20
Library Design for Leadlike Compounds: A Historical Perspective Tudor I. Oprea EST Lead Informatics
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | rosemary-anderson |
| View: | 220 times |
| Download: | 1 times |

Library Design for Leadlike Compounds:
A Historical Perspective
Tudor I. Oprea
EST Lead Informatics

Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
What Is A Lead?
• Many compounds are active, but not all actives are leads
• Leads have to meet project dependent criteria:
biological activity validated, both in primary and secondary screens, against known targets, for a series of compounds (when available)
• must be patentable, and display good initial DMPK profile
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
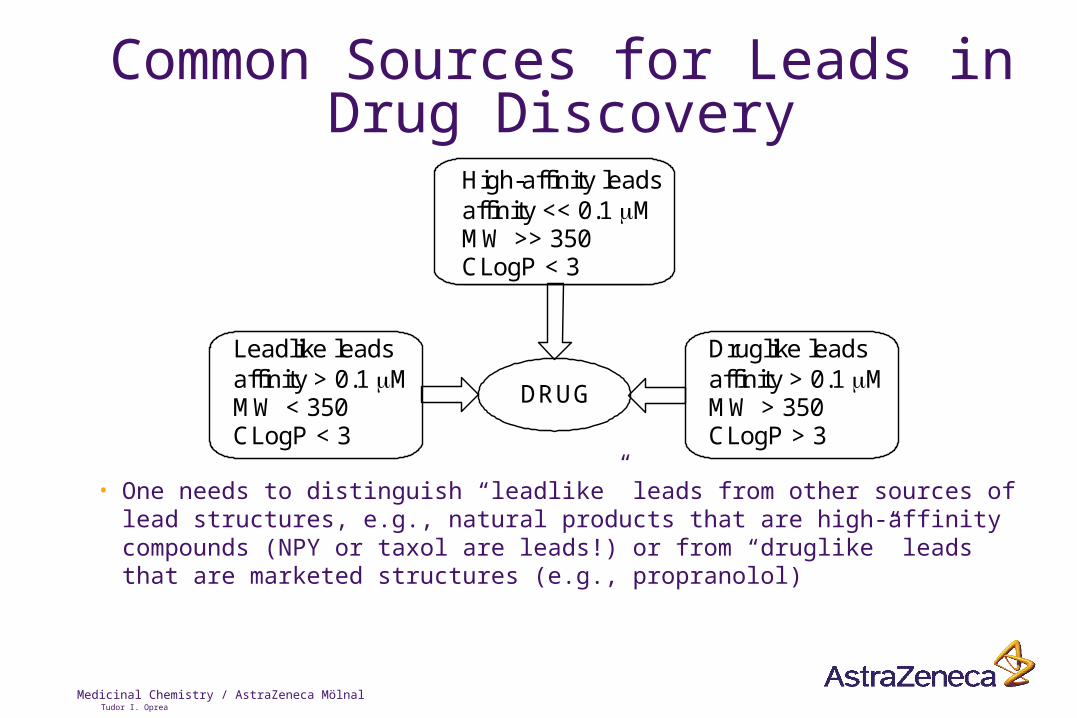
Common Sources for Leads in Drug Discovery
Druglike leadsaffinity > 0.1 MMW > 350CLogP > 3
Leadlike leadsaffinity > 0.1 MMW < 350CLogP < 3
DRUG
High-affinity leadsaffinity << 0.1 MMW >> 350CLogP < 3
• One needs to distinguish “leadlike” leads from other sources of lead structures, e.g., natural products that are high-affinity compounds (NPY or taxol are leads!) or from “druglike” leads that are marketed structures (e.g., propranolol)
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
Is There A Leadlike Space?
• There is a general consensus that lead discovery is an essential goal that precludes drug discovery
• For the time being, the only way to analyse the nature of the “leadlike” space is to examine the structures that, historically, were leads.
• The problem is: can these structures provide an objective link between lead-space and drug-space?
• Can we define how these two spaces overlap?

Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
Is There A Leadlike Space? (2)• Initial goal of the retrospective leadlike analysis: gather as
much information as possible about leads, i.e., which drug has been developed from which lead
• Only a few authors describe the chemical structure of the lead compound that was used to derive a given drug.
• Lead structures are often disclosed in a series (SAR), making it difficult to pinpoint at a given compound.
• Furthermore, a drug can have 1 or more leads
• a lead can be a drug
• a lead can lead to several drugs.
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
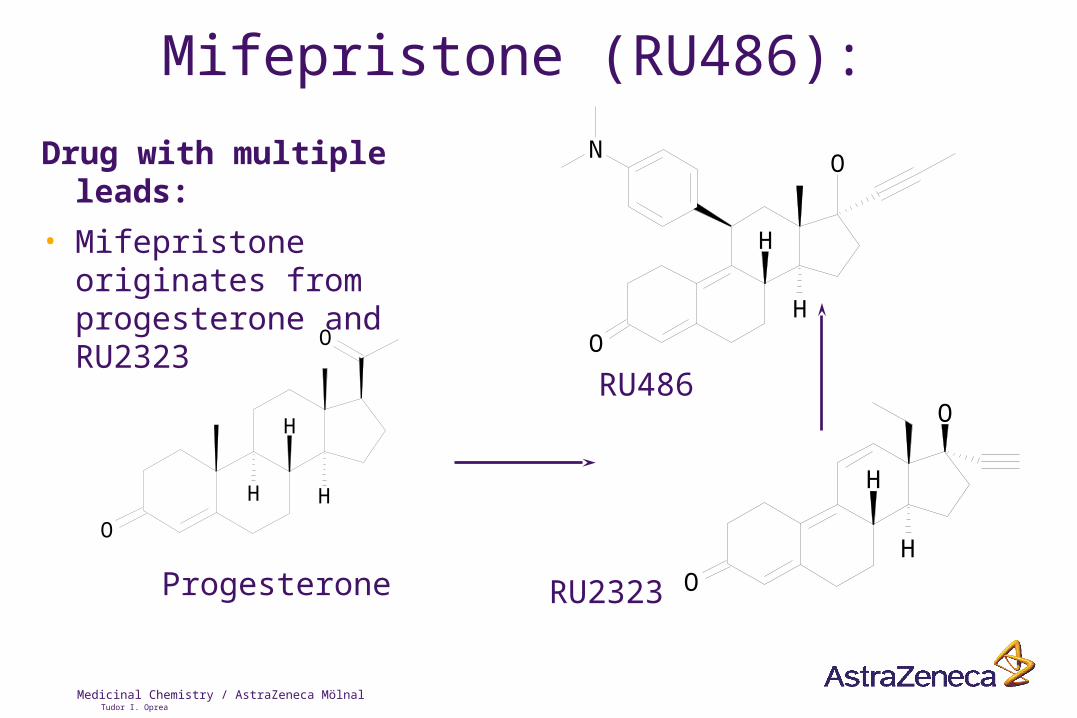
Mifepristone (RU486):
Drug with multiple leads:
• Mifepristone originates from progesterone and RU2323
O
O
H
H
H
O
OH
H
O
O
N
H
H
Progesterone RU2323
RU486
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
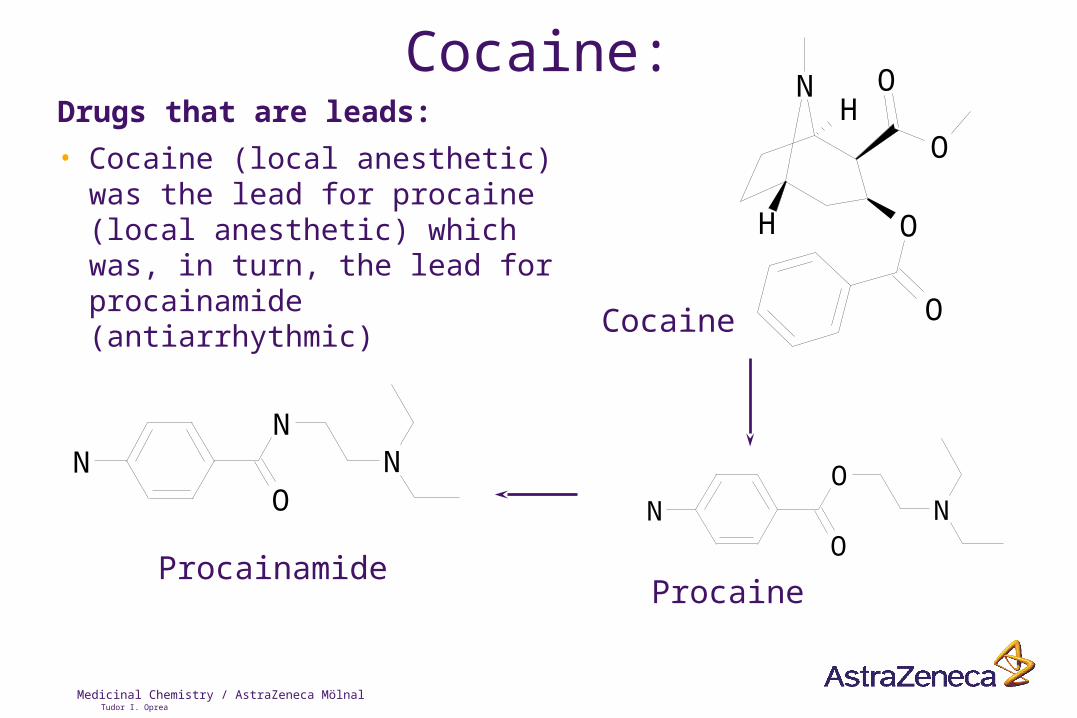
Cocaine:Drugs that are leads:
• Cocaine (local anesthetic) was the lead for procaine (local anesthetic) which was, in turn, the lead for procainamide (antiarrhythmic)
N
O
O
O
O
H
H
O
ON N
N
ON N
Cocaine
ProcaineProcainamide
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
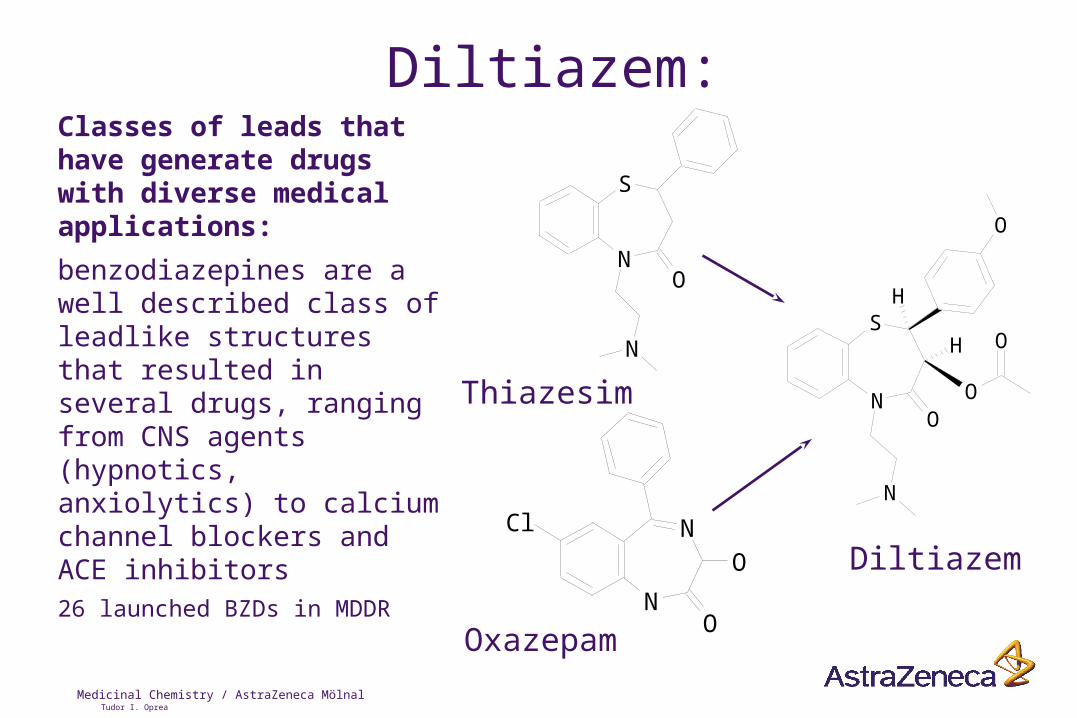
Diltiazem:Classes of leads that have generate drugs with diverse medical applications:
benzodiazepines are a well described class of leadlike structures that resulted in several drugs, ranging from CNS agents (hypnotics, anxiolytics) to calcium channel blockers and ACE inhibitors26 launched BZDs in MDDR
N
S
O
N
N
N
O
O
Cl
S
ONO
O
O
N
H
H
Thiazesim
Oxazepam
Diltiazem
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
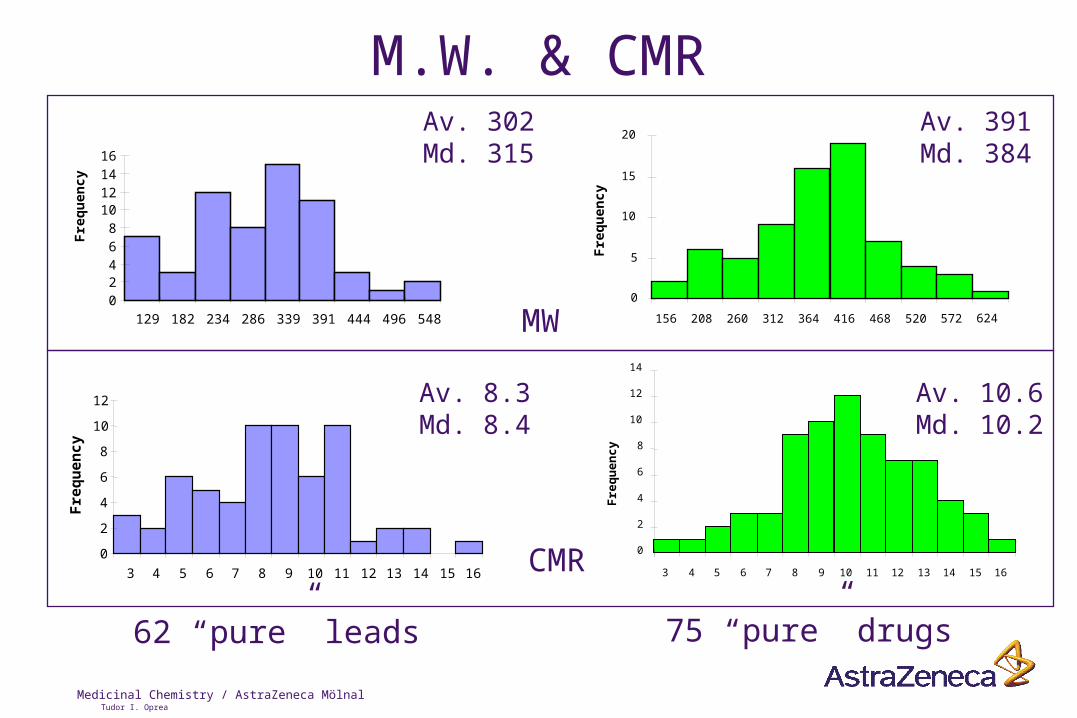
M.W. & CMRAv. 302Md. 315
Av. 391Md. 384
Av. 8.3Md. 8.4
Av. 10.6Md. 10.2
62 “pure” leads 75 “pure” drugs
CMR
MW0
5
10
15
20
156 208 260 312 364 416 468 520 572 624
Fre
qu
ency
02468
10121416
129 182 234 286 339 391 444 496 548
Fre
qu
ency
0
2
4
6
8
10
12
3 4 5 6 7 8 9 10 11 12 13 14 15 16
Fre
qu
ency
0
2
4
6
8
10
12
14
3 4 5 6 7 8 9 10 11 12 13 14 15 16
Fre
qu
en
cy
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
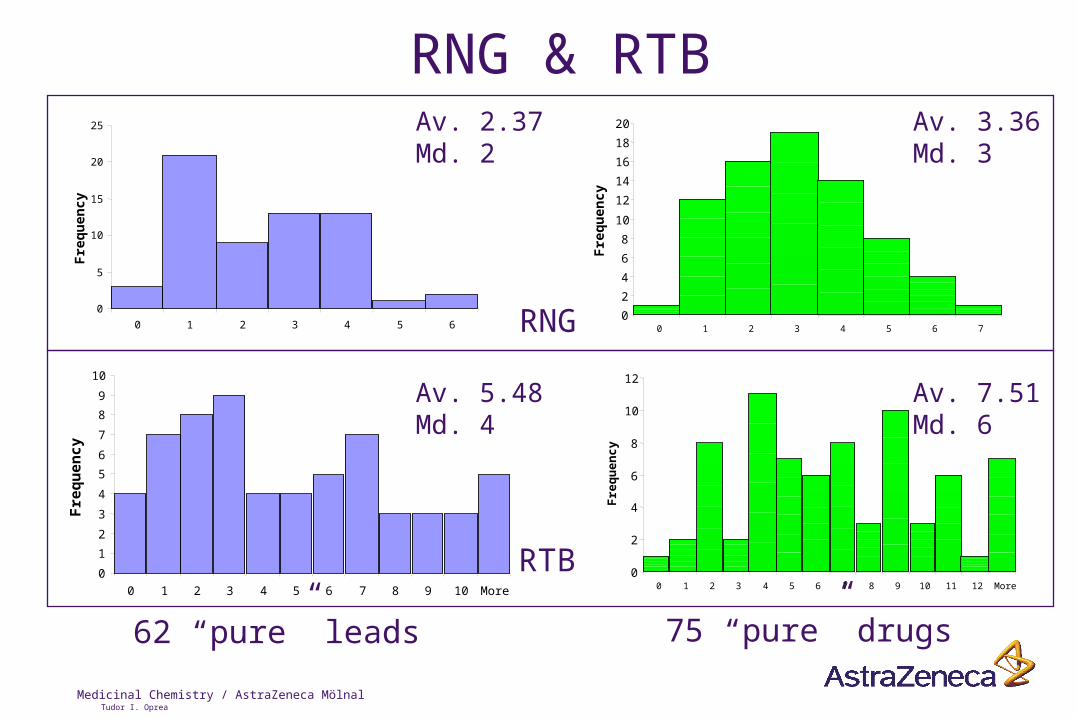
RNG & RTBAv. 2.37Md. 2
Av. 3.36Md. 3
Av. 5.48Md. 4
Av. 7.51Md. 6
62 “pure” leads 75 “pure” drugs
RTB
RNG
Fre
qu
ency
Fre
qu
ency
Fre
qu
ency
Fre
qu
en
cy
0
5
10
15
20
25
0 1 2 3 4 5 6
0
1
2
3
4
5
6
7
8
9
10
0 1 2 3 4 5 6 7 8 9 10 More
0
2
4
6
8
10
12
0 1 2 3 4 5 6 7 8 9 10 11 12 More
0
2
4
6
8
10
12
14
16
18
20
0 1 2 3 4 5 6 7

Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
CLogP & LogD7.4
Av. 0.72Md. 0.72n=57
Av. 1.69Md. 1.69n=71
62 “pure” leads 75 “pure” drugs
LogD7.4
Av. 1.57Md. 2.11n=58
Av. 2.73Md. 2.54 n=70
CLogP
0
2
4
6
8
10
12
- 7.5 - 6.5 - 5.5 - 4.5 - 3.5 - 2.5 - 1.5 - 0.5 0.5 1.5 2.5 3.5 4.5 5.5
Fre
qu
en
cy
0
2
4
6
8
10
12
14
- 7.5 - 6.5 - 5.5 - 4.5 - 3.5 - 2.5 - 1.5 - 0.5 0.5 1.5 2.5 3.5 4.5 5.5F
req
uen
cy
0
2
4
6
8
10
12
-2.3 -1.8 -1.3 -0.8 -0.3 0.3 0.8 1.3 1.8 2.3 2.8 3.3 3.8 4.3 4.8 5.3 5.8
Fre
qu
en
cy
0
1
2
3
4
5
6
7
-3.8 -2.8 -1.8 -0.8 0.3 1.3 2.3 3.3 4.3 5.3
Fre
qu
ency

Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
Donors & Acceptors
Av. 4.8Md. 4
Av. 5.8Md. 5
62 “pure” leads 75 “pure” drugs
HAC
Av. 2.3Md. 2
Av. 2.1Md. 2
HDO
0
24
6
8
1012
14
16
0 1 2 3 4 5 6 7 8 9 10 11
Fre
qu
ency
0
2
4
6
8
10
12
14
0 1 2 3 4 5 6 7 8 9 10 11 12 More
Fre
qu
en
cy
0
5
10
15
20
25
0 1 2 3 4 5 6 7 8 9
Fre
qu
ency
0
2
4
6
8
10
12
14
0 1 2 3 4 5 6 7 8 9 10 11 12 MoreF
req
ue
nc
y
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
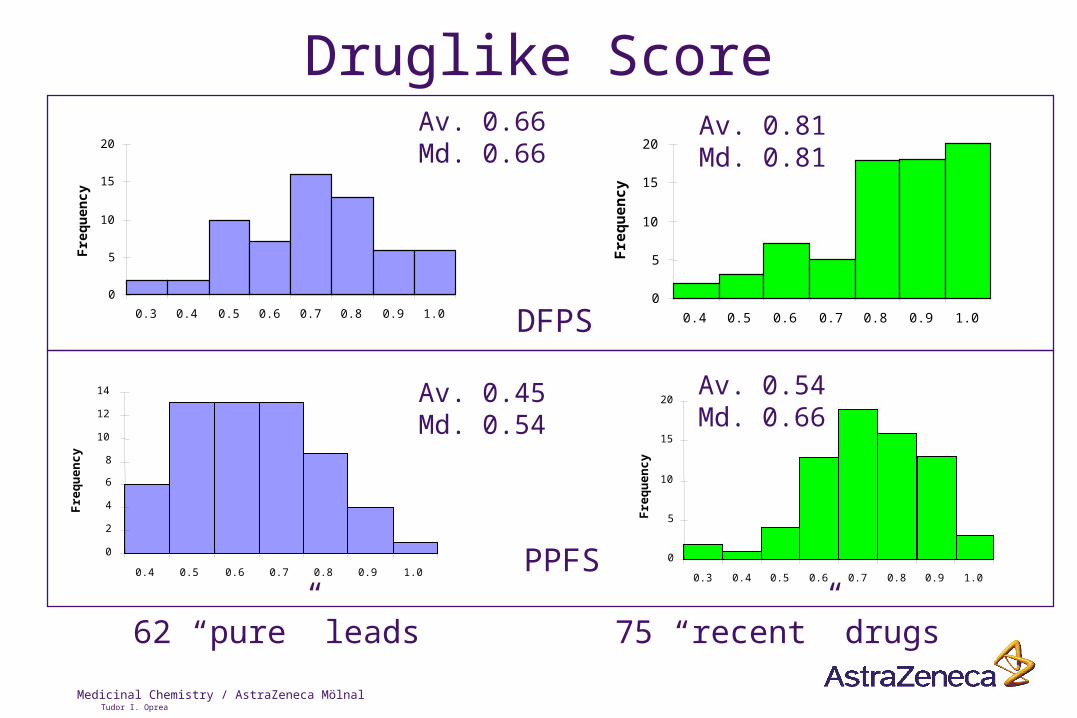
Druglike ScoreAv. 0.66Md. 0.66
Av. 0.81Md. 0.81
Av. 0.45Md. 0.54
Av. 0.54Md. 0.66
62 “pure” leads 75 “recent” drugs
PPFS
DFPS0
5
10
15
20
0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
Fre
qu
ency
0
2
4
6
8
10
12
14
0.4 0.5 0.6 0.7 0.8 0.9 1.0
Fre
qu
en
cy
0
5
10
15
20
0.4 0.5 0.6 0.7 0.8 0.9 1.0
Fre
qu
ency
0
5
10
15
20
0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
Fre
qu
en
cy
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
Is There A Difference?
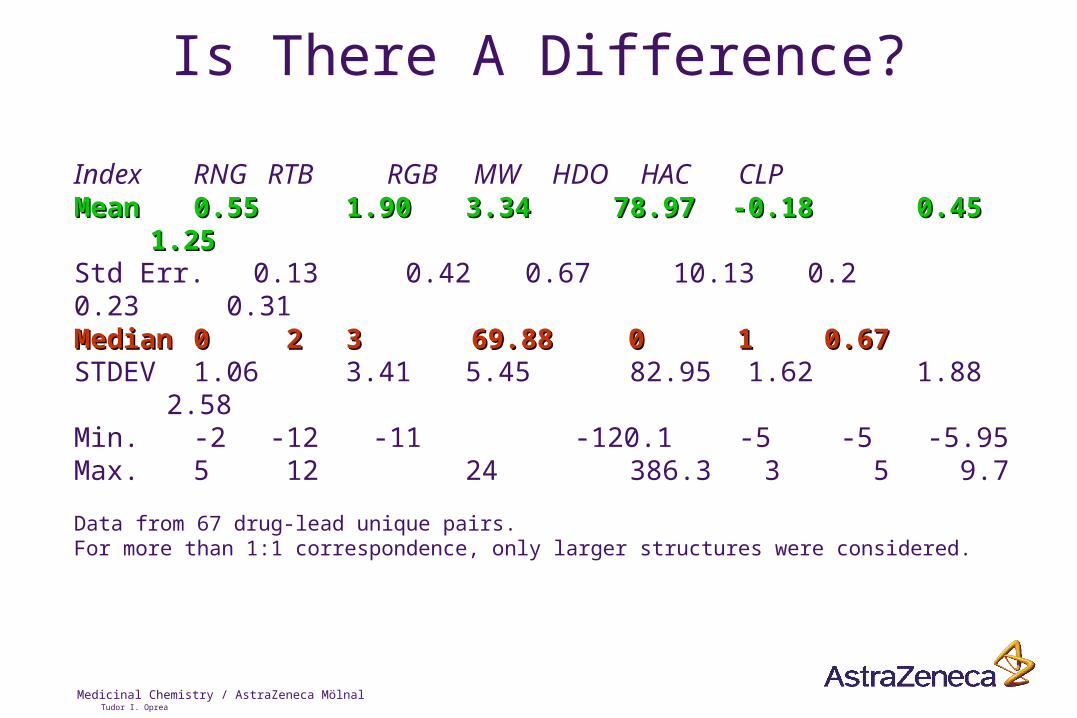
Index RNG RTB RGB MW HDO HAC CLPMeanMean 0.550.55 1.90 1.90 3.34 78.97 3.34 78.97 -0.18-0.18 0.45 0.45 1.25 1.25Std Err. 0.13 0.42 0.67 10.13 0.2 0.23 0.31MedianMedian 00 2 2 3 3 69.88 69.88 0 0 1 1 0.67 0.67STDEV 1.06 3.41 5.45 82.95 1.62 1.88 2.58Min. -2 -12 -11 -120.1 -5 -5 -5.95Max. 5 12 24 386.3 3 5 9.7
Data from 67 drug-lead unique pairs. For more than 1:1 correspondence, only larger structures were considered.
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
Is There A Real Difference?!
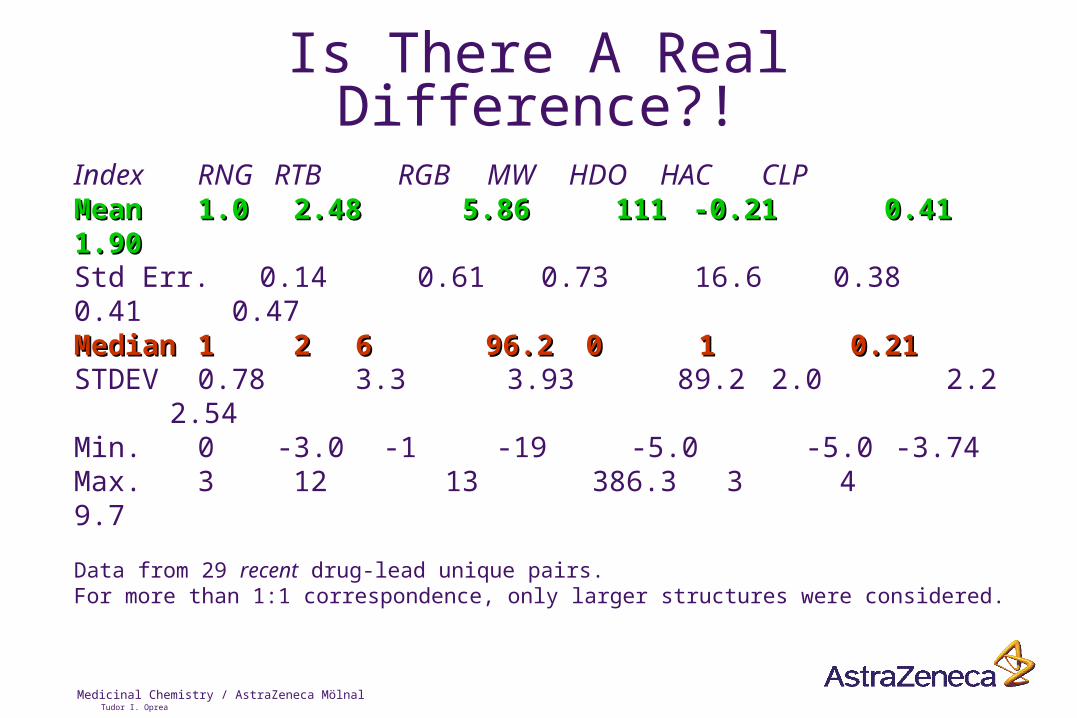
Index RNG RTB RGB MW HDO HAC CLPMeanMean 1.01.0 2.48 2.48 5.86 111 5.86 111 -0.21-0.21 0.41 0.41 1.90 1.90Std Err. 0.14 0.61 0.73 16.6 0.38 0.41 0.47MedianMedian 11 2 2 6 6 96.2 96.2 0 0 1 1 0.21 0.21STDEV 0.78 3.3 3.93 89.2 2.0 2.2 2.54Min. 0 -3.0 -1 -19 -5.0 -5.0 -3.74Max. 3 12 13 386.3 3 4 9.7
Data from 29 recent drug-lead unique pairs. For more than 1:1 correspondence, only larger structures were considered.
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
What Have We Learned?
• There is a difference between “leads” and “drugs”• However, this difference is apparent mostly in this difference is apparent mostly in
pairwise comparisonspairwise comparisons, as the “leadspace” and “drugspace” appear to overlap
• Average difference: 1 ring, 2 rotatable bonds, 100 1 ring, 2 rotatable bonds, 100 daltons, 1 acceptor and 0.5-1 LogP unitdaltons, 1 acceptor and 0.5-1 LogP unit
• Scoring leads yields 0.1-0.2 less units than drugs…
• The optimal way to use this information is to provide “leadlike” profiles for combichem libraries, as well as guidelines for HTS “hit” analysis in medicinal chemistry efforts

Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
How to Reach a Leadlike Profile?
• There is no universal answer for a leadlike library• However, depending on the final goal (e.g., CNS depending on the final goal (e.g., CNS
vs. urinary antiinflammatory drugs)vs. urinary antiinflammatory drugs), one can generate criteria to focus combichem or HTS libraries (go into “cherry-picking” mode right from the start)
• For example: 1-5 rings, 2-15 rotatable bonds, up to 1-5 rings, 2-15 rotatable bonds, up to 400 daltons, 0-2 donors, 1-8 acceptors and 0-3 400 daltons, 0-2 donors, 1-8 acceptors and 0-3 LogP units LogP units would cover MDDR-like space (75%)
• Additional criteria provided by druglike scoring schemes (e.g., DFPS > 0.4, PPFS > 0.4)
• PSA < 60 Å2 for CNS; PSA < 140 Å2 for oral activity...

Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
Lipinski’s Rule of 5: Just How Good Is It?!Lipinski’s Rule of 5: Just How Good Is It?!
0%
10%
20%
70%
80%
PASS FAIL SKIPPED
ACD
MDDRPDR
HB-acceptors
clogP
8070
6060
50
4030
2010
Ora
l abs
orpt
ion
2 3 4 5 6 7 8 9
More reagents than drugs pass the “Rule of 5” testMore reagents than drugs pass the “Rule of 5” test
Towards a computational model for oral absorption
Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
There Is A Leadlike Space
• The bottom line is that we can direct discovery towards leadlike profiling
• For the time being, we are limited by the number of lead-drug pairs in our historycal analysis
• An ISIS database is available for those interested.
• We are currently working on expanding this for including validated HTS hits (is there a “HTS-hits” space? Is it different from the leadlike space?)

Medicinal Chemistry / AstraZeneca MölnalTudor I. Oprea
Thanks to...
• Andy Davis, Simon Teague & Paul Leeson
• Bertil Samuelsson
• Mark Divers & Lennart Svensson
• Johan Gottfries, Ismael Zamora
• Thomas Kühler & Bob Carter

















