37
Living and Dying with COPD 15.00-15.40 Dr Patrick White Senior Lecturer King’s College London Department of General Practice and Primary Care
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | carol-diane-cunningham |
| View: | 213 times |
| Download: | 0 times |

Living and Dying with COPD15.00-15.40
Dr Patrick WhiteSenior Lecturer
King’s College LondonDepartment of General Practice and Primary
Care
COPD – a major cause of morbidity and mortality
• 5-10% of the population have it
• 1.5% diagnosed by clinicians
• <1% on QOF registers
• c65 in an average practice of 6500 patients
COPD – Exacerbations and admissions
• Moderate and severe COPD - 2-3 exacerbations a year per patient
with moderate or severe disease• Biggest single cause of emergency
admissions• Associated with major co-morbidity
- All the major smoking related diseases and the major degenerative diseases

Deaths and COPD
• 23500+ COPD deaths per year compared to 28,000 deaths caused by lung cancer in England and Wales
• Premature death – mean age of death from COPD 76 years
• Only c 40% of people with COPD die from it
• Soon to become 4th cause of mortality worldwide
The keys to COPD care
• Spirometry diagnosis• Active COPD register• Smoking cessation• Pulmonary rehabilitation
- Exercise, education, social engagement• Drugs
- Short-acting bronchodilators- Inhaled steroids- Long-acting bronchodilators- Theophyllines

The keys to COPD care
• Spirometry diagnosis• Active COPD register• Smoking cessation• Pulmonary rehabilitation
- Exercise, education, social engagement• Drugs
- Short-acting bronchodilators- Inhaled steroids- Long-acting bronchodilators- Theophyllines
? End of life or palliative care?
Advanced COPD – are research and service out of step?
• Powerful drive for providing palliative care for patients with advanced COPD
• Repeated assertions that COPD patients with <1 yr prognosis can be identified
• Assumption that because patients die from chronic illness their deaths can be prepared
End of life research in COPD
Key questions
• Where does the drive to provide palliative care for COPD come from?
• Can prognosis be defined in COPD?• What are the palliative care needs of
people with advanced COPD?

Why do we think people with COPD have palliative care needs?
• Heavy burden of symptoms • Symptoms are more severe than
lung cancer but services are limited with virtually no end of life care
• Gore et al Thorax 2000;55(12):1000-6. • Edmonds et al 2001 Palliat Med 2001;15(4):287-95.
• Elkington, White, et al Palliat Med 2005;19 485-91
• GPs want to know if some COPD patients should be on a palliative care register
End of life research in COPD

Why do we think people with COPD have palliative care needs?
• Heavy burden of symptoms • Symptoms are more severe than
lung cancer but services are limited with virtually no end of life care
• Gore et al Thorax 2000;55(12):1000-6. • Edmonds et al 2001 Palliat Med 2001;15(4):287-95.
• Elkington, White, et al Palliat Med 2005;19 485-91
• GPs want to know if some COPD patients should be on a palliative care register
End of life research in COPD

Health and social service needs in the last year of life of COPD
• Retrospective questionnaire survey of the informants of 399 COPD deaths
• All subjects who died from COPD between Jan-Jun 2001 in four London areas
• Physical and psychological symptoms, day to day functioning, home oxygen, contact with services, information about the illness, place of death
Elkington, White, et al Pall Med 2005 19:485-491
End of life research in COPD

Service Provision
• >35% of patients lacked regular follow up in hospital or in the community
• One third of patients saw their GP less than 3 monthly or never
• Lack of home-based services although many patients were housebound
Do people with COPD have palliative care needs?
• Symptom control• Information needs• Preferred place of care

Most who died from COPD may have had palliative care needs
In the last year of life40% had breathlessness unrelieved68% had low mood unrelieved51% had pain unrelieved
20% did not know they might die70% died in hospital (for 25% of whom it
was not the best place to die)

Palliative care of COPD as a non-malignant disease?
• End of life care strategy of NHS• Crescendo of calls for recognition of
palliative care needs of advanced COPD
Seamark J Roy Coll Phys 2007;
Rocker J Pall Med 2007; Curtis et al Eur Resp J 2007

Palliative care of COPD as a non-malignant disease
• Palliative care agenda – high quality care, right place, right time
• Patients who do not want admission • Patients who want to avoid non-invasive
ventilation • Patients who need symptom control as a priority• Patients who recover from acute exacerbations
and have to go back to very poor quality of life
Challenge for primary and secondary care is to consider alternatives in COPD patients with severe disease

How should the palliative care needs of COPD patients be defined?
• Gradual transition from general routine care to palliative care?
• When the prognosis reaches a certain critical point?
• When symptoms become uncontrolled and intolerable?
• When death becomes a high risk?

Can we make an accurate prognosis in COPD?
• Three reviews in the last year claim it is possible to identify COPD patients within last year of lifeSeamark J Roy Coll Phys 2007; Rocker J Pall Med 2007; Curtis
et al Eur Resp J 2007
• UK Gold Standards Framework suggests that using available cross-sectional parameters we can identify people with COPD who are within a year of death
http://www.goldstandardsframework.nhs.uk/

Making a prognosis in COPD
• Mortality in severe COPD is between 36% and 50% at 2 years
Connors et al. Am J Respir Crit Care Med 1996;154(4 Pt 1):959-67 Almagro et al. Chest 2002;121(5):1441-8
• Predictors of mortality include- Low BMI, Low FEV1, dyspnoea, low 6MWD,
Fat free body mass, number of hospital admissions, maintenance oral steroids, quadriceps strength, congestive heart failure, low albumin, cor pulmonale, oxygen saturation,
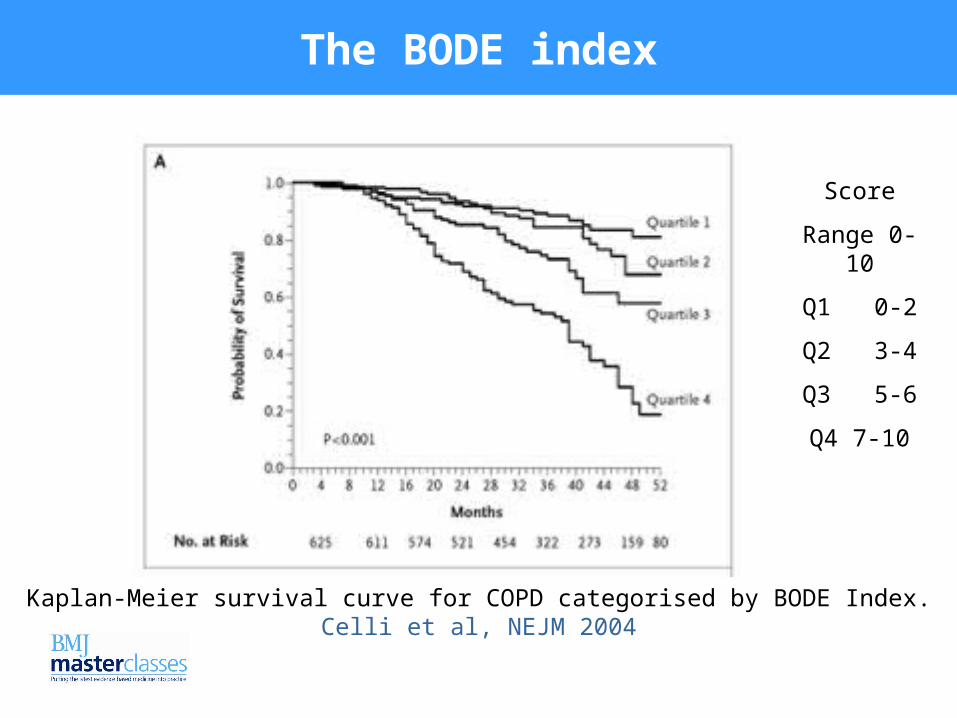
The BODE index
Score
Range 0-10
Q1 0-2
Q2 3-4
Q3 5-6
Q4 7-10
Kaplan-Meier survival curve for COPD categorised by BODE Index. Celli et al, NEJM 2004

Palliative care needs of the most severe
• 110 COPD patients (87 men), mean age 73 years who survived acute hypercapnic respiratory failure after non-invasive ventilation in Hong Kong in 2002
• 49.1% had died within a year. Chu et al, Thorax 2004, 59, 1020-25
Patients’ views about end of life discussions in COPD
• Review of 19 patient case studies in which advanced directives against further ventilation were made
• Mean length of survival from the decision not to be ventilated was 210 days
• 11 of 19 survived more than a year
Pang et al J Critical Care 2004

South London audit of COPD palliative care referrals
81 referrals over 2 years
68 deaths14 discharges (2 re-referred)
1 still under palliative care

South London audit of COPD palliative care referrals
• mean age at first referral = 74.4 years- range = 50 to 92 years.
• Mean age at death 74.8 yrs (50-92)

Time between first referral to palliative care team and death
02468
101214161820
Series1
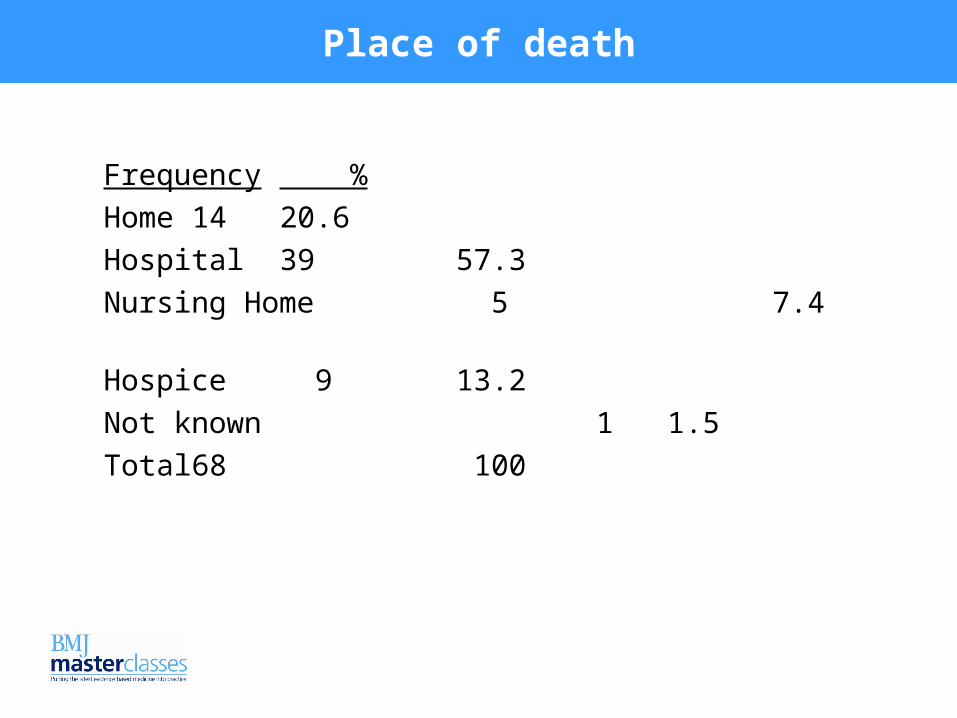
Place of death
Frequency %
Home 14 20.6
Hospital 39 57.3
Nursing Home 5 7.4
Hospice 9 13.2
Not known 1 1.5
Total 68 100

Resus/Ventilation Ever Discussed?
05
101520253035404550
Yes No NK
Nu
mb
er o
f ca
ses
Patient
Family
Preferred Place of Care Discussed?
0
5
10
15
20
25
30
35
40
Yes No NK
Nu
mb
er o
f ca
ses
Patient
Family
Prognosis Ever Discussed?
05
101520253035404550
Yes No NKN
um
ber
of
case
s
Patient
Family

EDDM last 6 wks life
(EDDM=equivalent daily dose morphine)
0
2
4
6
8
10
12
14
16
18
20
no. cases 12 19 4 8 6 6 13
0mg >1<10 11.-20 21.-30 >30<99mg >100mg Nk

Opioid indication last 6 weeks
• Pain 2• Dyspnoea 18• Pain and dyspnoea 12• Not recorded 21

Prospective study of palliative care needs of advanced COPD
White P, White S, Edmonds P, Moxham J, Gysels M, Shipman C. Funded by Guy’s and St Thomas Charity
• No prospective surveys of palliative care needs in COPD
• No reliable guidance for generalists or specialists on palliative care needs in COPD
• Our aim was to identify patients with palliative care needs and to define their needs
What we did
• Prospective community based survey• Patients with severe COPD from GP registers• Interview questionnaire (developed from
qualitative study) on symptoms, impact on daily life, use of services, use of drugs, caring and dependence, views of disease and treatments, information needs
• Lung function, BMI, HADS, Respiratory specific quality of life, MRC dyspnoea scale, Pain questionnaire

Patients in the study
• 44 (80%) of 55 practices took part• 163 (61%) of 265 eligible patients (4/6 per
practice)• Data on 145 with advanced disease
• Mean age 72 years (46-93), Female 50%• FEV1 <40% expected (Quanjer et al)• 88% short of breath most days/everyday• 45% housebound• 75% had a carer (45% in the home)
• Respondents at least as severe as non-respondents

Treatment of breathlessness in advanced COPDBreathlessness intervention service• Non-pharmacological interventions:
- Hand-held fan- Anxiety management- Physiotherapy
• Pharmacological- Opiates- Benzodiazepines- Phenothiazines
• Booth S, Moosavi SH, et al. Nat Clin Pract Oncol 2008 5(2):90-100.
• Booth S, Farquhar M, et al. Palliat Support Care 2006;4(3):287-93.

How does the role of prognosis in COPD compare with that in cancer?
• Prognosis in cancer is based on longitudinal data
• Every guide to prognosis in COPD uses cross-sectional data at a single point in time
• People with cancer see significant changes in symptoms and disability over months
• People with COPD develop symptoms and disability over years
• Issues of choice about place and type of care in advanced COPD take place in a unique context
What evidence is there for a palliative care approach in COPD?
• Needs in advanced COPD are considerable and match those of people with cancer
• Patients with advanced COPD are likely to have arrived at that point gradually
• Prognosis in COPD is not accurate enough to be useful in the short term (<one year)
• There are no useful disease specific indicators which indicate COPD patients suitable for a palliative care register

What next?
• Assessment of unrelieved breathless due to COPD in primary care
• Prognosis in COPD using longitudinal data
• Develop a breathlessness service for people with advanced COPD
• Trial of the palliation of breathlessness in advanced COPD
End of life research in COPD
I have received speaker honoraria from AstraZeneca, Bohringer Ingelheim, Glaxo, Pfizer for speaking at scientific meetings.
Patrick WhiteKing’s College LondonDepartment of General Practice and
Primary Care.
Declaration of interest

















