CLINICAL STUDY Long-term Outcome of Percutaneous Interventions for Hepatic Venous Outflow Obstruction after Pediatric Living Donor Liver Transplantation: Experience from a Single Institute Minoru Yabuta, MD, Toshiya Shibata, MD, PhD, Toyomichi Shibata, MD, PhD, Ken Shinozuka, MD, Hiroyoshi Isoda, MD, PhD, Shinya Okamoto, MD, PhD, Shinji Uemoto, MD, PhD, and Kaori Togashi, MD, PhD ABSTRACT Purpose: To evaluate retrospectively the long-term outcome of percutaneous interventions for hepatic venous outflow obstruction (HVOO) occurring after pediatric living donor liver transplantation (LDLT). Materials and Methods: Between October 1997 and December 2012, 48 patients (24 boys, 24 girls; median age, 6 y) who had undergone LDLT were confirmed to have HVOO using percutaneous hepatic venography and manometry. All patients underwent percutaneous interventions, including balloon angioplasty with or without stent placement. Technical success, clinical success, patency rates, stent placement, and major complications were evaluated. Results: Technical success was achieved in 92 of 93 sessions (99.0%) and in 47 of 48 patients (97.9%), and clinical success was achieved in 41 of 48 patients (85.4%). During the follow-up period (range, 1–182 mo; median, 51.5 mo), 28 patients were treated with a single session of balloon angioplasty, and 20 patients who developed recurrent stenosis were treated with repeated percutaneous interventions. The rates of primary and primary-assisted patency at 1, 3, 5, and 10 years after balloon angioplasty were 64%, 57%, 57%, and 52% (primary patency) and 98%, 95%, 95%, and 95% (primary-assisted patency). Of six patients with stent placement, four had no recurrent HVOO after the stent placement, but two developed recurrent stenosis. The stent migrated to the right atrium in one patient. Conclusions: Percutaneous interventions were effective treatments for HVOO after LDLT. ABBREVIATIONS HVOO = hepatic venous outflow obstruction, LDLT = living donor liver transplantation Liver transplantation has been an effective treatment for end-stage liver disease. (1,2). More recent advances in surgical techniques and immunosuppression have led to improved outcomes after transplantation, but vascular complications are still important causes of graft failure (3,4). Hepatic venous outflow obstruction (HVOO) is a rare complication; the frequency of HVOO in orthotopic liver transplantation is reported to be approximately 1.5%–2.5% (5,6). Living donor liver transplantation has arisen as a means to address the continuing cadaveric donor shortage (2); however, the rate of HVOO in LDLT has been reported to 2%–9% (4,7–11), which is higher than the rate associated with orthotopic liver trans- plantation owing to the shorter vascular pedicle, smaller anastomosis diameters, and the potential for a size mismatch in children (12). Percutaneous interventions, including balloon angioplasty and stent placement, are accepted treatments in patients with HVOO because of the effectiveness and minimal invasiveness (12–16). Bal- loon angioplasty is the accepted first therapeutic option for HVOO (10,17), although there has been a report describing the effectiveness of primary stent placement for HVOO (18). The purpose of our study was to & SIR, 2013 J Vasc Interv Radiol 2013; 24:1673–1681 http://dx.doi.org/10.1016/j.jvir.2013.07.010 None of the authors have identified a conflict of interest. From the Departments of Diagnostic Imaging and Nuclear Medicine (M.Y., Tos.S., Toy.S., K.S., H.I., K.T.) and Surgery (S.O., S.U.), Kyoto University Graduate School of Medicine, 54-Kawaharacho, Shogoin, Sakyo-ku, Kyoto 606-8507, Japan. Received April 22, 2013; final revision received July 5, 2013; accepted July 8, 2013. Address correspondence to Tos.S.; E-mail: ksj@kuhp. kyoto-u.ac.jp
Transcript
CLINICAL STUDY
Long-term Outcome of Percutaneous Interventionsfor Hepatic Venous Outflow Obstruction afterPediatric Living Donor Liver Transplantation:
Shinji Uemoto, MD, PhD, and Kaori Togashi, MD, PhD
ABSTRACT
Purpose: To evaluate retrospectively the long-term outcome of percutaneous interventions for hepatic venous outflowobstruction (HVOO) occurring after pediatric living donor liver transplantation (LDLT).
Materials and Methods: Between October 1997 and December 2012, 48 patients (24 boys, 24 girls; median age, 6 y) who hadundergone LDLT were confirmed to have HVOO using percutaneous hepatic venography and manometry. All patientsunderwent percutaneous interventions, including balloon angioplasty with or without stent placement. Technical success, clinicalsuccess, patency rates, stent placement, and major complications were evaluated.
Results: Technical success was achieved in 92 of 93 sessions (99.0%) and in 47 of 48 patients (97.9%), and clinical success wasachieved in 41 of 48 patients (85.4%). During the follow-up period (range, 1–182 mo; median, 51.5 mo), 28 patients were treatedwith a single session of balloon angioplasty, and 20 patients who developed recurrent stenosis were treated with repeatedpercutaneous interventions. The rates of primary and primary-assisted patency at 1, 3, 5, and 10 years after balloon angioplastywere 64%, 57%, 57%, and 52% (primary patency) and 98%, 95%, 95%, and 95% (primary-assisted patency). Of six patients withstent placement, four had no recurrent HVOO after the stent placement, but two developed recurrent stenosis. The stentmigrated to the right atrium in one patient.
Conclusions: Percutaneous interventions were effective treatments for HVOO after LDLT.
Liver transplantation has been an effective treatment forend-stage liver disease. (1,2). More recent advances insurgical techniques and immunosuppression have led toimproved outcomes after transplantation, but vascularcomplications are still important causes of graft failure(3,4). Hepatic venous outflow obstruction (HVOO) is a
& SIR, 2013
J Vasc Interv Radiol 2013; 24:1673–1681
http://dx.doi.org/10.1016/j.jvir.2013.07.010
None of the authors have identified a conflict of interest.
From the Departments of Diagnostic Imaging and Nuclear Medicine (M.Y.,Tos.S., Toy.S., K.S., H.I., K.T.) and Surgery (S.O., S.U.), Kyoto UniversityGraduate School of Medicine, 54-Kawaharacho, Shogoin, Sakyo-ku, Kyoto606-8507, Japan. Received April 22, 2013; final revision received July 5, 2013;accepted July 8, 2013. Address correspondence to Tos.S.; E-mail: [email protected]
rare complication; the frequency of HVOO in orthotopicliver transplantation is reported to be approximately1.5%–2.5% (5,6). Living donor liver transplantation hasarisen as a means to address the continuing cadavericdonor shortage (2); however, the rate of HVOO in LDLThas been reported to 2%–9% (4,7–11), which is higherthan the rate associated with orthotopic liver trans-plantation owing to the shorter vascular pedicle, smalleranastomosis diameters, and the potential for a sizemismatch in children (12). Percutaneous interventions,including balloon angioplasty and stent placement, areaccepted treatments in patients with HVOO because ofthe effectiveness and minimal invasiveness (12–16). Bal-loon angioplasty is the accepted first therapeutic optionfor HVOO (10,17), although there has been a reportdescribing the effectiveness of primary stent placementfor HVOO (18). The purpose of our study was to
Yabuta et al ’ JVIR1674 ’ Outcome of Percutaneous Interventions after Pediatric LDLT
evaluate retrospectively the long-term outcome of percu-taneous interventions for HVOO after LDLT in pediatricpatients in a single institute.
Sex
Male 24
Female 24
Age at initial percutaneous intervention
Range 2 mo–20 y
Median 6 y
Mode of transplantation
Lateral segment 31
Left lobe 16
Right lobe 1
Original disease
Biliary atresia 38
Fulminant hepatitis 2
Wilson disease 2
Alagille syndrome 1
Citrullinemia 1
Fulminant hepatic failure 1
Liver cirrhosis 1
Ornithine transcarbamylase deficiency 1
Primary sclerosing cholangitis 1
MATERIALS AND METHODS
The Human Subjects Research Review Board at ourinstitution approved our protocol and retrospective study.Informed consent for the retrospective study was notrequired. Informed consent regarding venography andinterventional procedures was obtained from patients orthe patient’s parents.
PatientsBetween October 1997 and December 2012, LDLT wasperformed in the Department of Surgery at Kyoto Uni-versity in 512 pediatric patients (age o 18 y). Of the 512patients, 68 patients were suspected to have HVOO duringpostoperative follow-up and underwent venography andmanometry. HVOO was clinically suspected based on thefollowing findings: (i) clinical symptoms, including ascites,pleural effusion, and hepatomegaly; (ii) Doppler ultra-sound findings, including the disappearance of pulsatilehepatic venous flow, flattening of the hepatic venous wave,or weak Doppler-detectable blood flow (o 10 cm/s); and(iii) liver biopsy findings of congestion, hemorrhage, andnecrosis around the central veins. Using venography andmanometry, 48 of the 68 patients were confirmed to haveHVOO. Inclusion criteria for HVOO were (i) 4 50%stenosis (diameter of stenosis/diameter of a hepatic vein onthe distal side) or (ii) 4 5 mm Hg pressure gradient acrossthe stenosis between the distal hepatic vein and theright atrium (9,12). Characteristics of the 48 patients areshown in Table 1. We included 16 pediatric patientsfrom our previous study (14). All 48 patients underwentpercutaneous interventions, including balloon angioplastywith or without stent placement. The age of the patientsranged from 2 months to 20 years (median, 6 y) at the firstintervention. The interval between the liver trans-plantation and the first percutaneous intervention was1–220 months (median, 18 mo). One patient underwentthe first percutaneous intervention in the acute period, 1month after LDLT; 5 patients received intervention in thesubacute period, 1–3 months after LDLT; and the remain-ing 42 patients received intervention 4–220 months afterLDLT.
ProceduresFour authors (M.Y., Tos.S., K.S., and Toy.S.) with 5, 29,5, and 17 years of experience in interventional radiologyperformed the procedures. Percutaneous interventionswere performed with general anesthesia in 32 patientsand with local anesthesia in 16 patients. The approachto the hepatic vein was transhepatic in 35 patientsand transjugular in 13 patients; we adopted a transju-gular approach in patients with ascites, patients with
coagulopathy, and patients o 3 years old. Balloonangioplasty was performed after venography and man-ometry with a 7.0-F percutaneous transluminal angio-plasty catheter (POWERFLEX Plus; Cordis, Warren,New Jersey) with a balloon diameter of 6–10 mm and alength of 40 mm. The diameter of the balloon was thesame as the vein on the hepatic side of the stenosis. Theballoon was inflated three times for 60 seconds with anatmospheric pressure of 10 atm. Venography and man-ometry were repeated to evaluate the effectiveness of theballoon angioplasty. Hemostasis was accomplished withmanual compression after sheath removal in patientstreated with the transhepatic approach without subse-quent embolization of the transhepatic tract.In contrast to patients treated with the transhepatic
approach, patients treated with the transjugularapproach were heparinized with 50 IU/kg heparin(Ajinomoto, Tokyo, Japan) intravenously. Heparin wasused for 2–3 days after the procedure as a transition towarfarin (Eisai, Tokyo, Japan). Warfarin administrationbegan the day after the procedure and was usuallycontinued for 4 6 months to maintain internationalnormalized ratio at 1.5–2.0.
Follow-up EvaluationLaboratory data and Doppler ultrasound were evaluatedbimonthly on an outpatient basis, and venography andmanometry were performed when recurrent HVOO wassuspected. Our current strategy for treatment of HVOOis shown in Figure 1. Stent placement was recommendedin patients who developed recurrent HVOO at the thirdintervention. We used self-expanding metallic stents,
Figure 1. Schema of our strategy for HVOO treatment.
Volume 24 ’ Number 11 ’ November ’ 2013 1675
including ZA stents (Cook, Inc, Bloomington, Indiana),S.M.A.R.T. stents (Cordis), and E-LUMINEXX stent(Bard Peripheral Vascular, Tempe, Arizona), with a dia-meter 20%–30% larger than the hepatic vein proximalto the stenosis and with sufficient length to cover thestricture. Early in our study, a few patients were treatedwith repeated multiple sessions of balloon angioplastybecause stent placement was not recommended in ourhospital at that time. Two authors (M.Y., Tos.S.)reviewed the patient’s medical records retrospectivelyand evaluated technical success, clinical success, patencyrate, stent placement, and major complications.
DefinitionsTechnical success was defined as successful completion ofpercutaneous interventions with o 20% stenosis at post-operative venography or o 3 mm Hg pressure gradientacross the stenosis at postoperative manometry. Clinicalsuccess was defined as resolution or marked improvement
of clinical symptoms, including ascites, Doppler ultrasoundfindings, or laboratory findings. Abnormal Doppler ultra-sound findings were defined as a disappearance of pulsatilehepatic venous flow, flattening of the hepatic venous wave,or weak Doppler-detectable blood flow (o 10 cm/s) (19).We also evaluated the serum levels of aspartate amino-transferase, alanine aminotransferase, total bilirubin, andalbumin. For patients presenting with marked ascites,abnormal Doppler ultrasound findings, and abnormallaboratory data, clinical success was verified using clinicalrecords and laboratory data describing marked improve-ment between just before the first balloon dilation and atthe end of the follow-up period. We evaluated primary pat-ency and primary-assisted patency rates. Primary patencywas defined as the interval between the initial balloonangioplasty and recurrent HVOO necessitating percutane-ous intervention. Primary-assisted patency was defined aspatency after the initial angioplasty until treatment withrepeated percutaneous interventions was abandoned. Theobservational endpoints were the end of the follow-up
Yabuta et al ’ JVIR1676 ’ Outcome of Percutaneous Interventions after Pediatric LDLT
period in our study and the patient’s death. We alsoevaluated nonresponders, defined as patients necessitatingmore than two sessions of percutaneous interventions, interms of presence or absence of kinks, longer lesions, andthe onset of HVOO. The timing of stent placement,additional interventions after stent placement, and thepatency of the stent also were evaluated. Complicationsrelated to the procedures were divided into major andminor categories according to Society of InterventionalRadiology (SIR) criteria (20). Major complications werealso evaluated.
Statistical AnalysesStatistical analyses of clinical success and the differencein the onset of HVOO between responders and non-responders were performed using the Wilcoxon test andMann-Whitney U test, respectively. P values o .05 wereconsidered statistically significant. Statistical analysis ofthe patency rate was performed using the Kaplan-Meiermethod. Data processing and analysis were performedusing software (SPSS for Windows version 21.0; SPSS,Chicago, Illinois).
RESULTS
Technical SuccessA total of 93 interventions were attempted in all 48patients with HVOO; 92 interventional sessions weresuccessfully performed, but stent migration into the rightatrium occurred in one patient. Technical success wasachieved in 92 of 93 sessions (99.0%) and in 47 of 48patients (97.9%).
Clinical SuccessClinical success was achieved in 41 of 48 patients (85.4%).Of the 38 patients presenting with marked ascites,resolution or marked improvement was observed in allpatients. The Doppler ultrasound findings normalized
Table 2 . Number of Interventional Sessions
Session
1 Session of BA
2 Sessions of intervention
2 Sessions of BA
1 Session of BA and 1 session for stent placement
3 Sessions of intervention
3 Sessions of BA
2 Sessions of BA and 1 session for stent placement
4 Sessions of BA
4 5 Sessions of intervention
7 Sessions of BA and 3 sessions for stent placement
9 Sessions of BA and 2 sessions for stent placement
Total 93 sessions in 48 patients.
BA ¼ balloon angioplastynA patient who experienced stent migration was included.
in all 44 patients presenting with abnormal Dopplerultrasound findings. Decreased serum aspartate amino-transferase, alanine aminotransferase, or total bilirubin orincreased albumin levels were observed in 24 of 31 patientspresenting with abnormal laboratory values. In these24 patients, the mean levels of serum aspartate amino-transferase were 43.6 U/L � 28.9 before the pro-cedure and 40.2 U/L � 22.7 at the end of the follow-upperiod (P ¼ .55). The mean levels of serum alanine amino-transferase were 37.7 U/L � 24.9 before the procedureand 29.1 U/L � 14.1 at the end of the follow-up period(P ¼ .83). The mean levels of serum total bilirubin were1.43 mg/dL � 1.88 before the procedure and 0.94 mg/dL� 0.67 at the end of the follow-up period (P ¼ .17). Themean levels of albumin were 3.46 g/dL � 0.82 before theprocedure and 3.74 g/dL � 0.62 at the end of the follow-up period (P ¼ .095). None of the differences were stati-stically significant.
Patency RateFollow-up periods in the 48 patients ranged from 1–182months (median, 51.5 mo). The outcomes are shown inTable 2 and Figure 2. Of patients, 28 were treated withsingle balloon angioplasty (Fig 3) and did not developrecurrent stenosis. In 11 patients, two sessions of percu-taneous interventions were performed. Two patientsunderwent more than five sessions of percutaneous inter-ventions, including stent placement. One patient, whounderwent seven sessions of balloon angioplasty and threesessions of stent placement, showed no recurrent HVOO.Another patient underwent nine sessions of balloon angio-plasty and two sessions of stent placement; however, thehepatic vein was thrombosed after the last balloonangioplasty, and retransplantation was performed.There were 10 nonresponders and 38 responders; no
kinks and longer lesions were seen in the 10 non-responders. A significant difference in the onset of theinitial HVOO was seen between the nonresponders (12.1
No. Patients
28
11
10
1
6
2
4*
1
2
1
1
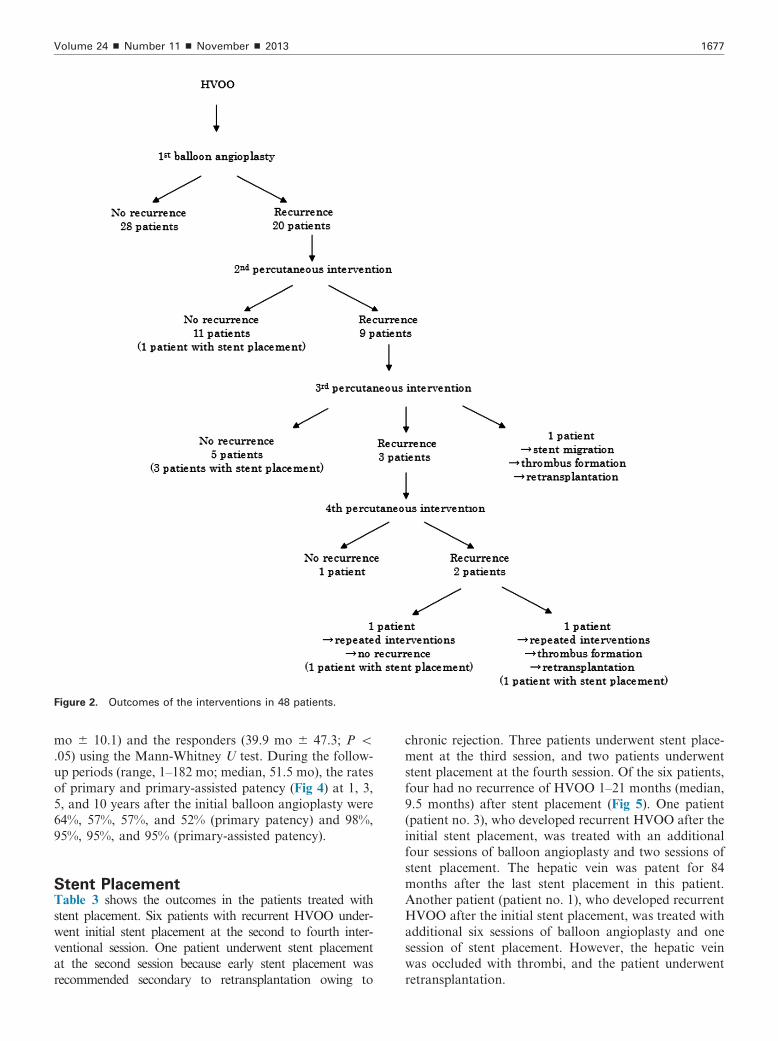
Figure 2. Outcomes of the interventions in 48 patients.
Volume 24 ’ Number 11 ’ November ’ 2013 1677
mo � 10.1) and the responders (39.9 mo � 47.3; P o.05) using the Mann-Whitney U test. During the follow-up periods (range, 1–182 mo; median, 51.5 mo), the ratesof primary and primary-assisted patency (Fig 4) at 1, 3,5, and 10 years after the initial balloon angioplasty were64%, 57%, 57%, and 52% (primary patency) and 98%,95%, 95%, and 95% (primary-assisted patency).
Stent PlacementTable 3 shows the outcomes in the patients treated withstent placement. Six patients with recurrent HVOO under-went initial stent placement at the second to fourth inter-ventional session. One patient underwent stent placementat the second session because early stent placement wasrecommended secondary to retransplantation owing to
chronic rejection. Three patients underwent stent place-ment at the third session, and two patients underwentstent placement at the fourth session. Of the six patients,four had no recurrence of HVOO 1–21 months (median,9.5 months) after stent placement (Fig 5). One patient(patient no. 3), who developed recurrent HVOO after theinitial stent placement, was treated with an additionalfour sessions of balloon angioplasty and two sessions ofstent placement. The hepatic vein was patent for 84months after the last stent placement in this patient.Another patient (patient no. 1), who developed recurrentHVOO after the initial stent placement, was treated withadditional six sessions of balloon angioplasty and onesession of stent placement. However, the hepatic veinwas occluded with thrombi, and the patient underwentretransplantation.
Figure 3. A 4-year-old girl with citrullinemia underwent left lobe LDLT. HVOO was suspected 3 months after LDLT, and venography
and manometry were performed. (a) Hepatic venogram obtained before treatment showed an anastomotic stricture between the left
hepatic vein and the inferior vena cava. The pressure gradient across the stenosis between the distal hepatic vein and the right atrium
was 17 mm Hg. (b) Fluoroscopic view during balloon angioplasty showed full expansion of the balloon. (c) Hepatic venogram obtained
after balloon angioplasty showed improved blood flow into the right atrium. The pressure gradient decreased to 2 mm Hg. HVOO did
not recur after balloon angioplasty.
Figure 4. Primary patency and primary-assisted patency rates.
Kaplan-Meier curve shows primary patency rate and primary-
assisted patency. Solid and dotted lines indicate primary
patency and primary-assisted patency, respectively. Vertical
lines on both lines indicate censored observations. The primary
patency and primary-assisted patency rates at 1, 3, 5, and 10
years after the first balloon angioplasty were 64%, 57%, 57%,
and 52% (primary patency) and 98%, 95%, 95%, and 95%
(primary-assisted patency).
Yabuta et al ’ JVIR1678 ’ Outcome of Percutaneous Interventions after Pediatric LDLT
Major ComplicationsThere was one major complication in a session of a5-year-old boy with recurrent HVOO. At the thirdintervention, he underwent balloon dilation followed bystent placement using the transhepatic approach and aS.M.A.R.T. stent 4 cm in length and 10 mm in diameter.After the stent was deployed, it shifted 1 cm toward the
right atrium. We attempted placement of a second stentto cover the first and inserted a catheter with the stent.However, the first stent migrated into the right atrium.Although we attempted to retrieve it with an AmplatzGooseNeck Snare (ev3 Endovascular, Inc, Plymouth,Minnesota), we were unsuccessful, and a median sternot-omy was performed surgically. The stent, which was lod-ged in the chordae tendineae cordis of the tricuspid valve,was removed via a right atrial incision. The hepatic veinwas thrombosed 1 month after the surgical procedure,and retransplantation was performed. The patientshowed no recurrent HVOO 19 months after retrans-plantation.
DISCUSSION
Without appropriate treatment for HVOO, hepaticcongestion, massive ascites, portal hypertension, andfinally liver cirrhosis and graft failure may occur. Itis important to diagnose and treat HVOO early basedon clinical symptoms, laboratory data, and Dopplerultrasound.Several reports have described the effectiveness of
balloon angioplasty for HVOO, and it has been acceptedas a first-line treatment for HVOO (14–16). Kubo et al(14) described the midterm outcomes of percutaneousinterventions in 20 patients who developed HVOO afterLDLT. In their study, 19 of 20 patients with HVOOwere treated with balloon angioplasty alone, and onewas treated with balloon angioplasty and stent place-ment. After the initial balloon angioplasty, 11 patientsshowed no recurrent HVOO, and the primary patency
Table 3 . Summary of Percutaneous Interventions in Patients Who underwent Stent Placement
Patient No. Total Procedures Procedure Description Result
4 3 Procedure 1–2: balloon angioplasty No recurrence
Procedure 3: stent placement
5 3 Procedure 1–2: balloon angioplasty No recurrence
Procedure 3: stent placement
6 3 Procedure 1–2: balloon angioplasty No recurrence
Procedure 3: stent placement
Figure 5. A 1-year-old girl with biliary atresia had undergone left lobe LDLT and two sessions of balloon angioplasty for HVOO.
Because recurrent HVOO was suspected owing to ascites, venography and manometry were performed. (a) A hepatic venogram
obtained before treatment showed a severe anastomotic stricture between the left hepatic vein and the inferior vena cava. The pressure
gradient across the stenosis between the distal hepatic vein and the right atrium was 14 mm Hg. (b) The fluoroscopic view during
balloon angioplasty before stent placement showed the notch of the balloon at the site of the anastomotic stricture. (c) A hepatic
venogram obtained after stent placement showed improved blood flow into the right atrium. The pressure gradient decreased to 2 mm
Hg, and HVOO did not recur after stent placement.
Volume 24 ’ Number 11 ’ November ’ 2013 1679
rates at 3, 6, 12, and 60 months after balloon angioplastywere 80%, 65%, 60%, and 60%. Ikeda et al (15) reportedthat 10 patients with HVOO after LDLT were treatedwith balloon angioplasty alone, and 5 of 10 patients hadno recurrent HVOO 5–73 months (median, 15 mo) afterthe first session of balloon angioplasty. The primarypatency rates at 1, 3, 6, 12, and 60 months after balloonangioplasty were 78%, 67%, 67%, 56%, and 56%. Lorenzet al (16) obtained a clinical success rate of 81% (13 of 16patients) in their study. The primary patency and primary-assisted patency rates at 3, 6, 12, 18, and 36 months after
first dilation were 72.7%, 60%, 55.6%, 50%, and 50%(primary patency) and 90.9%, 90%, 88.9%, 87.5%, and83.3% (primary-assisted patency). Our clinical success ratewas 85.4% (41 of 48 patients). We saw marked improve-ment of ascites and abnormal Doppler ultrasound findingsin all patients. Our results were comparable to the resultsof Lorenz et al (16), who reported that clinical failure wasrelated to the presence of comorbidities, such as rejection,hepatitis, and primary graft failure. Similar to theseauthors, we also found that improved laboratory datadid not always correlate with improvement of HVOO.
Yabuta et al ’ JVIR1680 ’ Outcome of Percutaneous Interventions after Pediatric LDLT
Although balloon angioplasty is effective for managingHVOO, stent placement is required in some patients withrecurrent HVOO refractory to balloon angioplasty (9,17).Ko et al (17) described 108 patients who developed early-onset HVOO after LDLT and who were treated withstent placement. The overall 1-, 3-, and 5-year primarypatency rates were 82.3% � 0.3, 75.0% � 0.4, and 72.4%� 0.5. The authors advocated primary stent placementfor early HVOO occurring early after transplantation, butwe believe that stent placement should be avoided inpediatric patients after LDLT if possible because of thepossibility of thrombosis, because the long-term patencyof metallic stents for decades is unknown, and because thesize of the graft hepatic vein may not match the size of theinserted stent when the patients grow. Ko et al (17)reported that among their 108 patients, only 3 patients o15 years of age underwent stent placement. In our study,28 patients treated with a single session of balloonangioplasty and 10 patients treated with two sessions ofballoon angioplasty showed no recurrent HVOO duringfollow-up. We believe that primary stent placement couldbe avoided for many pediatric patients with HVOObecause 79% (38 of 48) of our patients were successfullytreated with two sessions of balloon angioplasty alone.Stent placement maintains the patency of the hepatic
vein better than balloon angioplasty, and stent place-ment is needed in patients with HVOO refractory toballoon angioplasty. However, the appropriate timing ofstent placement for refractory HVOO after balloonangioplasty is unclear. Umehara et al (21) reportedthat stent placement should be considered in patientswith chronic rejection who are refractory to severalballoon angioplasties with early-onset or late-onsetHVOO. In our study, stent placement was performedat the third session of percutaneous intervention in threepatients, at the fourth session of percutaneous interven-tion in two patients, and at the second session ofpercutaneous intervention in one patient (Table 3).Three patients with stent placement at the third sessionof percutaneous intervention showed no recurrentHVOO, and additional percutaneous interventionswere not needed after the stent placement. One patientunderwent stent placement at the second session ofpercutaneous intervention because he had undergoneretransplantation owing to chronic rejection, and werecommended early stent placement. The patient did notdevelop recurrent HVOO after the stent placement. Twopatients who underwent stent placement at the fourthsession of percutaneous intervention developed recurrentHVOO and underwent additional interventions, in-cluding balloon angioplasty and stent placement. Atthe present time, we perform stent placement at the thirdpercutaneous intervention. Although our results suggestthat stent placement was effective in treating recurrentHVOO after repeated balloon angioplasty, there mightbe disadvantages. Stent migration occurs rarely, but it isa severe complication. Although stent migration may
occur secondary to incorrect selection of the appropriatestent size, it can also be very difficult sometimes to placethe stent safely between the hepatic vein and inferiorvena cava because of the discrepancy in the diameters ofthe vessels or because of respiratory motion (22). Also,metallic stents might reduce adequate surgical marginsof the hepatic veins at retransplantation.To prevent stent occlusion, drug-eluting stents have
been used clinically for coronary artery disease andperipheral artery disease (23,24). Although the long-term patency of these stents has not been established,they may be useful to prevent in-stent thrombosis inpatients with HVOO.Our study has some limitations, including the retro-
spective design. Also, early in our study, a defined treat-ment strategy for HVOO was not established. Because thenumber of patients in this study was small, a case-controldesign was not possible before and after the establishmentof our HVOO treatment strategy. Finally, the number ofpatients may have been too small to evaluate the compli-cations of the percutaneous interventions.In conclusion, balloon angioplasty was safe and
effective for HVOO occurring after LDLT. Stent place-ment might be needed in patients with recurrent HVOOrefractory to balloon angioplasty.
REFERENCES
1. Starzl TE, Demetris AJ, Van Thiel D. Liver transplantation (1). N Engl JMed 1989; 321:1014–1022.
2. Tanaka K, Uemoto S, Tokunaga Y, et al. Surgical techniques andinnovations in living related liver transplantation. Ann Surg 1993; 217:82–91.
3. Patkowski W, Nyckowski P, Zieniewicz K, et al. Biliary tract complica-tions following liver transplantation. Transplant Proc 2003; 35:2316–2317.
4. Buell JF, Funaki B, Cronin DC, et al. Long-term venous complicationsafter full-size and segmental pediatric liver transplantation. Ann Surg2002; 236:658–666.
5. Navarro F, Le Moine MC, Fabre JM, et al. Specific vascular complica-tions of orthotropic transplantation with preservation of the retrohepaticvena cava: review of 1361 cases. Transplantation 1999; 68:646–650.
6. Parrilla P, Sanchez-Bueno F, Figueras J, et al. Analysis of the compli-cations of the piggy-back technique in 1,112 liver transplants. Trans-plantation 1999; 67:1214–1217.
8. Chen HL, Concejero AM, Huang TL, et al. Diagnosis and interventionalradiological treatment of vascular and biliary complications after livertransplantation in children with biliary atresia. Transplant Proc 2008; 40:2534–2536.
9. Ko GY, Sung KB, Yoon HK, et al. Endovascular treatment of hepaticvenous outflow obstruction after living-donor liver transplantation. J VascInterv Radiol 2002; 13:591–599.
10. Egawa H, Inomata Y, Uemoto S, et al. Hepatic vein reconstruction in 152living-related donor liver transplantation patients. Surgery 1997; 121:250–257.
11. Broelsch CE, Emond JC, Whitington PF, Thistlethwaite JR, Backer AL,Lichtor JL. Application of reduced-size liver transplants as split grafts,auxiliary orthotopic grafts, and living related segmental transplants. AnnSurg 1990; 212:368–375.
12. Carnevale FC, Machado AT, Moreira AM, et al. Midterm and long-termresults of percutaneous endovascular treatment of venous outflowobstruction after pediatric liver transplantation. J Vasc Interv Radiol2008; 19:1439–1448.
13. Akun E, Yaprak O, Killi R, Balci NC, Tokat Y, Yuzer Y. Vascularcomplications in hepatic transplantation: single-center experience in 14years. Transplant Proc 2012; 44:1368–1372.
14. Kubo T, Shibata T, Itoh K, et al. Outcome of percutaneous transhepaticvenoplasty for hepatic outflow obstruction after living donor liver trans-plantation. Radiology 2006; 239:285–290.
15. Ikeda O, Tamura Y, Nakasone Y, et al. Percutaneous transluminalvenoplasty after venous pressure measurement in patients with hepaticvenous outflow obstruction after living donor liver transplantation. Jpn JRadiol 2010; 28:520–526.
16. Lorenz JM, Van Ha T, Funaki B, et al. Percutaneous treatment ofvenous outflow obstruction in pediatric liver transplants. J Vasc IntervRadiol 2006; 17:1753–1761.
17. Ko GY, Sung KB, Yoon HK, et al. Early posttransplant hepatic venousoutflow obstruction: long-term efficacy of primary stent placement. LiverTranspl 2008; 14:1505–1511.
18. Sakamoto S, Egawa H, Kanawaza H, et al. Hepatic venous outflowobstruction in pediatric living donor liver transplantation using left-sidedlobe grafts: Kyoto University Experience. Liver Transpl 2010; 16:1207–1214.
19. Hwang HJ, Kim KW, Jeong WK, et al. Hepatic outflow obstruction atmiddle hepatic vein tributaries or inferior right hepatic veins after livingdonor liver transplantation with modified right lobe graft: comparison
of CT and Doppler ultrasound. AJR Am J Roentgenol 2009; 193:745–751.
20. Omary RA, Bettmann MA, Cardella JF, et al. Quality improvementguidelines for the reporting and archiving of interventional radiologyprocedures. J Vasc Interv Radiol 2003; 14(Pt 2):S293–S295.
21. Umehara M, Narumi S, Sugai Y, et al. Hepatic venous outflowobstruction in living donor liver transplantation: balloon angioplasty orstent placement? Transplant Proc 2012; 44:769–771.
22. Dancy MD. Management of venous outflow complications after livertransplantation. Tech Vasc Interv Radiol 2007; 10:240–245.
23. Di Lorenzo E, Sauro R, Varricchio A, et al. Long-term outcome of drug-eluting stents compared with bare metal stents in ST-segment elevationmyocardial infarction: results of the paclitaxel- or sirolimus-eluting stentversus bare metal stent in Primary Angioplasty (PASEO) RandomizedTrial. Circulation 2009; 120:964–972.
24. Scheinert D, Katsanos K, Zeller T, et al. A prospective randomizedmulticenter comparison of balloon angioplasty and infrapopliteal stentingwith the sirolimus-eluting stent in patients with ischemic peripheralarterial disease: 1-year results from the ACHILLES trial. J Am Coll Cardiol2012; 60:2290–2295.