Page 1
Accepted Manuscript
Longitudinal Trends, Hemodynamic Profiles, and Prognostic Value of Abnormal LiverFunction Tests in Patients with Acute Decompensated Heart Failure: an Analysis ofthe ESCAPE Trial
Michael Scholfield , MD Matthew B. Schabath , PhD Maya Guglin , MD, PhD
PII: S1071-9164(14)00205-X
DOI: 10.1016/j.cardfail.2014.05.001
Reference: YJCAF 3297
To appear in: Journal of Cardiac Failure
Received Date: 24 October 2013
Revised Date: 6 May 2014
Accepted Date: 8 May 2014
Please cite this article as: Scholfield M, Schabath MB, Guglin M, Longitudinal Trends, HemodynamicProfiles, and Prognostic Value of Abnormal Liver Function Tests in Patients with Acute DecompensatedHeart Failure: an Analysis of the ESCAPE Trial, Journal of Cardiac Failure (2014), doi: 10.1016/j.cardfail.2014.05.001.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
Page 2
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Longitudinal Trends, Hemodynamic Profiles, and Prognostic Value of Abnormal Liver Function Tests in
Patients with Acute Decompensated Heart Failure: an Analysis of the ESCAPE Trial
Michael Scholfield, MD1*; Matthew B. Schabath, PhD
2; Maya Guglin, MD, PhD
1
1Department of Cardiology, University of South Florida, Tampa, FL;
2Department of Cancer Epidemiology, H.
Lee Moffitt Cancer Center and Research Institute, Tampa, FL
*Corresponding Author: Michael Scholfield, MD
University of South Florida
2 Tampa Circle, 5th
Floor Cardiology
Tampa, FL 33612
E-mail: [email protected]
813-361-7622
Fax: 813-259-0665
Running head: LFTs in Acutely Decompensated Heart Failure
Abstract Word Count: 230 words
Text Word Count: 6161 words
Tables and Figures: 4 Tables and 3 Figures
Key Words: Albumin, Bilirubin, Creatinine, MELD
Page 3
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
Introduction: This study analyzed liver function abnormalities in heart failure patients admitted with severe
acute decompensated heart failure (ADHF).
Methods: A post hoc analysis was conducted using data from the Evaluation Study of Congestive Heart Failure
and Pulmonary Artery Catheterization Effectiveness (ESCAPE). Liver function tests (LFTs) were measured at
seven time-points from baseline, discharge, and up to six months follow-up. Survival analyses were utilized to
assess the association between admission model of end-stage liver disease-excluding INR (MELD-XI) scores
and patient outcome.
Results: There was a high prevalence of abnormal baseline (admission) LFTs (albumin 23.8%, aspartate
transaminase 23.5%, alanine transaminase 23.8%, and total bilirubin 36.1%). The percentage of patients with
abnormal LFTs decreased significantly from baseline to six months follow-up. When mean hemodynamic
profiles were compared in patients with abnormal vs. normal LFTs, elevated total bilirubin was associated with
a significantly lower cardiac index (1.80 vs. 2.1; P<0.001) and higher central venous pressure (14.2 vs 12.0;
P=0.03). Multivariable analyses revealed that patients with elevated MELD-XI scores (≥ 16.8) had a 2-fold (HR
= 2.06; 95% CI 1.05 – 4.03) increased risk of death, re-hospitalization, or transplant after adjusting for baseline
LFTs, age, gender, race, BMI, diabetes, and systolic blood pressure.
Conclusions: Abnormal LFTs are common in the ADHF population and are a dynamic marker of an impaired
hemodynamic state. Elevated MELD-XI scores are associated with poor outcomes among patients admitted
with ADHF.
Page 4
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
Introduction
Most of what is understood about abnormal liver function tests (LFTs) in heart failure (HF) derives from the
stable chronic HF patient population (1, 2). Recent studies have analyzed abnormal LFTs in the acutely
decompensated heart failure (ADHF) patient population. Abnormalities in LFTs are common, occurring in
upwards to 70% of these patients, and show a vastly different distribution than those in stable HF (3, 4).
Presently little is known about longitudinal trends of LFTs in patients admitted with, and treated for ADHF.
Abnormal LFTs in HF patients occur from two hemodynamic states. A decreased cardiac output state
leading to impaired organ perfusion is associated with acute centrilobular hepatocellular damage, ischemic
hepatic injury, and necrosis. Additionally, elevated right atrial filling pressures may lead to congestive hepatic
injury and a pathologic finding described as “nutmeg liver”(5). There is growing evidence that individual
biochemical markers correlate with various hemodynamic states and the degree of hepatic injury depends on
the contribution from congestion verses poor perfusion. There is substantial variability between studies, and it
is still unclear if elevated liver enzymes in individuals with HF are surrogates of hemodynamics.
It is generally accepted that certain LFTs, namely total bilirubin, are strong independent predictors of
increased risk of death and poor outcomes (1, 2, 4). This parallels what we understand about hepatorenal
syndrome and renal dysfunction predicting multi-system involvement in HF. Multiple recent studies have
used the Model of End-stage Liver Dysfunction (MELD) scoring model, which combines markers of renal and
liver function to predict outcomes in HF patients and have found it to be a powerful predictive tool.
Traditionally, the MELD score is used in predicting mortality and morbidity in cirrhotic patients undergoing
surgery or liver transplant. Recently Kim et al. (6) applied MELD scoring to evaluate urgency for heart
transplant in ambulatory HF patients. A modified MELD score excluding INR calculated as: [MELD-XI = (5.11 *
Ln total bilirubin) + (11.76 * Ln creatinine) + 9.44], has been standardized owing to the large number patients
on anticoagulation, and is highly predictive in the HF population (7, 8). MELD-XI has been shown to predict the
Page 5
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
survival following left ventricular assist device implantation and is emerging as a highly predictive composite
score for multi-system dysfunction in heart failure (9).
The Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness
(ESCAPE) trial collected longitudinal LFTs from admission (baseline), discharge, and follow-up to six months
(10). Thus, utilizing data from the ESCAPE trial (10) the objective of this analysis was to: i) explore the
longitudinal changes of LFTs in patients treated for ADHF, ii) explore the effects of hemodynamic profile on
various LFTs, iii) explore the prognostic implications of MELD scoring on a broad HF population.
Page 6
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
Methods
Study Population
This study is a retrospective analysis of the publically available and de-identified limited access dataset from
the ESCAPE trial provided by the National Heart, Lung, and Blood Institute (NHLBI). According to NHLBI policy,
datasets from major clinical trials funded by NHLBI include the protocol and all collected variables with their
descriptions and definitions. Documentation for limited access datasets is comprehensive and sufficiently
clear to enable investigators who are not familiar with a specific dataset to use it.
The original study was a multicenter trial that compared therapy guided by pulmonary artery catheters
with therapy guided by clinical assessment in hospitalized patients with acute decompensated HF (10).
Patients were admitted for New York Heart Association (NYHA) class IV symptoms, had at least one prior
admission for exacerbation of HF within six months before randomization, and had left ventricular ejection
fraction (LVEF) < 30% by contrast ventriculography, radionuclide ventriculography, or quantitative
echocardiography within one year before randomization. For this paper, we analyzed the subset of patients
that had both total bilirubin and creatinine available at baseline (N = 346). However, not all patients had
complete LFT data for every time point.
Liver function tests
Liver function tests were recorded in both arms at admission, discharge, and follow-up of two weeks, one
month, two months, three months, and six months. For our analysis, patients without recorded baseline
creatinine or total bilirubin were excluded. The prevalence of patients with abnormal total bilirubin (Tbili),
aspartate transaminase (AST), alanine transaminase (ALT), albumin, and creatinine (Cr) were calculated from
admission with ADHF through the six-month follow up. The cut-offs for abnormal values were Tbili > 1.0
mg/dL, AST > 40 IU/L, ALT > 40 IU/L, serum albumin < 3.4 g/dL, and Cr > 1.3mg/dL.
Page 7
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
For patients randomized to the Swan-Ganz guided therapy arm, the following hemodynamic variables
were recorded and calculated: central venous pressure (CVP), pulmonary artery systolic, diastolic and mean
pressure, pulmonary capillary wedge pressure, systemic vascular resistance, mixed venous oxygen saturation,
arterial blood pressure, and cardiac index (CI). In this study we utilized CVP and CI values recorded at the time
of admission (decompensated heart failure). The Student’s t-test was utilized to determine if there are
significant differences in mean hemodynamic profiles (CVP and CI) by baseline LFT status (i.e., abnormal vs.
normal).
Statistical Analysis
The MELD-XI score was calculated using the following formula: (5.11* Ln total bilirubin) + (11.76 * Ln
creatinine) + 9.44]. Differences in baseline characteristics by MELD-XI score were compared using Pearson’s
chi-square for categorical variables, and Student’s t-test and Wilcoxon rank sum test for continuous variables.
A generalized estimating equation (GEE) was used to test for differences in LFT status (abnormal vs. normal)
from the baseline (admission) visit to the six-month visit. Student’s t-test was used to test for difference of
mean CVP and CI by LFT status (normal vs. abnormal). Kaplan-Meier survival curves and log-rank statistics
were utilized to assess admission (baseline) LFTs and MELD-XI score associated with a composite endpoint of
death, re-hospitalization, or heart transplant. Cox Proportional Hazard models were used to estimate risk of
the composite endpoint of death, re-hospitalization, or heart transplant for each of the baseline LFTs and
MELD-XI score. The LFTs were dichotomized by their respective abnormal cut-points as shown in Table 2 and
the MELD-XI was dichotomized at the median value. Baseline MELD-XI was categorized by the median value (<
11.4 vs. ≥ 11.4), tertiles (< 8.7 vs. ≥ 8.7 to < 13.9, vs. ≥ 13.9), quartiles (< 6.8 vs. ≥ 6.8 to < 11.4 vs. ≥ 11.4 to <
15.5 vs. ≥ 15.5),), and by using a classification and regression tree (CART) approach (< 16.8 vs. ≥ 16.8). CART is
a nonparametric data-mining tool that can segment data into meaningful subgroups and has been adapted for
failure time data using the Martingale Residuals of a Cox model to approximate chi-square values for all
Page 8
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
possible cut-points (http://econpapers.repec.org/software/bocbocode/s456776.htm). We applied the CART
approach to identify a potential novel cut-point that is not based on the distribution (i.e., median, tertiles, and
quartiles) of the MELD-XI score. All statistics was statistical analyses was performed using Stata/MP 12.1
(StataCorp LP, College Station, TX).
Page 9
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
Results
Study Population
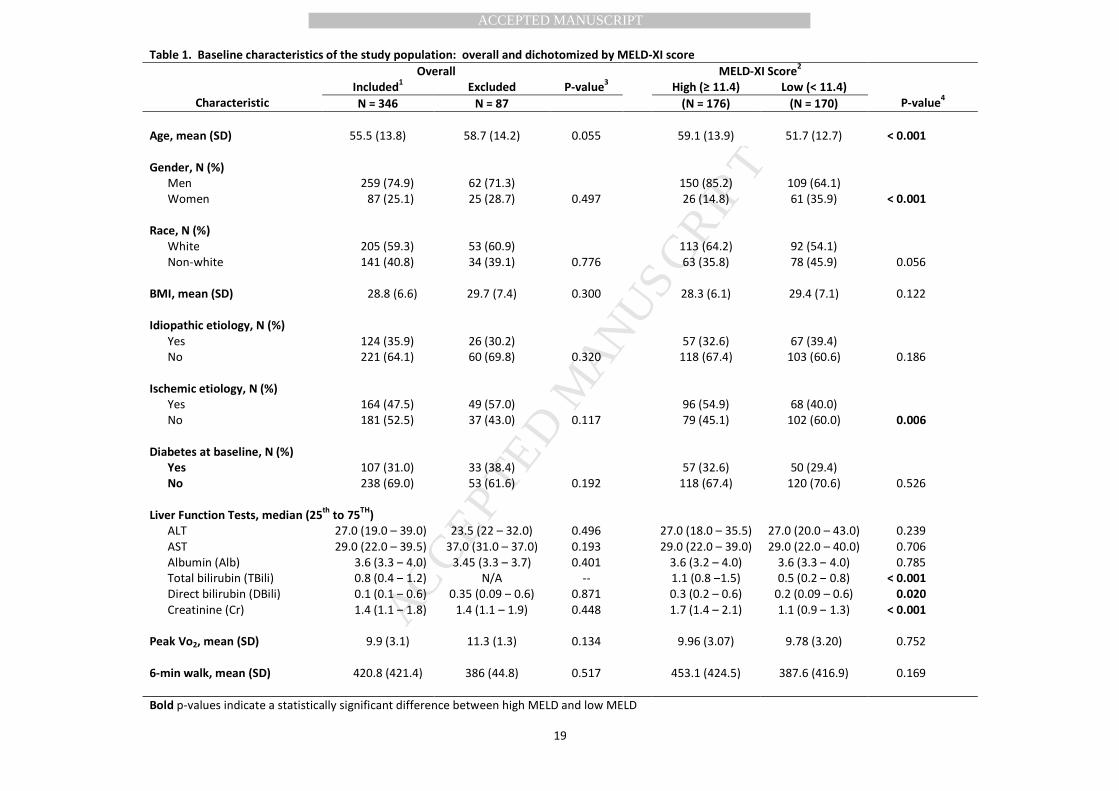
Among the 346 patients admitted with ADHF that had both total bilirubin and creatinine available at baseline,
75% were male, 59% were white, 47% had an ischemic cardiomyopathy and 31% has diabetes at baseline
(Table 1). When MELD score was dichotomized at the median value (11.4), we found statistically significant
differences for the baseline characteristics between high and low MELD-XI. Specifically, individuals with high
MELD (≥ 11.4) were older, and more likely to be male and to have an ischemic cardiomyopathy. Additionally,
total bilirubin, direct bilirubin, and creatinine were all significantly higher among invidious with high MELD
score.
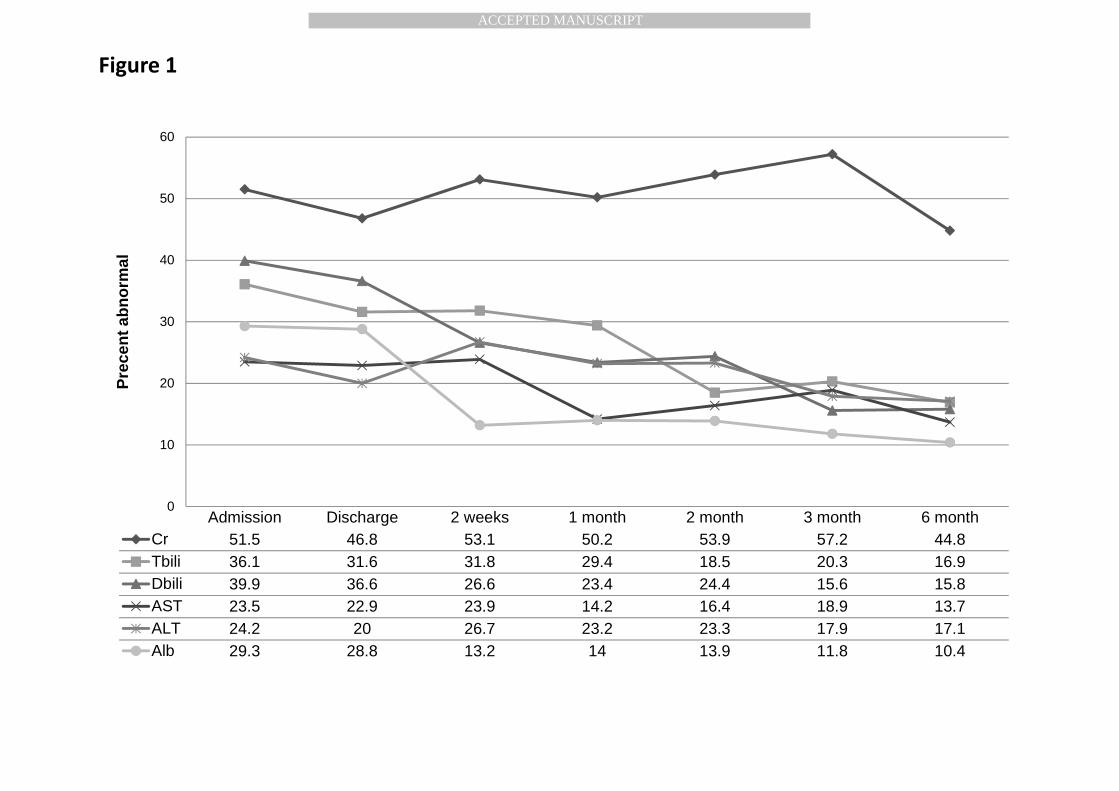
Longitudinal trends of LFTs
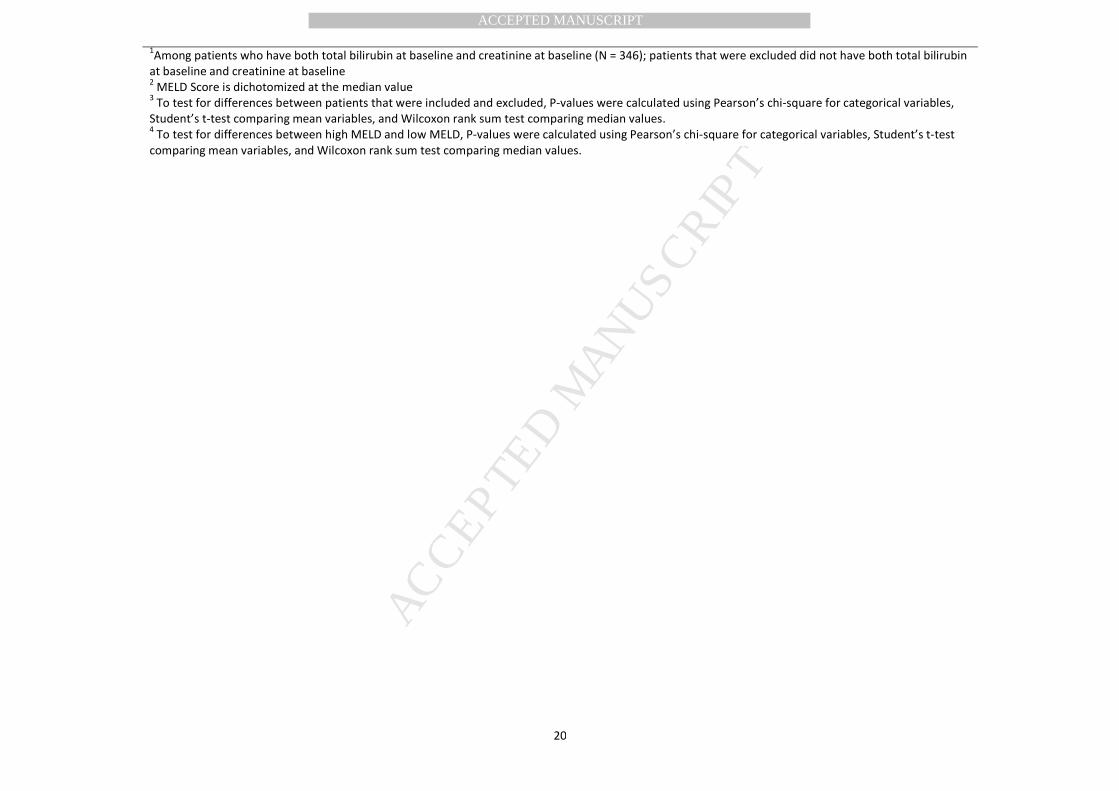
Overall, 312 patients (90%) had at least one abnormal LFT at baseline. The prevalence of individuals with an
abnormal LFT significantly decreased from baseline to six months for AST, ALT, albumin, total bilirubin, and
direct bilirubin, while there was no significant difference in the prevalence of abnormal creatinine (Table 2 and
Figure 1). LFTs appeared to be more labile than creatinine (Figure 1) from the decompensated state to stable
condition. The percentage of patients with elevated total bilirubin decreased from 36% on admission for ADHF
to 17% on a six-month follow-up, and percent of those with decreased albumin changed from 30% to 10% in
the same time frame, creatinine remained elevated in about half of the patients. In the end of the follow-up,
LFTs remained persistently elevated in 11 to 16% of patients while creatinine was increased in 45%, not
significantly different from the baseline (51.5%). The cohort was divided into patients that had morbidity or
mortality (cardiac re-hospitalization/transplant or death, respectively) in the follow up period, and the
prevalence of abnormal LFTs and creatinine was trended (data not included). In those patients that were re-
hospitalized or underwent transplant a similar trend was seen to that shown in figure 1. Whereas patients
that died in the follow up period did not show a significant trend.
Page 10
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
Hemodynamic profiles of cardiac hepatopathy
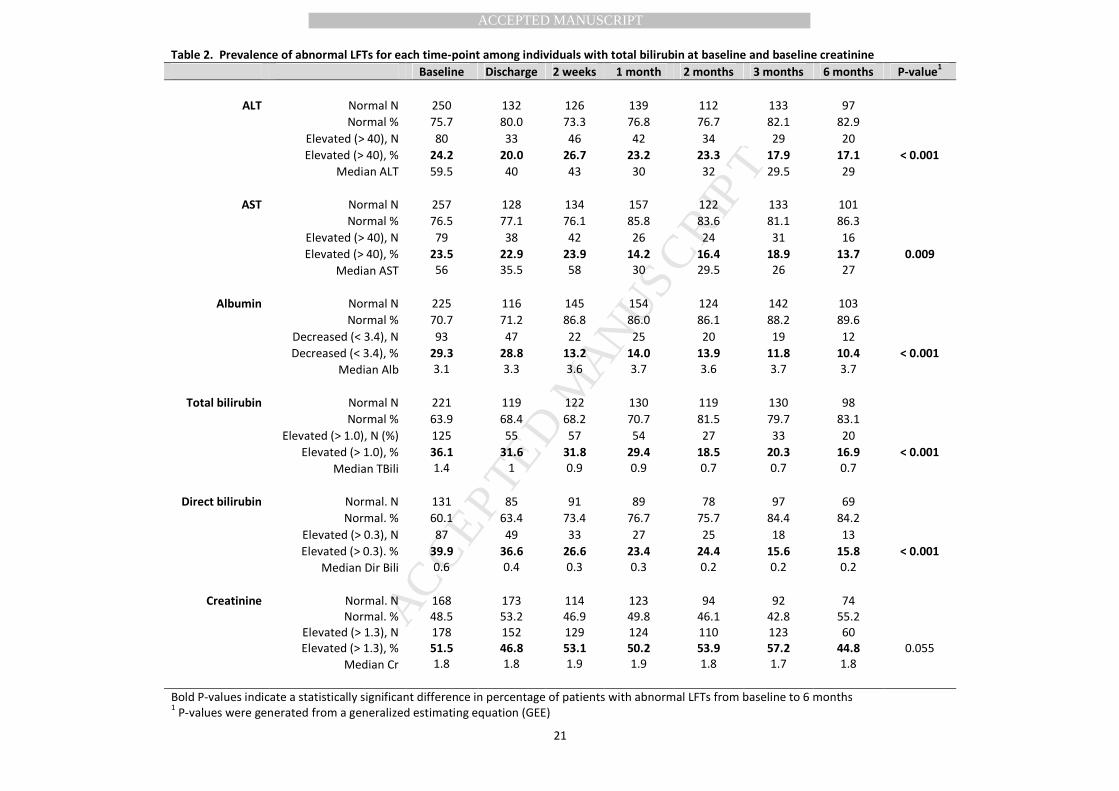
The hemodynamic profiles of patients randomized to the pulmonary arterial catheter arm with available LFTs
and Creatinine were analyzed to determine if there are significant differences in mean admission CVP and CI
comparing patients with abnormal vs. normal Creatinine, total bilirubin, albumin, AST and ALT (Table 3). CVP
was used as a surrogate for congestion, while CI reflected the output state. In patients with abnormal total
bilirubin, we found a significantly lower CI (1.8 vs. 2.1; P < 0.001) and higher CVP (14.2 vs. 12.0; P = 0.03) when
compared to patients with normal total bilirubin. Patients with elevated creatinine did not show significant
differences in mean CI or CVP when compared to patients with normal creatinine. Patients with elevated AST
had significantly higher CVP (15.4 vs. 12.2; P = 0.01) and a trend towards lower CI (Table 3). The levels of
albumin did not seem to be related to either hemodynamic profile.
Association of MELD-XI score and LFTs with a composite endpoint of death, cardiac re-hospitalization, and
heart transplant
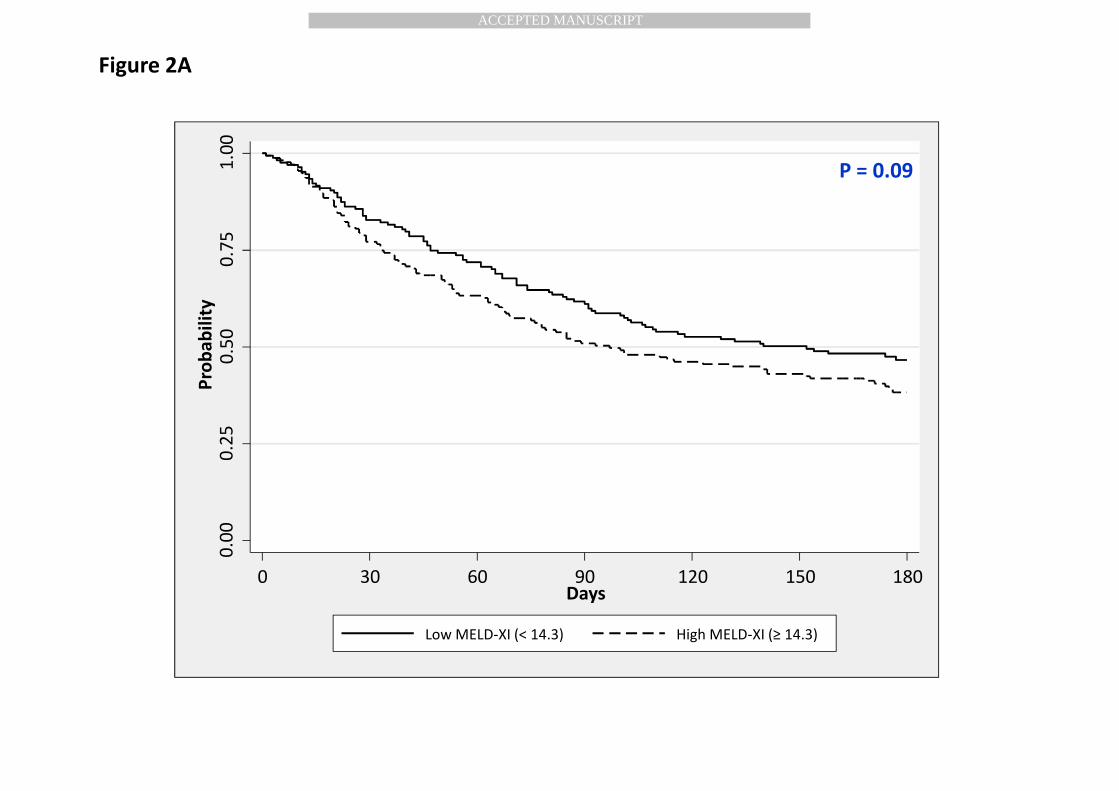
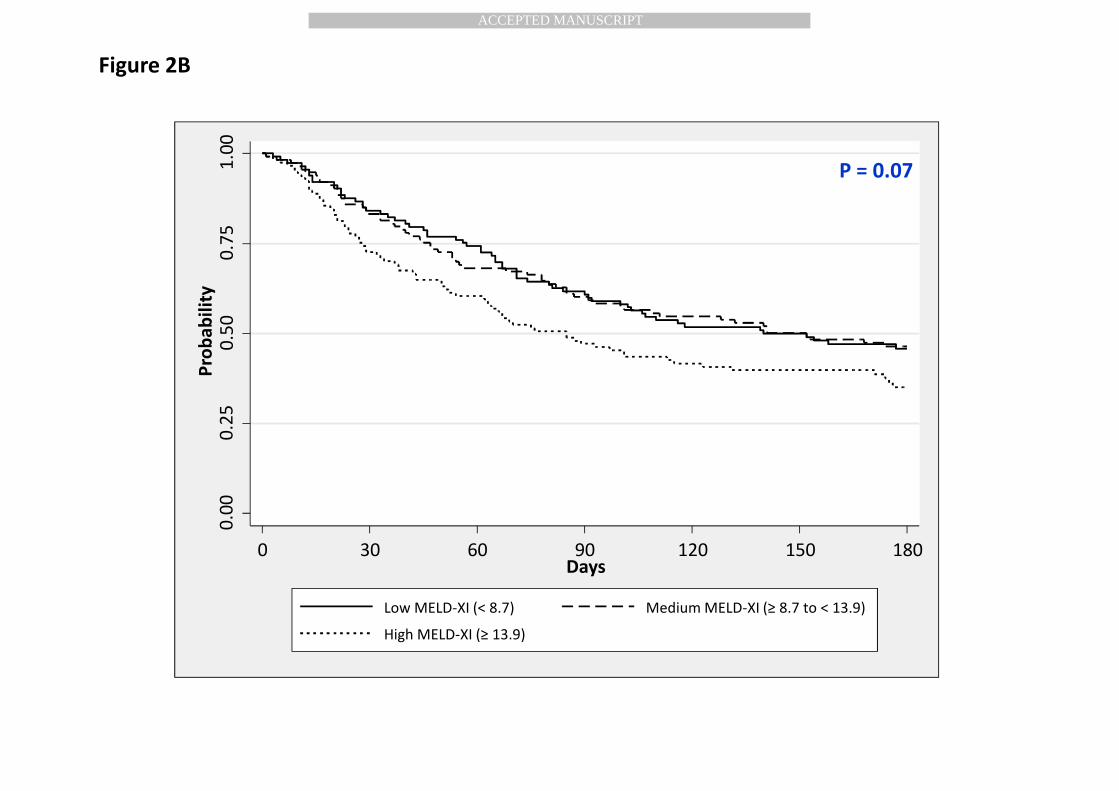
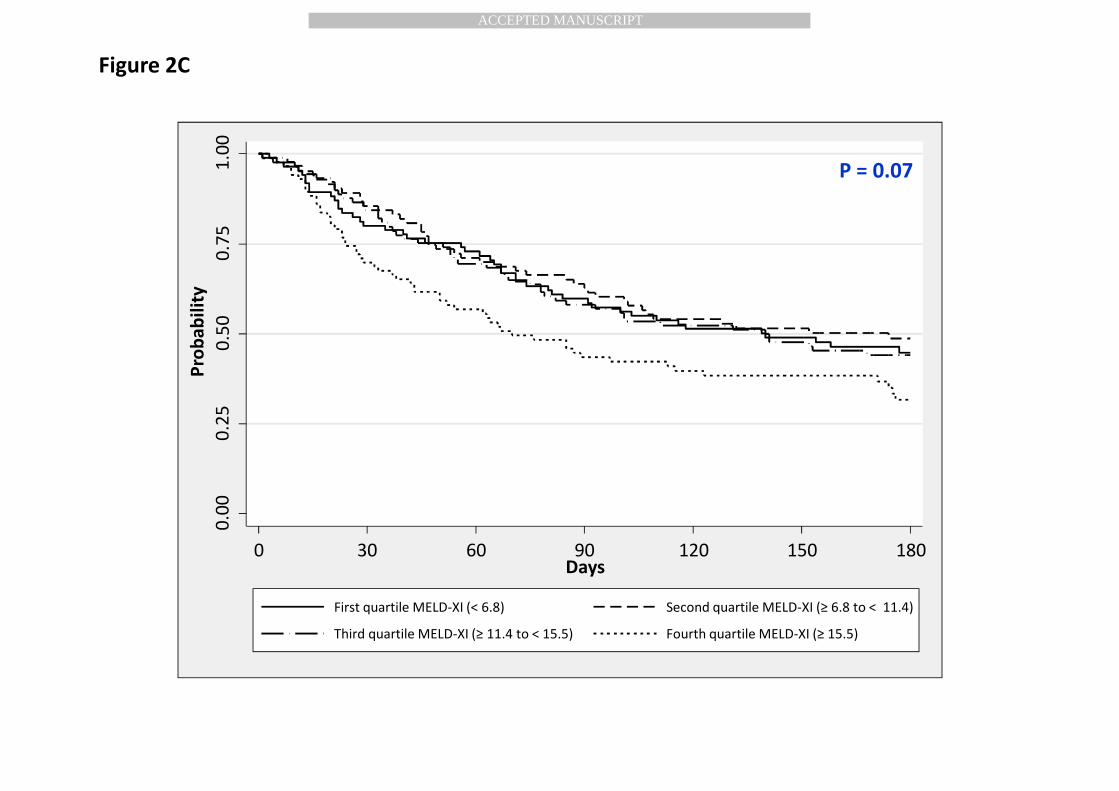
Of the 346 patients in this analysis of the ESCAPE cohort, 55.8% (N = 193) died, were re-hospitalized, or
underwent heart transplant in the six month follow-up period. When MELD-XI was categorized by percentile
cut-points (median, tertiles, and quartiles), the Kaplan-Meier survival curves (Figures 2A to 2C) revealed that
patients in the highest percentile categories (i.e., ≥ median, third tertile, and fourth quartile, respectively)
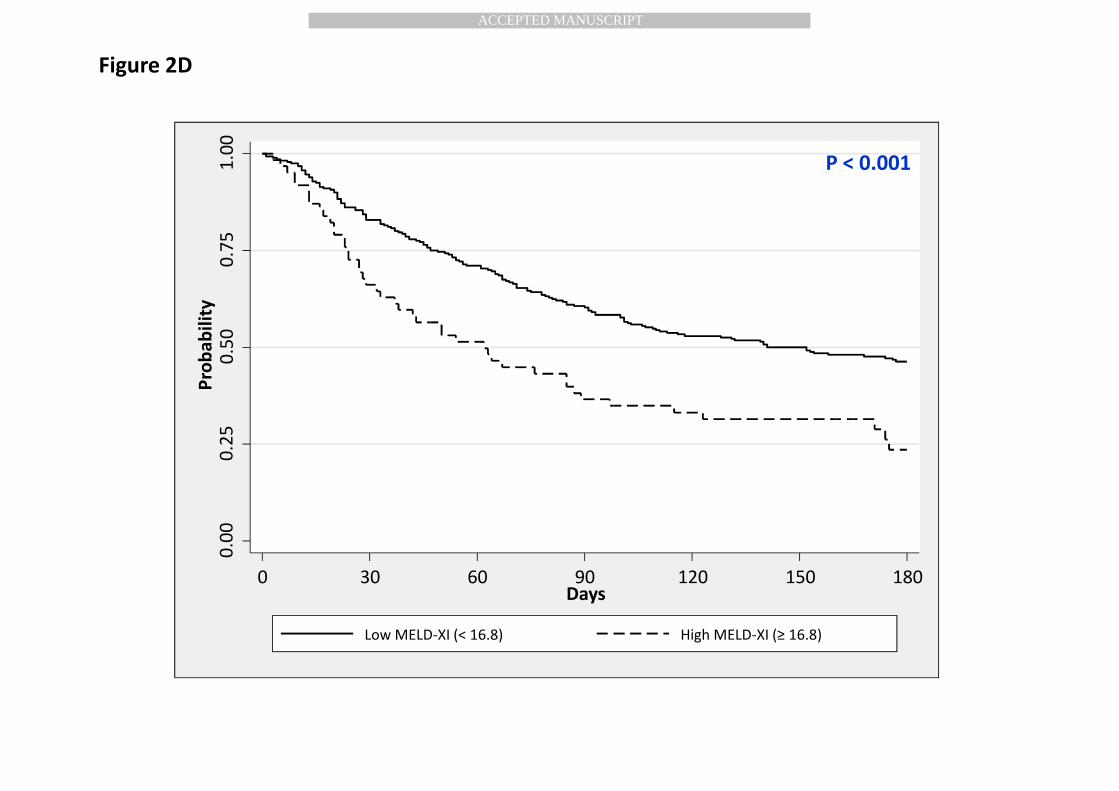
were associated with borderline significant poorer outcomes. When a CART approach was used to identify a
potential novel cut-point, we found that patients with a MELD-XI score ≥ 16.8 (observed in 18% of patients)
had a significantly poorer outcomes compared to patients with a MELD-XI < 16.8 (Figure 2D, P < 0.001). The 6-
month event-free survival was 23.5% for patients in the high MELD-XI score group (≥ 16.8) compared to 46.2%
for patient in the low MELD-XI score group (< 16.8). Because the MELD-XI score is comprised of total bilirubin
and creatinine, we also assessed whether they were associated with the composite end point. We found that
Page 11
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
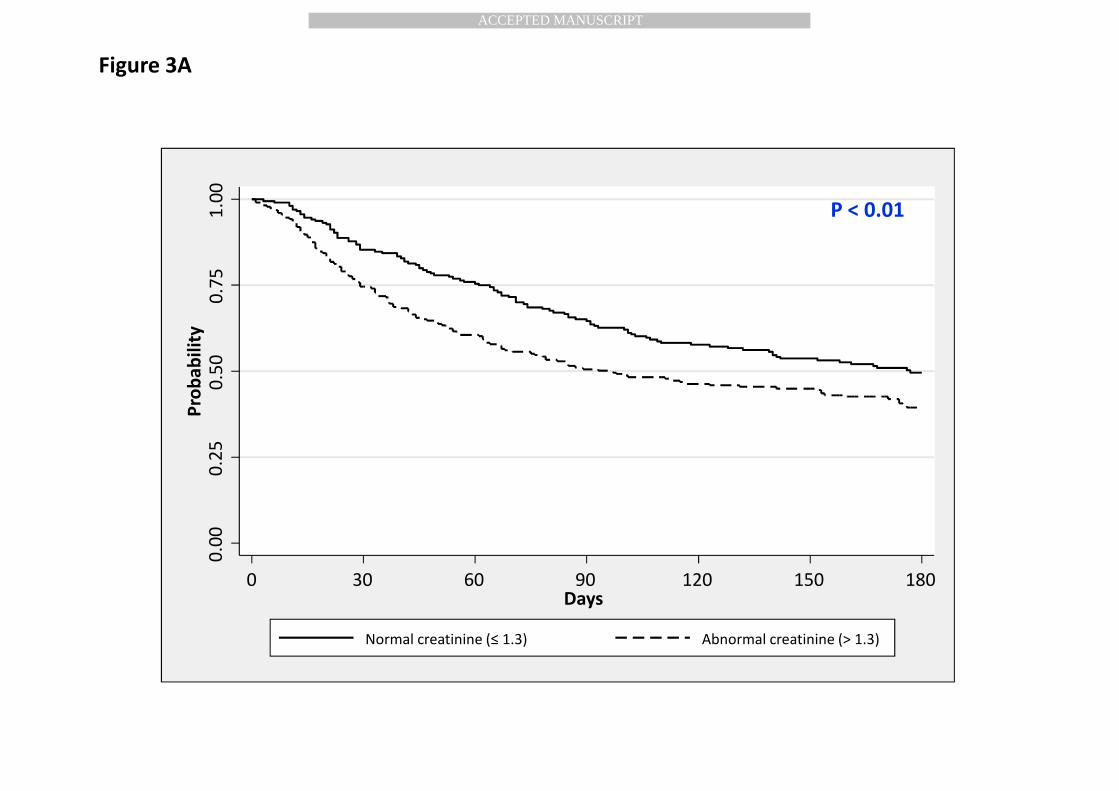
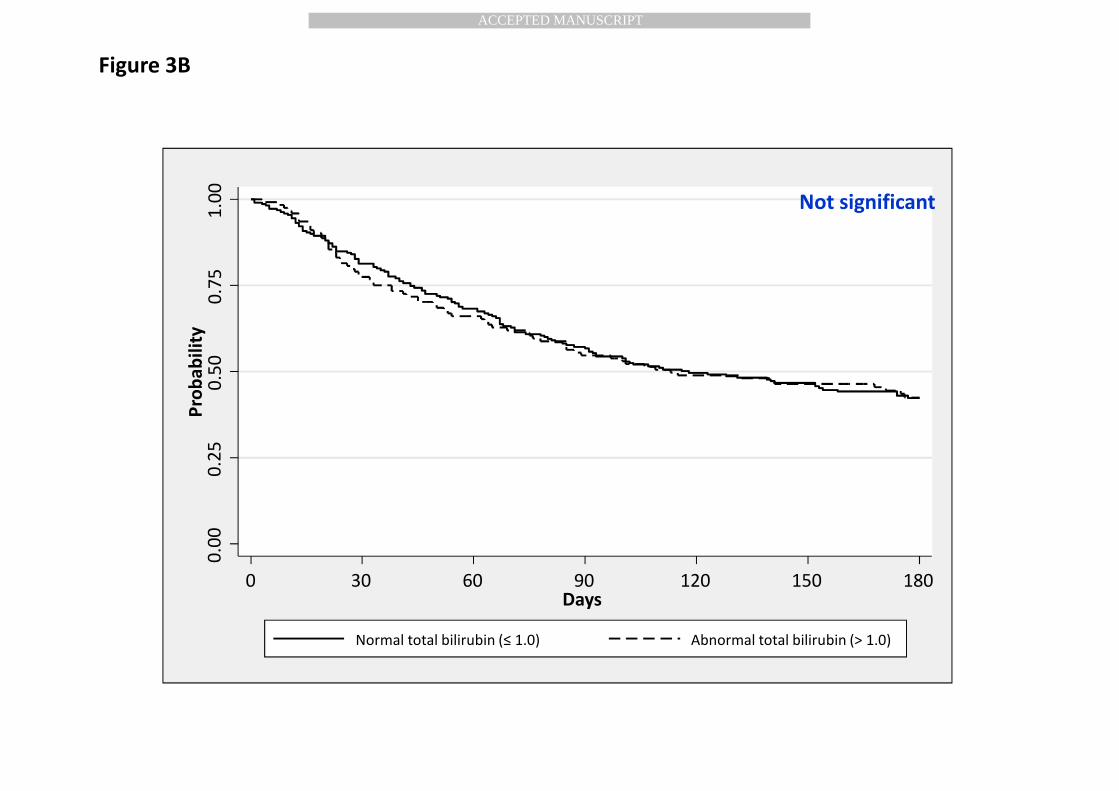
patients with abnormal creatinine (> 1.3) had a significantly increased risk of the composite endpoint (Figure
3A, P < 0.01) and there was no difference in outcomes for patients with abnormal (> 1.0) vs. normal total
bilirubin (Figure 3B). CART analyses did not yield a novel cut-point for any of the LFTs.
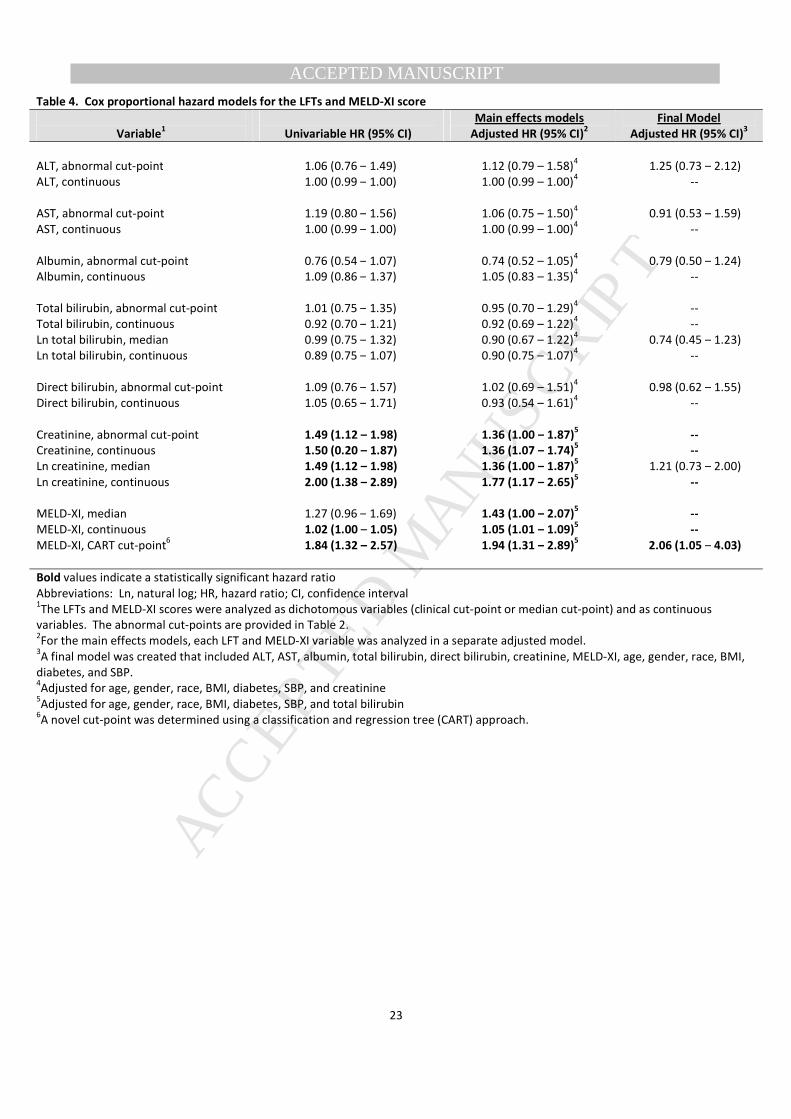
Cox proportional hazard models
The MELD-XI score and LFTs were analyzed in univariable Cox proportional hazard models to estimate the
magnitude of risk for the association with the composite endpoint (Table 4). Each LFT was analyzed as
dichotomous variable determined by the established clinical cut-points (same cut-points listed in Table 2) and
as continuous variables. The natural log (Ln) of total bilirubin and creatinine were also analyzed at the median
cut-point and as a continuous variable. ALT, AST, Albumin, total bilirubin, and direct bilirubin were not
associated with the composite endpoint. However, creatinine and MELD-XI were associated with increased
risk of the composite endpoint in the univariable analyses. When the main effects for each LFT and the MELD-
XI score were analyzed in separate multivariable models, creatinine and MELD-XI were still associated with
increased risk of the composite endpoint. However, when all the LFTs and the MELD-XI score dichotomized at
the CART cut-point were analyzed in a single model, adjusting for age, gender, race, BMI, diabetes, and SBP,
elevated MELD-XI score was associated with a 2-fold (HR = 2.06; 95% CI 1.05 – 4.03) increased risk of the
composite endpoint. None of the hazard ratios for the LFTs were statistically significant in the final model.
We also explored a final model using the original distributions of total bilirubin and creatinine, and the results
were consistent (data not shown).
Page 12
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
Discussion
In this post hoc analysis of the limited access dataset from the ESCAPE trial, we analyzed longitudinal trends of
LFTs and creatinine in patients treated for ADHF and found that LFTs are a more dynamic marker of a
decompensated state. While the proportion of patients with abnormal LFTs decreased two-and three-fold
from admission to the hospital with ADHF to a six month follow-up, creatinine remained elevated in about half
of the patients. In terms of absolute values, creatinine did not significantly change through the duration of the
study, while LFTs improved substantially, especially among patients who had abnormal LFTs at baseline.
We also found that both congestion and low output contributed to LFT abnormalities, particularly, total
bilirubin and AST. Albumin and, surprisingly, creatinine, did not differ between normal or elevated CVP
(surrogate of congestion) or normal and decreased CI (low output state). Finally, we found that elevated
MELD-XI score was associated with poor patient outcomes in this population of patients with ADHF even after
adjusting for baseline LFTs and patient characteristics.
High prevalence of abnormal LFTs in HF have been reported previously, although the results in our
analyses indicate a higher prevalence than in prior studies. Patients included in the ESCAPE cohort required an
EF < 30%, prior recent admissions for ADHF, and at least three months of symptoms. In the analysis of the
EVEREST (Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan) and SURVIVE
(The Survival of Patients with Acute Heart Failure in Need of Intravenous Inotropic Support) trials (3, 4)
patients with low SBP were excluded, these patients were included in the ESCAPE cohort, also the population
was sufficiently ill to make use of the pulmonary artery catheters reasonable. The inclusion of a greater
severity of HF in the ESCAPE trial likely explains why 90% of our patients had at least one abnormal LFT at
admission compared to near 50% in other cohorts.
The CHARM (Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity) trial
studied a mixed preserved and reduced LVEF population with chronic HF and found abnormal alanine
aminotransferase was present in 3.1% of patients, low albumin in 18.3%, and total bilirubin in 13.0% of
Page 13
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
patients (1). The results from the CHARM trial are similar to the six month follow-up values in our analysis, but
far lower than our baseline data on admissions for ADHF. Even their cohort of patients with reduced LVEF had
lower representation of abnormal LFTs than our cohort. In the EVEREST (Efficacy of Vasopressin Antagonism in
Heart Failure Outcome Study with Tolvaptan) analysis, the prevalence of LFT abnormalities was high at
baseline and remained virtually unchanged during hospitalization, with the exception of elevated total
bilirubin, but still the prevalence of abnormal LFTs they observed (ALB 17%, AST 21%, ALT 21%, and total
bilirubin 26%) was somewhat lower than ours (29%, 24%, 24%, and 36%, respectively)(4). However, in our
analysis, all LFTs showed significant post discharge improvement. Unlike in other studies, we could track the
LFTs of the ESCAPE patients until 6 months of follow-up, while the EVEREST patients were only followed for
eight weeks (4). Hence, we were able to report more detailed analysis of longitudinal changes of LFTs in HF
than previously published studies. We were also able to compare LFT trends with the respective changes in
creatinine and found that LFT mirrored more closely the pattern that is seen in B-type natriuretic peptide
(BNP) levels after treatment of ADHF. Conversely, the prevalence of creatinine abnormalities remained near
50% at all time points. We see that LFTs are more labile than creatinine from the decompensated state to
stable treated HF.
To evaluate which biomarker is associated with a congestive versus ischemic state we utilized patients
of the ESCAPE trial in the pulmonary artery catheter arm. We found that patients with elevated total bilirubin
had significantly lower CI and higher CVP. This result is similar to prior studies that evaluated a similar patient
population monitored with Swan-Ganz catheters (11, 12) but varies from other studies that found total
bilirubin to only be associated with an elevated central venous pressure and tricuspid regurgitation (13, 14).
We saw a similar trend with AST; patients with elevated AST had lower mean CI and significantly higher CVP.
In the CHARM trial cohort, the total bilirubin elevation was observed in patients with physical signs of
congestion, but invasive hemodynamics was not available(1). Van Deursen et al. showed that total bilirubin
levels, as well as AST and ALT, were associated with both low CI and elevated CVP(14). Interestingly, patients
Page 14
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
with abnormally low albumin did not, by our findings, have a significant difference in mean CI and CVP
suggesting albumin is less influenced by the hemodynamic state. Further prospective study is needed to
better evaluate the relationship between abnormal LFTs and hemodynamic compromise in ADHF. However, it
is clinically useful to understand the LFT profile one may expect in patients presenting with ADHF with varied
forms of hemodynamic compromise.
We also found that creatinine did not appear to be related to either elevated CVP or low CI. In the prior
studies, creatinine was shown to be higher in congested state (high CVP) (15, 16). However, in the Cleveland
Clinic series, the worsening of renal function (change in creatinine), rather than creatinine per se, was the
focus of the study. In the current paper, we did not target the change in creatinine, and therefore our data are
not directly comparable. As for the second study (15), the population was completely different from the
ESCAPE and included all comers to the catheterization laboratory for a Swan-Ganz catheter, with a significant
share of patients with better LVEF and generally less sick than patients included into the present analysis.
Because HF is a multi-system disease, application of the MELD-XI score, which combines parameters of
both hepatic and renal function for prognostic and risk-stratification purposes, is appealing. To our knowledge,
it has never been assessed in the broad HF population admitted for acute decompensation and followed for
substantial length of time. Previous studies have analyzed this score in different subsets of HF populations. In
patients undergoing heart transplantation, individuals with a higher pre-transplantation MELD or modified
MELD score (with albumin included instead of INR) had worse outcomes 30 days post-transplant and reduced
long-term survival over a 10-year follow-up (8). When the MELD-XI score was categorized by percentiles
(Figures 2A to 2C), we consistently found that high MELD-XI was associated with poor patient outcomes;
however, none of the log-rank P-values were statistically significant. Thus, using CART analyses we found a
novel cut-point which revealed that patients with a MELD-XI score ≥ 16.8 had significantly poorer patient
outcomes compared to patients with a MELD-XI score < 16.8 (Figure 2D). When all baseline LFTs, patient
characteristics, and MELD-XI score were included in a single multivariable model (Table 4), we found that high
Page 15
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
MELD-XI score was significantly associated with poor patient outcomes and none of the LFTs were statistically
significant. Thus, our results suggest that MELD-XI score, which includes the Ln of total bilirubin and
creatinine, is an independent predictor of patient outcomes. In a separate study of ambulatory patients with
HF awaiting heart transplant, MELD, MELD-XI, and MELD NA (including serum sodium) scores all predicted
poor outcomes, poor outcomes defined as death/transplantation/ventricular assist device requirement. In
that study, authors also found that MELD scores were related to congestion but not to low output. The MELD
scores were stronger predictors of adverse outcomes than their individual components(6). Of note, while total
bilirubin by itself was a predictor of poor outcomes, creatinine was not, opposite to our findings. In HF
patients undergoing ventricular assist device implantation, lower MELD or MELD-XI scores were associated
with better overall survival with a higher predictive power for MELD-XI (9). By their multivariable analysis, high
creatinine levels by themselves did not predict poor outcomes, meaning that bilirubin was a major contributor
to prognostic significance of the score. Some other data investigated the predictive role of LFTs in regards to
prognosis in HF. In chronic stable HF patients of the CHARM trial, total bilirubin predicted poor outcomes
stronger than creatinine (1). Total bilirubin and albumin predicted poor outcome in the EVEREST trial; no
comparison with creatinine was made (4, 12). In our analyses of advanced HF, high MELD-IX scores were
associated with poor outcomes at six months. When the MELD-XI scores were dichotomized at a novel cut-
point determined by CART analyses, patients with MELD-XI score ≥ 16.8 (observed in 18% of patients) had
increased risk of death, re-hospitalization, or transplant at the six months (Figure 2D). This is similar, although
slightly higher, than the average optimal cutoff value derived from 1-year ROC analyses of MELD scores in a
recent study of outpatients with severe heart failure undergoing transplant workup(6). Creatinine was
independently associated with poor outcomes (Figure 3A); however, in the final model, which adjusts for all
LFT’s and patient demographics, MELD-XI was the only factor significantly associated with the composite
endpoint. Worse outcomes are seen in patients with a greater degree of multi-system dysfunction and, as
expected, there appears to be added prognostic value when combining creatinine and bilirubin in this manner.
Page 16
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
Limitations
We acknowledge potential limitations of this analysis. Firstly, this was a post hoc analysis of data collected in
the context of a clinical trial with specific inclusion and exclusion criteria, which could limit the generalizability
of these findings. The sample size of patients with abnormal LFTs and Creatinine within the pulmonary artery
catheter arm of the data set was relatively small, limiting the power of our hemodynamic results. Additionally,
LFT data was not available for all patients at every time point of follow-up
Conclusions
Abnormalities in liver function tests are exceedingly common among acutely decompensated heart failure
patients, and therefore, further support the concept of heart failure as a multisystem disease. Our data
suggested the prevalence of abnormal LFTs showed a significant decline in the post-discharge period of
treated HF patients and is perhaps a better surrogate of systemic congestion than creatinine. Although
additional prospective studies are needed, multi-organ system composite scoring methods like MELD-XI may
have important prognostic implications when applied to the general heart failure population.
Page 17
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
Acknowledgments
The ESCAPE is conducted and supported by the NHLBI in collaboration with the ESCAPE Study
Investigators. This manuscript was prepared using a limited access dataset obtained from the NHLBI and does
not necessarily reflect the opinions or views of the ESCAPE or the NHLBI.
Disclosures
None.
Page 18
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
References
1. Allen LA, Felker GM, Pocock S, McMurray JJ, Pfeffer MA, Swedberg K, et al. Liver function abnormalities
and outcome in patients with chronic heart failure: data from the Candesartan in Heart Failure: Assessment of
Reduction in Mortality and Morbidity (CHARM) program. European journal of heart failure. 2009;11(2):170-7.
2. Yu SB, Cui HY, Qin M, Liu T, Kong B, Zhao QY, et al. [Prevalence and prognostic value of liver function
abnormalities in patients with chronic systolic heart failure]. Zhonghua yi xue za zhi. 2011;91(38):2673-7.
3. Nikolaou M, Parissis J, Yilmaz MB, Seronde MF, Kivikko M, Laribi S, et al. Liver function abnormalities,
clinical profile, and outcome in acute decompensated heart failure. European heart journal. 2013;34(10):742-9.
4. Ambrosy AP, Vaduganathan M, Huffman MD, Khan S, Kwasny MJ, Fought AJ, et al. Clinical course and
predictive value of liver function tests in patients hospitalized for worsening heart failure with reduced ejection
fraction: an analysis of the EVEREST trial. European journal of heart failure. 2012;14(3):302-11.
5. Moller S, Bernardi M. Interactions of the heart and the liver. European heart journal. 2013.
6. Kim MS, Kato TS, Farr M, Wu C, Givens RC, Collado E, et al. Hepatic dysfunction in ambulatory patients
with heart failure: application of the MELD scoring system for outcome prediction. Journal of the American
College of Cardiology. 2013;61(22):2253-61.
7. Heuman DM, Mihas AA, Habib A, Gilles HS, Stravitz RT, Sanyal AJ, et al. MELD-XI: a rational approach to
"sickest first" liver transplantation in cirrhotic patients requiring anticoagulant therapy. Liver transplantation :
official publication of the American Association for the Study of Liver Diseases and the International Liver
Transplantation Society. 2007;13(1):30-7.
8. Chokshi A, Cheema FH, Schaefle KJ, Jiang J, Collado E, Shahzad K, et al. Hepatic dysfunction and survival
after orthotopic heart transplantation: application of the MELD scoring system for outcome prediction. The
Journal of heart and lung transplantation : the official publication of the International Society for Heart
Transplantation. 2012;31(6):591-600.
Page 19
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
9. Yang JA, Kato TS, Shulman BP, Takayama H, Farr M, Jorde UP, et al. Liver dysfunction as a predictor of
outcomes in patients with advanced heart failure requiring ventricular assist device support: Use of the Model
of End-stage Liver Disease (MELD) and MELD eXcluding INR (MELD-XI) scoring system. The Journal of heart and
lung transplantation : the official publication of the International Society for Heart Transplantation.
2012;31(6):601-10.
10. Binanay C, Califf RM, Hasselblad V, O'Connor CM, Shah MR, Sopko G, et al. Evaluation study of
congestive heart failure and pulmonary artery catheterization effectiveness: the ESCAPE trial. JAMA : the
journal of the American Medical Association. 2005;294(13):1625-33.
11. Biegus J, Zymlinski R, Sokolski M, Nawrocka S, Siwolowski P, Szachniewicz J, et al. Liver function tests in
patients with acute heart failure. Polskie Archiwum Medycyny Wewnetrznej. 2012;122(10):471-9.
12. Shinagawa H, Inomata T, Koitabashi T, Nakano H, Takeuchi I, Naruke T, et al. Prognostic significance of
increased serum bilirubin levels coincident with cardiac decompensation in chronic heart failure. Circulation
journal : official journal of the Japanese Circulation Society. 2008;72(3):364-9.
13. Lau GT, Tan HC, Kritharides L. Type of liver dysfunction in heart failure and its relation to the severity of
tricuspid regurgitation. The American journal of cardiology. 2002;90(12):1405-9.
14. van Deursen VM, Damman K, Hillege HL, van Beek AP, van Veldhuisen DJ, Voors AA. Abnormal liver
function in relation to hemodynamic profile in heart failure patients. Journal of cardiac failure. 2010;16(1):84-
90.
15. Guglin M, Rivero A, Matar F, Garcia M. Renal dysfunction in heart failure is due to congestion but not
low output. Clinical cardiology. 2011;34(2):113-6.
16. Mullens W, Abrahams Z, Francis GS, Sokos G, Taylor DO, Starling RC, et al. Importance of venous
congestion for worsening of renal function in advanced decompensated heart failure. Journal of the American
College of Cardiology. 2009;53(7):589-96.
Page 20
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
Table 1. Baseline characteristics of the study population: overall and dichotomized by MELD-XI score
Overall MELD-XI Score2
Characteristic
Included1
Excluded P-value3
High (≥ 11.4) Low (< 11.4)
P-value4
N = 346 N = 87 (N = 176) (N = 170)
Age, mean (SD) 55.5 (13.8) 58.7 (14.2) 0.055 59.1 (13.9) 51.7 (12.7) < 0.001
Gender, N (%)
Men 259 (74.9) 62 (71.3) 150 (85.2) 109 (64.1)
Women 87 (25.1) 25 (28.7) 0.497 26 (14.8) 61 (35.9) < 0.001
Race, N (%)
White 205 (59.3) 53 (60.9) 113 (64.2) 92 (54.1)
Non-white 141 (40.8) 34 (39.1) 0.776 63 (35.8) 78 (45.9) 0.056
BMI, mean (SD) 28.8 (6.6) 29.7 (7.4) 0.300 28.3 (6.1) 29.4 (7.1) 0.122
Idiopathic etiology, N (%)
Yes 124 (35.9) 26 (30.2) 57 (32.6) 67 (39.4)
No 221 (64.1) 60 (69.8) 0.320 118 (67.4) 103 (60.6) 0.186
Ischemic etiology, N (%)
Yes 164 (47.5) 49 (57.0) 96 (54.9) 68 (40.0)
No 181 (52.5) 37 (43.0) 0.117 79 (45.1) 102 (60.0) 0.006
Diabetes at baseline, N (%)
Yes 107 (31.0) 33 (38.4) 57 (32.6) 50 (29.4)
No 238 (69.0) 53 (61.6) 0.192 118 (67.4) 120 (70.6) 0.526
Liver Function Tests, median (25th
to 75TH
)
ALT 27.0 (19.0 – 39.0) 23.5 (22 – 32.0) 0.496 27.0 (18.0 – 35.5) 27.0 (20.0 – 43.0) 0.239
AST 29.0 (22.0 – 39.5) 37.0 (31.0 – 37.0) 0.193 29.0 (22.0 – 39.0) 29.0 (22.0 – 40.0) 0.706
Albumin (Alb) 3.6 (3.3 – 4.0) 3.45 (3.3 – 3.7) 0.401 3.6 (3.2 – 4.0) 3.6 (3.3 – 4.0) 0.785
Total bilirubin (TBili) 0.8 (0.4 – 1.2) N/A -- 1.1 (0.8 –1.5) 0.5 (0.2 – 0.8) < 0.001
Direct bilirubin (DBili) 0.1 (0.1 – 0.6) 0.35 (0.09 – 0.6) 0.871 0.3 (0.2 – 0.6) 0.2 (0.09 – 0.6) 0.020
Creatinine (Cr) 1.4 (1.1 – 1.8) 1.4 (1.1 – 1.9) 0.448 1.7 (1.4 – 2.1) 1.1 (0.9 – 1.3) < 0.001
Peak Vo2, mean (SD) 9.9 (3.1) 11.3 (1.3) 0.134 9.96 (3.07) 9.78 (3.20) 0.752
6-min walk, mean (SD) 420.8 (421.4) 386 (44.8) 0.517 453.1 (424.5) 387.6 (416.9) 0.169
Bold p-values indicate a statistically significant difference between high MELD and low MELD
Page 21
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
1Among patients who have both total bilirubin at baseline and creatinine at baseline (N = 346); patients that were excluded did not have both total bilirubin
at baseline and creatinine at baseline 2 MELD Score is dichotomized at the median value
3 To test for differences between patients that were included and excluded, P-values were calculated using Pearson’s chi-square for categorical variables,
Student’s t-test comparing mean variables, and Wilcoxon rank sum test comparing median values.
4 To test for differences between high MELD and low MELD, P-values were calculated using Pearson’s chi-square for categorical variables, Student’s t-test
comparing mean variables, and Wilcoxon rank sum test comparing median values.
Page 22
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21
Table 2. Prevalence of abnormal LFTs for each time-point among individuals with total bilirubin at baseline and baseline creatinine
Baseline Discharge 2 weeks 1 month 2 months 3 months 6 months P-value1
ALT Normal N 250 132 126 139 112 133 97
Normal % 75.7 80.0 73.3 76.8 76.7 82.1 82.9
Elevated (> 40), N 80 33 46 42 34 29 20
Elevated (> 40), % 24.2 20.0 26.7 23.2 23.3 17.9 17.1 < 0.001
Median ALT 59.5 40 43 30 32 29.5 29
AST Normal N 257 128 134 157 122 133 101
Normal % 76.5 77.1 76.1 85.8 83.6 81.1 86.3
Elevated (> 40), N 79 38 42 26 24 31 16
Elevated (> 40), % 23.5 22.9 23.9 14.2 16.4 18.9 13.7 0.009
Median AST 56 35.5 58 30 29.5 26 27
Albumin Normal N 225 116 145 154 124 142 103
Normal % 70.7 71.2 86.8 86.0 86.1 88.2 89.6
Decreased (< 3.4), N 93 47 22 25 20 19 12
Decreased (< 3.4), % 29.3 28.8 13.2 14.0 13.9 11.8 10.4 < 0.001
Median Alb 3.1 3.3 3.6 3.7 3.6 3.7 3.7
Total bilirubin Normal N 221 119 122 130 119 130 98
Normal % 63.9 68.4 68.2 70.7 81.5 79.7 83.1
Elevated (> 1.0), N (%) 125 55 57 54 27 33 20
Elevated (> 1.0), % 36.1 31.6 31.8 29.4 18.5 20.3 16.9 < 0.001
Median TBili 1.4 1 0.9 0.9 0.7 0.7 0.7
Direct bilirubin Normal. N 131 85 91 89 78 97 69
Normal. % 60.1 63.4 73.4 76.7 75.7 84.4 84.2
Elevated (> 0.3), N 87 49 33 27 25 18 13
Elevated (> 0.3). % 39.9 36.6 26.6 23.4 24.4 15.6 15.8 < 0.001
Median Dir Bili 0.6 0.4 0.3 0.3 0.2 0.2 0.2
Creatinine Normal. N 168 173 114 123 94 92 74
Normal. % 48.5 53.2 46.9 49.8 46.1 42.8 55.2
Elevated (> 1.3), N 178 152 129 124 110 123 60
Elevated (> 1.3), % 51.5 46.8 53.1 50.2 53.9 57.2 44.8 0.055
Median Cr 1.8 1.8 1.9 1.9 1.8 1.7 1.8
Bold P-values indicate a statistically significant difference in percentage of patients with abnormal LFTs from baseline to 6 months
1 P-values were generated from a generalized estimating equation (GEE)
Page 23
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
22
Table 3. CVP and CI by baseline LFT and creatinine status
LFT Status at baseline1
CVP, mean (SD) CI, mean (SD)
AST abnormal (> 40) 15.4 (9.1) 1.9 (0.65)
AST normal (≤ 40) 12.2 (6.6) 2.0 (0.64)
P-value
0.010 0.482
ALT abnormal (> 40) 14.3 (6.4) 2.0 (0.62)
ALT normal (≤ 40) 12.4 (9.7) 2.0 (0.63)
P-value 0.139 0.941
Albumin abnormal (< 3.4) 13.1 (6.9) 1.9 (0.64)
Albumin normal (≥ 3.4) 12.7 (6.9) 2.0 (0.58)
P-value 0.693 0.629
Total bilirubin abnormal (> 1.0) 14.4 (6.5) 1.8 (0.48)
Total bilirubin li normal (≤ 1.0) 12.0 (6.8) 2.1 (0.69)
P-value 0.030 < 0.001
Direct bilirubin abnormal (≥ 0.3) 15.5 (6.7) 1.8 (0.56)
Direct bilirubin li normal (< 0.3) 9.9 (5.7) 2.1 (0.58)
P-value < 0.001 0.006
Creatinine abnormal (> 1.3) 13.8 (6.6) 2.0 (0.69)
Creatinine normal (≤ 1.3) 11.8 (6.8) 2.0 (0.56)
P-value 0.054 0.972
Bold P-values indicate a statistically significant difference
1P-values were calculated from Student’s t-test comparing mean CVP by baseline LFT Status and mean
CI by baseline LFT Status
Page 24
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
23
Table 4. Cox proportional hazard models for the LFTs and MELD-XI score
Variable1
Univariable HR (95% CI)
Main effects models
Adjusted HR (95% CI)2
Final Model
Adjusted HR (95% CI)3
ALT, abnormal cut-point 1.06 (0.76 – 1.49) 1.12 (0.79 – 1.58)4
1.25 (0.73 – 2.12)
ALT, continuous 1.00 (0.99 – 1.00) 1.00 (0.99 – 1.00)4
--
AST, abnormal cut-point 1.19 (0.80 – 1.56) 1.06 (0.75 – 1.50)4
0.91 (0.53 – 1.59)
AST, continuous 1.00 (0.99 – 1.00) 1.00 (0.99 – 1.00)4
--
Albumin, abnormal cut-point 0.76 (0.54 – 1.07) 0.74 (0.52 – 1.05)4
0.79 (0.50 – 1.24)
Albumin, continuous 1.09 (0.86 – 1.37) 1.05 (0.83 – 1.35)4
--
Total bilirubin, abnormal cut-point 1.01 (0.75 – 1.35) 0.95 (0.70 – 1.29)4
--
Total bilirubin, continuous 0.92 (0.70 – 1.21) 0.92 (0.69 – 1.22)4 --
Ln total bilirubin, median 0.99 (0.75 – 1.32) 0.90 (0.67 – 1.22)4 0.74 (0.45 – 1.23)
Ln total bilirubin, continuous 0.89 (0.75 – 1.07) 0.90 (0.75 – 1.07)4 --
Direct bilirubin, abnormal cut-point 1.09 (0.76 – 1.57) 1.02 (0.69 – 1.51)4
0.98 (0.62 – 1.55)
Direct bilirubin, continuous 1.05 (0.65 – 1.71) 0.93 (0.54 – 1.61)4
--
Creatinine, abnormal cut-point 1.49 (1.12 – 1.98) 1.36 (1.00 – 1.87)5 --
Creatinine, continuous 1.50 (0.20 – 1.87) 1.36 (1.07 – 1.74)5
--
Ln creatinine, median
1.49 (1.12 – 1.98) 1.36 (1.00 – 1.87)5
1.21 (0.73 – 2.00)
Ln creatinine, continuous 2.00 (1.38 – 2.89) 1.77 (1.17 – 2.65)5
--
MELD-XI, median 1.27 (0.96 – 1.69) 1.43 (1.00 – 2.07)5
--
MELD-XI, continuous 1.02 (1.00 – 1.05) 1.05 (1.01 – 1.09)5
--
MELD-XI, CART cut-point6
1.84 (1.32 – 2.57) 1.94 (1.31 – 2.89)5
2.06 (1.05 – 4.03)
Bold values indicate a statistically significant hazard ratio
Abbreviations: Ln, natural log; HR, hazard ratio; CI, confidence interval 1The LFTs and MELD-XI scores were analyzed as dichotomous variables (clinical cut-point or median cut-point) and as continuous
variables. The abnormal cut-points are provided in Table 2. 2For the main effects models, each LFT and MELD-XI variable was analyzed in a separate adjusted model.
3A final model was created that included ALT, AST, albumin, total bilirubin, direct bilirubin, creatinine, MELD-XI, age, gender, race, BMI,
diabetes, and SBP. 4Adjusted for age, gender, race, BMI, diabetes, SBP, and creatinine
5Adjusted for age, gender, race, BMI, diabetes, SBP, and total bilirubin
6A novel cut-point was determined using a classification and regression tree (CART) approach.
Page 25
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
24
Figure Legends
Figure 1. Prevalence of abnormal LFTs from admission to six-month follow-up. The cut-offs for abnormal
values were serum creatinine (Cr > 1.3mg/dL), total bilirubin (TBili > 1.0mg/dL), aspartate
transaminase (AST > 40 IU/L), alanine transaminase (ALT > 40 IU/L), and albumin (ALB < 3.4
g/dL).
Figure 2. Kaplan-Meier survival curves for the composite endpoint (death, cardiac re-hospitalization, and
Heart transplant (Htx) by MELD-XI score. (A) MELD-XI score dichotomized at the median, (B)
MELD-XI score categorized by tertiles, (C) MELD-XI score categorized by quartiles, and (D)
MELD-XI score dichotomized at a cut-point determined by CART analysis. P-values are from the
log-rank test.
Figure 3. Kaplan-Meier survival curves for composite endpoint (death, cardiac re-hospitalization, and
Heart transplant (Htx) by (A) baseline creatinine (abnormal [>1.3] vs. normal [≤ 1.3]), and (B)
baseline total bilirubin (abnormal [> 1.0] vs normal [≤ 1.0]). P-values are from the log-rank test.
Page 26
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 1
0
10
20
30
40
50
60
Admission Discharge 2 weeks 1 month 2 month 3 month 6 monthCr 51.5 46.8 53.1 50.2 53.9 57.2 44.8Tbili 36.1 31.6 31.8 29.4 18.5 20.3 16.9Dbili 39.9 36.6 26.6 23.4 24.4 15.6 15.8AST 23.5 22.9 23.9 14.2 16.4 18.9 13.7ALT 24.2 20 26.7 23.2 23.3 17.9 17.1Alb 29.3 28.8 13.2 14 13.9 11.8 10.4
Pre
cen
t ab
no
rmal
Page 27
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 2A
0.0
00
.25
0.5
00
.75
1.0
0P
rob
ab
ilit
y
0 30 60 90 120 150 180Days
Low MELD-XI (< 14.3) High MELD-XI (≥ 14.3)
P = 0.09
Page 28
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 2B
0.0
00
.25
0.5
00
.75
1.0
0P
rob
ab
ilit
y
0 30 60 90 120 150 180Days
Low MELD-XI (< 8.7) Medium MELD-XI (≥ 8.7 to < 13.9)
High MELD-XI (≥ 13.9)
P = 0.07
Page 29
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 2C
0.0
00
.25
0.5
00
.75
1.0
0
Pro
ba
bil
ity
0 30 60 90 120 150 180Days
First quartile MELD-XI (< 6.8) Second quartile MELD-XI (≥ 6.8 to < 11.4)
Third quartile MELD-XI (≥ 11.4 to < 15.5) Fourth quartile MELD-XI (≥ 15.5)
P = 0.07
Page 30
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 2D
0.0
00
.25
0.5
00
.75
1.0
0P
rob
ab
ilit
y
0 30 60 90 120 150 180Days
Low MELD-XI (< 16.8) High MELD-XI (≥ 16.8)
P < 0.001
Page 31
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
0.0
00
.25
0.5
00
.75
1.0
0
Pro
ba
bil
ity
0 30 60 90 120 150 180Days
Normal creatinine (≤ 1.3) Abnormal creatinine (> 1.3)
P < 0.01
Figure 3A
Page 32
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
0.0
00
.25
0.5
00
.75
1.0
0P
rob
ab
ilit
y
0 30 60 90 120 150 180Days
Normal total bilirubin (≤ 1.0) Abnormal total bilirubin (> 1.0)
Not significant
Figure 3B
Page 33
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Longitudinal Trends, Hemodynamic Profiles, and Prognostic Value of Abnormal
Liver Function Tests in Patients with Acute Decompensated Heart Failure: an
Analysis of the ESCAPE Trial
Highlights:
• We analyzed LFT abnormalities in severely decompensated heart failure patients.
• Patients admitted with heart failure have a high prevalence of abnormal LFTs.
• Abnormal LFTs are a dynamic marker of an impaired hemodynamic state.
• Elevated total bilirubin was associated with a lower cardiac index and higher CVP.
• Patients with elevated MELD-XI scores had a 2-fold increased risk of poor outcomes.