17
Lifting Monster BME 4013 BME Projects 1 Professor Nasir By: Owen Cameron Allaa Nori Date: 12/17/15

Lifting Monster
BME 4013 BME Projects 1
Professor Nasir
By: Owen Cameron
Allaa Nori
Date: 12/17/15

Abstract Our project goal is to collaborate with University of Detroit Mercy in the guided efforts to
produce a tangible device design for a spinal cord injury patient. The need statement is as
follows: An ability to lift dog bowls without bending of the spinal cord to assist a patient who
suffers Cauda Equina Syndrome. The design concept is a lifting apparatus which lifts bowls to
patient’s waist and lowers bowls to ground. Introducing an accessible button controller so patient
can have direct device interaction. The novelty for our project to provide a cheap or cost efficient
approach to the design with long lifetime and minimal maintenance as an approach.
Introduction Background
We are involved in a collaborative effort between Lawrence Technological University and
University of Detroit Mercy. The collaboration has guided efforts to assist a patient who suffers
cauda equina syndrome. She suffers partial paraplegia, clotting disorder and obesity. The patient
has two dogs and bending causes her back pain. Currently, she is undergoing therapy to
strengthen both lower limb muscles. We are interested in a mechanical based sub-systems 1 & 2
to create final design based on a product defined for class 1 or 2 device for adaptability for the
patient with no clinical trial need. Will allow the patient to adhere to the product more effectively
aligned with time constraints for UDM and LTU. The details of the design concept discuss the
selected design for the project.
Problem Identification
The patient suffers from cauda equina syndrome causing her to be a partial paraplegic. Bending
causes back pain and she has two dogs that she cannot currently feed on her own. Our patient
experiences difficulties in bending and symptoms of cauda equina syndrome include:
● Low back pain;
● Pain in one or both legs that starts in the buttocks and travels down the back of the thighs;
● Bladder and bowel problems (inability or difficulty urinating, incontinence, constipation);
● Weakness in lower extremities and loss of sensations.
The patient wants to be able to feed her dogs but cannot due to the bending required and her
disease states prohibits bending.
Disease State Fundamentals
Anatomy and Pathophysiology
The patient is suffers from cauda equina syndrome causing her to be a partial paraplegic.
Bending causes back pain and she has two dogs that she cannot currently feed on her own.
Symptoms of cauda equina syndrome include:
● Low back pain;
● Pain in one or both legs that starts in the buttocks and travels down the back of the thighs;
● Bladder and bowel problems (inability or difficulty urinating, incontinence, constipation);
● Weakness in lower extremities and loss of sensations.
Cauda equina syndrome is an uncommon compression of the nerves at the end of the spinal cord
within the spinal canal. The syndrome can be caused by any condition that results in direct
irritation or pinching of the nerves at the end of the spinal cord. Also, she is undergoing therapy
to strengthen both lower limb muscles.
Focus is identified for spinal cord injuries in general as economic impact with costs do not
specify otherwise:
Normal anatomy and physiology
Anatomy –
The spinal cord is part of the central nervous system (CNS) protected by the vertebral column. It
extends from the brain to the lower border of the 1st lumbar vertebra being around the thickness
of the little finger (45cm-males and 43cm-females). The spinal cord gray matter is surrounded by
the white matter at its circumference. White matter ceases toward the end of the spinal cord
while the gray matter blends into a single mass forming what is called as the cauda equine.
Physiology –
The spinal cord consumes the 3 most important functions of an individual: sensation, autonomic
and motor control. The spinal cord contains the link between the brain and the rest of the body
where all impulses from the brain throughout the body and various organs is carried through the
nerve tissue in the spinal cord. The same concept applies when organs and tissues sensory nerves
pass information to the brain by travelling up to the brain through the spinal cord.
Nógrádi, Antal, and Gerta Vrbová. "Anatomy and Physiology of the Spinal Cord."
Transplantation of Neural Tissue into the Spinal Cord. Springer US, 2006. 1-23.
Description of disease function, causal factors, and disease progression
Paraplegic patient due to a spinal cord injury. Injury within the thoracic level or below in the
spinal cord; result in poor trunk control due to lack of abdominal muscle control. T-1 lower level
spinal cord injury with normal hand function, preform all motor f unction of non-injured person,
with the exception of standing and walking. Ability of walking for short distances using walker
or long leg braces. Pain associated with standing and walking.
“Spinal Injury Network Paraplegia (Paraplegia) <http://www.spinal-
injury.net/paraplegia.htm>”
Clinical Presentation, Outcomes and Epidemiology
Clinical presentation associated with this disease/condition (spinal cord injury):
Focusing on symptoms related to the vertebral column (most commonly pain) and any motor or
sensory deficits. Ascertaining the mechanism of injury is also important in identifying the
potential for spinal injury. The axial skeleton should be examined to identify and provide initial
treatment of potentially unstable spinal fractures from both a mechanical and a neurologic basis.
The posterior cervical spine and paraspinal tissues should be evaluated for pain, swelling,
bruising, or possible malalignment. Logrolling the patient to systematically examine each
spinous process of the entire axial skeleton from the occiput to the sacrum can help identify and
localize injury. The skeletal level of injury is the level of the greatest vertebral damage on
radiograph.
“Spinal Cord Injuries Clinical Presentation (Spinal Cord Injuries Clinical Presentation: History
and Physical Examination) <http://emedicine.medscape.com/article/793582-clinical>”
Assess clinical outcomes and Epidemiology:
Clinical outcomes –
Loss of ventilatory muscle function from denervation and/or associated chest wall injury; Lung
injury such as pneumothorax, hemothorax, or pulmonary contusion; Decreased central
ventilatory drive that is associated with head injury or exogenous effect of alcohol and drugs.
“Spinal Cord Injuries Clinical Presentation (Spinal Cord Injuries Clinical Presentation: History
and Physical Examination) <http://emedicine.medscape.com/article/793582-clinical>”

Epidemiology –
Studies suggest the incidence rate of SCI is about 40 cases per million population. With a United
States population of over 300 million persons, over 12,500 new cases occur each year. There are
between 240,000 and 337,000 persons living with SCI in the United States. The average age at
injury has increased from 29 years during 1970s to 42 years since 2010. There is an about 4 to 1
male to female ratio. Approximately 24% of spinal cord injuries occur among blacks, which is
higher than the proportion of blacks in the general population (12%). (NSCISC)
Morbidity, Mortality, Incidence, and Prevalence of this condition
Morbidity –
250,000 Americans are spinal cord injured. 52% of spinal cord injured individuals are considered
paraplegic. (NSCISC)
Mortality –
Life Expectancies for persons with SCI are still significantly below life expectancies for those
without SCI and have not improved since the 1980s. Mortality rates are significantly higher
during the first year after injury than during subsequent years, particularly for severely injured
person. (NSCISC)
Incidence –
40 cases per million population in the U.S. or approximately 12,500 new cases each year.
(NSCISC)
Prevalence –
The number of people in the U.S. who are alive in 2014 who have SCI has been estimated to be
approximately 276,000 persons, with a range from 240,000 to 337,000 persons. (NSCISC)
Evaluate the Economic Impact
Cauda equina syndrome is often concurrent with congenital or degenerative diseases and
represents a high cost of care to those admitted to the hospital for surgery. Hospital stays
generally last 4 to 5 days, and cost an average of $100,000 to $150,000.

Overall cost of the disease on society/healthcare‐system:
Paraplegia (AIS ABS)
- First year = $518,905
- Each subsequent year = $68,739. (NSCISC)
Below is a table listing all of the average yearly expenses and estimated lifetime costs based on
severity of injury (NSCISC):
“Spinal Cord Injury Facts & Statistics (Spinal Cord Injury Facts & Statistics) <http://www.sci-
info-pages.com/facts.html>"
Observations and Interviews
Both the LTU and UDM met with the patient one time as a team to observe and interview the
patient. She appears to have a very open living room space providing easy access for her
motorized cart that she rests on. There are two dogs that are in an open cage when entering the
living room from the front door. Also, there are a few hand rails bolted into the studs on the
walls when entering and leaving the living room to the back deck awning. She appears to need a
device to allow her to feed her dogs that she can easily interact with that won’t cause her to bend.
Current Treatment Options
Existing and emerging solutions for diagnosis, treating, and managing given disease state
Diagnosis –
Computerized tomography (CT) scan. A CT scan may provide a better look at abnormalities seen
on an X-ray. This scan uses computers to form a series of cross-sectional images that can define
bone, disk and other problems.
X-rays. Medical personnel typically order these tests on people who are suspected of having a
spinal cord injury after trauma. X-rays can reveal vertebral (spinal column) problems, tumors,
fractures or degenerative changes in the spine.
Magnetic resonance imaging (MRI). MRI uses a strong magnetic field and radio waves to
produce computer-generated images. This test is very helpful for looking at the spinal cord and
identifying herniated disks, blood clots or other masses that may be compressing the spinal cord.
“Spinal cord injury (Tests and diagnosis) <http://www.mayoclinic.org/diseases-
conditions/spinal-cord-injury/basics/tests-diagnosis/con-20023837>”
Treatment and Management –
Cauda equina syndrome is a medical emergency. Decompression surgery is required to relieve
the substance that is causing pressure/pinching with the nerves of the spinal cord. Early surgery
can prevent further nerve damage that may be irreversible. Long-term management includes pain
medicine, physical therapy, supportive braces, urinary catheters, and other treatments.
A spinal cord injury needs to be treated right away. The time between the injury and treatment
can affect the outcomes. Medicines called corticosteroids are sometimes used to reduce swelling
that may damage the spinal cord. If spinal cord pressure is caused by a growth that can be
removed or reduced before the spinal nerves are completely destroyed, paralysis may improve.
Surgery may be needed to:
- Realign the spinal bones (vertebrae)
- Remove fluid or tissue that presses on the spinal cord (decompression laminectomy)
- Remove bone fragments, disk fragments, or foreign objects
- Fuse broken spinal bones or place spinal braces
- Bedrest may be needed to allow the bones of the spine to heal.
- Spinal traction may be recommended. This can help keep the spine from moving. The skull
may be held in place with tongs. These are metal braces placed in the skull and attached to
weights or to a harness on the body (halo vest). You may need to wear the spine braces for many
months.
“New York Times (Health Guide) <http://www.nytimes.com/health/guides/disease/spinal-cord-
trauma/overview.html>"
Market Analysis
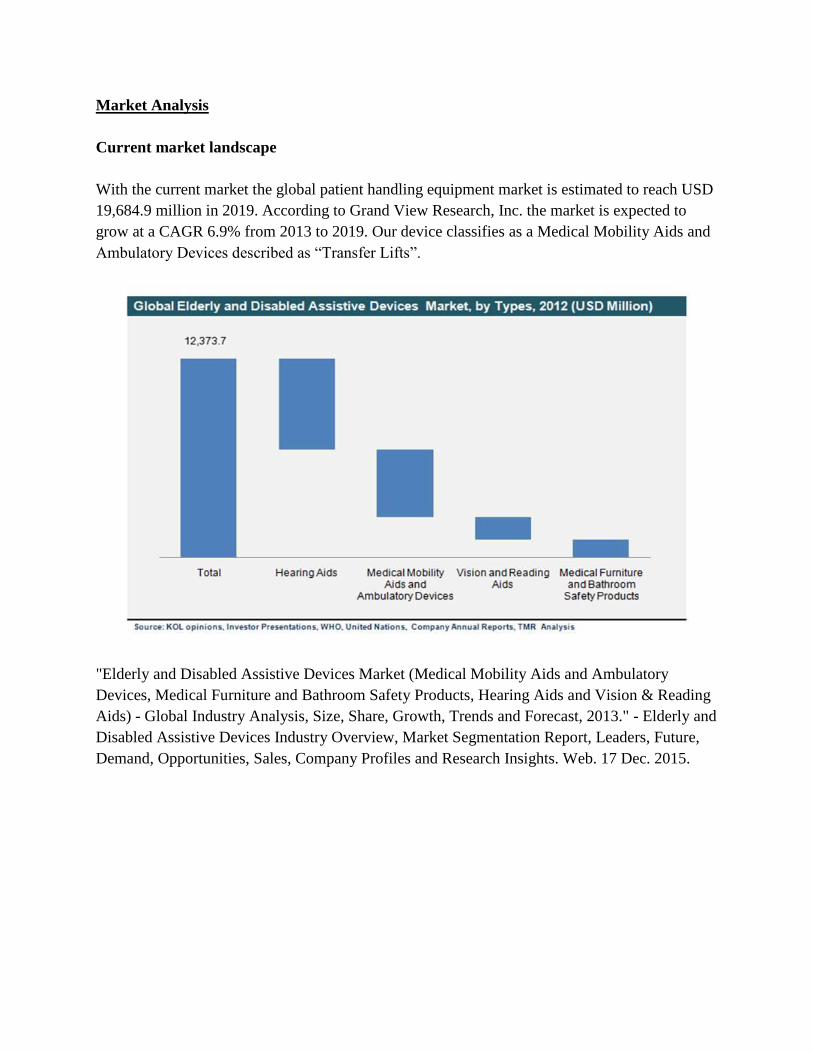
Current market landscape
With the current market the global patient handling equipment market is estimated to reach USD
19,684.9 million in 2019. According to Grand View Research, Inc. the market is expected to
grow at a CAGR 6.9% from 2013 to 2019. Our device classifies as a Medical Mobility Aids and
Ambulatory Devices described as “Transfer Lifts”.
"Elderly and Disabled Assistive Devices Market (Medical Mobility Aids and Ambulatory
Devices, Medical Furniture and Bathroom Safety Products, Hearing Aids and Vision & Reading
Aids) - Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013." - Elderly and
Disabled Assistive Devices Industry Overview, Market Segmentation Report, Leaders, Future,
Demand, Opportunities, Sales, Company Profiles and Research Insights. Web. 17 Dec. 2015.

Describing market segments
The personal mobility devices market can be segmented into the following: Pre-hospital, In-
hospital and Post Hospital. The results are either distributed for the hospital or home health care
usage.
Pre hospital:
- EMS
In hospital:
- Inpatient care
Post hospital:
- Rehabilitation Centers
- In-home care
Defining market size, growth, and competitive dynamics of each segment:
Post hospital (Rehabilitation Centers)
Market size –
Projects are currently located in the following states: Alabama, Colorado, District of Columbia,
Georgia, Illinois, Massachusetts, Michigan, New Jersey, New York, Ohio, Pennsylvania, Texas,
and Washington.
Growth –
Model SCI Centers across the United States work together to demonstrate improved care,
maintain a national database, participate in independent and collaborative research, and provide
continuing education relating to spinal cord injury.
Competitive dynamics –
Between Rehabilitation centers - spinal cord injury accredited centers and non-accredited
centers.
“Rehabilitation Centers (Christopher & Dana Reeve Foundation)
<http://www.christopherreeve.org/site/c.mtKZKgMWKwG/b.4514607/k.681B/Rehabilitation_C
enters.htm#>"

Pre hospital (EMS), In hospital (In-home care) and Post hospital (In-home care)
Market size –
North America (U.S.), Europe (Germany, UK, France, Italy, Spain, Austria, Switzerland), Asia
Pacific (Japan)
Growth –
$12.373 billion in 2013 to $19.684 billion in 2019;
Forecasted to grow at CAGR of 6.2% from 2013 to 2019.
Competitive dynamics –
Developing technologically advanced personal mobility devices via extensive R&D investments
and entering into strategic alliances with buyers are some key sustainability strategies are
adopted by these market players.
Describing to what extent stakeholder needs are being met in each segment
Clinicians –
Evaluate and dictate on which methods to pursue for optimal care for patient where resources are
able to be pursued.
Hospitals –
Based on the injury type and required healing methods hospitals make revenue through
programs, directly from patient or through insurance means. Improvements in R&D along with
inside the hospital enhance quality of care.
Insurance companies –
Based on treatments available they either accept or deny coverage based on specified cost/benefit
ratio. Companies choose most optimal coverage based on cost/benefit ratio to align with overall
needs of the patient and which options for pursuance.
Rehabilitation centers –
After stabilization, the person with a spinal cord injury needs to go to a specialized hospital
called a rehabilitation center. National Institute on Disability and Rehabilitation Research
(NIDRR) funds 14 Model Spinal Cord Injury Facilities in the U.S.

Listing key considerations for choosing a target market
- Existing solutions available in market segment
- Insurance coverage in market segment
- Number of patients in market segment
- Cost/benefit ratio in market segment
- Availability of resources in market segment
- Adaptability for usage in market segment
Stakeholder Analysis
Influential stakeholders
i. First Responders (EMS/paramedics (minimize effects of any head or neck trauma), EMTs,
clinician engagement)
ii. Hospital - Personnel/Care
iii. Rehabilitation Centers
iv. Surgeons (Neurosurgeon, Orthopedic surgeon, etc.)
v. Physiatrist (physical medicine and rehabilitation)
vi. Care-giver
vii. Physiatrist for rehabilitation
Potential conflicts
i. Patients need improved devices and treatment but insurance companies will not pay for it.
ii. Limited accredited Rehabilitation centers for optimal treatment and care
iii. Limited resources with inpatient and outpatient care
iv. Limited coverage from insurance companies for personal mobility devices for outpatient care
Recognizing which stakeholders are the decision makers
i. Clinicians (decision makers who would determine the injury level by collecting diagnosis
data.)
ii. Hospitals
iii. Insurance companies
iv. Rehabilitation Centers

Mapping the current continuum of care
i. Hospitalization / Surgeon referral
ii. Spinal cord treatment
iii. Outpatient extended care (monitor injury with infection prevention)
iv. Rehabilitation Centers
v. Utilization of walker around home
vi. Care-giver to help with daily needs
vii. Motorized chair when leaving home
viii. Physiatrist for rehabilitation
Design Concept

Design Justification
We have decided on a concept for design based on our patient need. The patient specifically
requested a device capable of lifting and lowering 2 dog bowls containing water and food. Also,
the patient wanted the device to be controlled by clicking button in terms of operating. Another
request our patient had, is for the device to have an excellent life-time. From there, UDM and
LTU teams decided on having a mechanical structure with a lifting apparatus. What is
considered novel about the design application and cost efficiency. After discussion and research
from both teams we have come across the lifting method using a stepper motor. A stepper motor
can work effectively and accurately for short periods of daily operations. The stepper motors
have a wide range of properties such as torque, speed and accuracy suiting our design perfectly.
As stepper motors come in variety of properties other components such as linear slides and
couplers come in wide range of specifications to adapt almost all kinds of stepper motors.
Materials
Stepper Motor including power supply, driver and controller
Ball screw linear slide
Coupler
Cables
Button switches

Methods
LTU and UDM teams have developed precise methods which need to be done in order to
get the project completed as follows:
1. Design the mechanical structure of the body
This part of the project is purely UDM side of responsibilities, where UDM team designs the
mechanical structure that will have the lifting prototype attached to it. For this part, UDM team
will need to consider all parameters and aspects associated with the making of the structure in
terms of stability and center of mass. UDM team are expected to perform structural analysis
within the making of the structure. UDM team will be using Solidworks for modeling the
structure which will be also used for testing. Since Solidworks provides multiple mechanical
stimulation constructs the program can give data related to 3D models, structures and failure
concerns.
2. Design/purchase ball screw linear slide
This part of the project will be LTU team responsibility, where LTU team decide on the proper
ball screw linear slide for the prototype. UDM team are expected to provide LTU team with the
final dimensions of the mechanical structure, and LTU team will consider human interaction
phase with the prototype by designing the lifting design to reach its lowest point on the ground
and its highest point up to patient’s waist for the most convenient handling to improve the patient
life.
3. Purchase stepper motor + coupler
Once getting the first two methods done while deciding on the platform material and weight by
both teams LTU is expected to figure the proper motor to use. Deciding on the proper motor to
use for the prototype is going to be associated with many consideration. The main consideration
is the motor torque and speed. The relation between the motor torque and the motor speed
defines the capabilities of the motor in terms of accuracy and lifting abilities. Finally, choosing
the proper coupler that will be the attachment between the motor and the linear slide.
4. Compile the actuator
Compiling the actuator has to do with the 2nd and 3rd methods. Testing the actuator performance
will be the main concern within this part of the methods where we are aiming to have a prototype
that has an excellent lifetime. Therefore, our testing of the actuator performance will take into
account all failure concerns to make justification if needed.
5. Write Arduino code and implement to controller
Writing Arduino code that will be the communication between the controller (2 buttons) and the
actuator to set limits and proper operation of the actuator.

6. Test final prototype for final confirmation or changes
Finally, testing the final prototype by using multiple subjects with different weight and shapes on
the platform for a variety of ranges of time. The approach assures prototype effectiveness while
more importantly assuring safety concerns and failure possibilities for improvement and/or
changes. In addition, electrical components will be test for safety concerns in terms of heating
and human/animals interactions.
Project Relevance and Broader Impact
There is approximately 12,000 new cases of spinal cord injury per year. The number of people is
around 270,000 persons who have SCI in the United States alone as of 2012. Designing our
device will allow patients who have SCI to bend and feed their pets that would otherwise be too
difficult or impossible. Within the next 7 years there is going to be an increase from around 12
billion in revenue to 19 billion for the global elderly and assisted devices market. With the
increased revenue expectations the need for our design will increase as the market segment
expands.
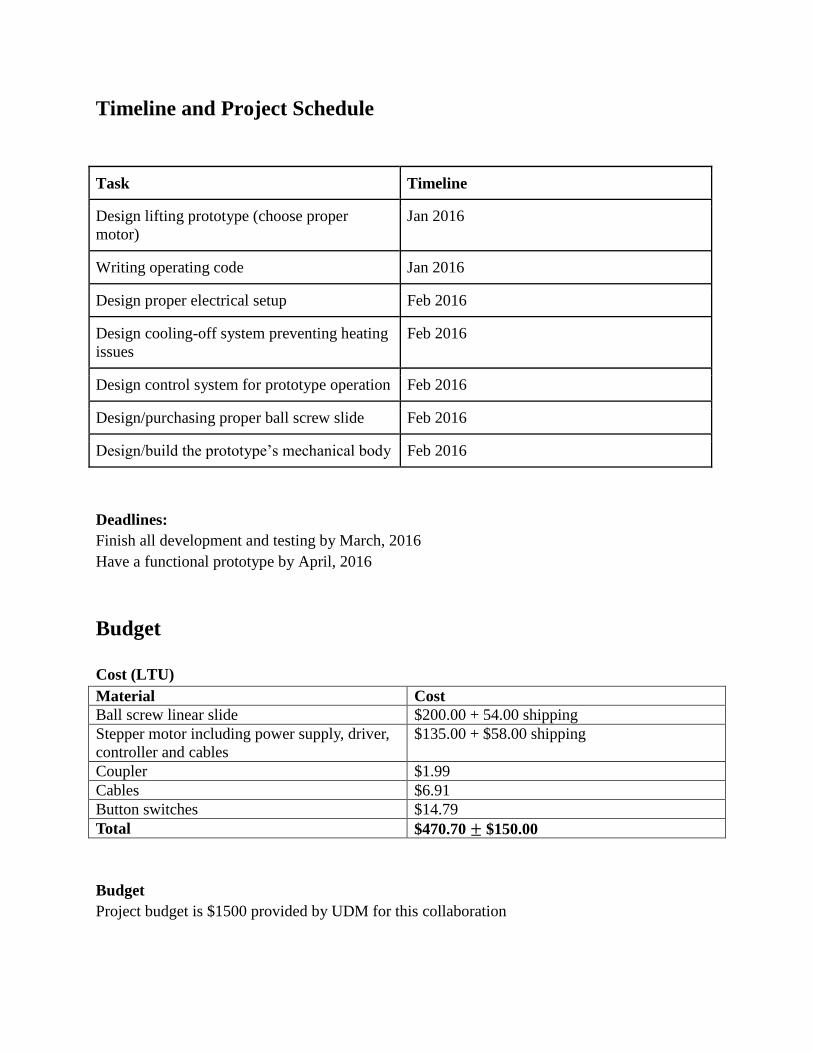
Timeline and Project Schedule
Task Timeline
Design lifting prototype (choose proper
motor)
Jan 2016
Writing operating code Jan 2016
Design proper electrical setup Feb 2016
Design cooling-off system preventing heating
issues
Feb 2016
Design control system for prototype operation Feb 2016
Design/purchasing proper ball screw slide Feb 2016
Design/build the prototype’s mechanical body Feb 2016
Deadlines:
Finish all development and testing by March, 2016
Have a functional prototype by April, 2016
Budget
Cost (LTU)
Material Cost
Ball screw linear slide $200.00 + 54.00 shipping
Stepper motor including power supply, driver,
controller and cables
$135.00 + $58.00 shipping
Coupler $1.99
Cables $6.91
Button switches $14.79
Total $470.70 ± $150.00
Budget
Project budget is $1500 provided by UDM for this collaboration

References
1) “Elderly and Disabled Assistive Devices Market (Medical Mobility Aids and Ambulatory
Devices, Medical Furniture and Bathroom Safety Products, Hearing Aids and Vision & Reading
Aids) - Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013." - Elderly and
Disabled Assistive Devices Industry Overview, Market Segmentation Report, Leaders, Future,
Demand, Opportunities, Sales, Company Profiles and Research Insights. Web. 17 Dec. 2015.
2) Nógrádi, Antal, and Gerta Vrbová. "Anatomy and Physiology of the Spinal Cord."
Transplantation of Neural Tissue into the Spinal Cord. Springer US, 2006. 1-23.
3) “Spinal Injury Network Paraplegia (Paraplegia) <http://www.spinal-
injury.net/paraplegia.htm>”
4) “Spinal Cord Injuries Clinical Presentation (Spinal Cord Injuries Clinical Presentation:
History and Physical Examination) <http://emedicine.medscape.com/article/793582-clinical>”
5) “Spinal Cord Injury Facts & Statistics (Spinal Cord Injury Facts & Statistics)
<http://www.sci-info-pages.com/facts.html>"
6) “Spinal cord injury (Tests and diagnosis) <http://www.mayoclinic.org/diseases-
conditions/spinal-cord-injury/basics/tests-diagnosis/con-20023837>”
7) “New York Times (Health Guide)<http://www.nytimes.com/health/guides/disease/spinal-
cord-trauma/overview.html>"
8) “Personal Mobility Devices Market Analysis By Product (Wheelchairs, Scooters, Walking
Aids, Canes, Crutches, Walkers, Premium Rollators, Low Cost Rollators) And Segment
Forecasts To 2020 (Personal Mobility Devices Market Analysis By Product And Segment
Forecasts To 2020) <http://www.grandviewresearch.com/industry-analysis/personal-mobility-
devices-market>"
9) “Rehabilitation Centers (Christopher & Dana Reeve Foundation)
<http://www.christopherreeve.org/site/c.mtKZKgMWKwG/b.4514607/k.681B/Rehabilitation_C
enters.htm#>"
9) “Elderly and Disabled Assistive Devices Market (Medical Mobility Aids and Ambulatory
Devices, Medical Furniture and Bathroom Safety Products, Hearing Aids and Vision & Reading
Aids) - Global Industry Analysis, Size, Share, Growth, Trends and Forecast, 2013." - Elderly and
Disabled Assistive Devices Industry Overview, Market Segmentation Report, Leaders, Future,
Demand, Opportunities, Sales, Company Profiles and Research Insights. Web. 17 Dec. 2015.”

















