Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center LTBI Conundrums: Illustrative Cases 1 LTBI Conundrums John Bernardo Boston University School of Medicine Massachusetts Department of Public Health Objectives • Review concepts of Infection, Latency • Cases – Understand: – How can new tools help the decision process? – MDR exposures? – What can be done to encourage adherence to treatment? Adapted from: Shaler, CR, et al. Clin Dev Immunol. 2012 TB disease progression and major events leading to protection “window” time time
Transcript
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 1
LTBI Conundrums
John Bernardo Boston University School of Medicine Massachusetts Department of Public
Health
Objectives
• Review concepts of Infection, Latency
• Cases – Understand:
– How can new tools help the decision process?
– MDR exposures?
– What can be done to encourage adherence to treatment?
Adapted from: Shaler, CR, et al. Clin Dev Immunol. 2012
TB disease progression and major events leading to protection
“window” time time
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 2
Primary TB
- Delayed-type Hypersensitivity develops 8-10wk post-infection: TST or IGRA-positive
Latency of M. tuberculosis
• Environment of granuloma favors altered metabolism: • Low pO2 • Reduced CHO • High Fat
• Replication time >>> 20hr. • Loss of acid fast staining properties • Mechanism(s) unknown
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 3
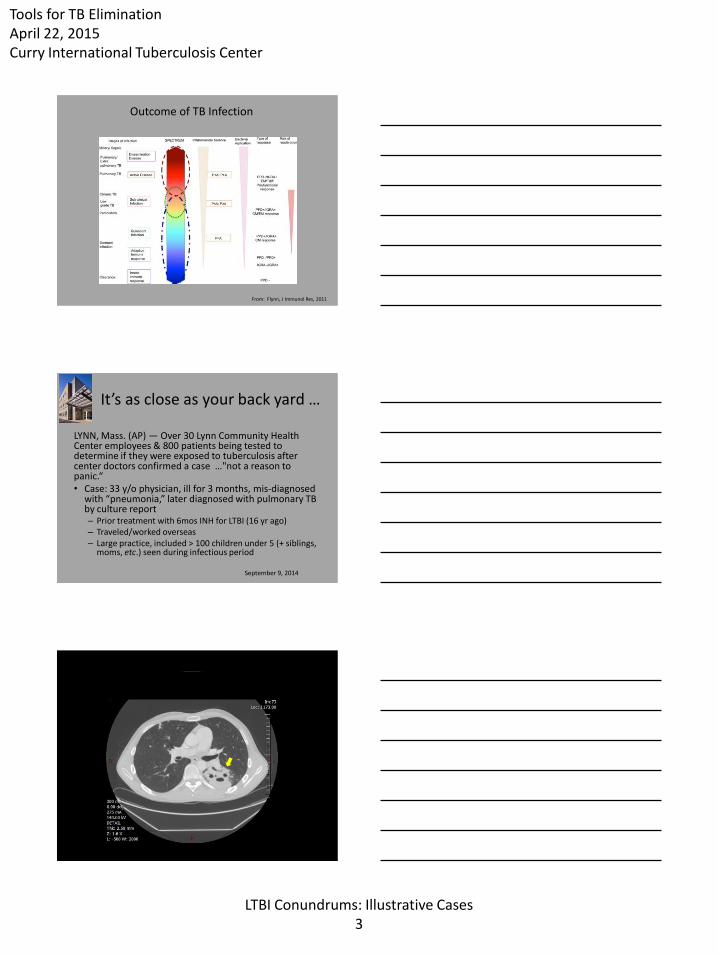
From: Flynn, J Immunol Res, 2011
Outcome of TB Infection
It’s as close as your back yard …
LYNN, Mass. (AP) — Over 30 Lynn Community Health Center employees & 800 patients being tested to determine if they were exposed to tuberculosis after center doctors confirmed a case …"not a reason to panic.“ • Case: 33 y/o physician, ill for 3 months, mis-diagnosed
with “pneumonia,” later diagnosed with pulmonary TB by culture report – Prior treatment with 6mos INH for LTBI (16 yr ago) – Traveled/worked overseas – Large practice, included > 100 children under 5 (+ siblings,
moms, etc.) seen during infectious period
September 9, 2014
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 4
Lynn CHC: Contact Investigation
• What do we know? – Patient was surprised!
• Did not even Think TB
– Smear negative/Culture positive • But that was 4 weeks ago (time spt was obtained for culture) • NAAT was not done
– Cavitary disease and coughing • Tried to limit cough when with patients
– DST pending • Recall travel, previous INH: Is this Drug Resistant disease?
– 17% of MA cases with isolates are resistant to at least 1 drug – 7 MA cases MDR in 2013
Special Considerations
• Only one MD at LCHC is trained in TB – Required collaboration and intervention by DPH
• Extensive Contact Investigation was announced – Family, patients and staff at health center: ?focus
• Children <5 y/o were of special concern – Often develop severe forms of TB forms with grave
– CXR: Nodular LUL infiltrate, new since 10/2014 film
– Admitted to respiratory isolation
– Sputum smear-POS (<1 organism/hpf), GeneXpert®MTB/RIF POS, Rif R
• Family support? – None; community associates and friends refused to
help (like care for child, …)
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 9
CT Same Day
What Now?
• Child (now 12 mos old)
– Had spent whole life with Mom (now sm POS; molecular test POS for Rif-R)
– NOT on treatment (TST now 4mm, IGRA neg)
– Looks and behaves well: Examination normal
– CXR (PA and Lat) negative
– TREAT??
– Repeat referral to RTMCC
• Continue to watch; repeat evaluation in 10 weeks
So?
• Child continued to be seen weekly – Remained well, no treatment – DPH arranged day care while Dad returned to work
• Laboratory – Confirmed Mom’s isolate as MDR TB, same DST as Dad’s
• At 10 weeks (March, 2015) – Examination: normal – CXR (PA and Lat): normal – TST and IGRA: negative
– Whew! (April, 2015) – We hope!! Child continues to be seen frequently
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 10
In the Beginning…In a TB Clinic Long, Long Ago…...
• 8 y/o Haitian female (USA-born) presents in the TB clinic 4/88
– Referral from a local NHC; school screening
• TST reported as “positive”
• No symptoms, normal examination
• CXR (PA and Lat) -negative
• Patient recommended for INH treatment
Follow-up…
• None; patient was non-adherent. Lost
• Returns to clinic two years later (3/90) to restart preventive therapy
• No symptoms, normal growth and development;
• No change in x-ray from previous film (4/88)
• Adherence issues reinforced
• Patient returns to clinic monthly and completes therapy in 6 months
Back to the Future……...
• November, 1997: Patient now 18 y/o presents in Pedi ED – Cough x one month, fever, night sweats
– CXR-RUL infiltrate
• Patient admitted to Pedi – Placed on respiratory Isolation
– Initial sputum AFB smears 4+ positive
– Culture +MTB • Pan-susceptible
• Refused to believe diagnosis of TB!
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 11
It Just Gets Better……..
• Family of household contacts agree to screening – Mother (TST- ) – Sister (6 y/o; TST-) – Girlfriend living with family (TST-)
• 3 m/o infant (TST 10mm)
• Infant evaluated at Clinic – Examination normal – CXR (PA and Lat) normal – Placed on INH - with DOT by PHN
• Suddenly…
– Girlfriend and infant disappear – Family have no knowledge of her whereabouts – Child was lost to follow-up UNTIL …
Two Years Later …
• Notified from Children’s Hospital (3/99) – 2 y/o girl admitted with TB meningitis
• Original 3 mos old household contact who moved
• RUL infiltrate
• Blind
– Her Mom • Cough x 2 months
• CXR: RUL infiltrate and cavity
• Child and Mom started on treatment – Relocated to another state
Classic Approach to TB Prevention
• Scheduled initial appointment at TB Clinic – Patients have no prior understanding of TB prevention – Process
• Intake – Personal information; risk assessments
• Medical evaluation – Chest x-ray; physical examination
• Treatment recommendation – I am the doctor; you are the patient – 1 month supply of medications; ? Costs, co-pays
• Monthly follow-up visits – Usually at-convenience of clinic
• Lots of defaults (DNKA) – Low completion rates
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 12
TB Prevention in the Private Sector
• Providers are not well-educated about TB – Unfamiliar with current standards
• Varying links to expertise in TB and public health – Many non-U.S. trained physicians hold native beliefs about TB
and its prevention (e.g. BCG) • TB prevention is not a priority
– Other health issues usually prevail • Few resources are available to patients
– Most lack health insurance coverage for TB prevention • Coverage for CXR, drugs, …
– Varying links to public health • Poor acceptance of principles of TB prevention among
providers and community
Cultural Approach to TB Prevention
• Tailoring approaches to health care to accommodate community beliefs, perceptions, and needs can be successful – AIDS and community approaches (Africa) – Cultural case management of LTBI (Seattle)
• Hypothesis: Improving community acceptance of TB prevention will result in increased numbers of infected persons completing treatment for LTBI – This will translate to lower incidence of disease in the
community
Cultural Approach to TB Prevention
• Understanding
• Trust
• Accessibility
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 13
Community-Based TB Prevention, Boston
Original model; utilized community health centers in neighborhoods with high rates of TB – 75 - 80% of Massachusetts TB cases are non-U.S. born
– Multi-cultural approach, relied on health center staff to provide community link
– Based on program of • assessment of community understanding, beliefs, health practices
• assessment of health center needs, systems of operation
• continuous provider education/training
• community education and information
• patient referral to the public health clinic, and
• monitoring of therapy in the community
1996; TBAA, NHLBI HL-33035
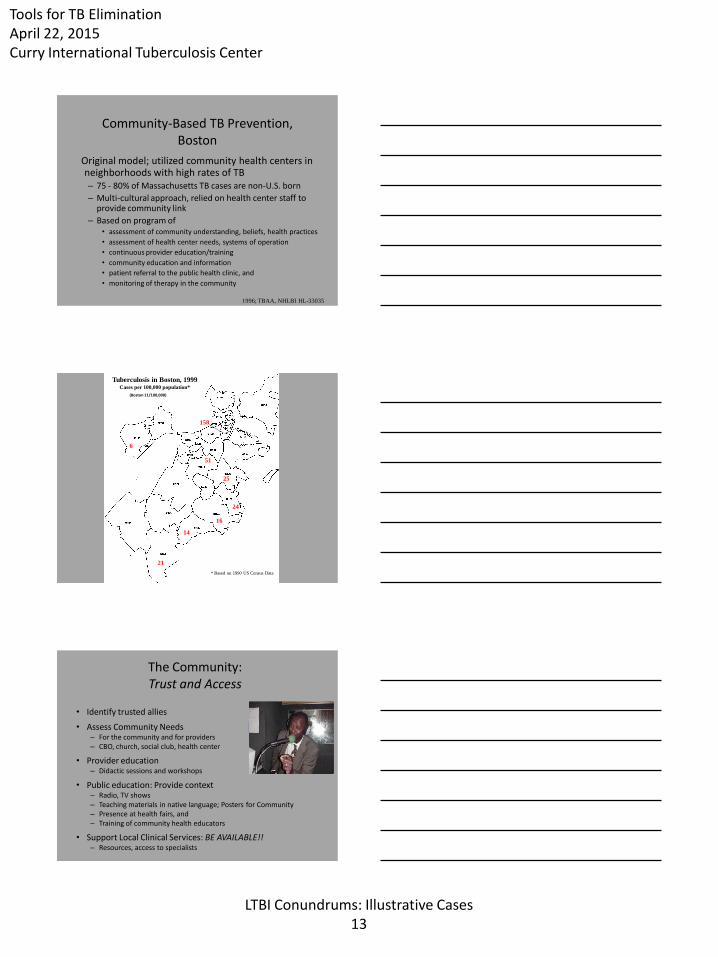
158
51
24
25
21
16
14
Tuberculosis in Boston, 1999 Cases per 100,000 population*
* Based on 1990 US Census Data
6
(Boston 11/100,000)
The Community: Trust and Access
• Identify trusted allies
• Assess Community Needs – For the community and for providers – CBO, church, social club, health center
• Provider education – Didactic sessions and workshops
• Public education: Provide context – Radio, TV shows – Teaching materials in native language; Posters for Community – Presence at health fairs, and – Training of community health educators
• Support Local Clinical Services: BE AVAILABLE!! – Resources, access to specialists
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 14
It always comes down to….
• EDUCATION…
• EDUCATION…
• EDUCATION…
Community-Based TB Prevention
Neighborhood Health Center BMC-TB Clinic
PPD + Evaluation
- Chest Radiograph
- Medical evaluation by Pulmonary MD, BUSM
- Baseline LFT’s
- TB/HIV education (HIV counseling/testing)
- Follow-up appointment at NHC
Monthly follow-up at NHC
- Assess adherence
- Evaluate for side effects
- Address other health care issues
- Reinforce TB education
- Dispense medications (DOPT if necessary)
- Forward documentation to TB Program Monitor
- Monthly evaluations, provide medications
- Completion of therapy for LTBI
- Feedback to NHC
- Education program for NHC staff
1996; TBAA, NHLBI HL-33035
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 15
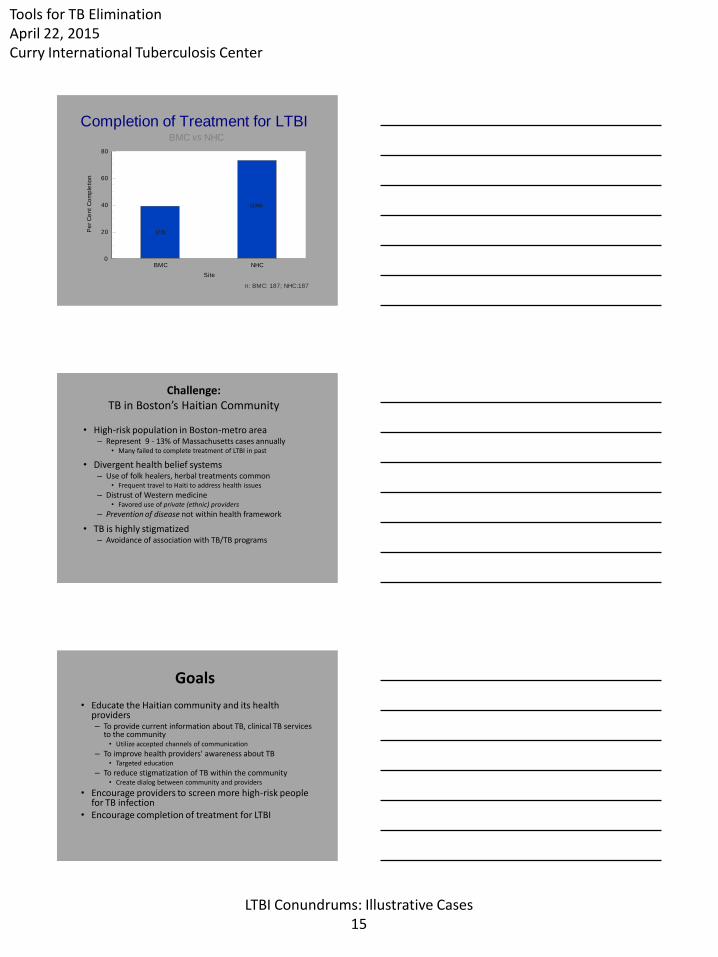
Completion of Treatment for LTBIBMC vs NHC
n: BMC: 187; NHC:187
BMC NHC
Site
0
20
40
60
80
Pe
r C
en
t C
om
ple
tio
n
(73)
(136)
Challenge: TB in Boston’s Haitian Community
• High-risk population in Boston-metro area – Represent 9 - 13% of Massachusetts cases annually
• Many failed to complete treatment of LTBI in past
• Divergent health belief systems – Use of folk healers, herbal treatments common
• Frequent travel to Haiti to address health issues
– Distrust of Western medicine • Favored use of private (ethnic) providers
– Prevention of disease not within health framework
• TB is highly stigmatized – Avoidance of association with TB/TB programs
Goals
• Educate the Haitian community and its health providers – To provide current information about TB, clinical TB services
to the community • Utilize accepted channels of communication
– To improve health providers' awareness about TB • Targeted education
– To reduce stigmatization of TB within the community • Create dialog between community and providers
• Encourage providers to screen more high-risk people for TB infection
• Encourage completion of treatment for LTBI
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 16
Selected Findings: Metro Boston’s Haitian Community
• TB is more stigmatizing than AIDS – Often viewed as a curse or a test from God
• No framework for “latent infection” – Treatment without symptoms = experimentation
• Translated words may carry different semantics – “Positive” PPD is common in Haiti; is a good thing
• Indicates that BCG is working
• Medications are dangerous – Not “natural;” represent pollutant chemicals – Liquid “safer” than pills – US medicines are appropriate for Americans, not for them
• Mistrust of American physicians/systems – Blood test for LTBI (QFT) may be accepted if presented by their doctor
• Health belief system is complex; poor health literacy – Secular, religious, mystical/supernatural forces
Selected Findings: Metro Boston’s Haitian Community
• Acceptance of program’s objectives by Haitian Community, providers
– Focus group findings: Annie E. Casey Foundation
• Acceptance translates to CHC model
– Focus group findings: TBESC Task Order 12
• Need to re-approach model
– In order to improve TB prevention in high risk communities
Rocket Science?
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 17
TB and the Homeless
Priorities
• Early diagnosis of infectious cases – Remove suspects from environment
– Early treatment of active cases: Shattuck Hospital
• Identification of high-risk infected persons: targeted testing – Case contacts, medical co-morbidities
• Treatment of MTB infection – Prioritize effective treatments and settings: TB Clinic,
Primary Care
Principles
• Take it to the clients –
– On their turf and their terms: Education, clinical
• Listen to their concerns and priorities
– Structure interventions around their life activities
• Treat people with respect
– Develop a dialog; understand their problems
• Public Health is Personal!
Tools for TB Elimination April 22, 2015 Curry International Tuberculosis Center
LTBI Conundrums: Illustrative Cases 18
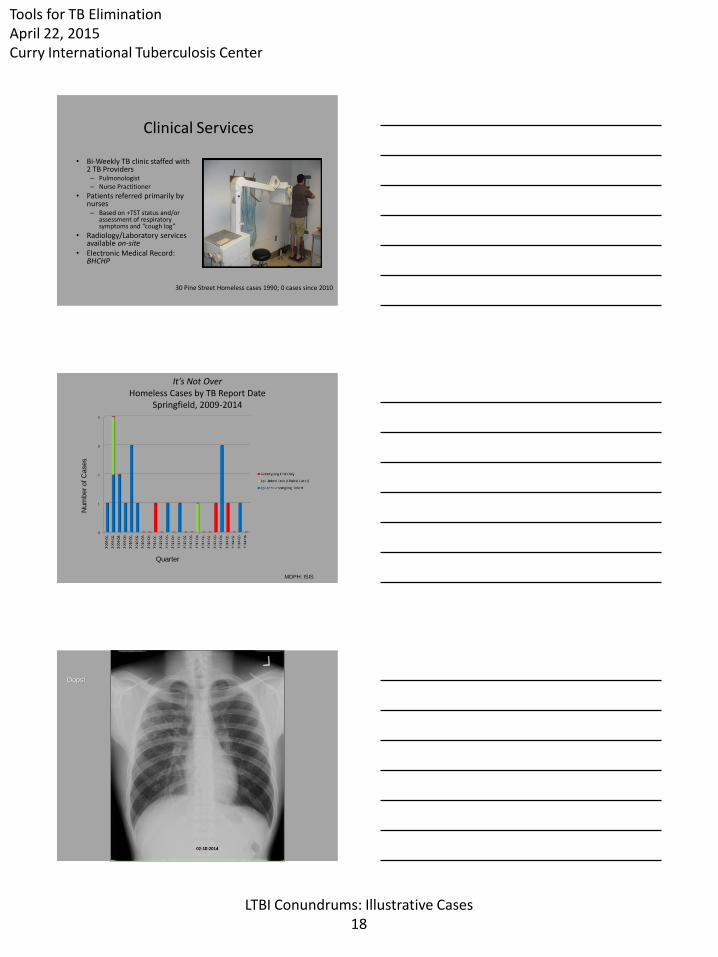
Clinical Services • Bi-Weekly TB clinic staffed with






![NID Online Services NID Form No SMS SC NID sq NID NID sot SMS 19xxxxxxxxxxxxxxx (so NID sq NID SC F D yyyy-mm-dd I SMS SC[space]F ... 08/00/ Sb" owoe/Sb- S8/0\O/Sb SY/oO/Sb" Sb ...](https://static.documents.pub/doc/80x56/5af9c99b7f8b9a5f588e90d5/nid-online-services-nid-form-no-sms-sc-nid-sq-nid-nid-sot-sms-19xxxxxxxxxxxxxxx.jpg)
















