Alcohol and Drug Assessments for Clergy and Pastoral Counselors. Los Angeles Metropolitan Churches African American Alcohol & Other Drug Council (AAAOD) and UCLA – Integrated Substance Abuse Programs Pacific Southwest Addiction Technology Training Center Faith Based Training Series - PowerPoint PPT Presentation
Los Angeles Metropolitan Churches African American Alcohol & Other Drug Council (AAAOD) and UCLA – Integrated Substance Abuse Programs Pacific Southwest Addiction Technology Training Center Faith Based Training Series Trainer: Cheryl A. Branch, MS March 16, 2013 Alcohol and Drug Assessments for Clergy and Pastoral Counselors
Transcript
Los Angeles Metropolitan Churches African American Alcohol & Other Drug Council (AAAOD)and UCLA – Integrated Substance Abuse ProgramsPacific Southwest Addiction Technology Training CenterFaith Based Training SeriesTrainer: Cheryl A. Branch, MS
March 16, 2013
Alcohol and Drug Assessments for Clergy and Pastoral Counselors
AgendaI: Open & Welcome – Cheryl A. Branch, PSATTC Trainer
-Reinforce participants understanding about alcohol and drug assessment and
screening using evidence-based practices and tools that will enable clergy and laity to
practice new science in addiction and alcohol treatment and to encourage faith communities in LAC to become users of
SAMHSA/CSAT TAPs and TIPs.
Big Picture Goals• To build a new breed of faith-based
organizations and churches in South LA through “developmental technical assistance” to guide their growth and development.
• In order to become providers of health and human services in their community FBOs must understand the rules of non-profit business and evidenced based programming in AOD services/counseling.
Big Picture Goals
• To Accelerate the dissemination of evidence-based practices into faith-based community practices in South LA.
• Particular focus on faith based agencies that work with offender populations (prison ministries).
TRAINING
Why Screen & Assess?
Screening, clinical assessment, and determining a client's readiness for treatment represent the beginning of the treatment process.
NIDA Risk Factors
• Unstable home environment due to parental substance abuse or mental illness
• Fractured relationship of parents and adolescent/child• Poor level of supervision of the adolescent's activities• Peer use of drugs• Liberal parental attitude of their own drug use or
adolescent's use of drugs
Screening Definition• The process by which the client is determined
appropriate and eligible for admission to a particular program.
• Screening Instruments – Screening instruments are the objective arm of the
screening procedure, providing uniformity, quality control, and structure to the process. Some instruments may be more appropriate than others in certain settings. Among the more commonly used instruments are the CAGE questionnaire, the MAST, and the OPI.
Assessment Tools• CAGE (alcohol)• ASI (Addiction Severity Index)/CJ ASI• Screening, Brief Intervention Referral to Treat
• Visit: CSAT Inventory of Effective Substance Abuse Treatment Practiceshttp://csat.samhsa.gov/treatment
ScreeningGlobal Criteria
1. Evaluate psychological, social and physiological signs and symptoms of alcohol and drug abuse.
2. Determine the client’s appropriateness for admission.3. Determine the client’s eligibility for admission or referral.4. Identify any co-existing conditions (medical, psychiatric,
physical, etc.) that indicate need for additional professional assessment and/or service.
5. Adhere to applicable laws, regulations and agency policies governing alcohol and other drug abuse services.
The CAGE Questionnaire
• The CAGE questionnaire is a simple but effective test designed to screen for alcohol abuse. It consists of four questions: 1. Have you ever felt the need to Cut down on your
drinking? 2. Do you feel Annoyed by people complaining
about your drinking? 3. Do you ever feel Guilty about your drinking? 4. Do you ever drink an Eye-opener in the morning
to relieve the shakes?
The Michigan Alcoholism Screening Test
• The MAST is a frequently used test that is more detailed than the CAGE questionnaire. The MAST consists of 25 questions and can be used during longer interviews or in holding and confinement situations. It is a commonly used indicator of alcoholism.
The Offender Profile Index • The OPI measures the client's drug use severity as well as his
or her "stakes in conformity" within a variety of contexts: family support, education, and school involvement; work, home, and correctional history; psychological and treatment history; drug use severity; and HIV-risk behaviors.
• It can be administered in about 30 minutes by an experienced probation officer, counselor, or other trained clinician.
• It includes a straightforward grading guide to help interpret the seriousness of an AOD abuser's problem. A day of training is required to be able to administer it, and a training manual is available. The client's numerical score has a corresponding treatment recommendation.
National Standards• TAP 21 - Addiction Counseling Competencies: The
Knowledge, -Skills and Attitudes of -Professional Practice
• In an effort to maximize certification Standards in the State of California, while elevating the level of professionalism within the field, AAAOD and LAM uses national standards for substance abuse counseling to educate FB counselors.
Intake Definition
• The administrative and initial assessment procedures for admission
IntakeGlobal Criteria
6. Complete required documents for admission to the program.
7. Complete required documents for program eligibility and appropriateness.
8. Obtain appropriately signed consents when soliciting from or providing information to outside sources to protect client confidentiality and
9. Rights.
Orientation Definition
Describing to the client the following: • general nature and goals of the program;• rules governing client conduct and • infractions that can lead to disciplinary action or
discharge from the program; • in a non-residential program the hours during which
services are available; • treatment costs to be borne by the client, if any and
rights
Orientation
Global Criteria
9. Provide an overview to the client by describing program goals and objectives for client care.
10. Provide an overview to the client by describing program rules and client obligations and rights.
11. Provide an overview to the client of program operations.
Assessment Definition
• The procedures by which a counselor/program identifies and evaluates an individual’s strengths, weaknesses, problems and needs for the development of a treatment plan.
Interrelationships between stages of screening,
assessment, and treatment
Foundation of Assessment• What in client’s story can you connect to as
counselor?• Who they are?• What they really want?• What do they really need/when are ready?• Importance of honesty for staff & clients• Empathetic connections with clients-values
Foundation of Assessment
• Importance of initial meeting– Story/Strength based discussion– What place/time in life was the person doing
really well• Identify that time period and “Begin” there • Identify strengths & capacity from that time
Role of Motivational Interviewing Techniques
• Advancing problem recognition, readiness for action, treatment suitability (availability and accessibility), and influences that lead to coercive pressure to seek treatment.
Understanding Self-Efficacy In Assessment
• Self–efficacy, or the confidence in personal ability, has been shown to predict a variety of health behavior outcomes (O’Leary 1985; Grembowski et al. 1993), including alcohol treatment outcome (Miller and Rollnick 1991).
• Self–efficacy may increase attention to goal attainment; thus it is important to measure goal setting and achievement, as well as other constructs believed to underlie self–efficacy, such as the client’s perceptions of personal ability to overcome barriers to change (Miller 1983).
Strength Based Model
• There are strengths & capacity within that time period of stability– Diagnostic goldmine for ASSESSMENT
• Utilize that time period for:– Screening– Building blocks for assessment– Building blocks for treatment planning
Foundation of Assessment
• Change the way we think about people• Build something that is right and different• Practice boundaries and ethics• How well do we know people through
strength-based screenings and assessment
Knowledge, Skills, Attitudes
• Transdisciplinary Foundations – identify the knowledge and attitudes that underlie competent practice
• Skills may vary across disciplines but the knowledge and attitudes provide a basis of understanding that should be common to all addiction professionals
Transdisciplinary Foundations
(A) Understanding Addiction
(B) Treatment Knowledge
(C) Application to Practice
(D) Professional Readiness
8 Practice Dimensions
Clinical evaluation (assessment/interview)Treatment planningReferralService coordinationCounselingClient, family and community educationDocumentationProfessional and ethical responsibilities
IV. Professional ReadinessIII. Application to PracticeII. Treatment Knowledge I. Understanding Addiction
Dimensions of Professional Practice
Addiction Counseling Competencies:The Knowledge, Skills and Attitudes of Professional Practice
Clin
ical
Eva
luat
ion
Tre
atm
ent P
lann
ing
Ref
erra
lR
efer
ral
Ser
vice
Coo
rdin
atio
n
Cou
nsel
ing
Clie
nt, F
amily
, &C
omm
unity
Edu
catio
n
Doc
umen
t ati o
n
Pro
fess
iona
l & E
thic
alR
espo
nsib
ilitie
s
Transdisciplinary Foundations
I II III IV V VI VII VIII
Clinical Evaluation (Screening & Assessment)
ScreeningIntakeOrientationAssessment
Knowledge, Skills, Attitudes 12 Core Functions
SBIRT
Screening
1. Screening is a quick, simple way to identify patients who need further assessment or treatment for substance use disorders.
2. It does not establish definitive information about diagnosis and possible treatment needs.
3. The goal of SBIRT is to make screening for substance abuse a routine part of medical care
Screening Process• A screen should be simple enough that it
can be administered by a wide range of health professionals.
• It should focus on the substance use severity (primarily consumption patterns) and a core group of associated factors such as legal problems, mental health status, educational functioning, and living situation.
Screening Process
• The client's awareness of the problem, feelings about his or her substance use, and motivation for changing behavior may also be solicited.
Brief Intervention • Brief intervention is a single session or multiple
sessions of motivational discussion focused on increasing insight and awareness regarding substance use and motivation toward behavioral change.
• Brief intervention can be tailored for variance in population or setting and can be used as a stand-alone treatment for those at-risk as well as a vehicle for engaging those in need of more extensive levels of care.
Brief Treatment• Brief treatment is a distinct level of care and is inherently
different from both brief intervention and specialist treatment.
• Brief treatment is provided to those seeking or already engaged in treatment who acknowledge problems related to substance use.
• Brief treatment in relation to traditional or specialist treatment has increased intensity and is of shorter duration. It consists of a limited number of highly focused and structured clinical sessions with the purpose of eliminating hazardous and/or harmful substance use.
Referral To Treatment• Referral to specialized treatment is provided to
those identified as needing more extensive treatment than offered by the SBIRT program.
• The effectiveness of the referral process to specialty treatment is a strong measure of SBIRT success and involves a proactive and collaborative effort between SBIRT providers and those providing specialty treatment to ensure access to the appropriate level of care.
Screening Instruments
• Three commonly used screening instruments are:
1. Alcohol Use Disorders Identification Test (AUDIT)
2. Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST)
• — a screening tool developed by the World Health Organization to identify persons whose alcohol consumption has become hazardous or harmful to their health. It is a 10-item screening questionnaire with 3 questions on the amount and frequency of drinking, 3 questions on alcohol dependence, and 4 on problems caused by alcohol. All of the questions are scored using a 5-point Likert scale.
Alcohol, Smoking and Substance Involvement Screening Test
• — an instrument developed for the World Health Organization (WHO) by an international group of substance abuse researchers to detect and manage substance use and related problems in primary and general medical care settings.
The Drug Abuse Screening Test (DAST)
• — DAST was designed to provide a brief instrument to detect drug abuse or dependence disorders. The DAST provides a general measure of lifetime problem severity that can be used to guide further inquiry into drug-related problems and to help determine treatment intensity.
BASICS
• Brief Alcohol Screening and Intervention of College Students (BASICS): A Harm Reduction Approach, is a preventive intervention for college students 18 to 24 years old.
• It is aimed at students who drink alcohol heavily and have experienced or are at risk for alcohol-related problems such as poor class attendance, missed assignments, accidents, sexual assault, and violence.
• BASICS is conducted over the course of only two interviews, and these brief, limited interventions prompt students to change their drinking patterns.
• Dimeff, L. A., Baer, J. S., Kivlahan, D. R., & Marlatt, G. A. (1999). Brief Alcohol Screening and Intervention for College Students (BASICS): A harm reduction approach. New York, NY: The Guilford Press.
Principles of Effective Treatment
Principles of Effective Treatment”First things first”
1. No single treatment is appropriate for all2. Treatment needs to be readily available3. Effective treatment attends to the multiple
needs of the individual4. Treatment plans must be assessed and
modified continually to meet changing needs5. Remaining in treatment for an adequate
period of time is critical for treatment effectiveness
Principles of Effective Treatment6. Counseling and other behavioral therapies
are critical components of effective treatment
7. Medications are an important element of treatment for many patients
8. Co-existing disorders should be treated in an integrated way
9. Medical detox is only the first stage of treatment
10. Treatment does not need to be voluntary to be effective
11. Possible drug use during treatment must be monitored continuously
12. Treatment programs should assess for HIV/AIDS, Hepatitis B & C, Tuberculosis and other infectious diseases and help clients modify at-risk behaviors
13. Recovery can be a long-term process and frequently requires multiple episodes of treatment
- NIDA (1999) Principles of Drug Addiction Treatment
Principles of Effective Treatment
Get Over the Barriers!Get Over the Barriers!• Administrative philosophy
• Organizational policy
• System structure
• Unclear literature
• Agency staff
• Client population
????????So, how do you decide what to do?
So, how do you decide what to do?
What Is Our Goal?
• To provide persistent, incremental improvements in the quality and effectiveness of substance abuse treatment which results in better quality recovery for more people.
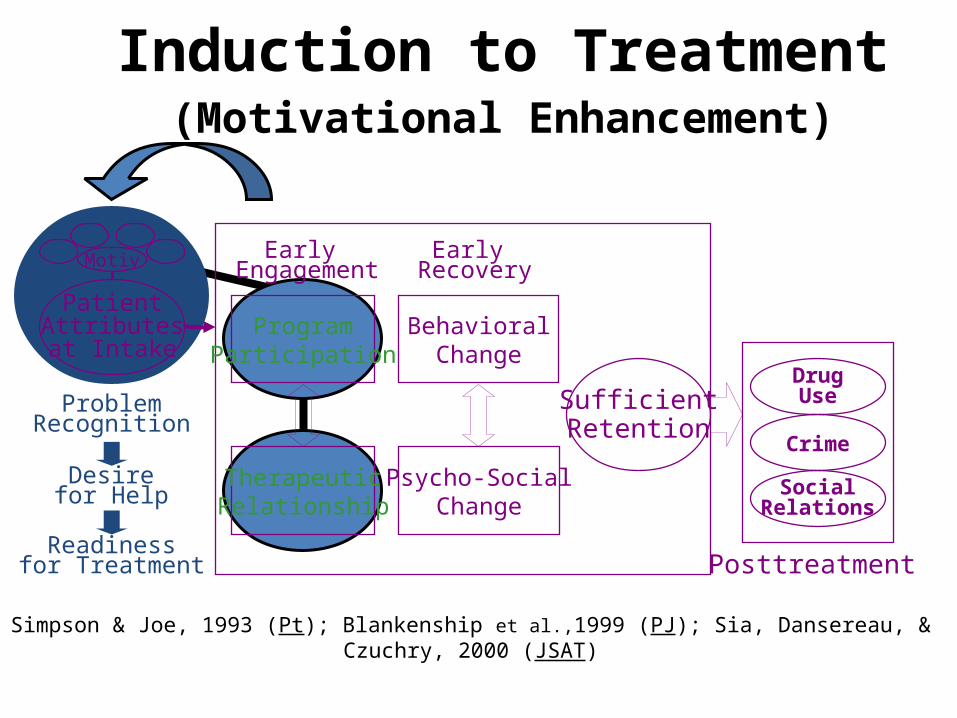
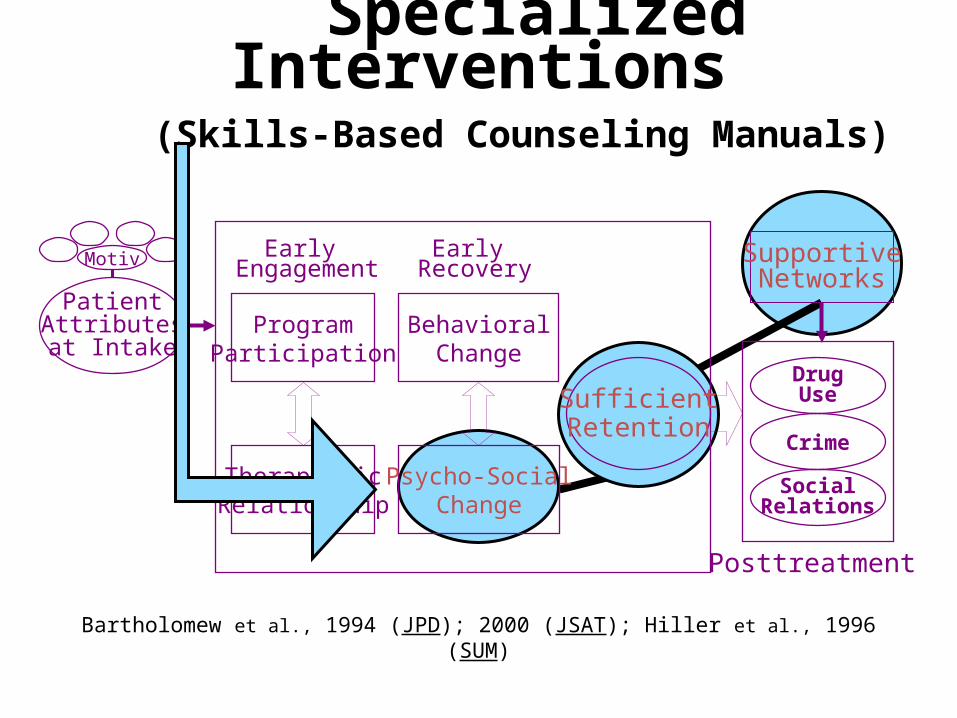
Bartholomew et al., 1994 (JPD); 2000 (JSAT); Hiller et al., 1996 (SUM)
SupportiveNetworks
SufficientRetentionSufficientRetention
Early Engagement
Early Recovery
Posttreatment
DrugUse
DrugUse
CrimeCrime
SocialRelations
SocialRelations
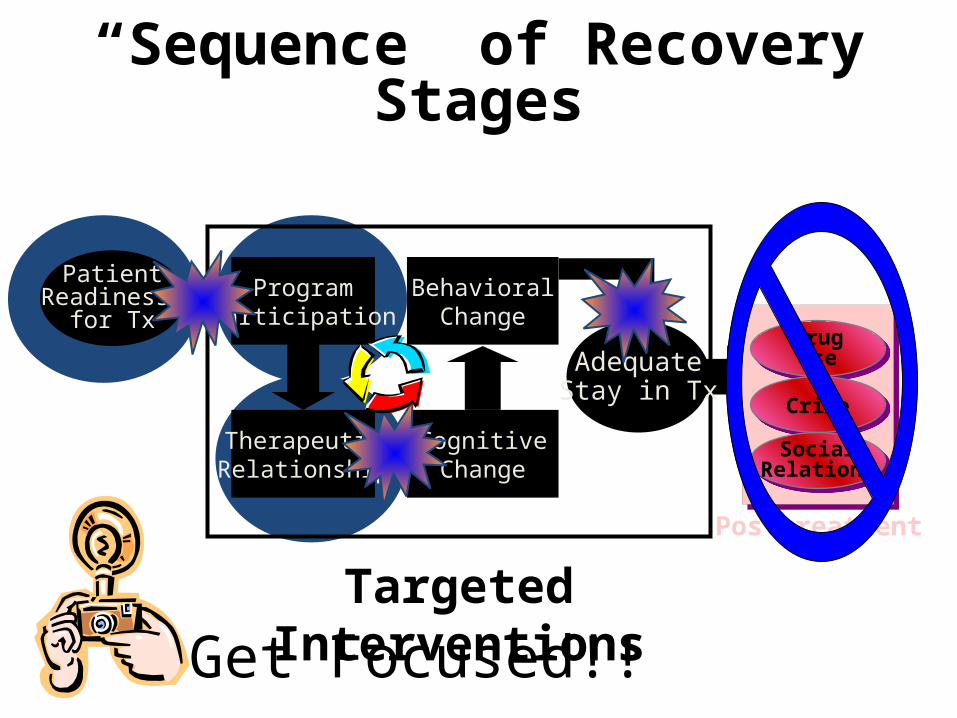
ProgramParticipation
ProgramParticipation
TherapeuticRelationship
TherapeuticRelationship
BehavioralChange
BehavioralChange
Psycho-SocialChange
Psycho-SocialChange
PatientAttributesat Intake
PatientAttributesat Intake
Motiv
Evidence-Based Treatment Model
EnhancedCounseling
BehavioralStrategies
Social SkillsTraining
Family &Friends
SupportiveNetworks
SupportiveNetworks
Induction Personal Health Services
Social Support Services
ProgramCharacteristics
ProgramCharacteristics
StaffAttributes
& Skills
StaffAttributes
& Skills
Simpson, 2001 (Addiction)
Resources:
1.Brief Interventions and Brief Therapies for Substance Abuse SAMHSA TIP #34 provides rich resources for varied and diverse provision of brief intervention.
2.Brief Interventions and Brief Therapies for Substance Abuse SAMHSA TIP #34 provides rich resources for varied and diverse provision of brief treatment.
3.The NNED is supported by the Substance Abuse and Mental Health Services Administration, National Institutes of Health/National Center on Minority Health and Health Disparities, and the Annie E. Casey Foundation