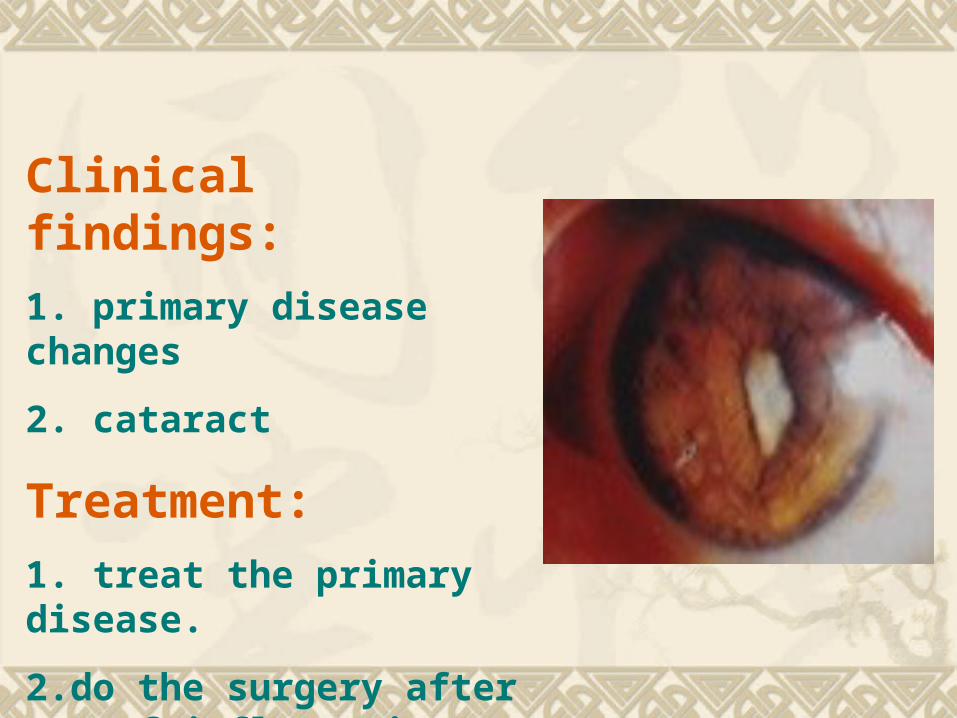
Clinical findings:
1. primary disease changes
2. cataract
Treatment:
1. treat the primary disease.
2.do the surgery after 3 m of inflammation control
(IV) Metabolic cataract
Diabetic cataractGalactose cataract: lack of enzyme
Tetany cataract: low blood calcium
Wilson’s disease (Hepatolenticular Degeneration): KF ring, sunflower-shaped
opacity,copper.
1. Diabetic cataract
Mechanism:
blood sugar↑ →sugar in the lens↑ → change
into sorbitol→plasma osmotic pressure↑
→absorb water→fibers swellen and
degenerate→lens opacity
classification: (1) real diabetic cataract
(2) age-related cataract of diabetic patientsClinical findings: (1) the first type: teenagers,bilateral,rapidly
progressive,eading to total cataract,combined
with refractive changes according to blood sugar
(2) the second type: high incidence,start earlier, fast
progressive, easy to be mature,similar with
senile cortical cataract
Treatment: (1) positively treat diabetes,control blood
sugar
(2) do the surgery if permitted
(3) positively postoperational infection and
bleeding prevention
(V) Drug-induced and toxic cataract
Corticosteroid cataract
Chlorpromazine cataract
Miotic cataract
Trinitrotoluence cataract
Metals
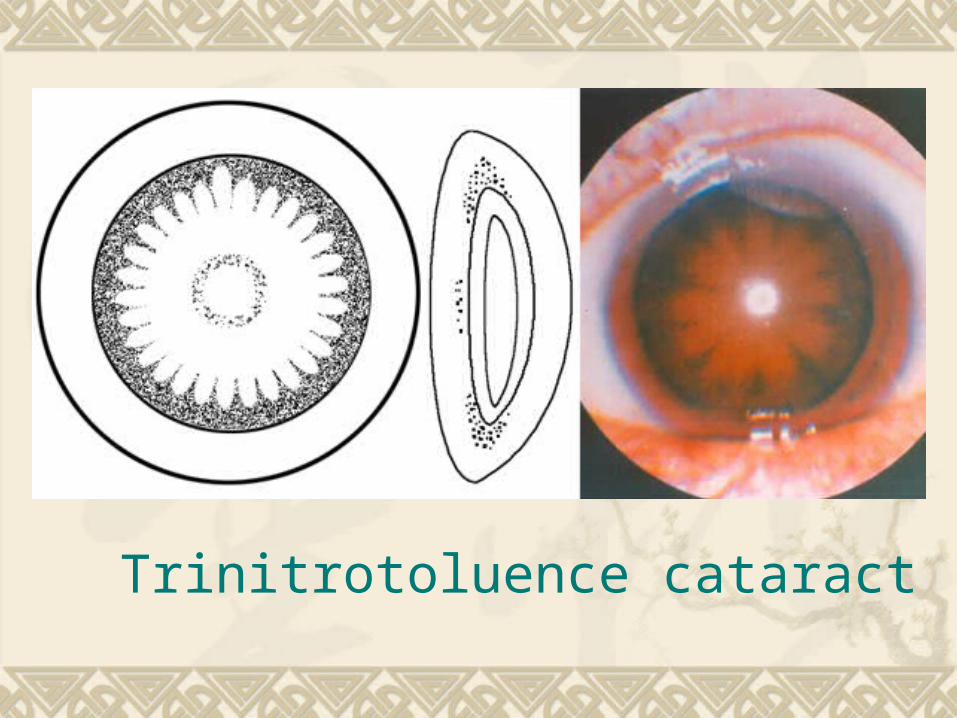
Trinitrotoluence cataract
(VI) Traumatic cataract
Classification: Contusive cataract
Penetrating cataract
Chemical injuries cataract
Radiation cataract
Electric cataract
Treatment: observation or surgery
(VII) Secondary cataract
Definitions: opacification of the posterior capsule due to partially
absorbed traumatic cataract or following extracapsular cataract extraction (posterior capsular opacification). It is the most common complication of cataract surgery
Clinical findings: vision decrease after cataract surgery;
Elschnig’s pearls
It is a significant problem in almost all pediatric patients unless the posterior capsule and anterior vitreous are removed at the time of surgery. Up to 30%-50% of all adult patients develop an opaque secondary membrane after cataract surgery
Treatment: neodymium:YAG capsulotomy

Treatment of cataract
There are many kinds of medicines,but none
has certain positive effect
Surgery is the chief method
Surgical treatment
Timing of the surgery: a 、 mature stage→visual acuity
b 、 consider the surgery conditions and the subjective requirements of patients
Preoperative Examination & preparation Ocular: VA,LP,color vision,anterior
segment,fundus,IOP,SLE ,EKG,VEP,ultrasonic,etc. System:BP,blood sugar,etc. Corneal curvature,the axial length of the
eye.calculate the diopter of the IOL Endothelial cell acount (specular microscopy) Wash conjunctival sac and lacrimal canal,dilate
the pupil
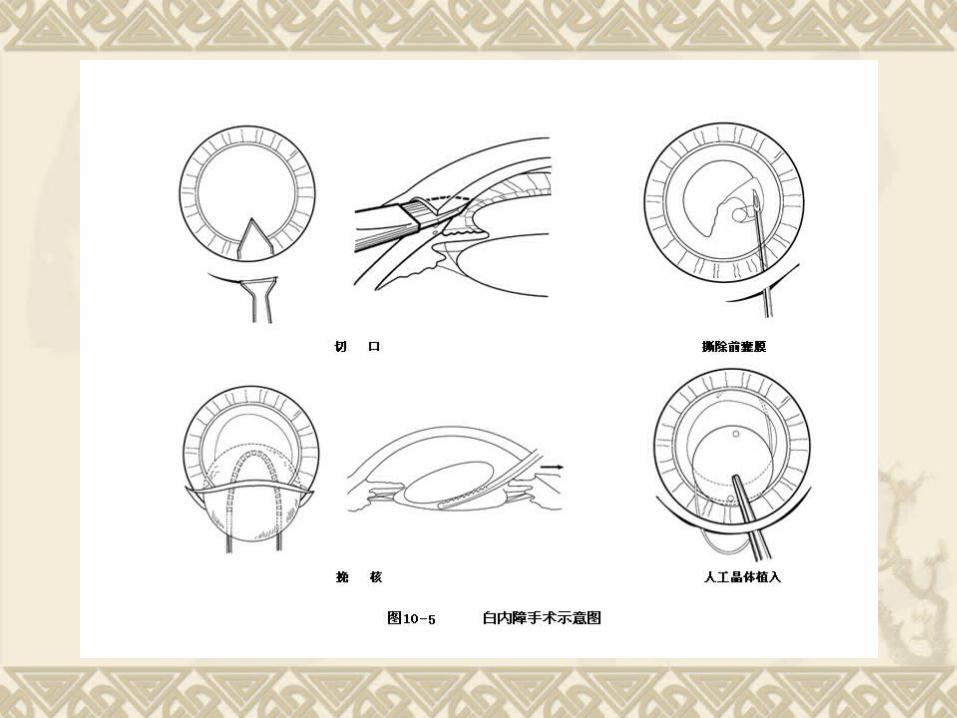
Way of the surgery
Couching( 针拨 ) of lens
Intracapsular cataract extraction (ICCE)
Extracapsular cataract extraction (ECCE)
Phacoemulsification (PHACO)
Laseremulsification
Intraocular lens implantation
Surgical complications
Complications during the surgery
(1)shallow or no anterior chamber
(2)intraocular tissue lesion
(3)hemorrhage
(4)posterior capsular rupture
Postoperational complication (1)hemorrhage
(2)high IOP
(3)endophthalmitis
(4)chronic uveitis
(5)posterior capsular opacification
(6)corneal astigmatism
(7)retinal phototoxicity
(8)cystoid macular edema, CME
Postoperational complications of IOL implantation
(1)pericorneal fibrous proteins exudation
(2)dislocation of IOL
(3)secondary glaucoma and decompensation of
corneal endothelium
(4)diopter inaccuracy of IOL
Refractive correction of aphakia
IOLs :Multifocal, Accommodatable
Spectacles
Contact lens
Refractive surgeries: keratophakia,
keratomileusis, epikeratophakia
Dislocated lens or ectopia lentis
Causes (1) congenital
simple dislocation; combined with lens or ocular
abnormalities; systemic syndromes (Marfan syndrome,
homocystinuria, Marchesani syndrome, Ehlers-Danlos
syndrome)
(2) traumatic
(3) spontaneous
Clinical findings (1) Partial dislocation:
the edge of the lens and the zonular fibers holding it in
place can be seen in the pupil. It is often complicated by deepen anterior chamber,iridodonesis and vitreous hernia. High myopia and monocular diplopia,or even secondary glaucoma may occur
(2) Complete dislocation:
include pupil entrapment,dislocated into anterior
chamber, dislocated into vitreous cavity,dislocated into
subconjunctiva or even extraocular

complications (1)Uveitis
(2)Secondary glaucoma
(3)Retinal detachment: the most common
(4)Corneal opacification

Treatment
(1) nonsurgical therapy: If no complications, dislocated lenses are best left
untreated. Close conservation and spectacles or contacts may have some value
(2) surgical therapy:
If uveitis or uncontrollable glaucoma occurs, lens
extraction must be done. The technique of choice is limbal or pars plana lensectomy using a motor-driven lens & vitreous cutter

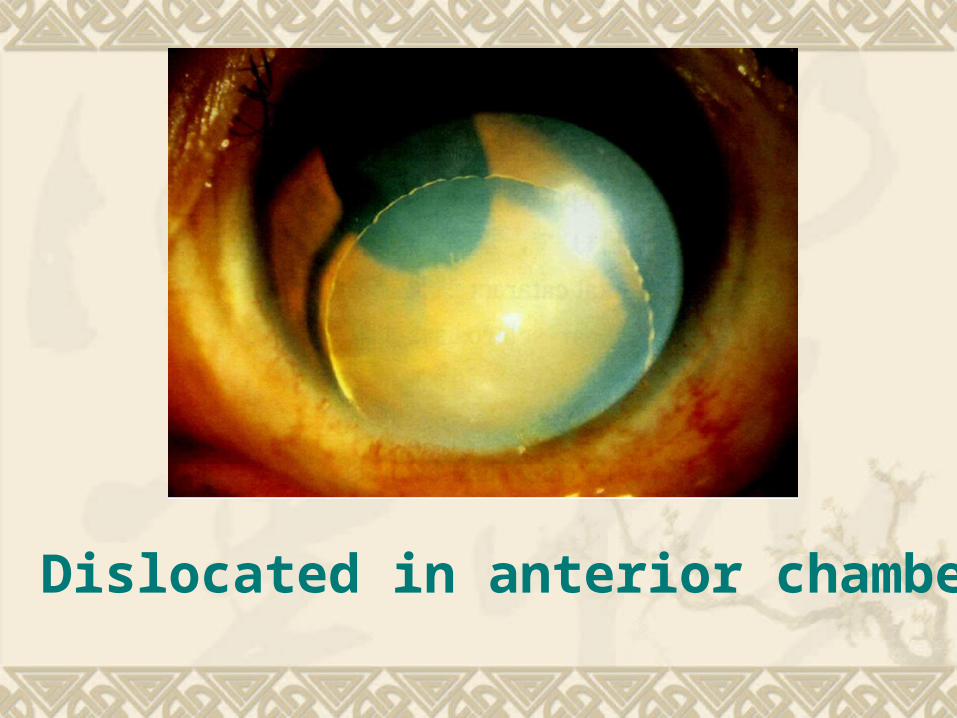
Dislocated in anterior chamber
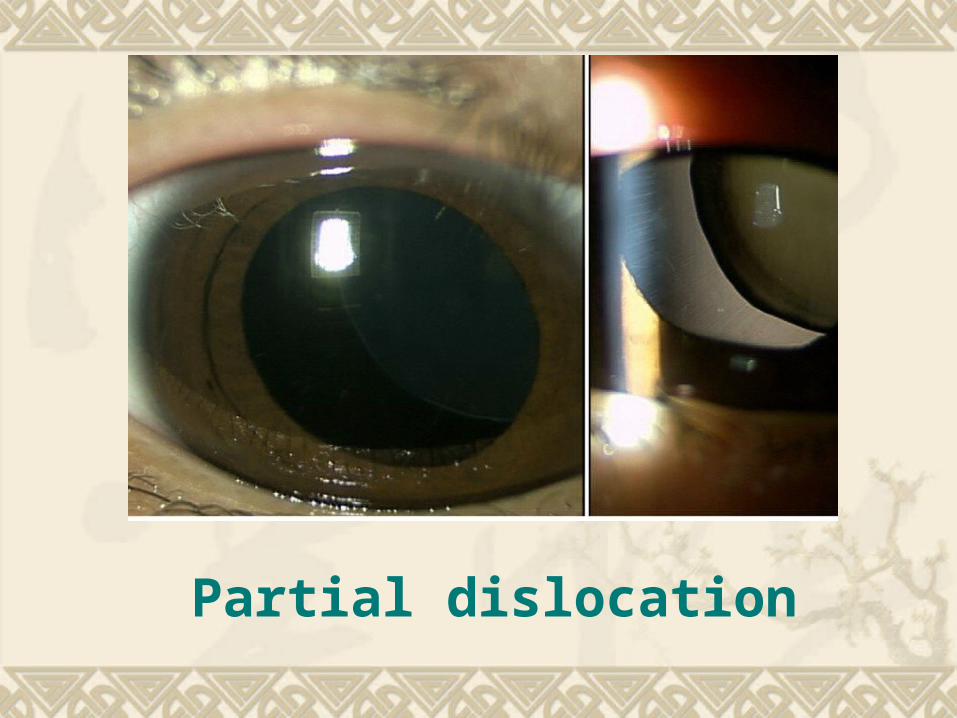
Partial dislocation
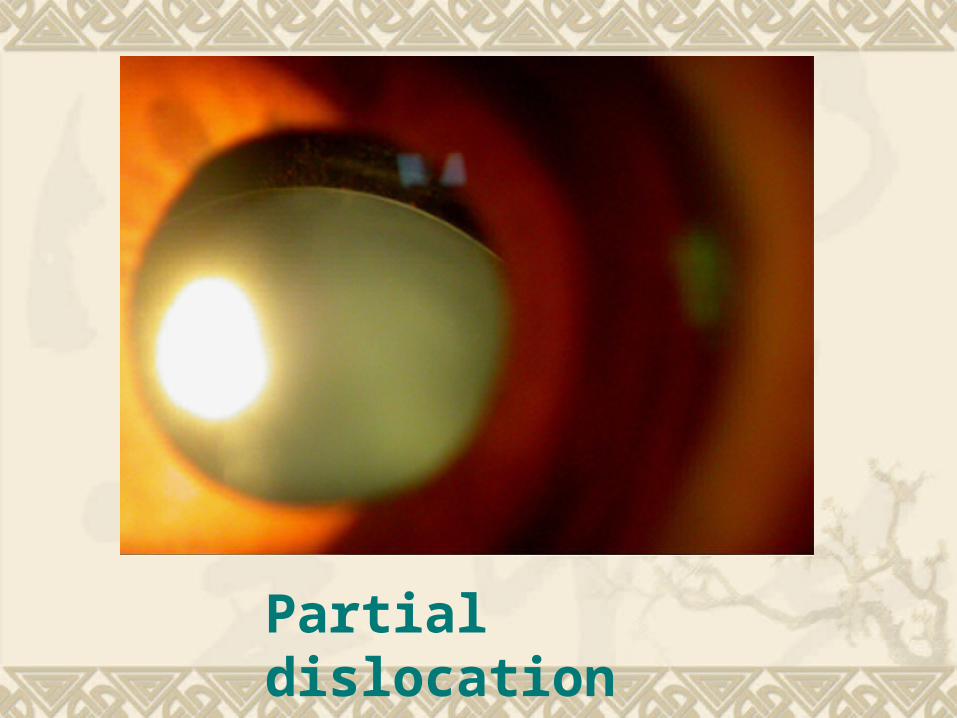
Partial dislocation






![TAESOO KIM[6] Seulbae Kim, Meng Xu, Sanidhya Kashyap, Jungyeon Yoon, Wen Xu, and Taesoo Kim. Finding Semantic Bugs in File Systems with an Extensible Fuzzing Framework. In Proceedings](https://static.documents.pub/doc/80x56/5e7a8f876e2c22260f530afd/taesoo-kim-6-seulbae-kim-meng-xu-sanidhya-kashyap-jungyeon-yoon-wen-xu-and.jpg)










