16
2013-14 Benefits Preview Look inside for important information about how to use your PEHP benefits. Weber State University 2013-2014
2013-14Benefits Preview
Look inside for important information about how to use your PEHP benefits.
Weber State University2013
-201
4

PAGE 2 www.PEhP.orG
Weber State University 2013-2014 » Contact Information
Welcome to PEHP
On the Web»myPEHP . . . . . . . . . . . . . . . . . . . . . . . . . . www.pehp.orgmyPEHP is your online source for personal health and plan benefit information. You can review your claims history, see a comprehensive list of your coverages, look up contracted providers, and more. Create a myPEHP account to enroll in PEHP benefits electronically.
CustOmer serviCe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 801-366-7555 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 800-765-7347Weekdays from 8 a.m. to 5 p.m. Have your PEHP ID or Social Security number on hand for faster service. Foreign language assistance available
Pre-nOtifiCatiOn/Pre-authOrizatiOn»Inpatient hospital pre-notification . . . . . . 801-366-7755 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 800-753-7754
mental health/substanCe abuse Pre-authOrizatiOn »PEHP Customer Service. . . . . . . . . . . . . . . .801-366-7555 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 800-765-7347
PresCriPtiOn drug benefits»PEHP Customer Service. . . . . . . . . . . . . . . .801-366-7555 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 800-765-7347
»Express Scripts . . . . . . . . . . . . . . . . . . . . . . . 800-903-4725 . . . . . . . . . . . . . . . . . . . . . . . . . . .www.express-scripts.com
sPeCialty PharmaCy »Accredo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 800-501-7260
PehP flex$/limited flex$»PEHP FLEX$ Department . . . . . . . . . . . . . 801-366-7503 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 800-753-7703
health savings aCCOunts (hsa)»Health Equity . . . . . . . . . . . . . . . . . . . . . . . . 866-960-8058 . . . . . . . . . . . . . . . . . . www.healthequity.com/stateofutah
Prenatal PrOgram» PEHP WeeCare . . . . . . . . . . . . . . . . . . . . . 801-366-7400 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 855-366-7400
Wellness and disease management» PEHP Healthy Utah . . . . . . . . . . . . . . . . . 801-366-7300 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 855-366-7300 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . www.healthyutah.org
» PEHP Waist Aweigh . . . . . . . . . . . . . . . . . 801-366-7478 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 888-753-7478
» PEHP Integrated Care . . . . . . . . . . . . . . . 801-366-7555 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 800-765-7347 . . . . . . . . . . . . . . . . . . . . . . . . . . . . www.pehp.org/weecare
value-added benefits PrOgram» PEHPplus . . . . . . . . . . . . . . . . . . . .www.pehp.org/plus
»Blomquist Hale . . . . . . . . . . . . . . . . . . . . . . 800-926-9619 . . . . . . . . . . . . . . . . . . . . . . . . . . . .www.blomquisthale.com
Online enrOllment helP line . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 801-366-7410 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . or 800-753-7410
Claims mailing addressPEhP560 East 200 SouthSalt Lake City, Utah 84102-2004
We want to make accessing and understanding your healthcare benefits simple. This Benefits Summary contains important information on how best to use PEHP’s comprehensive benefits.
Please contact the following PEHP departments or affiliates if you have questions.
4-1-13

PAGE 3 www.PEhP.orG
Weber State University 2013-2014 » Benefit Changes & Reminders
Benefit Changes & RemindersAll Medical Plans
» Healthcare Reform requires a Summary of Benefits and Coverage (SBC) to be distributed to all benefit-eligible employees before open enrollment. This will be distributed through a WSU Special Campus Bulletin during the first week of April.
» Effective Jan. 1, 2013, new preventive services for women have been added to the Affordable Care Act list. Please see the Master Policy for a complete list of preventive services.
» Accupuncture services are no longer a covered benefit.
» Medco, PEHP’s pharmacy benefit manager, is now known as Express Scripts and can be found online at www.express-scripts.com.
» Members who made changes to their PEHP plans will receive a new ID card in the mail from Express Scripts. It will serve as your medical, pharmacy, and out-of-state network ID card. If you did not make changes, continue to use your current card(s).
» Members can shop for value, compare prices, and save money using PEHP’s new Cost & Quality Tools, accessible through their myPEHP account.
» Medicare Supplement plansPEHP offers three Medicare Supplement Medical plans and Medicare Part D approved Prescription Drug plans. PEHP also offers a value-added Discount Dental plan to individuals who enroll in one of the PEHP Medicare Medical Supplement options. Please contact PEHP Customer Service for more details and enrollment information.
The STAR Plan
» The STAR Plan will continue to be an option using the Advantage and Summit Care networks. The STAR Plan has two components: A High Deductible Health Plan HDHP) and a Health Savings Account (HSA). There is no employee cost share for this plan. Those enrolled in the STAR PLAN will receive semi-monthly contributions to their HSA in the amount of $31.25 single / $62.50 double and family each pay day.
FLEX$ Changes
» Due to Federal Healthcare Reform, the medical Flexible Spending Account maximum has been reduced to $2,500. The dependent day care maximum will remain at $5,000.
» Beginning April 1, 2013, PEHP FLEX$ card holders may be required to enter a Personal Identification Number (PIN) when making point-of-sale purchases.To view your PIN, you will need your PEHP member ID (last 6 digits) and FLEX$ card number. Log in to your myPEHP account and, once on the FLEX$ page, click on Card Status. Follow the online steps to view your PIN, as well as PINs for other cardholders on your account.Questions? Please contact PEHP FLEX$ at 801-366-7503.

PAGE 4 www.PEhP.orG
Weber State University 2013-2014 » PEHP Medical NetworksMedical Networks
PEHP Medical NetworksPEHP Advantage Care
The PEHP Advantage Care network of contracted providers consists of predominantly Intermountain Healthcare (IHC) providers and facilities. It includes 34 participating hospitals and more than 7,500 participating providers.
PARTICIPATING HOSPITALS
PEHP Preferred CareThe PEHP Preferred Care network of contracted providers consists of providers and facilities in both the Advantage Care and Summit Care networks. It includes 46 participating hospitals and more than 12,000 participating providers.
PEHP Summit CareThe PEHP Summit Care network of contracted Providers consists of predominantly IASIS, MountainStar, and University of Utah hospitals & clinics providers and facilities. It includes 38 participating hospitals and more than 7,500 participating providers.
PARTICIPATING HOSPITALS
Find Participating ProvidersGo to www.pehp.org to look up participating providers for each plan.
Beaver County Beaver Valley Hospital Milford Valley Memorial Hospital
Box Elder County Bear River Valley Hospital
Cache County Logan Regional Hospital
Carbon County Castleview Hospital
Davis County Davis Hospital
Duchesne County Uintah Basin Medical Center
Garfield County Garfield Memorial Hospital
Grand County Moab Regional Hospital
Iron County Valley View Medical Center
Juab County Central Valley Medical Center
Kane County Kane County Hospital
Millard County Delta Community Medical Center Fillmore Community Hospital
Salt Lake County Alta View Hospital Intermountain Medical Center
Salt Lake County (cont.) The Orthopedic Specialty Hospital (TOSH) LDS Hospital Primary Children’s Medical Center Riverton Hospital
San Juan County Blue Mountain Hospital San Juan Hospital
Sanpete County Gunnison Valley Hospital Sanpete Valley Hospital
Sevier County Sevier Valley Medical Center
Summit County Park City Medical Center
Tooele County Mountain West Medical Center
Uintah County Ashley Valley Medical Center
Utah County American Fork Hospital Orem Community Hospital Utah Valley Regional Medical Center
Wasatch County Heber Valley Medical Center
Washington County Dixie Regional Medical Center
Weber County McKay-Dee Hospital
Beaver County Beaver Valley Hospital Milford Valley Memorial Hospital
Box Elder County Bear River Valley Hospital Brigham City Community Hospital
Cache County Logan Regional Hospital
Carbon County Castleview Hospital
Davis County Lakeview Hospital Davis Hospital
Duchesne County Uintah Basin Medical Center
Garfield County Garfield Memorial Hospital
Grand County Moab Regional Hospital
Iron County Valley View Medical Center
Juab County Central Valley Medical Center
Kane County Kane County Hospital
Millard County Delta Community Medical Center Fillmore Community Hospital
Salt Lake County Huntsman Cancer Hospital Jordan Valley Hospital
Salt Lake County (cont.) Pioneer Valley Hospital Primary Children’s Medical Center Riverton Children’s Unit St. Marks Hospital Salt Lake Regional Medical Center University of Utah Hospital University Orthopaedic Center
San Juan County Blue Mountain Hospital San Juan Hospital
Sanpete County Gunnison Valley Hospital Sanpete Valley Hospital
Sevier County Sevier Valley Medical Center
Summit County Park City Medical Center
Tooele County Mountain West Medical Center
Uintah County Ashley Valley Medical Center
Utah County Mountain View Hospital Timpanogos Regional Hospital
Wasatch County Heber Valley Medical Center
Washington County Dixie Regional Medical Center
Weber County Ogden Regional Medical Center

PAGE 5 www.PEhP.orG
Weber State University 2013-2014 » Understanding Your Benefit Grid
Understanding Your Benefits Grid
mediCal deduCtibleThe set dollar amount that you must pay for yourself and/or your family members before PEHP begins to pay for covered medical ben-efits.
PharmaCy deduCtibleThe set dollar amount — separate from the medical plan year deductible —that you must pay for pharmacy for yourself and/or your family members before PEHP begins to pay for covered pharmacy benefits.
Plan year Out-Of-POCket maximumThe maximum dollar amount that you and/or your family pays each year for covered medical services in the form of copayments and coinsurance (includes deductibles on The STAR Plan).
maximum lifetime benefitThe total amount the plan pays for each cov-ered family member in his or her lifetime.
Pre-existing COnditiOn Waiting PeriOdA condition that is present six months before your plan enrollment date for which medical treatment, consultation, or diagnostic testing was received. This section tells you if you have a waiting period before coverage for a pre-existing condition begins.
COPaymentA specific amount you pay directly to a provider when you receive covered services. This can be either a fixed dollar amount or a percentage of the PEHP Maximum Allowable Fee.
COntraCted Contracted benefits apply when you receive covered services from contracted providers. You are responsible to pay the applicable copayment.
nOn-COntraCtedIf your plan allows the use of non-contracted providers, non-contracted benefits apply when you receive covered services. You are responsible to pay the applicable copayment, plus the difference between the billed amount and PEHP’s Maximum Allowable Fee (see Page 12).
maximum allOWable fee (maf)A schedule of maximum allowable fees established by PEHP and accepted by contracted providers, along with any required member copayment as payment in full (see Page 12).
PEHP » www.PEHP.org » PAgE 15
State of Utah 2009-2010 » Benefit Changes State of Utah 2009-2010 » Medical Benefits Grid » Advantage Care
Advantage Care » MEDICAL BENEFITS GRIDRefer to the Advantage Care Provider Plan Master Policy for specific criteria for the benefits listed below, as well as information on Limitations and Exclusions.
DeDuctibles, Plan MaxiMuMs, anD liMits
Plan year Deductible Does not apply to Out-of-Pocket Maximum
$250 per individual, $500 per family. Only applies for inpatient, outpatient hospital charges and major diagnostic services
Pharmacy Deductible Does not apply to Out-of-Pocket Maximum
$100 per individual, $200 per family.
Plan year Out-of-Pocket Maximum $2,000 per individual, $4,000 per family
Maximum Lifetime Benefit None
Pre-existing Condition Waiting Period 9-month Waiting Period— waived with evidence of prior Creditable Coverage
inPatient facility services
Medical and Surgical | Requires Pre-notification 90% of MAF after Deductible
Skilled Nursing Facility | Non-custodial Up to 60 days per plan year. Requires Pre-authorization and Medical Case Management
90% of MAF after Deductible
Hospice | Up to 6 months in a 3-year period. Requires Pre-authorization and Medical Case Management
100% of MAF
Rehabilitation | Up to $75,000 Lifetime Maximum. Requires Pre-authorization and Medical Case Management
90% of MAF after Deductible
Mental Health | Requires Pre-authorization through Mental Health Care of Utah (MHCU) at 1-800-541-9432
90% of MAF after Deductible
Substance Abuse | Requires Pre-authorization through Mental Health Care of Utah (MHCU) at 1-800-541-9432
90% of MAF after Deductible
OutPatient facility services
Outpatient Facility and Ambulatory Surgery 95% of MAF after Deductible
Ambulance (ground or air) Medical emergencies only, as determined by PEHP
80% of MAF
Emergency Room Medical emergencies only, as determined by PEHP
100% of MAF after $125 Copayment per visit Non-contracted: 100% of MAF after $250 Copayment per visit
Urgent Care Facility 100% of MAF after $45 Copayment per visit
Diagnostic Tests, X-rays, Minor For each test allowing $350 or less
100% of MAF
Diagnostic Tests, X-rays, Major For each test allowing more than $350
80% of MAF after Deductible
Chemotherapy, Radiation, and Dialysis 90% of MAF
Physical and Occupational Therapy Limited to 28 visits per plan year for all therapy types combined. Requires Pre-authorization after 16 visits
100% of MAF after applicable office Copayment per visit
Contracted Provider
1
54
32
1
2
3
4
5
Medical Deductible
Weber State University 2013-2014 » Medical Benefits Grid » Advantage, Summit & Preferred Care
PAGE 6 www.PEhP.orG
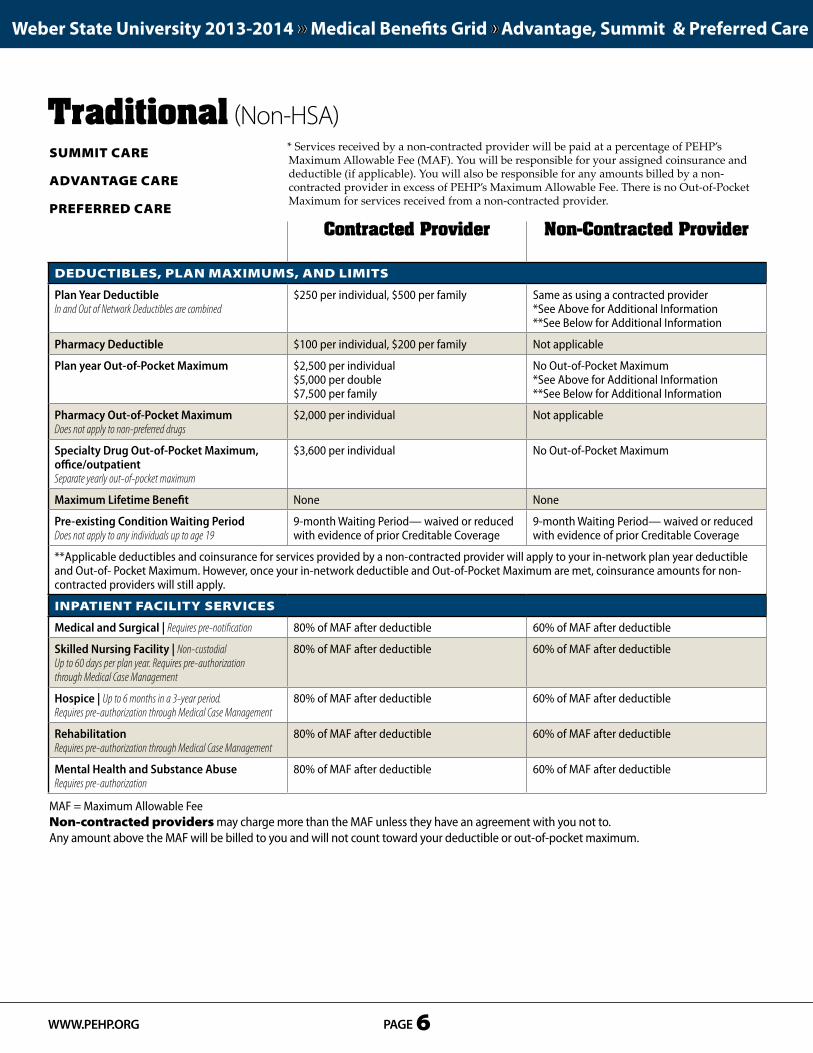
Traditional (Non-HSA)* Services received by a non-contracted provider will be paid at a percentage of PEHP’s Maximum Allowable Fee (MAF). You will be responsible for your assigned coinsurance and deductible (if applicable). You will also be responsible for any amounts billed by a non-contracted provider in excess of PEHP’s Maximum Allowable Fee. There is no Out-of-Pocket Maximum for services received from a non-contracted provider.
deduCtibles, Plan maximums, and limits
Plan Year Deductible In and Out of Network Deductibles are combined
$250 per individual, $500 per family Same as using a contracted provider*See Above for Additional Information**See Below for Additional Information
Pharmacy Deductible $100 per individual, $200 per family Not applicable
Plan year Out-of-Pocket Maximum $2,500 per individual $5,000 per double $7,500 per family
No Out-of-Pocket Maximum*See Above for Additional Information**See Below for Additional Information
Pharmacy Out-of-Pocket Maximum Does not apply to non-preferred drugs
$2,000 per individual Not applicable
Specialty Drug Out-of-Pocket Maximum,office/outpatient Separate yearly out-of-pocket maximum
$3,600 per individual No Out-of-Pocket Maximum
Maximum Lifetime Benefit None None
Pre-existing Condition Waiting Period Does not apply to any individuals up to age 19
9-month Waiting Period— waived or reduced with evidence of prior Creditable Coverage
9-month Waiting Period— waived or reduced with evidence of prior Creditable Coverage
**Applicable deductibles and coinsurance for services provided by a non-contracted provider will apply to your in-network plan year deductible and Out-of- Pocket Maximum. However, once your in-network deductible and Out-of-Pocket Maximum are met, coinsurance amounts for non-contracted providers will still apply.
inPatient faCility serviCes
Medical and Surgical | Requires pre-notification 80% of MAF after deductible 60% of MAF after deductible
Skilled Nursing Facility | Non-custodial Up to 60 days per plan year. Requires pre-authorization through Medical Case Management
80% of MAF after deductible 60% of MAF after deductible
Hospice | Up to 6 months in a 3-year period. Requires pre-authorization through Medical Case Management
80% of MAF after deductible 60% of MAF after deductible
RehabilitationRequires pre-authorization through Medical Case Management
80% of MAF after deductible 60% of MAF after deductible
Mental Health and Substance AbuseRequires pre-authorization
80% of MAF after deductible 60% of MAF after deductible
Contracted Provider Non-Contracted Provider
summit Care
advantage Care
Preferred Care
MAF = Maximum Allowable Feenon-contracted providers may charge more than the MAF unless they have an agreement with you not to. Any amount above the MAF will be billed to you and will not count toward your deductible or out-of-pocket maximum.

PAGE 7 www.PEhP.orG
Weber State University 2013-2014 » Medical Benefits Grid » Advantage, Summit & Preferred Care
OutPatient faCility serviCes
Outpatient Facility and Ambulatory Surgery 80% of MAF after deductible 60% of MAF after deductible
Ambulance (ground or air) Medical emergencies only, as determined by PEHP
80% of MAF after deductible 80% of MAF after deductible
Emergency Room Medical emergencies only, as determined by PEHP.If admitted, inpatient facitlity benefit will be applied
80% of MAF, minimum $150 copayment per visit 80% of MAF, minimum $150 copayment per visit
Urgent Care Facility 100% of MAF after $45 copayment per visit 60% of MAF after deductible
University of Utah Medical Group Urgent Care FacilityPreferred Care only
100% of MAF after $50 copayment per visit Not applicable
Diagnostic Tests, X-rays, Minor For each test allowing $350 or less
80% of MAF after deductible 60% of MAF after deductible
Diagnostic Tests, X-rays, Major For each test allowing more than $350
80% of MAF after deductible 60% of MAF after deductible
Chemotherapy, Radiation, and Dialysis 80% of MAF after deductible 60% of MAF after deductible Dialysis with non-contracted providers requires pre-authorization
Physical and Occupational Therapy Requires pre-authorization after 8 visits per plan year
100% of MAF after applicable office copayment per visit
60% of MAF after deductible
PrOfessiOnal serviCes
Inpatient Physician Visits 100% of MAF after applicable office copayment per visit
60% of MAF after deductible
Surgery and Anesthesia 80% of MAF after deductible 60% of MAF after deductible
Primary Care Office Visits and Office Surgeries 100% of MAF after $25 copayment per visit 60% of MAF after deductible
Specialist Office Visits and Office Surgeries 100% of MAF after $35 copayment per visit 60% of MAF after deductible
University of Utah Medical Group Preferred Care only
100% of MAF after $50 copayment per visit Not applicable
Emergency Room Specialist 100% of MAF after $35 copayment per visit 100% of MAF after $35 copayment per visit
Diagnostic Tests, X-rays, Minor For each test allowing $350 or less
80% of MAF after deductible 60% of MAF after deductible
Diagnostic Tests, X-rays, Major For each test allowing more than $350
80% of MAF after deductible 60% of MAF after deductible
Mental Health and Substance Abuse No pre-authorization required for outpatient services. Inpatient services require pre-authorization
Outpatient: 100% of MAF after $35 copayment per visit Inpatient: 80% of MAF after deductible
Outpatient: 60% of MAF after deductibleInpatient: 60% of MAF after deductible
Contracted Provider Non-Contracted Provider
MAF = Maximum Allowable Feenon-contracted providers may charge more than the MAF unless they have an agreement with you not to. Any amount above the MAF will be billed to you and will not count toward your deductible or out-of-pocket maximum.
PAGE 8 www.PEhP.orG
Weber State University 2013-2014 » Medical Benefits Grid » Advantage, Summit & Preferred Care
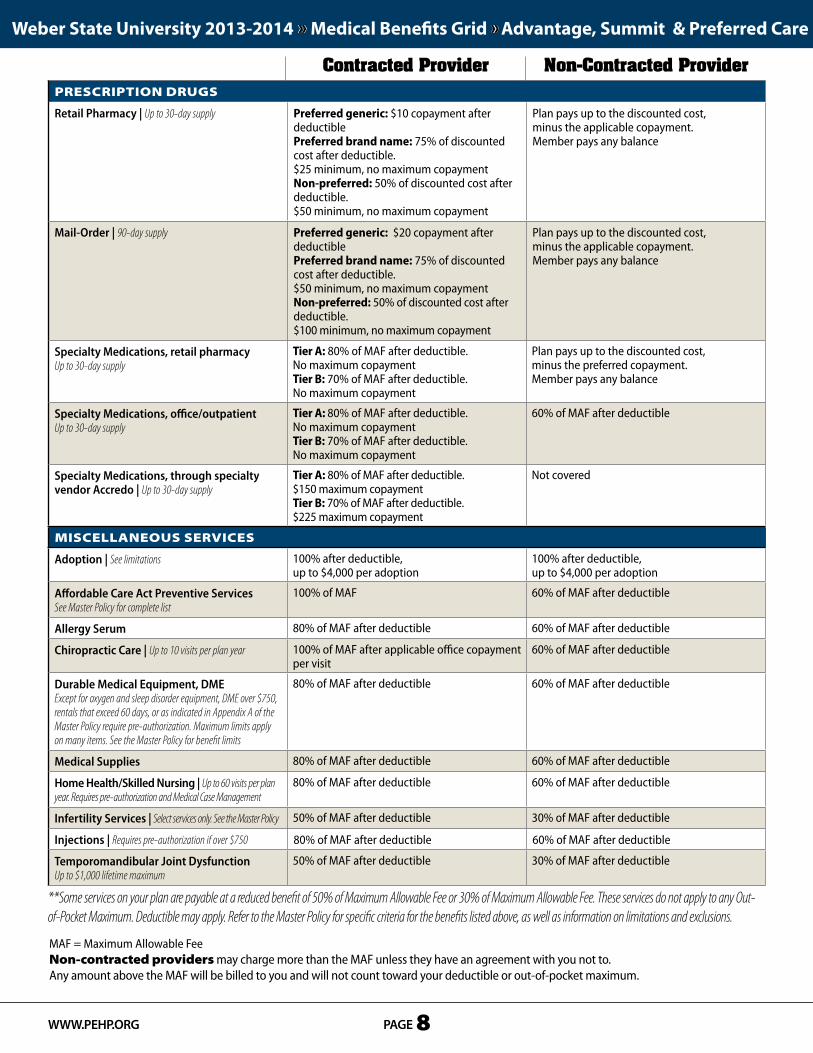
PresCriPtiOn drugs
Retail Pharmacy | Up to 30-day supply Preferred generic: $10 copayment after deductible Preferred brand name: 75% of discounted cost after deductible. $25 minimum, no maximum copaymentNon-preferred: 50% of discounted cost after deductible. $50 minimum, no maximum copayment
Plan pays up to the discounted cost,minus the applicable copayment.Member pays any balance
Mail-Order | 90-day supply Preferred generic: $20 copayment after deductible Preferred brand name: 75% of discounted cost after deductible. $50 minimum, no maximum copaymentNon-preferred: 50% of discounted cost after deductible. $100 minimum, no maximum copayment
Plan pays up to the discounted cost,minus the applicable copayment.Member pays any balance
Specialty Medications, retail pharmacy Up to 30-day supply
Tier A: 80% of MAF after deductible.No maximum copaymentTier B: 70% of MAF after deductible.No maximum copayment
Plan pays up to the discounted cost,minus the preferred copayment.Member pays any balance
Specialty Medications, office/outpatient Up to 30-day supply
Tier A: 80% of MAF after deductible.No maximum copaymentTier B: 70% of MAF after deductible.No maximum copayment
60% of MAF after deductible
Specialty Medications, through specialty vendor Accredo | Up to 30-day supply
Tier A: 80% of MAF after deductible.$150 maximum copaymentTier B: 70% of MAF after deductible.$225 maximum copayment
Not covered
misCellaneOus serviCes
Adoption | See limitations 100% after deductible, up to $4,000 per adoption
100% after deductible, up to $4,000 per adoption
Affordable Care Act Preventive ServicesSee Master Policy for complete list
100% of MAF 60% of MAF after deductible
Allergy Serum 80% of MAF after deductible 60% of MAF after deductible
Chiropractic Care | Up to 10 visits per plan year 100% of MAF after applicable office copayment per visit
60% of MAF after deductible
Durable Medical Equipment, DME Except for oxygen and sleep disorder equipment, DME over $750, rentals that exceed 60 days, or as indicated in Appendix A of the Master Policy require pre-authorization. Maximum limits apply on many items. See the Master Policy for benefit limits
80% of MAF after deductible 60% of MAF after deductible
Medical Supplies 80% of MAF after deductible 60% of MAF after deductible
Home Health/Skilled Nursing | Up to 60 visits per plan year. Requires pre-authorization and Medical Case Management
80% of MAF after deductible 60% of MAF after deductible
Infertility Services | Select services only. See the Master Policy 50% of MAF after deductible 30% of MAF after deductible
Injections | Requires pre-authorization if over $750 80% of MAF after deductible 60% of MAF after deductible
Temporomandibular Joint Dysfunction Up to $1,000 lifetime maximum
50% of MAF after deductible 30% of MAF after deductible
Contracted Provider Non-Contracted Provider
**Some services on your plan are payable at a reduced benefit of 50% of Maximum Allowable Fee or 30% of Maximum Allowable Fee. These services do not apply to any Out-of-Pocket Maximum. Deductible may apply. Refer to the Master Policy for specific criteria for the benefits listed above, as well as information on limitations and exclusions.
MAF = Maximum Allowable Feenon-contracted providers may charge more than the MAF unless they have an agreement with you not to. Any amount above the MAF will be billed to you and will not count toward your deductible or out-of-pocket maximum.

PAGE 9 www.PEhP.orG
Weber State University 2013-2014 » Medical Benefits Grid » Advantage & Summit STAR
The PEHP STAR Plan (HSA-Qualified)Refer to the applicable Master Policy for specific criteria for the benefits listed below, as well as information on limitations and Exclusions. * Services received by a non-contracted provider will be paid at a percentage of PEHP’s Maximum Allowable Fee (MAF). You will be responsible for your assigned coinsurance and deductible (if applicable). You will also be responsible for any amounts billed by a non-contracted provider in excess of PEHP’s Maximum Allowable Fee. There is no Out-of-Pocket Maximum for services received from a non-contracted provider.
deduCtibles, Plan maximums, and limits
Plan Year Deductible $1,500 single plan $3,000 double or family plan
Same as using a contracted provider*See Above for Additional Information
Plan Year Out-of-Pocket MaximumIncludes amounts applied to deductible and prescription drugs
$2,500 single plan $5,000 double plan $7,500 family plan
No Out of Network Out-of-Pocket Maximum*See Above for Additional Information
Maximum Lifetime Benefit None None
Pre-existing Condition Waiting Period Does not apply to any individuals up to age 19
9-month Waiting Period— waived or reduced with evidence of prior Creditable Coverage
9-month Waiting Period— waived or reduced with evidence of prior Creditable Coverage
inPatient faCility serviCes
Medical and Surgical | Requires pre-authorization 80% of MAF after deductible 60% of MAF after deductible
Skilled Nursing Facility | Non-custodial Up to 60 days per plan year. Requires pre-authorization through Medical Case Management
80% of MAF after deductible 60% of MAF after deductible
Hospice | Up to 6 months in a 3-year period. Requires pre-authorization through Medical Case Management
80% of MAF after deductible 60% of MAF after deductible
RehabilitationRequires pre-authorization through Medical Case Management
80% of MAF after deductible 60% of MAF after deductible
Mental Health and Substance AbuseRequires pre-authorization
80% of MAF after deductible 80% of MAF after deductible
Contracted Provider Non-Contracted Provider
summit Care*
advantage Care*
MAF = Maximum Allowable Feenon-contracted providers may charge more than the MAF unless they have an agreement with you not to. Any amount above the MAF will be billed to you and will not count toward your deductible or out-of-pocket maximum.
PAGE 10 www.PEhP.orG
Weber State University 2013-2014 » Medical Benefits Grid » Advantage & Summit STAR
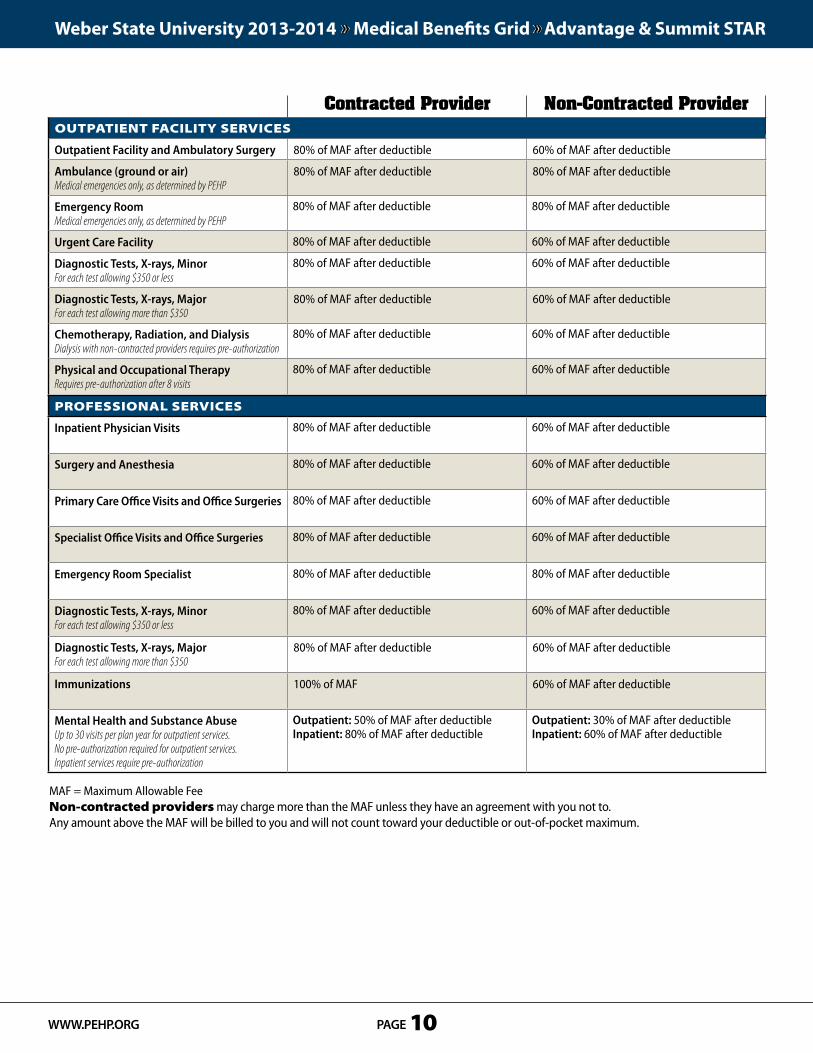
OutPatient faCility serviCes
Outpatient Facility and Ambulatory Surgery 80% of MAF after deductible 60% of MAF after deductible
Ambulance (ground or air) Medical emergencies only, as determined by PEHP
80% of MAF after deductible 80% of MAF after deductible
Emergency Room Medical emergencies only, as determined by PEHP
80% of MAF after deductible 80% of MAF after deductible
Urgent Care Facility 80% of MAF after deductible 60% of MAF after deductible
Diagnostic Tests, X-rays, Minor For each test allowing $350 or less
80% of MAF after deductible 60% of MAF after deductible
Diagnostic Tests, X-rays, Major For each test allowing more than $350
80% of MAF after deductible 60% of MAF after deductible
Chemotherapy, Radiation, and Dialysis Dialysis with non-contracted providers requires pre-authorization
80% of MAF after deductible 60% of MAF after deductible
Physical and Occupational Therapy Requires pre-authorization after 8 visits
80% of MAF after deductible 60% of MAF after deductible
PrOfessiOnal serviCes
Inpatient Physician Visits 80% of MAF after deductible 60% of MAF after deductible
Surgery and Anesthesia 80% of MAF after deductible 60% of MAF after deductible
Primary Care Office Visits and Office Surgeries 80% of MAF after deductible 60% of MAF after deductible
Specialist Office Visits and Office Surgeries 80% of MAF after deductible 60% of MAF after deductible
Emergency Room Specialist 80% of MAF after deductible 80% of MAF after deductible
Diagnostic Tests, X-rays, Minor For each test allowing $350 or less
80% of MAF after deductible 60% of MAF after deductible
Diagnostic Tests, X-rays, Major For each test allowing more than $350
80% of MAF after deductible 60% of MAF after deductible
Immunizations 100% of MAF 60% of MAF after deductible
Mental Health and Substance Abuse Up to 30 visits per plan year for outpatient services.No pre-authorization required for outpatient services. Inpatient services require pre-authorization
Outpatient: 50% of MAF after deductible Inpatient: 80% of MAF after deductible
Outpatient: 30% of MAF after deductibleInpatient: 60% of MAF after deductible
Contracted Provider Non-Contracted Provider
MAF = Maximum Allowable Feenon-contracted providers may charge more than the MAF unless they have an agreement with you not to. Any amount above the MAF will be billed to you and will not count toward your deductible or out-of-pocket maximum.

PresCriPtiOn drugs
Retail Pharmacy | Up to 30-day supply Preferred generic: $10 copayment after deductible Preferred brand name: 75% of discounted cost after deductible. $25 minimum, no maximum copaymentNon-preferred: 50% of discounted cost after deductible. $50 minimum, no maximum copayment
Plan pays up to the discounted cost after deductible, minus the applicable copayment.Member pays any balance
Mail-Order | 90-day supply Preferred generic: $20 copayment after deductible Preferred brand name: 75% of discounted cost after deductible. $50 minimum, no maximum copaymentNon-preferred: 50% of discounted cost after deductible. $100 minimum, no maximum copayment
Plan pays up to the discounted cost after deductible, minus the applicable copayment.Member pays any balance
Specialty Medications, retail pharmacy Up to 30-day supply
Tier A: 80% of MAF after deductible. No maximum copayment. Tier B: 70% of MAF after deductible. No maximum copayment.
Plan pays up to the discounted cost after deductible, minus the applicable copayment.Member pays any balance
Specialty Medications, office/outpatient Up to 30-day supply
Tier A: 80% of MAF after deductible. No maximum copayment. Tier B: 70% of MAF after deductible. No maximum copayment.
60% of MAF after deductible
Specialty Medications, through specialty vendor Accredo Up to 30-day supply
Tier A: 80% of MAF after deductible. $150 maximum copayment. Tier B: 70% of MAF after deductible.$225 maximum copayment.
Not covered
misCellaneOus serviCes
Adoption | See limitations 100% after deductible, up to $4,000 per adoption
100% after deductible, up to $4,000 per adoption
Affordable Care Act Preventive ServicesSee Master Policy for complete list
100% of MAF 60% of MAF after deductible
Allergy Serum 80% of MAF after deductible 60% of MAF after deductible
Chiropractic Care | Up to 10 visits per plan year 80% of MAF after deductible 60% of MAF after deductible
Durable Medical Equipment, DME Except for oxygen and sleep disorder equipment, DME over $750, rentals that exceed 60 days, or as indicated in Appendix A of the Master Policy require pre-authorization. Maximum limits apply on many items. See the Master Policy for benefit limits
80% of MAF after deductible 60% of MAF after deductible
Medical Supplies 80% of MAF after deductible 60% of MAF after deductible
Home Health/Skilled Nursing Up to 60 visits per plan year. Requires pre-authorization and Medical Case Management
80% of MAF after deductible 60% of MAF after deductible
Infertility Services Select services only. See the Master Policy for details
50% of MAF after deductible 30% of MAF after deductible
Injections Requires pre-authorization if over $750
80% of MAF after deductible 60% of MAF after deductible
Temporomandibular Joint Dysfunction Up to $1,000 lifetime maximum
50% of MAF after deductible 30% of MAF after deductible
Contracted Provider Non-Contracted Provider
MAF = Maximum Allowable Feenon-contracted providers may charge more than the MAF unless they have an agreement with you not to. Any amount above the MAF will be billed to you and will not count toward your deductible or out-of-pocket maximum.
Weber State University 2013-2014 » Medical Benefits Grid » Advantage & Summit STAR
PAGE 11 www.PEhP.orG

Weber State University has established a supplemental plan with PEHP to cover members whose individual out-of-pocket pharmacy costs exceed $2,000 during the plan year.
While the State pharmacy out-of-pocket maximum is $3,000, Weber State’s supplemental coverage will cap your qualified out-of-pocket pharmacy expenses at $2,000 per individual per plan year.
Out-of-pocket costs that apply to this supplemental coverage include preferred generic drugs, preferred brand name drugs, and preferred specialty medications obtained through the pharmacy benefit.
Out-of-pocket costs that are not eligible for supplemental coverage include non-preferred drugs, the cost difference between generic drug and brand name drugs when a substitute is available, and specialty medications obtained through the medical benefit.
Meeting your deductible » It is PEHP’s discounted cost of an eligible medication that is applied toward the deductible.
» Once the deductible is met, you are responsible to pay the applicable copayment or coinsurance.
Meeting your pharmacy out-of-pocket Maximum » Your Pharmacy deductible does apply to the pharmacy
out-of-pocket maximum.
» If your pharmacy deductible is applied to the purchase of a non-preferred medication, it does not apply to the out-of-pocket maximum because non-preferred medications do not apply to the pharmacy out-of-pocket maximum.
» Once your pharmacy deductible is met, your pharmacy copayments or coinsurances are applied to your pharmacy out-of-pocket maximum.
Weber StateSupplemental Pharmacy
Weber State University 2013-2014 » Benefits Preview » Supplemental Pharmacy
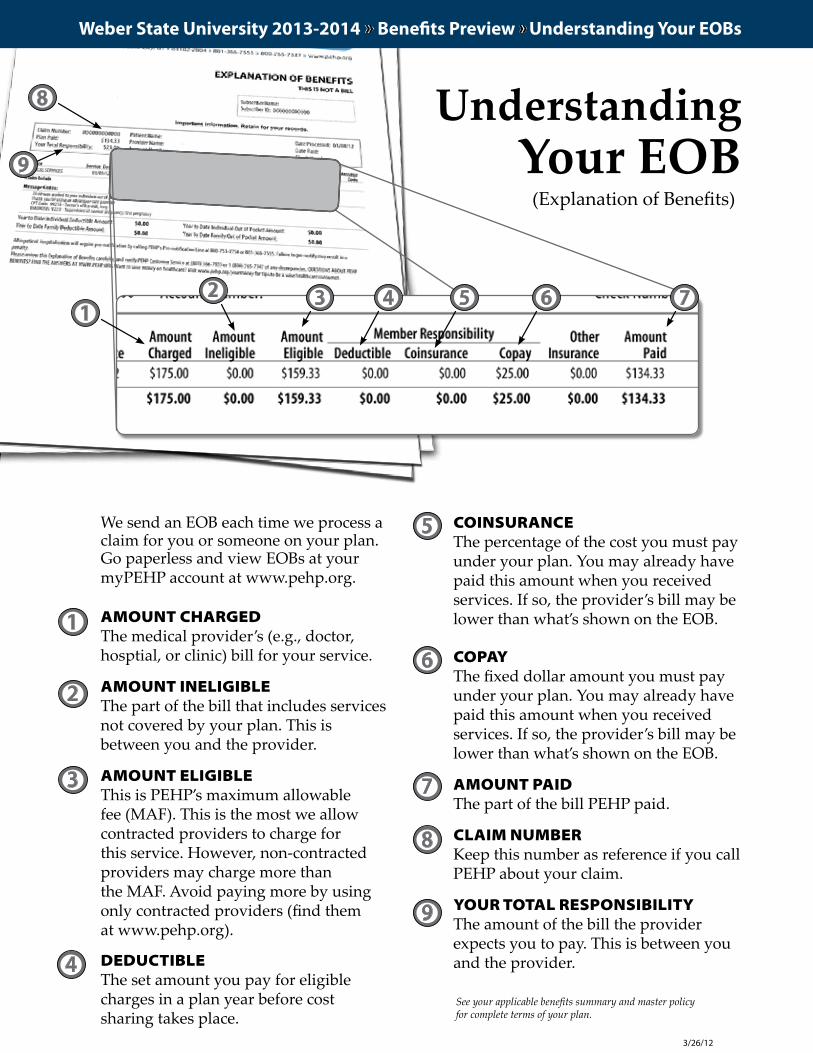
We send an EOB each time we process a claim for you or someone on your plan. Go paperless and view EOBs at your myPEHP account at www.pehp.org.
AMOUNT CHARGEDThe medical provider’s (e.g., doctor, hosptial, or clinic) bill for your service.
AMOUNT INELIGIBLEThe part of the bill that includes services not covered by your plan. This is between you and the provider.
AMOUNT ELIGIBLEThis is PEHP’s maximum allowable fee (MAF). This is the most we allow contracted providers to charge for this service. However, non-contracted providers may charge more than the MAF. Avoid paying more by using only contracted providers (find them at www.pehp.org).
DEDUCTIBLEThe set amount you pay for eligible charges in a plan year before cost sharing takes place.
COINSURANCEThe percentage of the cost you must pay under your plan. You may already have paid this amount when you received services. If so, the provider’s bill may be lower than what’s shown on the EOB.
COPAYThe fixed dollar amount you must pay under your plan. You may already have paid this amount when you received services. If so, the provider’s bill may be lower than what’s shown on the EOB.
AMOUNT PAIDThe part of the bill PEHP paid.
CLAIM NUMBERKeep this number as reference if you call PEHP about your claim.
YOUR TOTAL RESPONSIBILITYThe amount of the bill the provider expects you to pay. This is between you and the provider.
1
2
3
5
6
Understanding Your EOB
2 3 4 5 6 7
4
7
8
9
1
8
9
3/26/12
(Explanation of Benefits)
See your applicable benefits summary and master policy for complete terms of your plan.
Weber State University 2013-2014 » Benefits Preview » Understanding Your EOBs
Weber State University 2013-2014 » Benefits Preview » myPEHP
during OPen enrOllment, yOu Can aCCess Online enrOllment. yOu Can alsO aCCess yOur Claims histOry, exPlanatiOn Of benefits (eOb) and COverage levels Online at my PehP.
You can enroll, access claims history, download explanation of benefits (EOB), check coverage levels, and much more by logging on to myPEHP.
Here’s how to set up your personal account:
SteP 1: Go to www.pehp.org
SteP 2: Locate the “myPEHP Login” on the right side of the page. The first time you log in, you must create an account. Once you have successfully set up your profile, enter your user ID and password into the boxes to access your information.
SteP 3: To set up an account, click on “Create my PEHP account.” You must agree to the conditions detailed in the document on the next page to proceed. Once you have read and agreed to the terms,
click “I Agree” to continue creating your personal profile.
SteP 4: Enter your Social Security number, date of birth, and PEHP subscriber ID number to verify your identity. The 16-digit subscriber ID number can be found on your Medco/PEHP insurance card. If you do not have the number, call PEHP or fill out the online request to receive your ID number in the mail. Then, you will be asked to select a user name and password for future access.
Once you have successfully logged in, you are ready to enroll during open enrollment. You will also see a summary of all the plans you have enrolled in, a detailed list of all claims submitted to PEHP, and PDF files of your EOBs. You may also update your mailing address. However, if you wish to make any other changes outside of annual enrollment to your existing plans, you must submit a signed Change Form to PEHP.
StePS FOR ONLINe eNROLLMeNt: See next page.
Graphical website depictions may vary from actual website.
How to Set Up Your myPEHP Account
Weber State University 2013-2014 » Benefits Preview » Online Enrollment
Graphical website depictions may vary from actual website.
How to Enroll OnlineDuring open enrollment, if you’re not adding or deleting dependents or changing benefit plans, you don’t need to re-enroll. You must re-enroll in FLEX$ every year.During open enrollment, online enrollment is available
to active employees who have PEHP medical coverage. Early retirees, COBRA, and LTD enrollees must complete a paper enrollment form to make any plan changes.During open enrollment, online enrollment for FLEX$ is
available only if you have been previously enrolled in medical and FLEX$. Otherwise, you must complete a paper enrollment form.New employees must complete enrollment forms for all plans.
SteP 1: Log in to your myPEHP account. See instructions on the previous page about how to create yours.
SteP 2: If you’re a returning user, you’ll be directed to the myPEHP main page. During open enrollment, you will have access to online enrollment through a link on the menu at left.
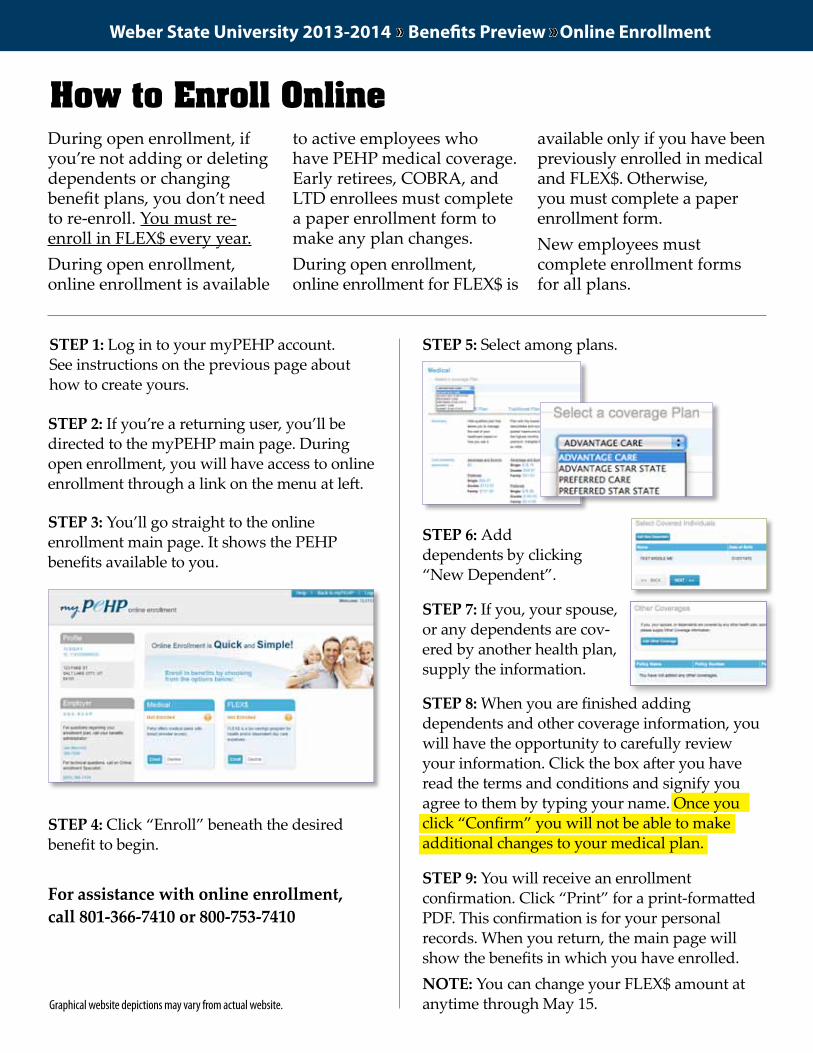
SteP 3: You’ll go straight to the online enrollment main page. It shows the PEHP benefits available to you.
SteP 4: Click “Enroll” beneath the desired benefit to begin.
SteP 6: Add dependents by clicking “New Dependent”.
SteP 7: If you, your spouse, or any dependents are cov-ered by another health plan, supply the information.
SteP 8: When you are finished adding dependents and other coverage information, you will have the opportunity to carefully review your information. Click the box after you have read the terms and conditions and signify you agree to them by typing your name. Once you click “Confirm” you will not be able to make additional changes to your medical plan.
SteP 9: You will receive an enrollment confirmation. Click “Print” for a print-formatted PDF. This confirmation is for your personal records. When you return, the main page will show the benefits in which you have enrolled.NOte: You can change your FLEX$ amount at anytime through May 15.
SteP 5: Select among plans.
For assistance with online enrollment, call 801-366-7410 or 800-753-7410


















