27
Leveraging Data Sharing Klaus Romero MD MS FCP Director of Clinical Pharmacology Critical Path Institute
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | milton-cameron |
| View: | 215 times |
| Download: | 1 times |
Leveraging Data Sharing
Klaus Romero MD MS FCPDirector of Clinical Pharmacology
Critical Path Institute

2
C-Path & FDA MOUOctober 14, 2005
“purpose… to establish an overarching framework for collaboration… to foster development of new evaluation tools to inform medical product development”

C-Path Consortium Model
3
FDAEMA
Patients
NIH
Academia
AA
BC
D
E
Precompetitive Neutral ground
Multiple Companies
Formal Legal
Agreement
Critical Path Institute (C-Path) has developed a consortium structure that provides a unique neutral, precompetitive environment to increase collaborative efforts for drug development

C-Path Collaborators

Creating Consensus
Six global consortia collaborating with 1,000+ scientists and 41 companies

Informal discussion with FDA/EMA.
Sponsor submits a letter of intent requesting formal qualification. FDA/EMA Review Team formed.
Sponsor submits briefing document.
F2F meeting between sponsor and FDA/EMA Review Team. Review Team may request additional information.
Sponsor submits full data package. Review process within FDA/EMA begins.
Consultation and
Advise Process
6
Regulatory decision qualifying or endorsing the submitted tools
Success!!!
Regulatory Review Process: What’s success?

What Was Learned?ADAS-Cog Variability
Sponsor 1 Sponsor 2 Sponsor 3 Sponsor 4 Sponsor 5 Sponsor 6 Sponsor 7
Item 1 Word Recall Word Recall Word Recall Word Recall Word Recall Word Recall Word Recall
Item 2 Commands Name Obj/fing. Name Obj/fing. Commands Name Obj/fing. Name Obj/fing. Name Obj/fing.
Item 3 Constr. Praxis Delayed recall Commands Constr. Praxis Commands Commands Commands
Item 4 Delayed recall Commands Constr. Praxis Delayed recall Delayed recall Constr. Praxis Constr. Praxis
Item 5Naming Obj/fing. Constr. Praxis Idea Praxis Name Obj/fing. Constr. Praxis Idea. Praxis Idea. Praxis
Item 6 Idea. Praxis Idea Praxis Orientation Idea. Praxis Idea. Praxis Orientation Orientation
Item 7 Orientation Orientation Word Recog Orientation Orientation Word Recog Word Recog
Item 8 Word Recog. Word Recog. Remem. Instr. Word Recog Word Recog Remem. Instr.Spoken Lang Abil.
Item 9 Remem Instr. Remem Instr.Spoken Lang. Abil. Remem. Instr. Remem. Instr.
Spoken Lang. Abil. Comprehension
Item 10 ComprehensionSpoken Lang. Abil.
Word Finding Dif.
Spoken Lang Abil.
Spoken Lang Abil. Word Finding Dif. Word Finding Dif.
Item 11Word Finding Dif.
Word Finding Dif. Comprehension
Diff. Spont. Speech
Word Finding Dif. Comprehension Remem. Instr.
Item 12Spoken Lang. Abil. Comprehension Concentration Comprehension Comprehension Concentration
Item 13 Number cancel. Concentration Concentration Concentration

Benefits of Data Standards
• SDTM clinical data standard used / preferredwithin FDA – standards required in PDUFA V
• Enable data sharing between organizations
• Enable aggregation and querying of data
• When implemented from the start, can lower costs of acquiring and analyzing data
CDISC Standards
8

CDISC and C-Path
C-Path Mission:
To improve human health and well-being by developing new technologies and methods to accelerate the development and review of medical products
CDISC Mission:
To develop and support global, platform independent ‐data standards that enable information system interoperability to improve medical research and related areas of healthcare
9

C-Path and CDISC Collaborations
C-Path – FDA Qualification
Collaborations
CAMD – Alzheimer’sCAMD – Parkinson’sPKD – Polycystic Kidney DiseasePSTC – Safety TestingCPTR – Tuberculosis
CDISC – Data Standards

C-Path Data Repository

C-Path and CDISC announce formal release of data standard for Alzheimer’s Disease

~6000 Patients
• Seven companies remapped and pooled data from 21 trials for ~6000 patients: value = $400 Million
• Database open to >200 qualified research teams in 35 countries
C-Path’s Data Repository for Alzheimer’s Disease

CODR – integrated CDISC data model
C-Path Online Data Repository (CODR)
CODR is a relational database with a data model designed around the CDISC SDTM clinical data standard
CDISC domains and variables are integrated into the database architecture
Common framework for easy generation of new data repositories based on applicable CDISC domains
14

CAMD Process Overview
WG1Data
WG 2Modeling
and Simulation
WG 3Biomarkers &
Imaging
Models Biomarkers
Regulatory Review,Qualification, Acceptance
WG 4Health Authorities
Submission
Consensus
15

16
Quantitative Disease-Drug-Trial Models
DiseaseModel
Drug Model
TrialModel
Biology Natural Progression Placebo Biomarker-Outcome
Pharmacology Effectiveness Safety
Early-Late Preclinical-Healthy-Patient
Patient Population Drop-out Compliance
FDA Data
DiverseExpertise
Physiology
Disease-drug-trial models are mathematical representations of the time course of biomarker-clinical outcomes, placebo effects, drug’s pharmacologic effects and trial execution characteristics for both the desired and undesired responses, and across experiments.
Janet Woodcock
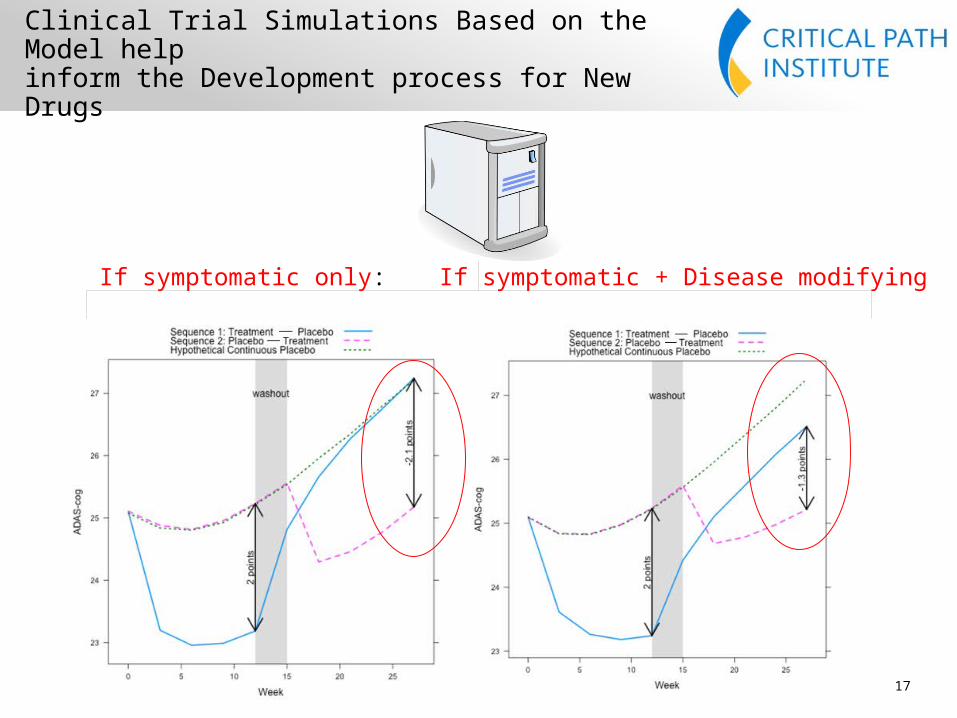
Clinical Trial Simulations Based on the Model helpinform the Development process for New Drugs
17
If symptomatic only: If symptomatic + Disease modifying

78-week Parallel Study Design versus 91 Week Delayed Start Design by Varying Disease Modifying Effects
18

When Given a Regulatory Decision, Sponsors will be able to more Confidently use the Tool and the Review Process for New Drugs will be Streamlined
19
CAMD Regulatory Path for AD Disease-Drug-Trial Model
MAY 2012
Team responding to Agency questions

C-Path Project Pipeline
FDA EMA
PMDACAMDDisease or Target Drug Development Tool
Feasibility1 Scoping2 Research3 Submitted4 Qualified5
Alzheimer's disease (AD)
Imaging Biomarkers
CSF Biomarkers
Disease model of mild and moderate AD
Disease model of Mild Cognitive Impairment
Parkinson's disease (PD)
PD imaging biomarkers
C-Path and CDISC announce formal release of data standard for Alzheimer’s Disease
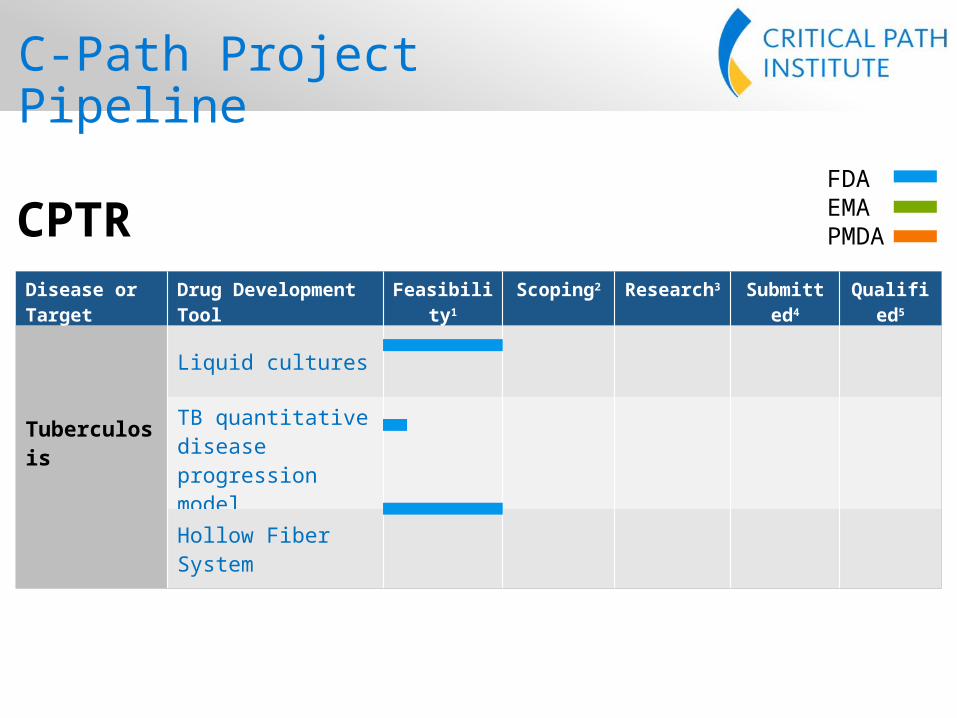
C-Path Project Pipeline
FDA EMA
PMDACPTRDisease or Target Drug Development Tool
Feasibility1 Scoping2 Research3 Submitted4 Qualified5
Tuberculosis
Liquid cultures
TB quantitative disease progression model
Hollow Fiber System

Clinical Trial Inventory
23
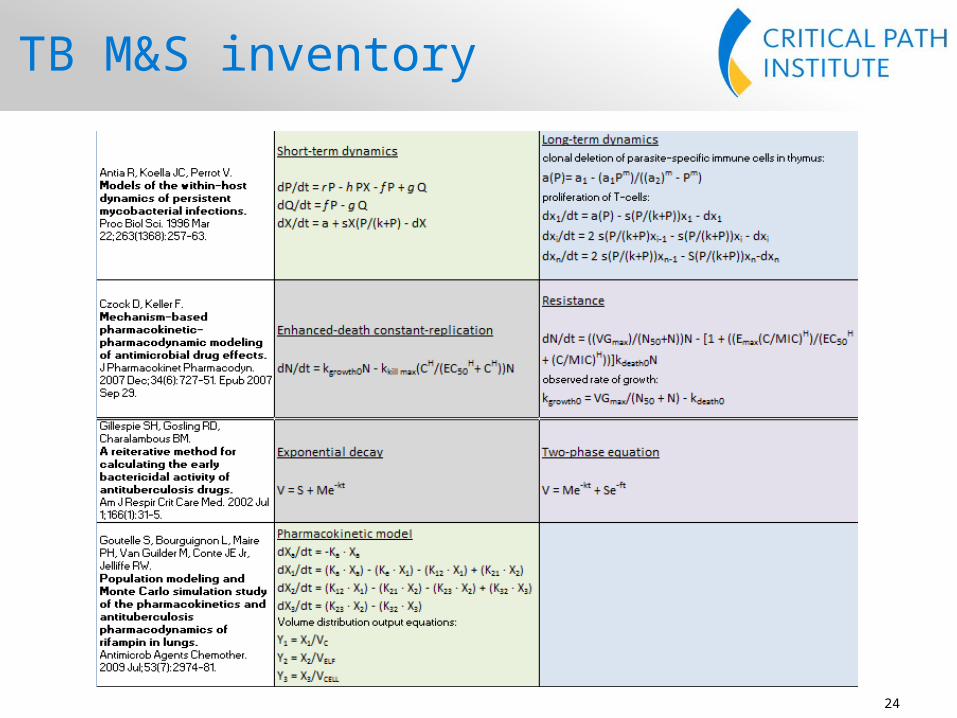
TB M&S inventory
24

Approaches from other areas
Predator-Prey models in HCV may provide useful insights for TB modeling and simulation.
Guedj J. et al. Understanding HCV dynamics with direct-acting antiviral agents due to interplay between intracellular replication and cellular infection dynamics. J Theor Bio 2010;267:330-40

What about HCV?
C-Path firsts
Are industry and regulators interested?
Which DDTs are a priority?
What is the current status of data standardization?
Which are the relevant potential data sources?
How can we collaborate?


















