43
David Vassilaros Sr. Vice President, Operations Benecon Population Health Management The employer & broker perspective
| Date post: | 13-Apr-2017 |
| Category: |
Healthcare |
| Upload: | centralpahef |
| View: | 140 times |
| Download: | 0 times |

David Vassilaros Sr. Vice President, Operations
Benecon
Population Health Management
The employer & broker perspective

population health management
2
noun; “the art and practice of getting people to do stuff they probably don’t really want to do because you know stuff about their health they don’t think you know or even know themselves”
Employer definition

PPACA & leverage
3

4
15%
85%
Small employers (<200)
Self-‐funded Fully-‐insured
Employers who care the most
91%
9%
Large employers (5,000+)
Self-‐funded Fully-‐insured
60%
40%
All U.S. employers
Self-‐funded Fully-‐insured

5
Hi, my name is Data. Big Health Data.
So a guy walks into a bar…
That’s ok, I already know who you are. And why you went to the doctor last week.
Hi I’m…

6
Data is the new “black”
What they’re actually getting What employers think they’re getting

7
“The Bet”

8
The 9.6% question
How much are employers willing to invest to turn their data into healthy employees, and ultimately health cost savings?

Employers & brokers must answer these questions:
1. Do they really want to do something? 2. Are they willing to use their influence to leverage
change? 3. Do they understand data isn’t perfect? 4. What are they willing to invest?
9

Adding value to self-funding
BeneconPLUS
take control of claim costs
Maximize value
11
data repor?ng analysis interven?on analysis interven?on repor?ng
take control

how
it w
orks
Benefit informatics
value to you
no
addiAonal cost
carriers share claim data with BI
Benecon access via secure web
Benecon runs reports, analysis
can’t fix what isn’t measured
focus on your actual claim trends
savings & control
12

Unleash the power
13
data reporAng 1
data analysis 2
real intervenAon 3
savings & control

14
Nurse NavigaAon
Tailored Support
Healthy Goals
Culture of Health
ConsultaAon on creaAng own healthy culture
Research Support PaAent advocacy
Set and achieve healthy goals Diet, exercise, stress relief, sleep & more CerAfied health coach & experienced RN
Webinars Lunch & Learns WriVen materials

Listening to Employers: How health systems can support pop
health management Health System PerspecAve
John Holmes VP Finance, Pop Health & Payor ContracAng
WellSpan Health

The current state of health care is unsustainable.
SO WHAT CAN EMPLOYERS DO ABOUT IT? • There are several conflicts that need to be resolved/managed: -‐ healthcare exp growth > revenue growth -‐ engaging employees in their own health w/out being big brother -‐ finding a health partner who can help you vs just milk you
• What role do health systems have in all this?

HEALTH SYSTEMS & POP HEALTH
• TradiAonal health care vs. pop health – electrician example
• Health systems learning how to get paid for value & keeping folks healthy -‐ complete retooling necessary
• Having skin in the game -‐ financial risk (follow the money)
• Intended result -‐ consistent alignment of objecAves w/employers

ENGAGING YOUR HEALTH SYSTEM
• Need to define/explain our pop health journey & how it impacts community
• What are we doing to accomplish the Triple Aim: -‐ Improving paAent experience -‐ Improving employee health -‐ Reducing cost of health care
• What insurers are we partnering with?
• Engaging employers to reduce their healthcare costs

POP HEALTH ISSUE: ACCESS
• Provider access & pop health are a conundrum -‐ Employees want complete provider access -‐ Employers want to control costs (unAl they are the employee!) -‐ Health systems need to manage care within their span of control
• Suggested soluAon: employee choice w/product offerings/benefit design -‐ IncenAves for narrow network (with access) -‐ Unlimited access will cost employees more

POP HEALTH ISSUE: COST
• Narrow network trade-‐off s/b lower employer/employee cost (codeword: bigger discounts vs. tradiAonal network)
• Status of our system’s clinical transformaAon – where are we with retooling? How does this help keep healthcare costs down?
• What is being done to promote price transparency (ease) to protect health systems from niche retail providers?
• How are our providers incented to work (volume or value)? Is there (their) skin in the game financially?

Clinical TransformaCon
LIFT-‐PCMH (by prac?ce)
Quality Improvement Teams Care CoordinaAon Teams PracAce Specific ReporAng
Case Management (care of the individual)
Rising risk and high uAlizer populaAons
U?liza?on Management (op?mal use of services) System UM CommiVees:
Pharmacy Laboratory Imaging
Procedural emerging technology Hospital UR
Disease Management (focusing on the care
con?nuum) Service Line Projects
Specialist Physician Champions
Clinical EffecAveness Teams

POP HEALTH ISSUE: QUALITY
• Need to define what consAtutes quality in your health system – you can’t do it all
• Avoid cycling thru quality measures as flavors of the month – sAck with them
• Look to be as consistent in your P4V opportuniAes as much as possible
• Make quality a gateway to financial reward vs. an amerthought

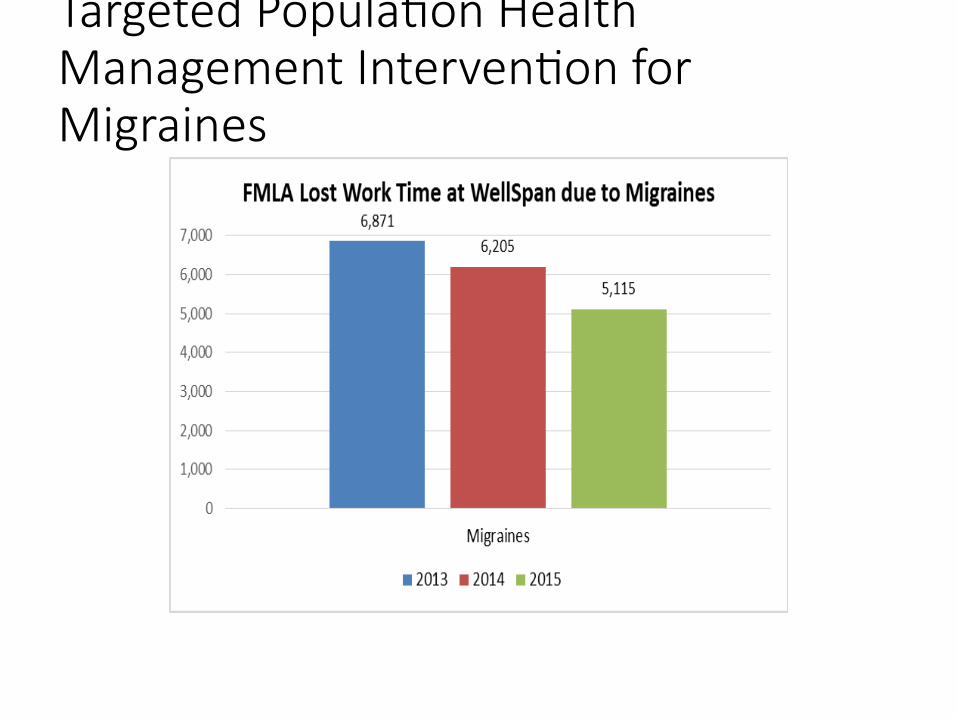
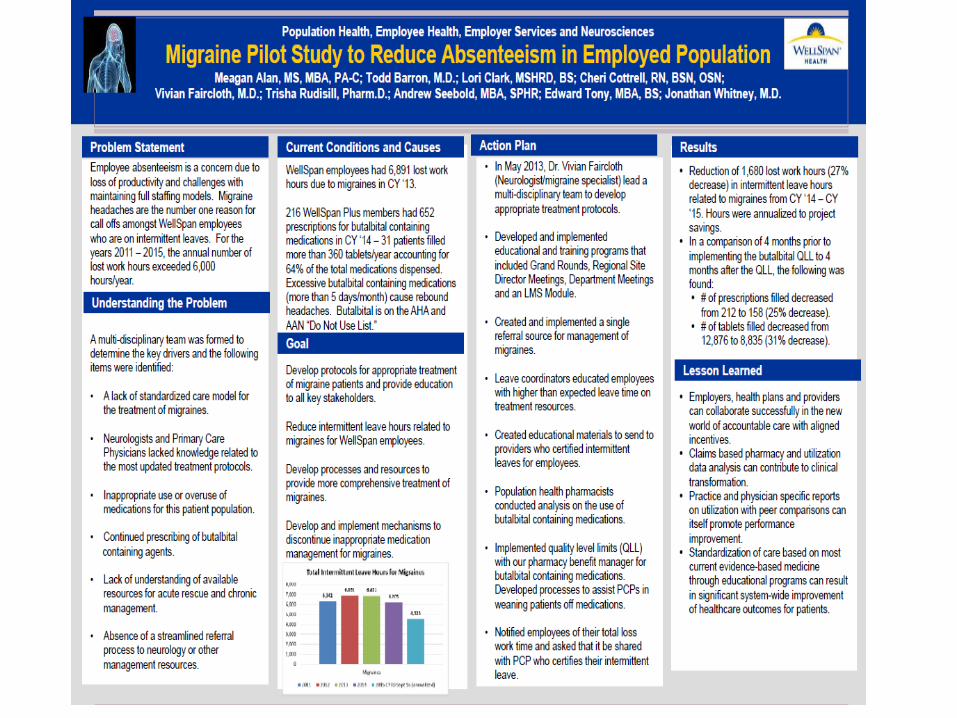
Targeted PopulaCon Health Management IntervenCon for Migraines

Q & A

Listening to Employers: How Health Systems Can Support Population Health Management
Employer Coalition Perspective
Diane N. Hess, CLU CEBS
Interim Executive Director

Business Group on Health
Vision – To provide a forum and a voice for the business community on healthcare through collaboration among stakeholders
Mission – To promote continuous improvement in the quality and cost of healthcare for our member companies, their employees and dependents

Our Strategy

What we know about healthcare cost drivers
� Statistically 80% of claims come from less than 20% of covered population
� Who is in the 20% can change from year to year
� A large portion of healthcare costs could be avoided
� It is difficult to get people’s attention until they need care and then it may be too late!
� Managing health is a long term process

BGH members and healthcare � Costs have continued to escalate and in our market now
exceed the national average
� Employers continue to look for tools to help mitigate cost increases
� Many are using wellness programs to engage employees and covered dependents in the efforts to stem the tide of ever-increasing costs
� Obesity/Diabetes is a major driver of costs in our market
� Plan designs and procedures have become increasing complicated

What employees really want…
Good
Cheap Fast

What employers really want…
Good
Cheap Fast

How does ‘population health’ fit into the conversation?
1. What are we trying to manage - health or sick care?
2. How do we get employees engaged in the process?
3. Since population health management is a long term strategy, how do we get short-term buy-in from the C-Suite?
4. How do all the new delivery models impact employee behavior and the overall health of the population?

The challenge - the new ‘divide’
Before ACA, coverage is all we talked about -
Insured Uninsured

The challenge - the new ‘divide’
After ACA?
Gov’t mandated, fully insured plans controlled by few carriers / providers
Value-designed, self-funded plans using open markets, innovative providers, products and services
Small Group / Individual Large Group

What the market looks like
Carrier Provider Provider
Gov’t
Carrier
Gov’t
Before ACA After ACA
$$
Current Outcomes (Industry sectors will dominate)
� Market consolidation of both carriers and health systems: (less choice)
� Economies of scale
� Market power and influence (narrow networks)
� Protect current industry players
� Providers absorb more financial ‘risk’
� More Gov’t regulation / refinements � Wellness regulation: EEOC, ACA, ADA
� Compliance requirements / reporting
� Medicare/Medicaid payment changes

Where we need to go “Free markets will always undermine central planning.”
Alan Greenspan, former Federal Reserve Chairman
Disintermediation: disˌin(t)ərmēdēˈāSH(ə)n/
� reduction in the use of intermediaries between producers and consumers
� The opportunity to deliver a product or service to a consumer with a higher perceived value than the incumbent by changing the delivery method

Resulting Outcomes (The market will dominate)
� Personalized technology (me-centered)
� Crowd sourcing
� Retail health / specialty niche players
� Smaller, patient-centered facilities with lower overhead
� Use of lower priced labor (PA’s, certified nurse practitioners)
� Concierge services (peer-to-peer)
� Alternative convalescent care (home, rehab, self-monitoring)
� Data & price transparency

BGH Initiatives
� ACTRx Diabetes Management Program
� CoActive
� Wellness education
� Data Initiative

Questions?
Thank you…

















