Clinical leprosy is characterized by varying manifesta- tions between tuberculoid and lepromatous leprosy. In the former state the patient is able to elicit a cell-mediated immune response whereas in the latter, there is usually a humoral response. An understanding o f this immuno- logical balance is crucial in the search for a vaccine which will control the disease. The development o f a possible anti- Mycobacterium leprae vaccine has been advanced by the isolation o f organisms from the infected tissues o f the nine-banded armadillo, Dasypus novemcinctus: 125 000 doses can be prepared from one animal In addition, recent studies on the biochemical activities o f these organisms may provide the knowledge required to allow cultivation on a laboratory medium. Eventually it may be possible to produce a combined leprosy:tuberculosis vaccine for use in those parts of the world where both diseases are prevalent.
The origins of leprosy are lost in antiquity and we must rely on historical and biblical scholars to interpret ancient writings. According to Baron 1, the disease was described in Egyptian papyri written circa 5000 BC. Indeed, some historians believe that the source of leprosy is the central plain of Egypt in the upper reaches of the Nile 2'3. In his History of Egypt, Manetho (270 BC) indicated that the Israelites were allowed to leave Egypt in 1250 BC because they had leprosy 4. b.:xodus 4: 6-7, can be interpreted as an indication that Moses had leprosy, but was cured. According to Fiennes 5 biblical references indicate a true knowledge oftuberculoid or anaesthetic type leprosy - see Leviticus 13 and 14, Numbers 12: 9.
Modern controversy is centred on the translation of the Hebrew tsara'ath in the Old and New Testaments. Literally, the word is associated with scaly blemishes on the skin and biblical references to leprosy could certainly have described a variety of dermatological conditions, e.g. psoriasis, vitiligo, seborrhoeic dermatitis or scabies.
Whether leprosy was transported to India from Egypt or whether there were two independent foci existing at the same time is unknown. However, accounts of leprosy are recorded in Indian scripts of 600 BC and Japanese scripts of 400 BC. Hippocrates (c. 420 BC) used the word lepta but this was applied to skin diseases very similar to psoriasis
Department of Microbiology Research Unit, University of Glasgow, Alexander Stone Building, Garscube Estate, Bearsden, Glasgow G61 1QH, UK
and not to leprosy. The troops of Alexander the Great may have introduced leprosy to Greece after their return from the Indian campaign in 327-326 BC. The disease was known to Aristotle and was described by Erasistratos (300-250 BC) but was referred to as elephantiasis Graecorum tuberosa.
Leprosy is thought to have reached Europe by way of Pompey's legionaries or slaves brought from Africa. A clear case of leprosy in fourth century Britain was detected by ReadeP in the bones exhumed from the Romano-British cemetery at Poundbury Camp, Dorchester. The individual's shin bones were rough and showed periostitis. The phalanges were eroded and pointed (Figure 1). The right foot also showed marked resorption of the capitula. Was the individual an indige- nous person or a legionary brought to Britain from the Middle East? The disease apparently reached the rest of Europe from the tenth to the fourteenth century and it seems certain that the Crusaders re-introduced the disease to Britain.
The disease was also prevalent in Scandinavian countries. It is ironic that Mycobacterium leprae was the first bacterium to be associated with a specific human disease when it was identified by the Norwegian, Dr G. Armauer Hansen in 18747. In a fascinating study, Irgens 8 followed the decline of leprosy in Norway from 1856 until the 1950s using the epidemiological data obtained from the National Leprosy Registry of Norway for 8231 patients. The decline was such that today the disease has been almost eradicated in Norway; between
Figure 1 Radiograph of the Poundbury Roman leper feet [reproduced from Reader, R. J. Archael. ScL 1974, 1, 205 by permission of the.Department of the Environment, HM Government, London Crown copyrightl
S K U L L OF K ING ROBERT BRUCE
showing chronic disease of facial bones, suppozed to be leprosy
(Fu,m a cast in the ,4 natomical Museura, University of Edinburgh)
Leprosy - - in pursu i t o f a vaccine: D.ES. Stewart-Tuff
Leprosy was introduced into America either from Spain and Portugal or from West Africa. The disease continues to be a serious problem in South America (208 679 cases in a WHO survey 13) especially in Brazil, Columbia, Paraguay and Argentina. For many years there has been a campaign to remove the terms leper and leprosy from common usage. Although the Brazilian state of Sao Paulo discontinued the use of the pejorative terms in 1968 ~4 support for this was obtained only from the US Public Health Service, Portugal, Cameroon and some services in Latin America. Rotberg '5 proposedHanseniasis for leprosy and Mycobacteriurn hansenii for Mycobacterium leprac: The International Committee on Systematic Bacteriology declined such a change and concluded that whatever name the organism received, it would soon become associated with the disease in the minds of ordinary people. There does seem to be a case for considering the use of an alternative terminology for the disease in countries where there is a high incidence and where the term leprosy is synonymous with filth and uncleanliness. In educated societies, as my daughter pointed out, one could find the meaning of Hanseniasis in a dictionary! Unlortunately, a change in name will not automatically correct the fear and persecution long associated with the term leprosy. There would seem to be a minimal advantage associated with a change in nomen- clature of the bacterium. No doubt the debate will continue; opposing opinions are presented by Rotberg ~ and Stringe?L
Whatever the name, some 15-20 million people in the tropical and sub-tropical areas of the world where the disease is endemic, are infected with M. leprae and there is a real need for an efficacious vaccine.
Figure 2 Skull of King Robert Bruce showing chronic disease of facial bones supposed to be leprosy [reproduced from Comrie, J.D. "History of Scottish Medicine' Vol. 1, p 193 by permission of Bailliere Tindall]
1921-1970, only 14 patients were reported as compared to 1088 patients with the year of onset before 1851. The relative frequency of lepromatous leprosy was 53.8% and this type of infection was more frequent in males than in females in the 25-60 age group. The rapid decline in leprosy over the period was attributed to the physical isolation of infectious patients in leprosy hospitals.
M¢ller_Christensen 9,~0 identified bone alterations due to leprosy in 650 skeletons from the cemetery of the Naestved mediaeval leprosy hospital in Denmark and founded the art of osteoarchaeology in leprosy. In many cases the sharp anterior nasal spine of the skull may disappear because of bone resorption. The median maxillary alveolar process atrophies with increasing exposure of the roots of the upper front teeth 9. The skull of King Robert Bruce of Scotland shows the extreme case where bone atrophy causes loss of the incisors (Figure2) H. StJbramanianl and Max'ks lz reported thal aheolar bone loss around the maxillary central incisors was signi- ficantly greater in leprosy patients in the lepromatous range.
In England it was forbidden tbr leprosy sufferers to enter London. Institutions known as lazar houses, after the nursing order of the Knights of St Lazarus. were established throughout Europe. There were some 326 of these in Britain at the time, see Figures 3 and4, but by the end of the eighteenth century the incidence of leprosy had declined in Europe.
The clinical disease
Transmission o f M. l e p r a e There is great uncertainty about the precise mode of
transmission of M. leprae from one human being to another. Apart from the finding of an indigenous disease in armadillos, no animal reservoir has been found. In addition, epidemiological evidence has eliminated the possibility that the armadillo has any importance in the spread of disease. There is no evidence at present to implicate the healthy human carrier as a source of infection.
Figure 3 Leprosarium chapel of Saint Bartholomew's Hospital, Cowley Road, Oxford; built in 1137. Photograph kindly provided by Professor Graham Weddell, Oxford
Vaccine, Vol. 2., December 1984 239
Leprosy- in pursuit o f a vaccine: D.ES. Stewart-Tuff
Figure4 (A) Ten "lepers' healed by Christ, from an Eng sh manuscript dated 1397 [reproduced from Ms. LandMisc. 165 by permission ofthe Bodleian Library, Oxford fol. 363R]. (B) Case of diffuse lepromatous leprosy with leonine facies. Note the similarity with the facial characteristics shown in (A). Photograph provided by Dr. Stanley G. Browne
It is generally supposed that M. leprae is a weakly pathogenic organism with slight invasive powers which causes an infection after a long incubation period. In many instances the first sign of leprosy is a single skin lesion; this may take the form of a tuberculoid patch in a high proportion of patients (Figure 5). In lepromatous leprosy patients, large numbers ofM. leprae are found in the upper part of the corium of the skin. Organisms may sometimes be found in the subcorneal and corneal layers of the epidermis. A minor scratch could bring these organisms to the skin surface. Organisms may also pass to the surface in secretions from sebaceous glands. The discharge from ulcerative skin lesions usually contains many bacilli. Shepard and McRae TM showed that as few as ten solid-staining bacilli could cause an infection in mice. Consequently, transmission by contact of abraded skin with the discharge of one of these ruptured vesicular lesions, is possible.
In 1960, Dunga119 queried the role of insects in trans- mission of leprosy. It was found that species of Musca Calliphora and Stomoxys were capable of taking up large numbers of solid-staining M. leprae from nasal mucus 2° and it is not uncommon to see flies on open ulcers. These organisms may be transferred by the insects when they alight on skin abrasions and cuts. The mouth-parts of Stomoxys are also contaminated so in this case direct t r a n s m i s s i o n can occur during feeding; biting insects are abundant in countries where leprosy is endemic.
In lepromatous leprosy patients, large numbers of organisms are obtained from the nasal dischargeZL This presents the possibility that leprosy could be transmitted by droplet infection. This was shown to be theoretically possible in thymectomized, irradiated mice (T900r) exposed to aerosols containing I × 105 M. leprae. Two years later, 10 out of 30 mice had acid-fast bacilli in one or more homogenates from ears, footpads, nose or lungs 2~'23.
Desikan 24 found that M. leprae survived for nine days outside the body so dust-borne organisms could be acquired by susceptible people. If the usual route of transmission was by direct droplet infection, one would expect an even greater incidence than >1% found in susceptible groups. The real question is whether the number of organisms that could be transmitted by the respiratory route exceeds the minimal infective dose.
Pedley z5 microscopically cxamined the breast secretion of a non-lactating 60-year-old Nepali woman with lepromatous leprosy. Large numbers of acid-fast solid- staining bacilli were found and also numerous globi. He concluded that if the woman had been of child-bearing age and lactating, her child would have been ingesting large numbers of M. leprae. It was suggested that the primary lesion may be located in the gastro-intestinal tract. However, Leiker 26 dismissed this possibility because a high incidence of leprosy would be expected in children aged between 4-5 years who had been breast-fed by mothers with lepromatous leprosy. The incidence of leprosy in children of this age group is comparatively low.
At present, it does seem that the main route of transmission is predominantly via the skin, but we should be aware of other routes which may give rise to a low incidence of disease under certain circumstances.
Disease manifestation in m a n The clinical appearance of leprosy varies between two
polar forms - - tuberculoid (TT) and lepromatous leprosy (LL). Between these, it is possible to find patients with varying manifestations of the typical polar lesions so borderline tuberculoid (BT), borderline or indeterminate (BB) and borderline lepromatous (BL) stages have been
2 4 0 Vaccine, Vol. 2., December 1 9 8 4
Lep rosy - in pursuit of a vaccine: D.ES. Stewart-Tuff
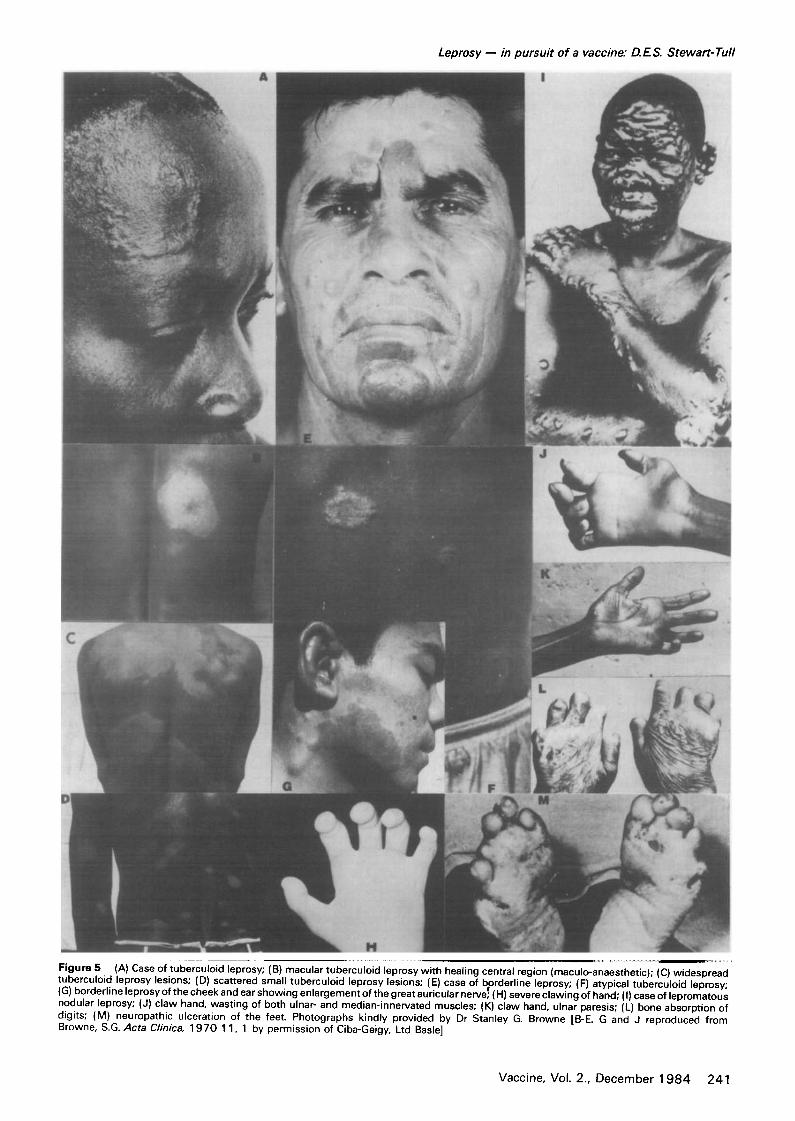
Figure S (A) Case of tuberculoid leprosy; (B) macular tuberculoid leprosy with healing central region (maculo-anaesthetic); (C) widespread tuberculoid leprosy lesions; (D) scattered small tuberculoid leprosy lesions; (E) case of bqorderline leprosy; (F) atyp ca tuberculoid leprosy; (G) borderline leprosy of the cheek and ear showing enlargement of the great auric ula r nerve; ( H} severe clawing of hand; (I) case of lepromatous nodular leprosy; (J) claw hand, wasting of both ulnar- and median-innervated muscles; (K) claw hand, ulnar paresis; (L) bone absorption of digits; (M) neuropathic ulceration of the feet. Photographs kindly provided by Dr Stanley G. Browne [B-E. G and J reproduced from Browne, S.G. Acta Clinica, 1970 11, 1 by permission of Ciba-Geigy, Ltd Basle]
Vaccine, Vol. 2., December 1 9 8 4 241
Leprosy - in pursuit of a vaccine." DES. Stewart-Tuff
recognized (Figure 5). These categories are referred to as the Ridley-Jopling classification 27.
In patients with tuberculoid leprosy, a single skin lesion may be found with a raised erythematous margin. The lesion is usually hypopigmented and anaesthetic, but as the lesion heals pigmentation and feeling are restored. If these lesions persist for a long time, peripheral nerves may become involved. Tuberculoid leprosy lesions show a marked infiltration with small lymphocytes and epithe- lioid cells of the macrophage series but M. leprae organisms are not found. The lesions are often self- healing. A patient with tuberculoid leprosy may show progression towards the borderline state as the number of lesions increase. The skin lesions are more pronounced and there may be an accompanying polyneuritis.
In borderline leprosy, reddish-coloured papules, nodules or plaques with a smooth surface are charac- teristically found. Numerous patterns of lesion dis- tribution occur on different parts of the body which accounts for the indeterminate designation of borderline leprosy. In some patients with borderline leprosy there may be evidence of lymphocyte infiltration. The macro- phages in these patients have an undifferentiated appearance.
As the disease spectrum moves towards the lepro- matous form, a patient has discrete skin lesions which may ulcerate. There is no tendency to self-healing and spread of infection may occur through skin and nasal discharges. Granulomatous lesions containing epithe- lioid macrophages packed with leprosy bacilli give rise to nodular masses. The lesions show a decrease in the number of small lymphocytes. Many different organs are affected including the kidneys, eyes, liver and spleen together with the skin and peripheral nerves.
Erythema nodosum occurs in some patients towards the lepromatous end of the spectrum. The condition is characterized by painful erythematous subcutaneous nodules. Disfigurement is common and the nodular lesions of the face and bone destruction of the nose may cause the leonine form (Figure 4). Also, the fingers may become clawed through bone resorption (Figure 5). Nerve damage may be found later which results in loss of sensory activity. Tissue destruction and infiltration of bones also occur. In advanced chronic cases, patients may suffer from blindness and severe deformities. Unless the disease is checked, there may be chronic progression; following nerve damage, the extremities may lose sensa- tion and become vulnerable to physical damage, and secondary infection of wounds is not uncommon.
Godal et aL 28 produced experimental evidence of a higher incidence of positive lymphocyte transformation in people living in an area of endemic leprosy. Recent immigrants to the same area showed a lower incidence of lymphocyte transformation. They concluded that sub- clinical infections must occur in some individuals living in these endemic areas. For a more extensive coverage of the clinical features of the disease, the reader is referred to Cochrane and Davey 29, Ridley and Waters 3°, Browne 3~ and Ridley 32.
I m m u n o l o g i c a l s ta tu s o f p a t i e n t s in the var ious s tages o f leprosy
The relationship between the cell-mediated and humo- ral immune responses are summarized in Figure 6. The ability to elicit a cell-mediated immune response against M. leprae is essential to prevent the disease progressing towards the lepromatous end of the spectrum. Bullock and FasaP 3 and Godal et al. 34 showed that lymphocytcs
from patients with tuberculoid leprosy transformed in the presence of M. leprae, whereas those from lepromatous leprosy patients did not. In addition, the migration of leucocytes from tuberculoid patients was inhibited by M. leprae as the antigen3L These findings were confirmed by the fact that such patients were able to elicit a delayed type hypersensitivity skin response to 100 /.tg or 50 /zg dinitrochlorobenzene (DNCB) 36, or phytohaemag- glutinin 33. Turk and Waters 37 found that patients who did not respond to DNCB could be sensitized to keyhole- limpet haemocyanin (KLH). They suggested the KLH provided a greater stimulus than DNCB but this also showed incomplete anergy to cell-mediated immunity in these patients.
Patients with tuberculoid leprosy also showed positive skin reactions after the injection ofM. leprae as antigen. The lepromin test is read after 48-72 h (a typical delayed response - - the Fernandez reaction) or after 3-4 weeks (a papular granulomatous reaction - - the Mitsuda reaction). Meyers, Kvernes and Binford 38 skin-tested 115 leprosy patients to lepromins prepared from human and arma- dillo tissues. They found that the lepromin derived from armadillos provoked similar responses to the human lepromin and suggested that the armadillo could be used to provide a source of standardized lepromin. Identical results were obtained by Millar, Gannon and Chan 39 who compared the Fernandez and Mitsuda reactions.
The presence of serum antibodies in leprosy patients was investigated by Abe 4°,4~ by fluorescent antibody techniques. Myrvang, Feek and Goda142 measured the serum anti-mycobacterial precipitin levels in a double diffusion in gel technique. More recently, Harboe et al. 43 detected antibodies by a radioimmunoassay done with M. leprae antigen derived from armadillo tissue. The results of these various studies showed that a gradient of humoral antibody existed which increased from the tuberculoid pole to the lepromatous pole.
As a consequence of the studies of Rees and his colleagues in London on the stimulation ofa lepromatous type of disease in immunologically compromised mice, the possibility that a dysfunction of the cell-mediated immune response in leprosy patients was explored. Newel144 suggested that this effect was genetically con- trolled because the incidence of lepromatous leprosy did not decrease in parallel with the decrease in leprosy within a population. Turid 5 postulated that the loss of cell- mediated immunity in leprosy could be due to the development of specific immunological tolerance in an individual who already has a basic constitutional defect in the ability to mount a cellular response. With progressive infiltration of the tissue with M. leprae, the defect is aggravated so that a nonspecific failure of cell mediated immunity occurs. Goda146 concluded that the precise mechanism behind the T-cell defect remains obscure. The B-cell functions do not appear to be compromised in lepromatous leprosy.
In an important study, Mehra et aL 47 investigated the role of immunological suppression in leprosy. They examined the in vitro lymphocyte responses of 61 leprosy patients and 30 normal individuals to the mitogen concanavalin A (Con A) in the presence or absence of lepromin (Table 1). Lepromin-induced suppression of the mitogenic response to Con A occurred with lymphocytes of lepromatous and borderline, but not tuberculoid, leprosy patients. At least two cell populations were involved in the in vitro lepromin-induced suppressor activity, namely an adherent cell and a T-cell. All the T-cell suppressor activity was associated with a 20-30% subset of human T-cells recognized by a "[H~ xenogeneic
242 Vaccine, Vol. 2., December 1984
Tuberculoid:
Leprosy - in pursuit of a vaccine: D.ES. Stewart-Tull
Localized, well defined lesions. Epithelioid cell response with effective phagocytosis. Responds to chemotherapeutic agents.
Lymphocytic inf i l t rat ion~
Lymphocyte transformation.
Lepromin reaction
BT
TT 9% ~ . , ~ , AFB in granulomas
in nose
AnTI-M teproe antibodies
Lepromin Mitsuda
reaction
BB BB 8 % Development of erythema nodosum
Epithelioid cells
+++
BL ~ ~ ~ F - ~ BL 10%
- -
LL 4 9 % ~
Circulating antibodies anti-mycobacterial precipit ins
Lepromotous : Diffuse lesions containing many bacilli. Accumulation of bacill i in macrophoges with foamy cytoplasm. Sluggish response to chemotherapeutic agents.
Figure 6 The spectrum of leprosy showing the characteristics associated with tuberculoid, borderline and lepromatous leprosy
Table 1 The in vitro lymphocyte responses of leprosy patients to concanavalin A in the presence or absence of lepromin
Number of patients and disease state
Lepromin induced suppression of Con A stimulation of lymphocytes
antithymocyte serum or OKT 8 rnonoclonal antibodies (TH2+/OKT8 + subset) this may be involved in sup- pressing the specific antigenic response of blood lympho- cytes of some LL and BB patients to M. leprae antigens. These authors indicated that there may be a number of mechanisms regulating the immune response toM. leprae. They cautioned that before in vitro findings should be attributed to clinical leprosy, the following questions should be answered. Namely:
(1) Is the in vitro suppression in untreated patients similarly produced by T cells and/or monocytes at various stages of the disease?
(2) Is the lepromin-induced suppression modulated by duration or type of treatment?
(3) Is the suppression specifically induced only by antigens ofM. leprae?
(4) Is there a T-cell-mediated suppression in lepro- matous leprosy in addition to that described above, which is genetically restricted?
Mehra et a148 separated T-cells from lepromatous patients into T n + and T H- subsets using the fluo- rescence-activate~] cell sorter.~The'TH2 +, some 20% of the total population, exerted a lepromin-induced suppression of the mitogenic response to Con A by the normal donor's lymphocytes. All the suppressor activity in the patients" cells appeared in the TH2 ÷ subset. It was suggested that an anti-TH + antiserum might inhibit the suppressor activity and per]nit the development of functional TH cells. These would produce lymphokines and activate macroph, ages and in the process might assist in the conversion of patients from a lepromatous to tuberculoid state, thereby restricting or eliminating the infectious organisms.
The reader is referred to a more extensive coverage of the immunological aspects of leprosy research 45,46,49-53 and on suppressor cells 54-56. These investigations have a wider significance in the field of vaccine production. Elucidation of the mechanisms which control the immune status in tuberculoid (cell-mediated response) or lepromatous (humoral response) disease states might enable vaccines to be formulated which would specifically stimulate one particular arm of the immune response.
Vaccine, Vol. 2., December 1984 243
Leprosy - - in p u r s u i t o f a vaccine: D.E.S. Stewar t -Tu f f
Therapy v e r s u s prophylaxis in leprosy
T r e a t m e n t w i th d r u g s
For many years the mainstay of therapeutic drugs for the treatment of leprosy has been the sulphone derivative 4A'-diamino diphenylsulphone (DDS or dapsone). In the mouse M. leprae was sensitive to 0.0001% dapsone in the diet; the minimal inhibitory concentration (MIC) was 0.01 pg ml -~ 57-6o. In human patients, the drug is admini- stered orally in amounts increasing slowly from 25-200 mg per week. Waters, Rees and Ellard 61 showed that 1.0 mg dapsone given daily caused the death of the majority of M. leprae in patients. The drug apparently inhibits the multiplication of deep pockets of bacilli in the tissues. Treatment is usually continued for at least two years in tuberculoid or borderline tuberculoid and for at least four years in borderline lepromatous and lepromatous disease. Browne n suggested that treatment at half dosage should be continued for life after the disease was controlled. Derivatives of dapsone have also been investigated, 4,4'- diacetyldiaminodiphenylsulphone (DADDS) suppressed the multiplication ofM. leprae in mice at a dose level of 6 pg g-~ 62. Russell et a163 showed no adverse effects produced by acedapsone after some two years of treatment.
As early as 1964, Pettit and Rees 64 produced clinical and experimental proof of the existence of secondary dapsone resistance. This resistance develops through multiple step mutation, as found with penicillin. Concern was expressed about the establishment of primary dapsone resistance since this indicated that control of leprosy by drug therapy would be unattainable 65,66. Such primary dapsone resistance in leprosy was detected in a 10 year old boy with tuberculoid leprosy 67. 'The disease progressed to the lepromatous pole during dapsone therapy and theM. leprae were found to be fully resistant to dapsone. The boy's father was a known case of leprosy with secondary acquired dapsone resistance.
Baquillon et al. 6s calculated that the prevalence of dapsone resistance in patients treated for 10-29 years was 5.7% in Bamako, Mali, see also 69,7°. Four cases of dapsone resistance in patients from the Upper Volta region were found after long term treatmentTL The rifamycin antibio- tics were shown to arrest the development of leprosy in human patients at a dose of 1.0 g day -~ 72. The adminis- tration of 0.03% in the diet of mice for two days killed the majority of bacilli 73. The orally-active rifampicin, or rifampin, was effective at a dose level of 0.6 g day -~ 74. The
bacilli were non-infectious to mice after 24 days of treatment. Similar results were obtained by Shepard, Levy and FasaW. Three rifamycin derivatives were tested against mouse footpad infections withM, leprae; although one of these was eight times more potent than rifamycin it could not be administered more than once every two weeks 76. Waters et aL 77 showed after nine years experience with the use of rifampicin in more than 100 patients with lepromatous leprosy that rifampicin was more effective than dapsone. They confirmed the rapid bactericidal effect but noted the persistence of small numbers of M. leprae after at least five years treatment. Unfortunately, Jacobson and Hastings TM obtained a rifampicin-resistant strain ofM. leprae from a patient with an infection that had persisted for thirty one years. The resistance is thought to develop as a single-step mutation of the streptomycin type.
A notable advance in the therapy of leprosy was the demonstration that a r iminophenazine derivative clofa- zimine (Lamprene B663) was not only bactericidal for M. leprae but also possessed anti-inflammatory properties 7a,8°. The effective dose of clofazimine was between 0.00001 and 0.001%8L Doses of 100-300 mg day -1 in Caucasians caused an objectionable red pigmentation of the skin. It would seem inevitable that resistance to clofazimine will eventually occur. A number of other drugs have been screened for their activity against M. leprae. Ethionamide and prothionamide possessed bactericidal activity at a dose level of 0.01-0.1% with an MIC of 0.05 pg m1-1, thiambutosine (M1C 0.5 pg ml-l), thiacetazone (MIC 0.2 p,g m1-1) and thiocarlide (MIC 0.5 pg m1-1 were bacteriostatic for M. leprae in mice 82,s3. In 1978, Pattyn s4 showed that ethionamide or prothionamide were less effective in mice if administered less frequently than three times a week. Pattyn and van Loo s5 examined the combined chemotherapy of dapsone, ethionamide or prothionamide, thiacetazone and strep- tomycin against M. leprae in the mouse footpad. There was some synergism between dapsone and thionamide and also in combinations which included streptomycin. Ethionamide, three times weekly, was inactive. Pattyn and Saerens s6 had previously shown that streptomycin had a bactericidal activity against M. leprae and that it was less effective than dapsone and more effective than prothionamide.
Further information on the strategy of chemo- therapeutic treatment of leprosy can be found in the WHO memorandum 87 and in Pattyn 88. The existence of drug resistant organisms in patients means that the search will be worthwhile for new chemotherapeutic drugs and essential for an effective vaccine in attempts to arrest the progression of the disease.
D e v e l o p m e n t o f an ant i - M. ieprae vacc ine As early as 1939, Fernandez s9 in Argentina showed that
after inoculation with M. bovis BCG, lepromin-negative children were converted to lepromin-positivity. Sub- sequently, two major trials were undertaken in Uganda and Burma but the results were conflicting and no real conclusions evolved about the usefulness of BCG.
In Uganda, children from families with known cases of leprosy were initially tuberculin-tested by the Heaf multiple puncture procedure. Children with grade O (-ve)-ll (___ve) were placed in an unvaccinated group (8152) or BCG-vaccinated group (8149). The results showed that 174 cases of leprosy occurred among the unvaccinated children whereas only 27 cases occurred among the BCG- vaccinated group. BCG produced an 84% reduction in the
244 Vaccine, Vol. 2., December 1984
incidence of the disease; 19.3/1000 of unvaccinated and 3.0/1000 of BCG-vaccinated. Brown and his colleagues showed that BCG vaccine conferred substantial protec- tion against early forms of leprosy for at least two years 9°,91. They pointed out that 92% of patients in Uganda had tuberculoid leprosy and cautioned against the application of these results in areas of the world where the disease was predominantly of the lepromatous type.
In Burma the proportion of lepromatous disease is 40-70% and Bechelli et aL 92 reported after nine years that children under four years of age vaccinated with BCG did show a lower incidence of the disease than the control unvaccinated group. However, household contacts, or children aged 5-14 years were not protected by BCG. Nevertheless, they concluded that BCG-vaccinated children suffered from a less severe form of leprosy than the unvaccinated children.
Recently, it has been possible to separate 492 mg (dry weight) ofM. leprae from 323 g (wet weight) of armadillo infected liver and spleen with a two phase system (Dextran T500 and polyethylene glycol 6000). This procedure has enabled the bacilli to be separated from armadillo tissue components and an experimental vaccine to be prepared 93 (Shepard et al., 1980). Dr 1LJ.W. Rees (personal communication) has indicated that 125 000 vaccine doses can be prepared from one armadillo. Some 180 g of freeze-dried M. leprae can be harvested from the tissues of 150 armadillos. However, one wonders how many armadillos would be required to provide sufficient vaccine doses to support a campaign to control leprosy. The cost of separating the bacilli from the armadillo tissue on a large-scale may also be prohi- bitive in areas of the world where governments can spend as little as $1 per annum on health care per head of the population.
In addition, it is possible to prepare a lepromin
Table 2 The protective effect of M. bovis BCG and M. leprae against leprosy and tuberculosis. (Data provided by Dr R.J.W. Rees, Medical Research Council, Mill Hill, London)
Vaccine, one injection
Protection against
M. leprae M. tuberculosis
Animals Man Animals Man
Live 114. bovis BCG ++ + - - - -++ ++ ++ dead M. bovis BCG 0 ? 0 0 Live M. leprae ++ ? NT NT Dead M. leprae a ++ "-~ +++ ? NT NT
"The organisms were killed by irradiation or by autoclaving. The protective index was based on + fair to -H-+ very good protection. NT, not tested
Leprosy - in pursuit of a vaccine: D.E S. Stewart-Tull
suspension from armadillo tissue. The bacilli are killed in vivo using ~-irradiation (2.5 Mrad, the LDs0 is 10 krad). After this treatment, it has been calculated that one viable organism in 106 ~ g tissue remains. Also 1.0 pgM. leprae protein is sufficient to produce a positive skin test in tuberculoid patients; a negative response is found in lepromatous patients. Some 10-15% cross-reactivity is found in individuals vaccinated with BCG. The armadillo lepromin preparation contains < 0.03% of armadillo tissue in the bacterial preparation. Some serum proteins and liver antigens from D. novemcinctus cross-react with corresponding human proteins 94. Consequently, vaccines and lepromins prepared from armadillo-grown bacilli must be routinely checked for such cross-reacting anti- gens, see Stewart-Tull 9~. However, encouraging results were obtained in animal experiments done at the Medical Research Council laboratories at Mill Hill (Tables 2 and 3). Both living and dead M. leprae protected animals against subsequent challenge 93,96. In the group of animals injected with living M. leprae a classical Koch's pheno- menon was observed after the injection of the challenge dose of living M. leprae.
Convit et al. 97 noted that the intradermal injection of killed M. leprae plus BCG into lepromatous patients caused clearance ofM. leprae organisms by activation of macrophages. In 1975, Convit et aL 98 prepared a supernatant antigen by centrifugation of human lepromin 1.6 × l0 s ml -I acid-fast bacilli (AFB) for2 h at 192 000g. The supernate was filtered through a 0.45 pm membrane to yield the supernatant antigen (SA). Subsequently, Convit et al. 99,1°° have shown that immunization with killed armadillo-derived M. leprae (6.4 × 108 AFB m1-1) and driedM, boris BCG (1.0 mg ml -~) injected 6-8 times intra- dermally in 0.1 ml amounts produced a therapeutic effect on indeterminate, borderline and lepromatous leprosy patients. They were converted to positive lepromin skin reactivity andM. leprae organisms were cleared from their skin lesions. In addition, the in vivo 148 h and 30 day reactions to lepromin, the 48 h reaction to SA and in vitro lymphocyte transformation to human and armadillo M. leprae organisms showed positive reactions. Mehra et aZ ~ol showed that the suppressor activity and the number of Ia +, T cells returned to normal levels during a 1-2 year period in those patients who showed clinical improvement and conversion to skin positivity. They concluded from these various studies that a combined autoclaved armadilloM, leprae suspension plus BCG has potential as a therapeutic vaccine in highly susceptible individuals or those already infected.
The dose of both M. leprae and M. bovis BCG in the combined vaccine must be determined in order to obtain the maximal therapeutic response with minimal side effects 99. Since M. leprae organisms ~°2 and M. boris
Table 3 Delayed-type hypersensit ivity reactions to soluble M. leprae protein (SML) and PPD (1 TU) in healthy skin-negative individuals immunised with M. leprae and BCG, alone or combined, six weeks previously. Data provided by R.J.W. Rees
72 h skin reaction to
SML ( t .0 pg) PPD (1 tuberculin unit) Number of
individuals Proportion Mean increase Proportion Mean increase in group Immunizat ion positive (mm) ± s.e. positive (mm) ± s.e.
7 114. leprae 6 10.4 a ± 2 .14 0 0.4 ± 0 .76 8 M. boris BCG (Japanese) 2 1.6 ± 1.06 8 10.2 a ± 1.32 8 M ' b ° v i s B C G ( 1 . 5 x l O e ) + M . leprae(2 .0x lO s) 7 1 0 . 7 a ± 1 . 9 7 8 7 . 4 a ± 1 . 2 7 7 None (control) 0 0.5 ± 0 .57 0 0.2 + 0 .43
aSignfiicantly different from the control group (p < 0.001 )
Vaccine, Vol. 2., December 1984 245
Leprosy ~ in pursu i t o f a vaccine: D.ES. Stewart-Tuff
BCG whole cells ~°3 are both known immunopotentiators, the use of such a vaccine is subject to the same constraints placed on the use of mycobacterial adjuvants in vaccines. I have discussed the harmful effects and the dosage effect of mycobacterial adjuvants 95,~°4,1°5 and these are relevant to the development of a leprosy vaccine. It is also established that mycobacterial adjuvants stimulate the cell-mediated arm of the immune response. In this respect, it is interesting that healthy individuals injected with a combined vaccine showed 7/8 lepromin positives and 8/8 tuberculin positives. The development of a combined vaccine for leprosy and tuberculosis for use in areas of the world where both diseases are prevalent, is worthy of the attention of pharmaceutical companies.
However, one must consider the effect on the world's population of armadillos and a concerted effort is required to enlarge our knowledge of the biochemical activities of the organism. The recent studies of Wheeler and his colleagues ~06-108 have established a number of specific biochemical activities ofM. leprae derived from armadillo tissue and one hopes that such information will ultimately lead to the laboratory cultivation of the organism. The difficulties encountered by many workers have been discussed (Stewart-Tull, 1982); nevertheless these must be overcome in the pursuit of an economical, commercial vaccine.
The problems associated with leprosy vaccines are numerous s3 but research on vaccine development deserves high priority because the ultimate impact would be "an increase in the awareness of both health profes- sionals and the general populations in countries with endemic leprosy, that leprosy is a disease that can be prevented and cured" 53
Acknowledgements My thanks are due to colleagues who have provided me with illustrative material, to Mrs Netta Roberts for secretarial help and Mr Ian McKie for his photographic expertise. The constructive criticism of Dr R.J.W. Rees and Dr P. Draper during the preparation of the manuscript was most useful.
References 1 Baron, A.L. In: Man against germs, R. Hale, Ltd., London
1958 2 Leonard, W.E. and Lucretius Carus, T. In: Of the nature of
things, Dent, London 1916 3 Bergmann, A.V. In: 'Die Lepra' Verlag von Ferdinand, Lake,
Stuttgart 1897 4 Waddell, W.G. In: M a n e t h o - an English translation,
Heinemann, London 1940 5 Fiennes, R. In: Man, Nature and Disease, New English Library
Ltd. London 1965 6 Reader, R. New evidence for the antiquity of leprosy in early
Britain. J. ArchaeoL ScL 1974, 1 ,205 7 Hansen, G.A. Undersogelser angaende spedalskhedens
Waaler, E. Changes in the anterior nasal spine and the alveolar process of the maxillary bone. Int J. Lepr. 1952, 20, 335
10 M~ller-Christensen, V. Ten lepers from Naestved in Denmark. A study of skeletons from a medieval leper hospital. Danish Science Press Ltd., Copenhagen 1953, p. 160
11 Comrie, J.D. In: HistoryofScottish Medicine. Bailliere, Tindall and Cox, London 1932
12 Subramaniam, K. and Marks, S.C. Alveolar bone loss in leprosy; a clinical and radiological study. Lepr. Rev. 1978, 49, 287
13 World Health Organization. Leprosy surveillance. Wkly Epidem. Rec. 1979, 54, p. 161
14 Rotberg, A. 'Hanseniasis' - the new official name of leprosy in Sao Paulo, Brazil. Dermatol. Int. 1969, 8, 40
16 Rotberg, A. The serious Latin-American problems caused by the complex 'leprosy': The Word, The Disease and an appeal for world co-operation. Lepr Rev. 1972, 43, 96
17 Stringer, T.A. Leprosy and 'A Disease called Leprosy'. Lepr. Rev. 1973,44, 70
18 Shepard, C.C. and McRae, D.H. Mycobacterium leprae in mice: minimal infectious dose, relationship between staining quality and infectivity and effect of cortisone. J. Bacteriol. 1965, 89, 365
19 Dungal, X. Is leprosy transmitted by insects? Lepr. Rev. 1960, 31 ,25
20 Geater, J.G. The fly as potential vector in the transmission of leprosy. Lepr. Rev. 1975, 46, 279
21 Shepard, C.C. Acid-fast bacilli in nasal excretions in leprosy and results of inoculation of mice. Am. J. Hyg. 1960, 71, 147
22 Rees, R.J.W. and McDougall, A.C. Airborne infection with M. leprae in mice. J. Med. Microbiol. 1977, 10, 63
23 Rees, R.J.W. and Meade, T.W. Comparison of the modes of spread and the incidence of tuberculosis and leprosy. Lancet 1974, 1, 47
24 Desikan, K.V. Viability of Mycobacterium leprae outside the human body. Lepr. Rev. 1977, 48, 231
25 Pedley, J.C. The presence of M. leprae in the breast secretion of a non-lactating woman with lepromatous leprosy. Lepr. Rev. 1968, 39, 111
26 Leiker, D.L. On the mode of transmission of M. leprae. Lepr. Rev. 1977, 48, 9
27 Ridley, D.S. and Jopling, W.H. Classification of leprosy according to immunity. A five-group system. Int. J. Lepr. 1966, 34, 255
28 Godal, T., Myrvang, B., Stanford, J.L. and Samuel, D.R. Recent advances in the immunology of leprosy with special reference to new approaches in immune-prophylaxis. Bull. Inst. Pasteur, Paris 1974, 72, 273
29 Cochrane, R.G. and Davey, T.F. In: Leprosy in Theory and Practice. John Wright, Bristol, 1959
30 Ridley, D.S. and Waters, M.F.R. Significance of variations within the lepromatous group. Lepr. Rev. 1969, 40, 143
31 Browne, S.G. Leprosy. Acta clinica 1970, 11, 1 32 Ridley, D.S. Histological classification and the immunological
spectrum of leprosy. Bull. WHO 1974, 61,451 33 Bullock, W.E. and Fasal, P. Studies of immune mechanisms in
leprosy. J. Immunol. 1971, 106, 888 34 Godal, T., Myklestad, B., Samuel, D.R. and Myrvang, B.
Characterization of the cellular immune defect in lepromatous leprosy: a specific lack of circulating Mycobacterium leprae- reactive lymphocytes. Clin. Exp. Immunol. 1971,9, 821
35 Godal, T., Myrvang, B., Fr~land, S.S., Shao, J. and Melaku, G. Evidence that the mechanism of immunological tolerance (central failure) is operative in the lack of host resistance in lepromatous leprosy. Scand. J. Immunol. 1972, 1, 311
36 Waldorf, D.S., Sheagren, J.N., Trautman, J.R. and Block, J.B. Impaired delayed hypersensitivity in patients with lepro- matous leprosy. Lancet 1966, ii, 773
37 Turk, J.L. and Waters, M.F.R. Cell-mediated immunity in patients with leprosy. Lancet 1969, ii, 243
38 Meyers, W.M., Kvernes, S. and Binford, C.H. Comparison of reactions to human and armadillo lepromins in leprosy. Int. J. Lepr. 1975, 43, 218
39 Millar, J.W., Gannon, C. and Chan, C.S.P. Comparison in leprosy patients of Fernandez and Mitsuda reactions using human and armadillo antigens. A double-blind study. Int. J. Lepr. 1975, 43, 226
40 Abe, M. Identification of Mycobacterium leprae by fluore- scent antibody technics. Int. J. Lepr. 1971,39, 87
41 Abe, M. Anti-M. leprae antibodies in leprosy patients as demonstrated by indirect immunofluorescence. Int. J. Lepr. 1973, 41 ,549
42 Myrvang, B., Feek, C.M. and Godal, T. Antimycobacterial antibodies in sera from patients throughout the clinico- pathological spectrum of leprosy. Acta. Pathol. microbiol. Scand. 1974, 82, 701
43 Harboe, M., Closs, O., Bjune, G., Kronvatl, G. and Axelsen, N.H. Mycobacterium leprae specific antibodies detected by radioimmunoassay. Scand. J. Immunol. 1978, 7, 111
2 4 6 Vaccine, Vol. 2., December 1 9 8 4
44 Newell, K.W. An epidemiologist's view of leprosy. Bull. WHO 1966, 34, 827
45 Turk, J.L. Cell-mediated immunological processes in leprosy. Bull, WHO 1969, 4 1 , 7 7 9
46 Godal, T. Immunological Aspects of leprosy- present status. Prog. Allergy 1978, 25, 211
47 Mehra, V., Mason, L.H., Fields, J.P. and Bloom, B.R. Lepromin-induced suppressor cells in patients with leprosy. J. Immunol. 1979, 123, 1813
48 Mehra, V., Mason, L.H., Rothman, W., Reinherz, E., Schlossman, S.F. and Bloom, B.R. Delineation of a human T cell subset responsible for lepromin-induced suppression in leprosy patients. J. Irnrnunol. 1980, 125, 1183
49 Turk, J.L. and Bryceson, A.D.M. Immunological phenomena in leprosy and related diseases. Adv. Irnrnunol. 1971, 13, 209
50 World Health Organization. Immunological problems in leprosy research 1. Bull WHO 1973, 48, 345
51 World Health Organization. Immunological problems in leprosy research 2. Bull, WHO 1973, 48, 483
53 Bloom, B.R. and Godal, T. Selective primary health care: strategies for control of disease in the developing world V leprosy. Rev. Infect. Dis. 1983, 5, 765
54 Tada, T., Taniguchi, M. and Takemori, T. Properties of primed suppressor T cells and their products. Transplant. Rev. 1975, 26, 106
55 Asherson, G.L. and Zembala, M. Suppressor T cells in cell mediated immunity. Br. Med. Bull, 1976, 32, 158
56 Benacerraf, B. Suppressor T cells and Suppressor Factor (Eds. Dixon, F.J. and Fisher, D.W.). In: The Biology of Immunologic Disease. Sinauer Associates Inc., Massachusetts 1983, p. 49
57 Shepard, C.C., McRae, D.H. and Habas, J.A. Sensitivity of Myc. leprae to low levels of 4,4'-diaminodiphenylsulfone. Proc, Soc. Exp. Biol. Med, 1966, 12.2, 893 Rees, R.J.W. Leprosy. A preliminary review of the experi- mental evaluation of drugs fo r the treatment of leprosy. Trans. Roy. Soc. Trop. Med. Hyg. 1967, 61, 581 Shepard, C.C. Activity of repository sulfones against Mycobacteriurn leprae in mice. Proc. Soc. Exp. Biol. Me(/. 1967, 124, 430 Shepard, C.C., Levy, L. and Fasal, P. The sensitivity to Dapsone (DDS) of Mycobacteriurn leprae from patients with and without previous treatment. Am. J. Trop. Med. Hyg. 1969, 18, 258 Waters, M.F.R., Rees, R.J.W. and Ellard, G.A. Experimental and clinical studies on the minimum inhibitory concentra- tions (MIC) of dapsone (DDS) in leprosy. Int. J. Lepr. 1968, 3 6 , 651 Shepard, C.C., Tolentino, J.G. and McRae, D.H. The thera- peutic effect of 4,4'-diacetyl-diaminodiphenyl sulfone (DADDS) in leprosy. Am. J. Trop. Med. Hyg. 1968, 17, 192 Russell, D.A., Shepard, C.C., McRae, D.H., Scott, G.C. and Vincin, D.R. Treatment with 4,4'-diacetyldiaminodiphenyl sulphone (DADDS) of leprosy patients in the Karimui, New Guinea Am. J. Trop. Med. Hyg. 1971,20, 495 Pettit, J.H.S. and Rees, R.J.W. Sulphone resistance in leprosy. An experimental and clinical study. Lancet 1964, ii, 673 Pettit, J.H.S., Rees, R.J.W. and Ridley, D.S. Studies on sulphone resistance in leprosy 1. Detection of cases. Int. J. Lepr. 1966, 34, 375 Pearson, J.M.H., Cap, J.A., Halle, G.S. and Rees, R.J.W. Dapsone-resistant leprosy and its implications for leprosy control programmes. Lepr. Rev. 1977, 48, 83 Waters, M.F.R., Laing, A.B.G. and Rees, R.J.W. Proven primary dapsone resistance in leprosy- a case report. Lepr. Rev. 197849, 127 Baquillon, G., Ferracci, C., Saint-Andre, P. and Pattyn, S.R. Dapsone-resistant leprosy in a population of Bamako (Mall) Lepr. Rev, 1980, 51, 315 Pattyn, S.R., Baquillon, G., Ferracci, C. and Saint-Andre, P. Premier cas de lepre a resistance secondaire a la dapsone en Afrique occidentale. Med. Afr. Noire 1979, 26, 8 Pattyn, S.R., Dockx, P., Rollier, M.T., Rollier, R. and Saerens, E.J. Mycobacteriurn leprae persisters after treat- ment with dapsone and rifampicin. Int. J. Lepr, 1976, 44, 154
58
59
60
61
62
63
64
65
66
67
68
69
70
L e p r o s y - in pursui t o f a vaccine: D.ES. Stewart-Tuff
71 Pattyn, S.R., van Loo, G. and Sansarricq, H. Quatre cas de lepre dapsone resistants en Haute-Volta. MedicineAfr. Noire 1981,28, 147
72 Opromolla, D.V.A., de Souza Lima, L. and Caprara, G. Rifamycin SV in the treatment of lepromatous leprosy. Lepr. Rev. 1965 36, 123
73 Shepard, C.C. The first decade in experimental leprosy. Bull, WHO 1971,44, 821
74 Rees, R.J.W., Pearson, J.M.H. and Waters, M.F.R. Experi- mental and clinical studies on rifampicin in treatment of leprosy. Br. Med. J. 1970, 1, 89
75 Shepard, C.C., Levy, L. and Fasal, P. Rapid bactericidal effect of rifampin on Mycobacterium leprae. Am. J. Trop. Med. Hyg. 1972, 21 ,446
76 Pattyn, S.R. and Saerens, E.J. Activity of three new rifamycin derivatives on the experimental infection by Mycobacteriurn leprae. Ann. Soc. Beige Med. Trop. 1977, 57, 169
77 Waters, M.F.R., Rees, R.J.W., Pearson, J.M.H., Laing, A.B.G., Helmy, H.S. and Gelber, R.H. Rifampicin for lepromatous leprosy: nine years experience. Br. Med. J. 1978, 1, 133
79 Barry, V.C. and Conalty, M.L. The antimycobacterial activity of B663. Lepr, Rev. 1965, 36, 3
80 Browne, S.G. B663 (Geigy) - further observations on its suspected anti-inflammatory action. Lepr. Rev. 1966, 37, 141
81 Shepard, C.C. Minimal effective dosages in mice of clofa- zimine (B663) and of ethionamide against Mycobacteriurn leprae. Proc. Soc. Exp. Biol. NY 1969, 132, 120
82 Colston, M.J., Ellard, G.A. and Gammon, P.T. Drugs for combined therapy: experimental studies on the anti-leprosy activity of ethionamide and prothionamide- a general review. Lepr. Rev. 1978, 49, 115
83 Colston, M.J., Hilson, G.R.F., Ellard, G.A. and Gammon, P.T. The activity of thiacetazone, thiambutosine, thiocarlide and sulphamethoxypyridazine against M. leprae in mice. Lepr. Rev. 1978, 49, 101
84 Pattyn, S.R. Further data on the effect of ethionamide and prothionamide in experimental leprosy. Lepr. Rev. 1978, 49, 199
85 Pattyn, S.R. and van Loo, G. Combined chemotherapy against Mycobacterium leprae in the mouse. Ann. Soc. Beige Med. Trop. 1980, 60, 291
86 Pattyn, S.R. and Saerens, E. Evaluation of the activity of streptomycin on Mycobacterium leprae in mice. Lepr. Rev. 1978, 49, 275
87 World Health Organization. Experimental chemotherapy in leprosy. Bull. WHO 1976, 53, 425
88 Pattyn, S.R. The strategy of leprosy treatment: a personal view. Ann. Soc. Beige Med. Trop. 1980, 60, 253
89 Fernandez, J.M.M. Estudio comparativo de la reacion de Mitsuda con las reacciones tuberculinicas. Rev. Argent. Derrnatosifilol. 1939, 23, 425
90 Brown, Kinnear J.A. and Stone, M.M. BCG vaccination of children against leprosy: first results of a trial in Uganda. Br. Med. J. 1966, 7
91 Brown, Kinnear J.A., Stone, M.M. and Sutherland, I. Trial of BCG vaccination agaisnt leprosy in Uganda. Lepr. Rev. 1969 40, 3
92 Bechelli, M.L., et al. BCG vaccination o f children against leprosy: nine year findings of the controlled WHO trial in Burma, Bull. WHO 1974, 51, 93
93 Shepard, C.C., Draper, P., Rees, R.J.W. and Lowe, C. Effect of purification steps on the immunogenicity of Mycobacteriurn leprae. Br. J. Exp. PathoL 1980, 61 ,376
94 Negassi, K., Closs, O. and Harboe, M. Cross-reaction between serum proteins and water-soluble liver tissue antigens of the nine-banded armadillo and man. C/in. Exp. Immunol. 1979, 3 8 , 135
95 Stewart-Tull, D.E.S. and Davies, M. In: The Immunology of the bacterial cell envelope. John Wiley, Chichester, UK 1985
96 Smelt, A.H.M., Rees, R.J.W. and Liew, F.Y. Induction of delayed-type hypersensitivity to M. leprae in healthy indi- viduals. C/in. Exp. ImrnunoL 1981 44, 501
97 Convit, J., Pinardi, M.E., Rodriguez Ochoa, G., Ulrich, M., Avila, J.L. and Goihman-¥ahr, M. Elimination of Myco- bacterium leprae subsequent to local in vivo activation of macrophages in lepromatous leprosy by other mycobacteria. C/in. Exp. Irnnrnunol. 1974, 17,261
Vaccine, Vol. 2., December 1 9 8 4 2 4 7
Leprosy - - in pursui t o f a vaccine: D.ES. Stewart-Tul l
98 Convit, J., Pinardi, M.E., Avila, J.L. and Aranzazu, N. Specificity of the 48-hour reaction to Mitsuda antigen. Bull. WHO 1975, 52, 187
99 Convit, J., Aranzazu, N., Pinardi, M. and Ulrich, M. Immuno- logical changes observed in indeterminate and lepromatous leprosy patients and Mitsuda -ve contacts after the inocu- lation of a mixture of M. leprae and BCG. C/in. Exp. Immunol. 1979, 36, 214
100 Convit~ J., Aranzazu, M., Ulrich, M., Pinardi, M.E., Reyes, O. and Alvarado, J. Immunotherapy with a mixture of Myco- bacterium leprae and BCG in different forms of leprosy and in Mitsuda-negative contacts. Int, J. Lepr. 1982, 50, 415
101 Mehra, V., Convit, J., Rubinstein, A. and Bloom, B.R. Activated suppressor T cells in leprosy. J. Immunol. 1982, 129, 1946
102 Stewart-Tull, D.E.S. and Davies, M. Adjuvant activity of Mycobacterium leprae. Infect. Immun. 1972, 6, 909
103 Stewart-Tull, D.E.S., Shimono, T., Kotani, S., Kato, M., Ogawa, Y., Yamamura, Y., Koga, T. and Pearson, C.M. The adjuvant activity of a non-toxic water-soluble glycopeptide present in large quantities in the culture filtrate of M. tuberculosis strain DT. Immunology 1975, 29, 1
104 Stewart-Tull, D.E.S. The immunological activities of bacterial peptidoglycans. Ann. Rev. Microbiol. 1980, 34, 311
105 Stewart-Tull, D.E.S. Immunologically important components of mycobacteria. In: The Biology of Mycobacteria (Eds. Ratledge, C. and Stanford, J.L.) Academic Press, London, 1983 p. 3
106 Wheeler, P.R. and Gregory, D. Superoxide dismutase, peri- oxidatic activity and catalase in Mycobacterium leprae purified from armadillo liver. J. Gen. Microbiol. 1980, 121, 457
107 Wheeler, P.R. Metabolism of carbon sources by Myco- bacterium leprae: a preliminary report. Ann. Microbiol. Inst. Pasteur 1982, 133B, 141
108 Wheeler, P.R., Bharaway, V.P. and Gregory, D. N-acetyl-l~- glucosaminidase, 8-glucuronidase and acid phosphatase in Mycobacterium leprae. J. Gen. Microbiol. 1982, 128, 1063
109 Wheeler, P.R. Catabolic pathways for glucose, glycerol and 6-phosphogluconate in Mycobacterium leprae grown in armadillo tissues. J. Gen. Microbiol. 1983, 129, 1481
110 Wheeler, P.R. Oxidation of carbon sources through the tricarboxylic acid cycle in Mycobacterium leprae grown in armadillo liver. J. Gen. MicrobioL 1984, 130, 381
111 Stewart-Tull, D.E.S. Mycobacterium leprae - the bacterio- logist's enigma. In: The Biology of the Mycobacteria (Ed. Ratledge, C. and Stanford, J.) Academic Press, London, 1982, Vol 1 p. 273