LOWER LIMB AMPUTATIONS AND PROSTHESES: EXPERIENCE OF THE « VIVRE DEBOUT » CENTRE, ABIDJAN B.K. Manou 1 , A-L Pillah 1 , J. Bombo 1 , A. D. Alloh 1 , J. Kouakou 1 , D Akadje 1 , Tano 1 M, A. Coulibaly 2 , E.K.Konaté A Cissé 2 , B.M Nandjui 1
Transcript
LOWER LIMB AMPUTATIONS AND PROSTHESES:
EXPERIENCE OF THE « VIVRE DEBOUT » CENTRE, ABIDJAN
B.K. Manou1, A-L Pillah1, J. Bombo1, A. D. Alloh1, J. Kouakou1, D Akadje1, Tano1 M, A. Coulibaly2, E.K.Konaté A Cissé2, B.M Nandjui1
INTRODUCTION (1)
• The Prosthetic Centre of Abidjan « Vivre Debout » has existed since 2000. – Handicap International Belgium, European Union and
Belgium cooperation.– Expanded the competancy pf the Medical and Physical
rehabilitationwhich functioned previously in physiotherapy only
• large large range of equipment including lower limbprostheses
INTRODUCTION (2)
PRC = responds to the need for rehabilitation for the increasing number amputees + provision of prostheses‐ Due to: ‐ Cardiovascular accidents
‐ Military/political conflicts(in 2002 et 2011).
Material used = thermoformable plastic, polypropylène (PPP), which is resistant to a tropical climate which is hot and humid
The objectives of PRC are: Produce and maintain orthopaedic equipment and technical aids at affordable costs ‐ a technology adapted to the environment of the Ivory Coast. Promote the training of professionals in the field of equipment and physical rehabilitationPromote the establishment of centres and institutions for equipment throughout the country
PLAN
• INTRODUCTION• OBJECTIVE OF THE STUDY• MATERIALS AND METHODS• RESULTS• DISCUSSION• CONCLUSION
OBJECTIVE
Our study examined the production capacity of prosthetic devices of PRC in order to identify its competence and limitations in supervising ortho‐prosthetic technology
MATERIALS AND METHODS(1) Type: a retrospective descriptive study from 2008 to 2012
Location: « Vivre Débout » prosthetics service centre of MPR
Inclusion criteria: ‐ All amputees , regardless of age , who have been examined and have received a lower limb prosthesis during this period
Exclusion criteria:‐ Amputees not fitted because of severe orthopaedic complications‐ Patients fitted with prostheses outwith the centre who had come for repair and/or adjustment of their prostheses
MATERIAL AND METHODS(2)
• VARIABLES STUDIED: Age, sex, cause of amputation, type of protheses made, date of amputation, date of production and delivery
• DATA ANALYSIS: Epi info version 2000
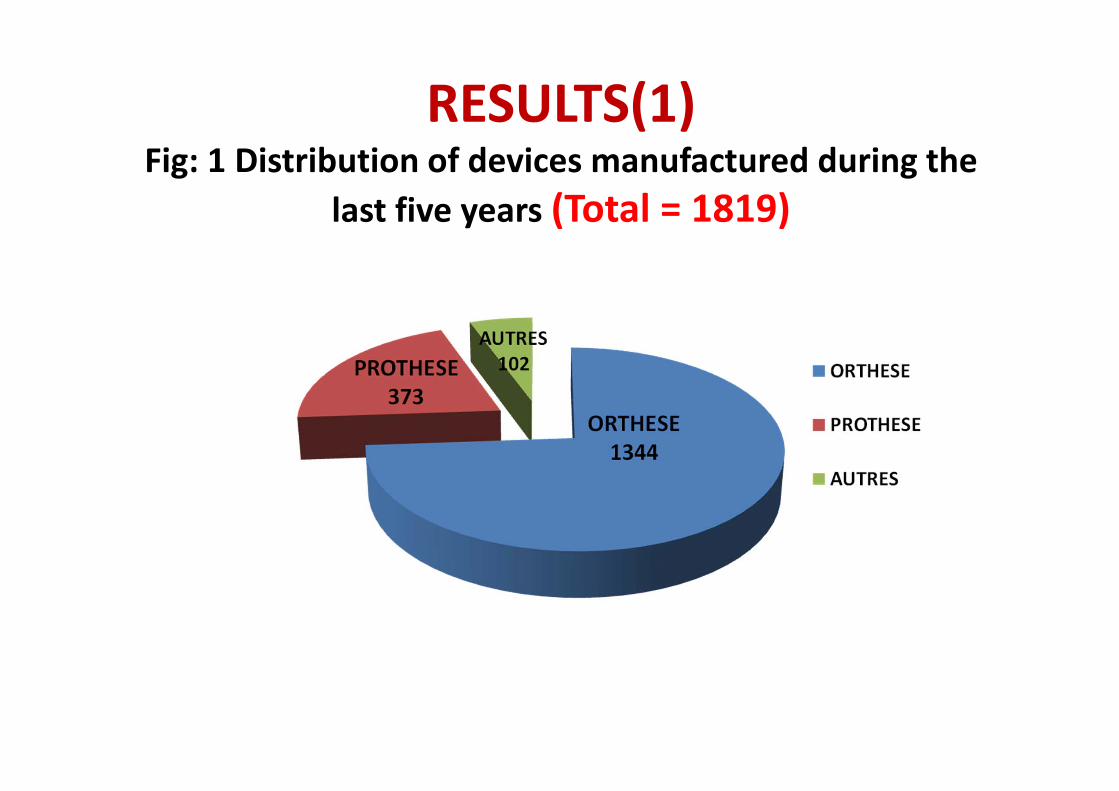
RESULTS(1)Fig: 1 Distribution of devices manufactured during the
last five years (Total = 1819)
RESULTS (2)
Patients fitted at PCR
Number = 373 people withamputations 230 Men (61.7%) 143 Women (38.3%)
Sex ratio = 1.6:1 male:female
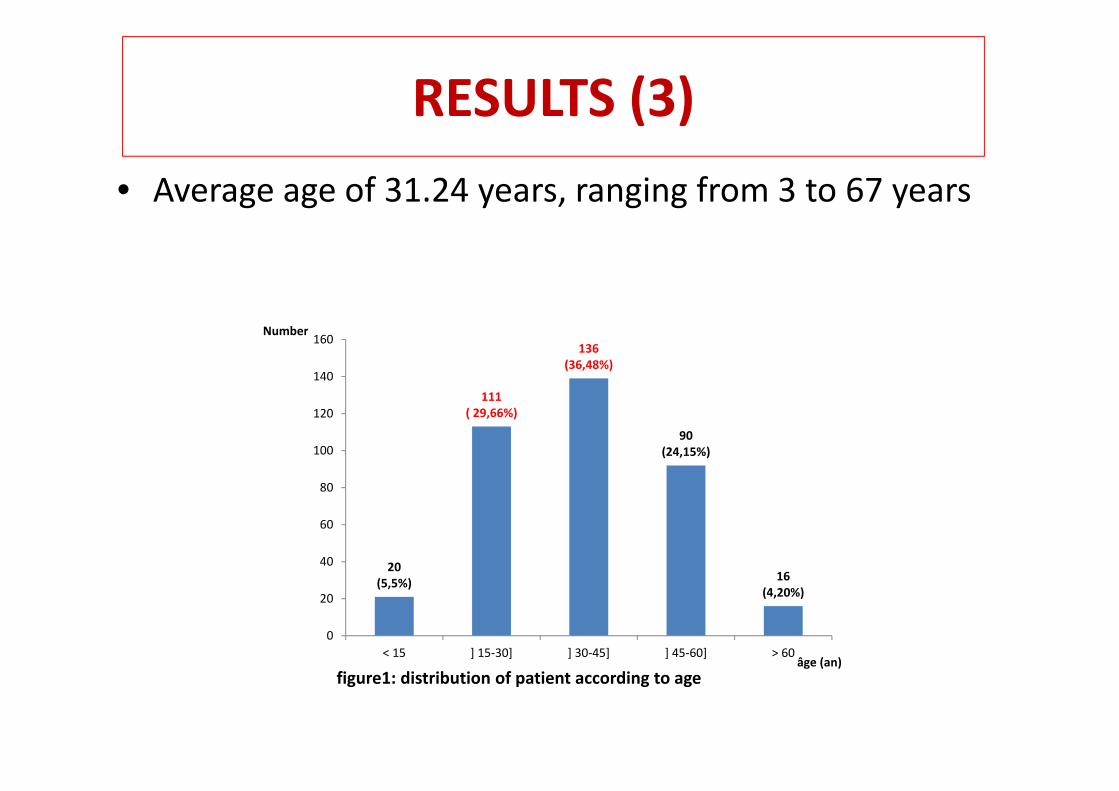
RESULTS (3)• Average age of 31.24 years, ranging from 3 to 67 years
20(5,5%)
111( 29,66%)
136(36,48%)
90(24,15%)
16(4,20%)
0
20
40
60
80
100
120
140
160
< 15 ] 15‐30] ] 30‐45] ] 45‐60] > 60
Number
âge (an)figure1: distribution of patient according to age
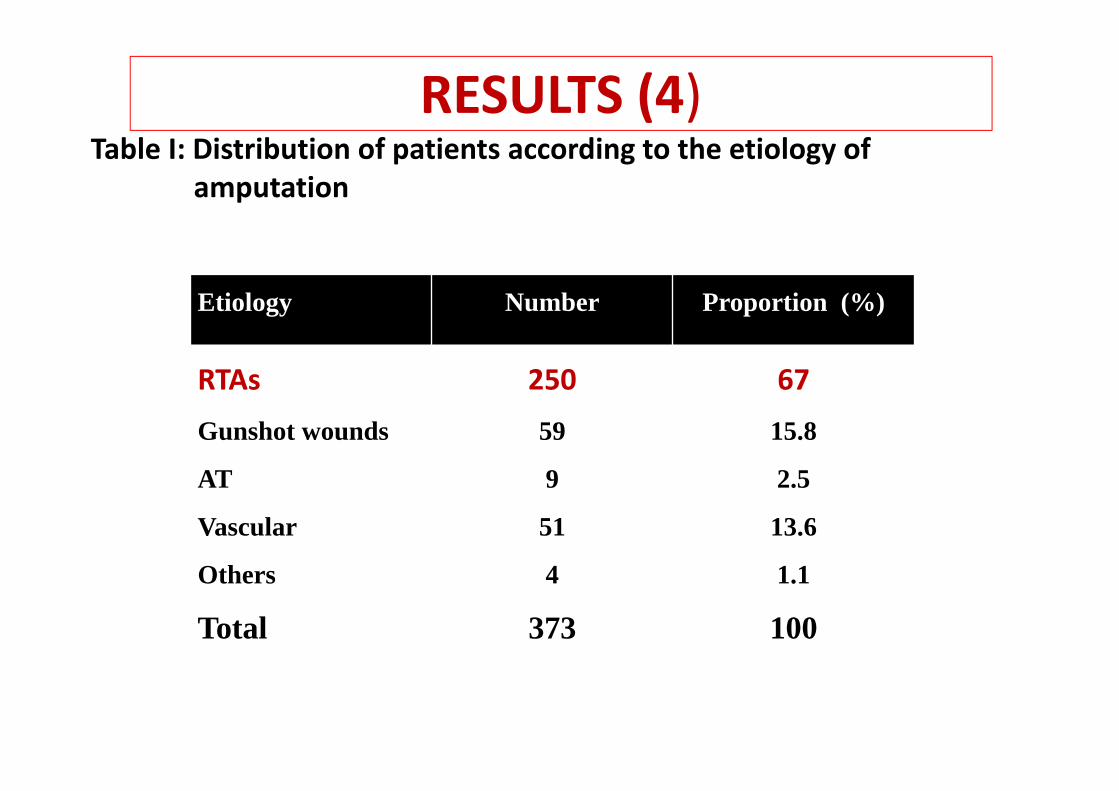
RESULTS (4)Table I: Distribution of patients according to the etiology of
amputation
Etiology Number Proportion (%)
RTAs 250 67
Gunshot wounds 59 15.8
AT 9 2.5
Vascular 51 13.6
Others 4 1.1
Total 373 100
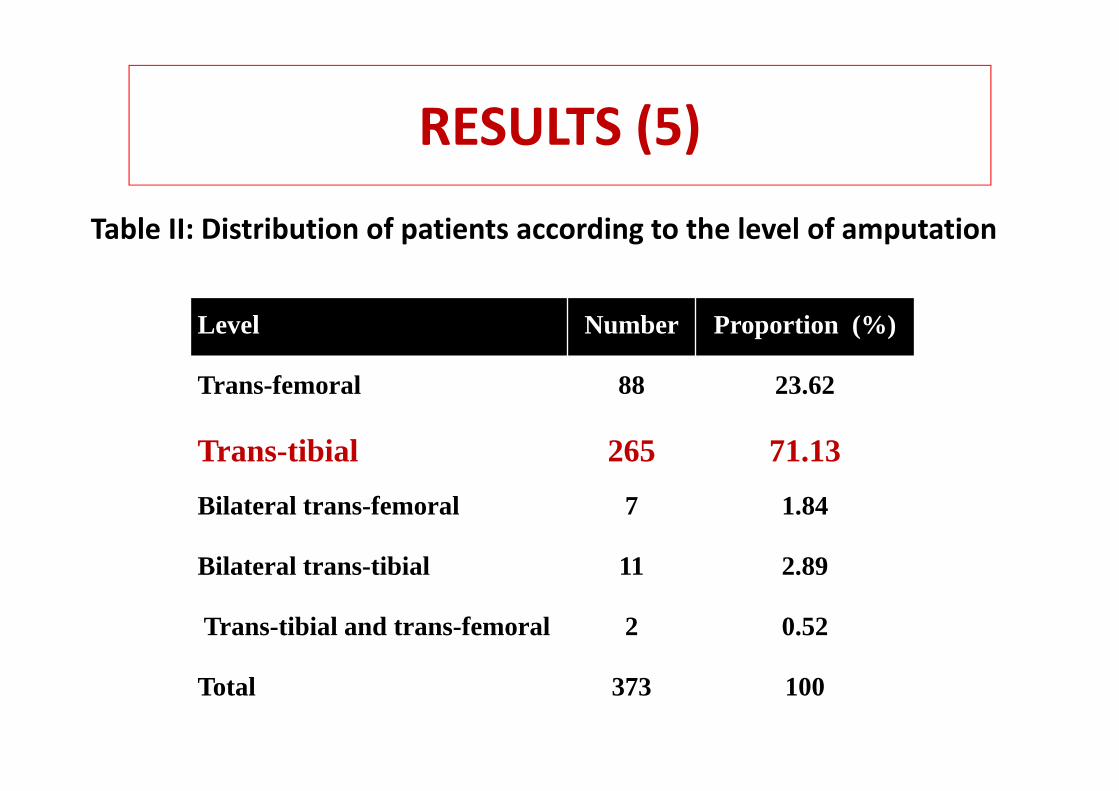
RESULTS (5)
Table II: Distribution of patients according to the level of amputation
Level Number Proportion (%)
Trans-femoral 88 23.62
Trans-tibial 265 71.13
Bilateral trans-femoral 7 1.84
Bilateral trans-tibial 11 2.89
Trans-tibial and trans-femoral 2 0.52
Total 373 100
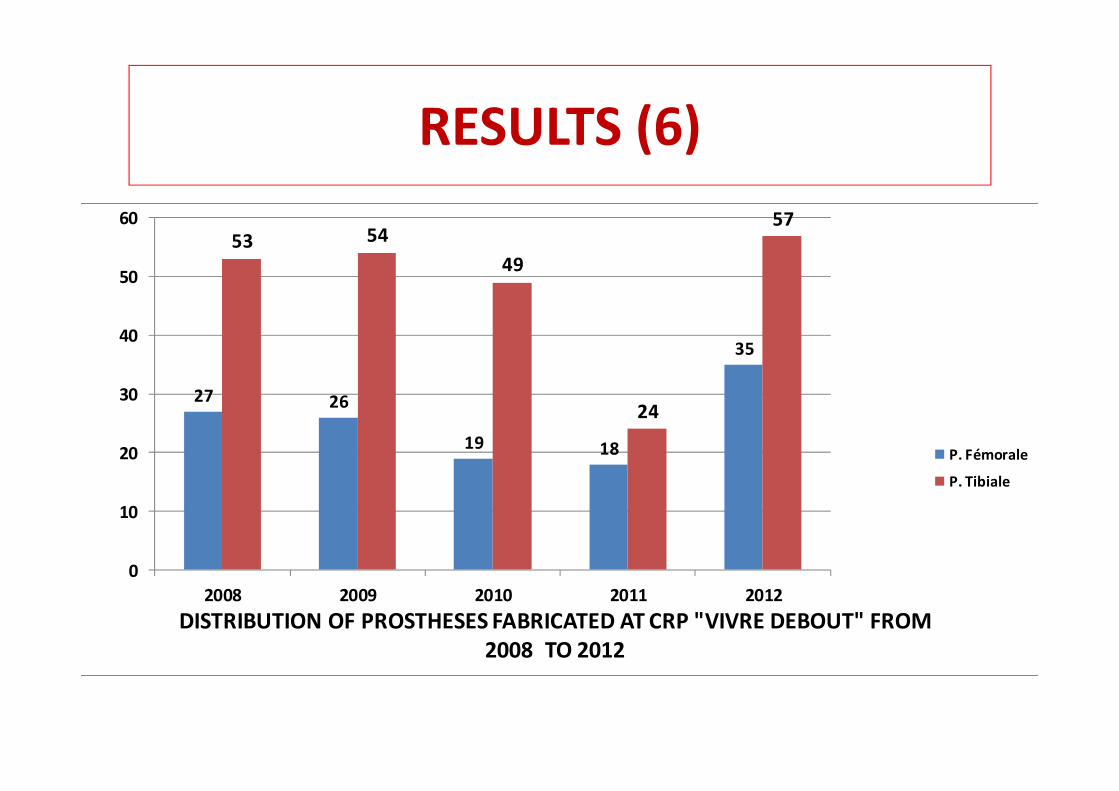
RESULTS (6)
27 26
19 18
35
53 5449
24
57
0
10
20
30
40
50
60
2008 2009 2010 2011 2012DISTRIBUTION OF PROSTHESES FABRICATED AT CRP "VIVRE DEBOUT" FROM
2008 TO 2012
P. Fémorale
P. Tibiale
RESULTS (7)
• Average time of manufacture:‐Trans‐femoral prosthesis: 21 days (extremes 11 to 30 days)
‐Trans‐tibial prostheses: 15 days (extremes 7 to 25 days)
• Delivery time:‐Trans‐femoral prosthesis: 30 to 45 days‐Trans‐tibial prosthesis: 25 to 35 days
Discussion (1)LIMITATIONS OF THE STUDY
– Strictly hospital data and cannot be extrapolated to all amputees in the Ivory Coast
– However, it gives us an idea of the epidemiological profile of amputees in Africa because some of our findings are consistent with previously published data
DISCUSSION (2)AGE• Age ranges
‐ 15‐30 years = 111 (29.66%) ‐ 30‐45 years = 136 (36.48%).
Mean age = 31.24 years• These results are:
‐ NASDAB, UK (2004‐2005) 54% of of the amputeesare over the age of 65years
‐ In Tunisia, MEZGHANI‐MASMOUDI found the amputee population to be young
DISCUSSION (3)• These young amputees are in full occupation and mostly have had an amputation due to road traffic accidents or work accidents
• 05.5% amputations due to trauma occurred in children under 15 years of age
• These child amputees pose problems of bone/ soft tissue growth, resulting in revision operations and difficulties in fitting
DISCUSSION (4)SEX146 are male (61.67%) ‐ a sex ratio of 1.6:1• MEZGHANI‐MASMOUDI, DILLINGHAM, GERMANAUD, BRUNEL all reported a male predominance
• Our results indicated the that the populationat risk in our professional context were men in high risk occupations
• However, women amputees working outside were often victims of road traffic accidents
.
DISCUSSION (5)ETIOLOGY OF AMPUTATIONS
RTAs = is the cause of more than 1/3 of amputations Car: ‐ saturation and dilapidated road network ‐ indiscipline and breach of the highway code‐ Young and inexperienced drivers
PVD: is the cause of amputation in more than 80% of cases
DISCUSSION (6)LEVEL OF AMPUTATION75% of amputations are at the trans‐tibial levelthe trans‐tibial prothesis:
‐ ease of fabrication, ‐ good possibilities for walking‐greater energy cost
The bilateral amputees at trans‐tibial and trans‐femoral levels‐fitted without difficulty‐ but difficulties with ambulation
CONCLUSION (1)
• The "Vivre Debout" centre in the long term plans to become a reference centre in the field of orthopedic device production in the Ivory Coast and the sub‐region.
CONCLUSION (2)
• To maintain accessibility in the cost of these devices to all social strata , the centre seeks partners to provide technical and/or financial support in the activities of the centre and the training of technicians