Page 1
MACRA, MIPS, and APM’sUnderstanding Medicare’s Quality Payment Program (QPP)
John Patrick Yeatts, M.D., M.P.H.Division of Hospital MedicineOffice of the Vice President for Medical Affairs / CMODuke University Health System
Page 3
CurrentHospitalist at Duke University HospitalMedical Director within the Office of the Health System VPMA / CMO
Strategic initiatives related to Payer Strategy, Network Development
EducationUNC-Chapel Hill - Economics and Politics, Morehead ScholarGoldman Sachs International, London - AnalystBryn Mawr College – Post Bac Pre MedUNC Chapel Hill – M.D. / M.P.H.Duke University Hospital – Internal Medicine / Management & Leadership
My Background
Page 4
1. Appreciate the historical context for the current state of health care payment reform
2. Understand the essential elements of the Quality Payment Program (QPP) created by MACRA
3. Identify the potential implications of the QPP on provider practice
Learning Objectives
Page 5
Historical Context for Payment Reform
Understanding the Quality Payment Program
Implications and Insights
Agenda
Page 6
Why we’re here today
Deloitte’s2016SurveyofUSPhysiciansn =523physicians(non-pediatricgeneralistsandspecialists)
Page 7
Why we’re here today
Deloitte’s2016SurveyofUSPhysiciansn =523physicians(non-pediatricgeneralistsandspecialists)
Page 8
Ignore at your own risk!
Page 9
Historical Context for Payment Reform
Understanding the Quality Payment Program
Implications and Insights
Agenda
Page 10
The U.S. spends a lot on healthcare
10.0
12.0
14.0
16.0
18.0
20.0
1990 1994 1998 2002 2006 2010 2014 2018 2022
ShareofGDP
(%)
Source:CucklerGetal.,“NationalHealthExpenditureProjections,2012–22:SlowGrowthuntilCoverageExpandsandEconomyImproves”HealthAffairs 32,no.10(2013).
U.S. Healthcare Spending, as a share of GDP
Page 11
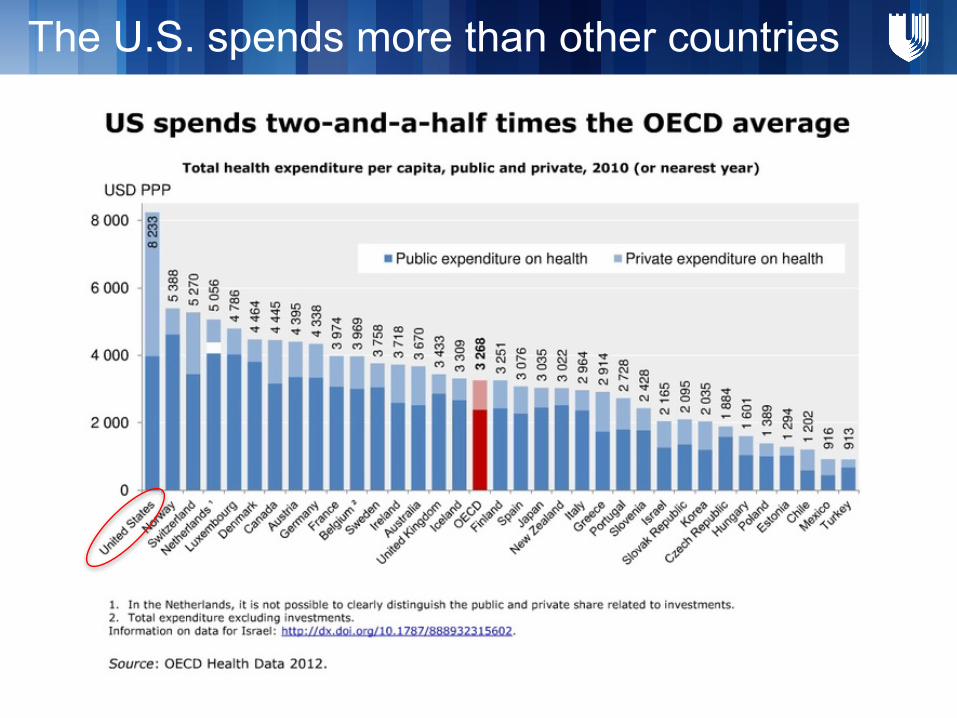
The U.S. spends more than other countries
Page 12
U.S. health care spending is variable
Page 13
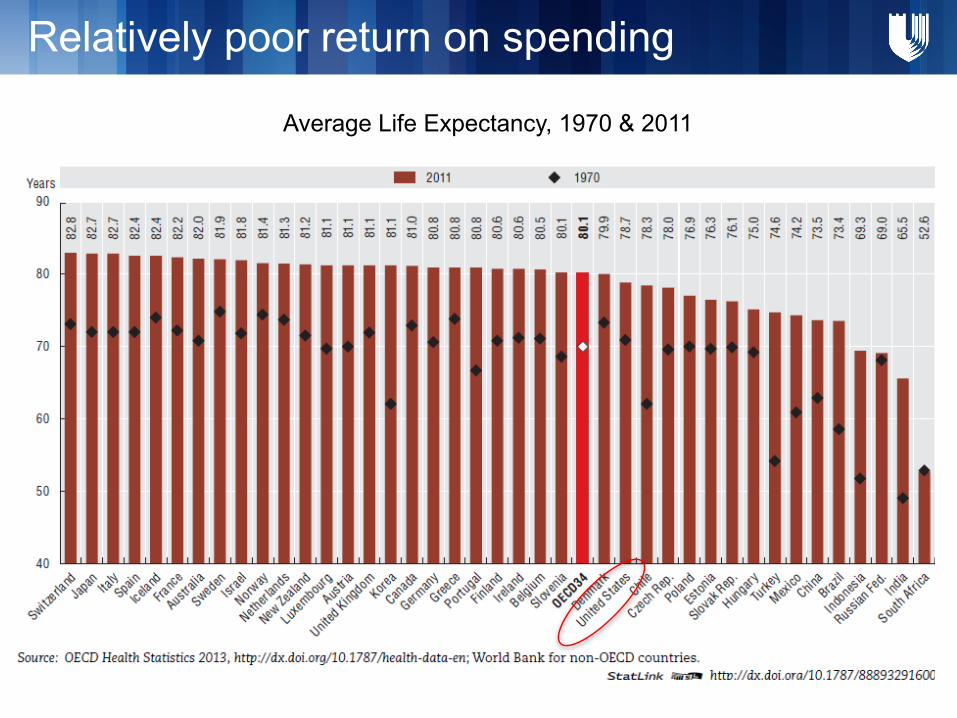
Average Life Expectancy, 1970 & 2011
Relatively poor return on spending
Page 14
Thereisanunclearreturnonourspending
And it’s not just life expectancy
Page 15
ToErrisHumanInstituteofMedicine,1998
98,000peopledieannuallyintheU.S.frommedicalerror
Medicalerrorsareprimarilyasystemproblem
Increasing Attention to Quality
CrossingtheQualityChasmInstituteofMedicine,2001
Outlinespathforimprovingqualityinhealthcaredelivery
Healthcareshouldbe:- Safe- Effective- Patient-centered- Timely- Efficient- Equitable
Page 16
Past:Volume- Based Future:Value- Based
Careforindividuals Managepopulations
Specialtycarefocus Primarycarefocus
Facilitatingthistransitionisamajorundertakingforpayers,providersandpatients
Feeforservice Value/Riskbasedreimbursement
A New Paradigm: Value-Based Care
Page 17
Nobody Knew Health Care Could Be So Complicated
Whatis“value”inhealthcare?Whogetstodefineit?
• Pharmaceuticals:– Should we pay $$$$ for drugs to treat XYZ disease?
• Technology:– Should we start using the newest “ABC” implant or device?
• Providers– Should we pay “inefficient” or “low quality” hospitals and doctors less?
• Population health: – Should we pay for population based outcomes?
Page 18
Brief Historical Context for Payment Reform
Understanding the Quality Payment Program
Implications and Insights
Agenda
Page 19
The QPP was formed by MACRA
MACRA:MedicareAccessandCHIPReauthorizationActof2015
MedicareSustainableGrowthRate(SGR)
MedicareQualityPaymentProgram(QPP)
Repealed Created
MIPS:Merit-basedIncentivePaymentSystem
APMs:AdvancedPracticeModels
a pieceoflegislation
Page 20
A Word about the SGR
MedicareSustainableGrowthRate(1997– 2015)
• LegislativemechanismtoensureannualincreasesinMedicareexpensedidnotexceedgrowthinGDP
• Regulatedproviderexpenseandsomeexpensesincidentaltoprovidervisits(labtests,imaging,physician-administereddrugs)
• Medicarebudgetdeterminedannually• Actualspendingcomparedwithbudget
Ø Ifspendinghigher,providerpaymentsdecreasedthefollowingyear
Ø Ifspendinglower,providerpaymentsincreasedthefollowingyear
Page 21
The SGR: In practice
1997– 2001:Actualexpenditures<budgeted,paymentsincreased
2002:Actualexpenditures>budgeted,-4.8%paymentadjustment
2003 - 2015:Actualexpenditures>budgeted,multiple“docfixes”toavoidfurthercuts
2015:MACRArepealstheSGR
M.E.I.=MedicareEconomicIndex(indexofthecosttooperateatypicalmedicalpractice)
Page 22
MACRA has two tracks
MACRA:MedicareAccessandCHIPReauthorizationActof2015
MedicareQualityPaymentProgram(QPP)
Created
MIPS:Merit-basedIncentivePaymentSystem
CombinesCMS’existingqualityreportingprogramsintoonenewprogram
APMs:AdvancedPracticeModels
Createsnewframeworksforrewardinghealthcareproviderswhoprovidevalue-basedcare
MACRA appliestopaymenttoPROVIDERSonly,nottohospitalsorotherfacilities
Page 23
2016 2018
NewCMSGoals:
30%
85%50%
90%
The Merit-based Incentive Payment System (MIPS) links
fee-for-service payments to quality and value.
\
MACRA also provides incentives for participation in Alternative Payment Models (APMs) and bonus payments to “eligible”
APMs
All Medicare fee-for-service (FFS) payments
Medicare FFS payments linked to quality and value
Medicare payments linked to quality and value via APMs
Medicare Payments to those in “eligible” (most highly advanced) APMs under MACRA
How MACRA Helps CMS Accomplish Its Goals
Page 24
Which track will you belong to?
500,000providers
70,000– 120,000providers
Page 25
What is “MIPS”?
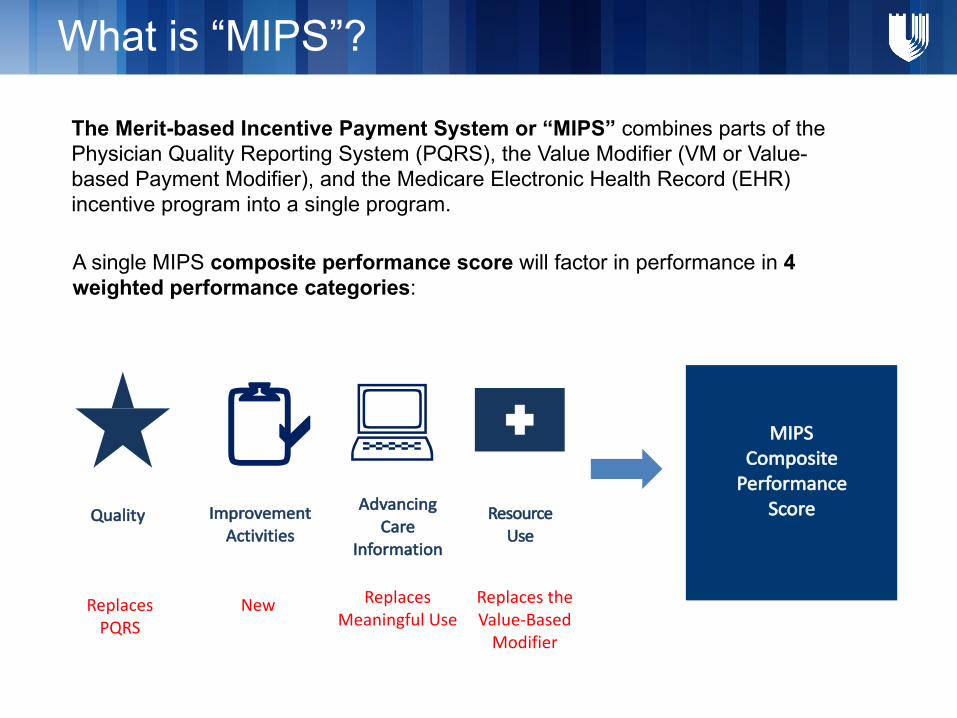
The Merit-based Incentive Payment System or “MIPS” combines parts of the Physician Quality Reporting System (PQRS), the Value Modifier (VM or Value-based Payment Modifier), and the Medicare Electronic Health Record (EHR) incentive program into a single program.
A single MIPS composite performance score will factor in performance in 4 weighted performance categories:
MIPSCompositePerformance
ScoreQuality ResourceUse
:Advancing
CareInformation
2aImprovementActivities
ReplacesPQRS
New ReplacesMeaningfulUse
ReplacestheValue-BasedModifier
Page 26
Weighted Performance Categories Under MIPS
Inanygivenyear,themajority(60%)ofscoreisbasedonQualityandResourceUse(a.k.a.,cost)
October2016– FinalRule– ResourceUse=0%andQuality=60%
Page 27
Measures: A Closer Look
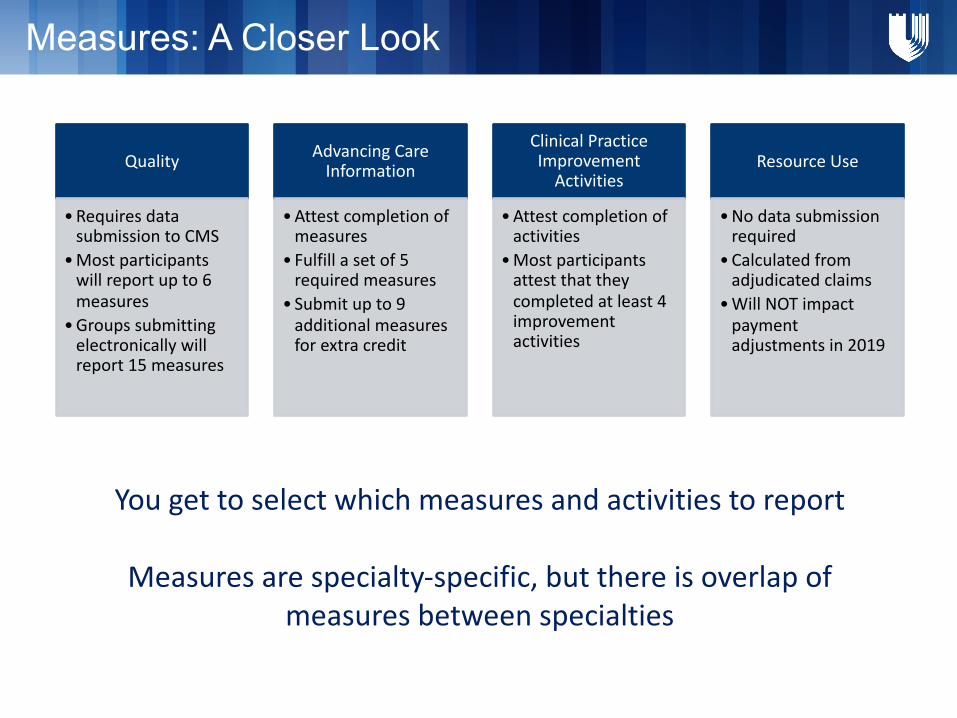
Quality
•RequiresdatasubmissiontoCMS
•Mostparticipantswillreportupto6measures
•Groupssubmittingelectronicallywillreport15measures
AdvancingCareInformation
•Attestcompletionofmeasures
• Fulfillasetof5requiredmeasures
• Submitupto9additionalmeasuresforextracredit
ClinicalPracticeImprovementActivities
•Attestcompletionofactivities
•Mostparticipantsattestthattheycompletedatleast4improvementactivities
ResourceUse
•Nodatasubmissionrequired
•Calculatedfromadjudicatedclaims
•WillNOTimpactpaymentadjustmentsin2019
Yougettoselectwhichmeasuresandactivitiestoreport
Measuresarespecialty-specific,butthereisoverlapofmeasuresbetweenspecialties
Page 28
Examples of Quality Measures (Submit Data)
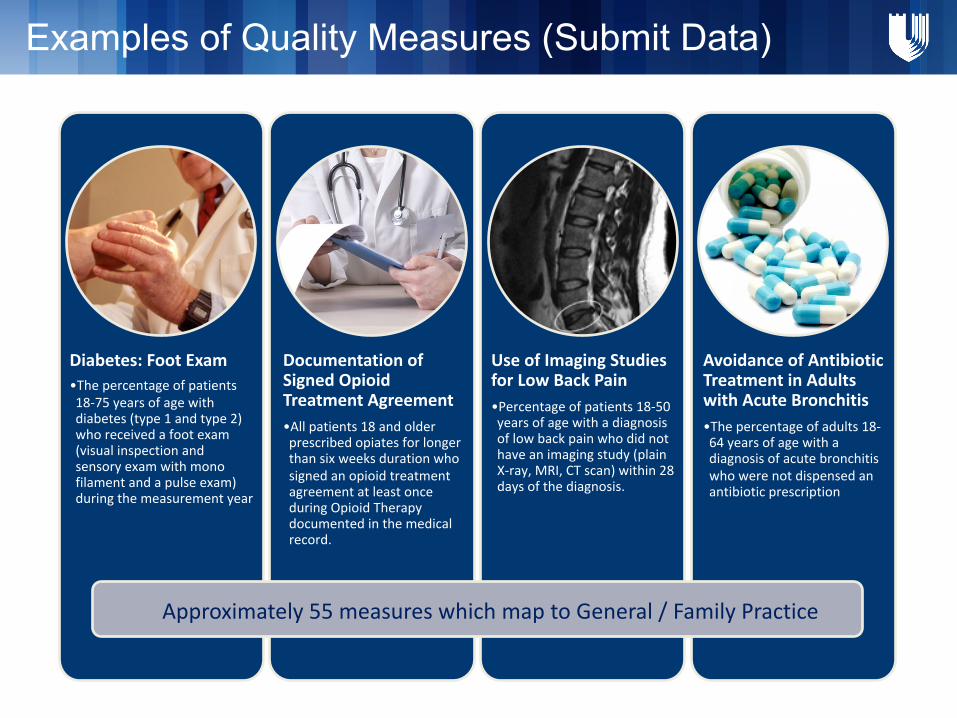
Diabetes:FootExam•Thepercentageofpatients18-75yearsofagewithdiabetes(type1andtype2)whoreceivedafootexam(visualinspectionandsensoryexamwithmonofilamentandapulseexam)duringthemeasurementyear
DocumentationofSignedOpioidTreatmentAgreement•Allpatients18andolderprescribedopiatesforlongerthansixweeksdurationwhosignedanopioidtreatmentagreementatleastonceduringOpioidTherapydocumentedinthemedicalrecord.
UseofImagingStudiesforLowBackPain•Percentageofpatients18-50yearsofagewithadiagnosisoflowbackpainwhodidnothaveanimagingstudy(plainX-ray,MRI,CTscan)within28daysofthediagnosis.
AvoidanceofAntibioticTreatmentinAdultswithAcuteBronchitis•Thepercentageofadults18-64yearsofagewithadiagnosisofacutebronchitiswhowerenotdispensedanantibioticprescription
Approximately55measureswhichmaptoGeneral/FamilyPractice
Page 29
Advancing Care Information (Attest)
FiveRequiredMeasures• SecurityRiskAnalysis:Perform1• E-Prescribing:Transmitatleast1prescriptionelectronically• ProvidePatientAccess:Onlineaccessforatleast1patient• SendSummaryofCare:Createandsendforatleast1encounter• Request/AcceptSummaryofCare:Receiveandincorporateforatleast1newpatient
AdditionalMeasures(Examples)• SecureMessaging: Sendtoorreceivefromatleast1patient• ClinicalDataRegistryReporting: Haveanactiveengagementtosendclinicaldataelectronicallytoaclinicaldataregistry
• Patient-GeneratedHealthData: Incorporatepatient-generateddataintotheHERforatleast1patient
Page 30
Examples of Improvement Activities (Attest)
Implementationoffallscreeningandassessmentprograms•Implementationoffallscreeningandassessmentprogramstoidentifypatientsatriskforfallsandaddressmodifiableriskfactors(e.g.,Clinicaldecisionsupport/promptsintheelectronichealthrecordthathelpmanagetheuseofmedications,suchasbenzodiazepines,thatincreasefallrisk).
Collectionandfollowuponpatientexperienceandsatisfactiondataonbeneficiaryengagement•Collectionandfollow-uponpatientexperienceandsatisfactiondataonbeneficiaryengagement,includingdevelopmentofimprovementplan.
Regulartrainingincarecoordination•Implementationofregularcarecoordinationtraining
Over90activitiestochoosefrom
Page 31
• Based on the Composite Performance Score, providers will receive positive, negative or neutral adjustments
• Each provider will receive a quality score between 1 and 100
• Those above average will be eligible for incentives, those below average will receive penalties
MAXIMUMAdjustments
Adjustment to provider’s base rate of Medicare Part B payment
4% 5%7%9%
2019 2020 2021 2022 onward
-4%-5% -7%-9%
How Payment Works for Providers Under MIPS
Page 32
Exceptions to MIPS:
What about APM’s?
ProvidersintheirfirstyearofMedicareparticipation
ProvidersbelowMedicare’slowvolumethreshold•Youbilllessthanorequalto$30,000inallowableMedicarePartBchargesperyearOR•Youseefewerthan100Medicarebeneficiariesperyear
Providerswhoaren’toneofthefollowing•MD•PA•NP•ClinicalNurseSpecialists• CertifiedRegisteredNurseAnesthetist
QualifyingParticipants(QP’s)inEligibleAPMs
Page 33
What is an APM?
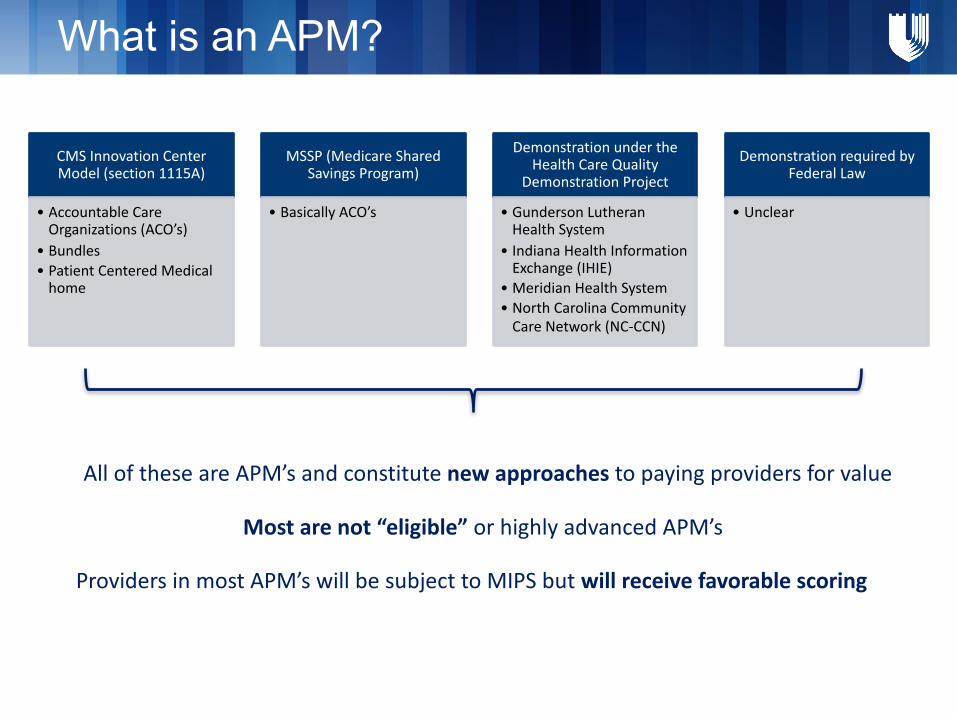
Mostarenot“eligible”orhighlyadvancedAPM’s
ProvidersinmostAPM’swillbesubjecttoMIPSbutwillreceivefavorablescoring
AlloftheseareAPM’sandconstitutenewapproachestopayingprovidersforvalue
CMSInnovationCenterModel(section1115A)
• AccountableCareOrganizations(ACO’s)
• Bundles• PatientCenteredMedicalhome
MSSP(MedicareSharedSavingsProgram)
• BasicallyACO’s
DemonstrationundertheHealthCareQuality
DemonstrationProject
• GundersonLutheranHealthSystem
• IndianaHealthInformationExchange(IHIE)
• MeridianHealthSystem• NorthCarolinaCommunityCareNetwork(NC-CCN)
DemonstrationrequiredbyFederalLaw
• Unclear
Page 34
What is an “eligible” or advanced APM?
Eligible APMs are the most advanced APMs that meet the following criteria according to the MACRA law:
• Base payment on quality measures comparable to those in MIPS
• Require use of certified EHR technology
• Either (1) bear more than nominal financial risk for monetary losses OR (2) are a medical home model expanded under CMMIauthority
ProviderswhoreceivepaymentsfromaneligibleAPMaredefinedaseitherQualifyingParticipants(QP’s)orPartialQualifyingParticipantsbasedonmeetingeitherthePaymentor PatientRequirement
Page 35
APM Participation Requirement
PaymentThreshold TotalPaymentsinEligibleAPM
TotalPartBPayments=
Determination of Qualifying Participants or Partial Qualifying Participants status is based onwhether or not a percentage of total Part B payments or Patients is derived from an eligible APM.
• Qualifying participants:• Meet the payment or patient threshold• Receive a 5% bonus on their total Part B payments• Do not have additional MIPS reporting• 0.75% payment adjustment in 2026
• Partial qualifying participants:• Fall short of revenue threshold• Do not receive a 5% bonus on their total Part B payments• 0.25% payment adjustment in 2026• Can choose whether to report MIPS*
• Choosing not to report will result in no payment adjustment for that year• Decision is made at the entity level and applies to all providers
PatientThreshold AttributionEligiblePatients
AttributedPatients=
*Unclearwhetherthiswillbeachoiceorimposed
Page 36
Payment and Patient Thresholds
Boththresholdsincreaseovertime
Page 37
List of Advanced APM’s
ComprehensiveESRDCare– TwoSidedRisk
ComprehensivePrimaryCarePlus(CPC+)
NextGenerationACOModel
SharedSavingsProgram– Track2
SharedSavingsProgram– Track3
OncologyCareModel(OCM)– Two-SidedRisk
ComprehensiveCareforJointReplacementPaymentModel(Track1)
CMSintendstoexpandlistofAdvancedAPMseachyear
Page 38
Initial performance period: Jan 1, 2017 – Dec 31, 2017Can start collecting data anytime, but the more the betterMust submit data to CMS by March 31, 2018First payment adjustment on Jan 1, 2019
Timeline and Key Dates
Page 39
Choices in 2017: Data Submission
If… Then… When?
Youdonot submitanydatatoCMS
Automatic4%negativeadjustment
2019
Yousubmita“minimum”ofdatatoCMS
Nodownwardadjustment,butnoincreaseeither
2019
Yousubmit90daysofdatatoCMS
Eligiblefora partialfeescheduleadjustment
2019
Yousubmitafullyear’sworth ofdata
Eligible forafullfeescheduleadjustment
2019
Feeschedule“adjustment”=positiveornegative
Page 40
Agenda
Historical Background for Payment Reform
Overview of the Quality Payment Program
Implications and Insights
Page 41
MACRA ≠ ACA
2009
“Obamacare”
AccesstoCare
Partisansupport
FutureTBD
2015
“MACRA”
ProviderPaymentReform
Bipartisansupport
Notgoingaway
Page 42
Risk = cost of provider services
MACRA shifts risk to providers
ProvidersinMIPSwillbeheldincreasinglyaccountableforcostovertime
RemembertheFinalRule:ResourceUse=0%inYear1
Page 43
Risk = cost of provider services
MACRA shifts risk to APM providers, too
ProvidersinAPMsbetterhavetheirmodelhonedby2025,whenthe5%bonusesend
5%bonusends
Page 44
• MIPS is budget neutral• This differs from meaningful use, where
everyone who hits a threshold gets incentive
• Provider bonuses for some will be offset by penalties for others
• Competition among providers, but not in the traditional sense of just patients in the door
MIPS may foster competition
Page 45
Budget neutrality will mean funds will flow from small group practices to larger group practices
Small practices will be adversely affected
TheburdensofMIPSwillbebetterabsorbedbylargerpractices
Page 46
Help for smaller practices
ProvisioninMACRAtohelppracticeswith<15clinicians,includingthoseinrural,medicallyunderserved,andhealthprofessionalshortageareas
CMSnamesalocalorganizationto:- Assistpracticeswithqualityreportingmeasures- Engagepracticesincontinuousqualityimprovement- OptimizehealthITwithpractices- Evaluateapractice’soptionsforjoininganadvancedAPM
ForNC/SC/Georgia/FloridathisisAlliantGMCF(GeorgiaMedicaid),aMedicareQualityInnovationNetwork-QualityImprovementOrganization(QIN-QIO)
Page 47
CMS wants you to become an APM
The5%bonusinyears2019– 2024ismeanttoentice:
1. ProviderstogravitatetowardsAPMsandbecomeQP’sinaneligible(or“advanced”)APM
2. ForexistingpracticestoseekalignmentwithaneligibleAPM
3. Fornon-eligibleAPM’stobecomeeligible
Justremember:
EligibleAPMsbearsignificantfinancialrisk
Page 48
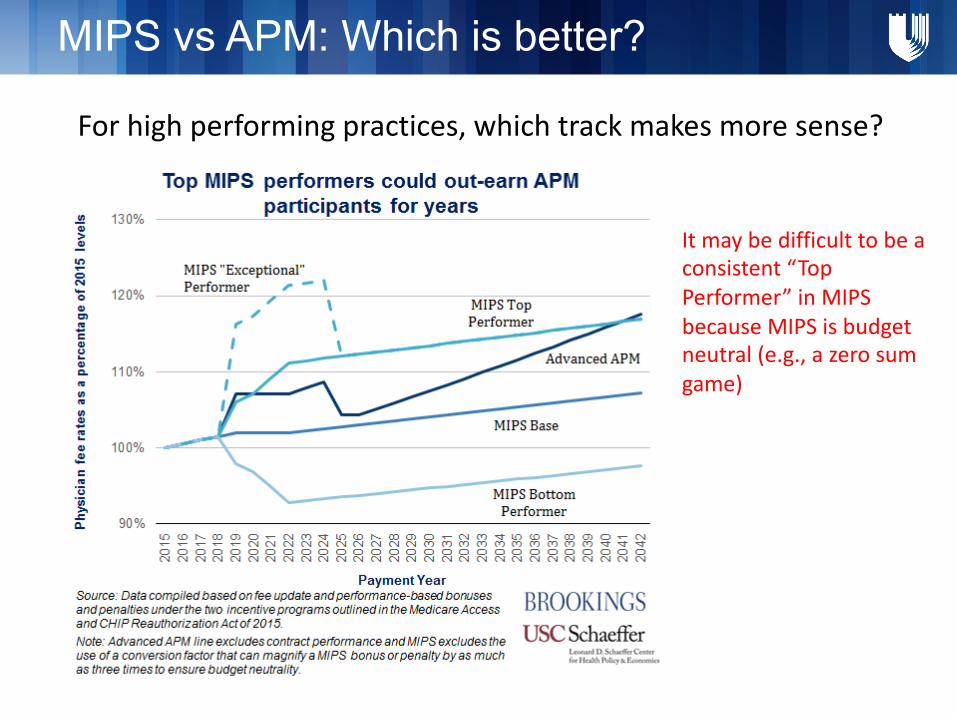
MIPS vs APM: Which is better?
Forhighperformingpractices,whichtrackmakesmoresense?
Itmaybedifficulttobeaconsistent“TopPerformer”inMIPSbecauseMIPSisbudgetneutral(e.g.,azerosumgame)
Page 49
• Will CMS provide practices data-driven feedback in a timely manner to drive performance?
• How easy will it be to move between pathways?
• How will MACRA affect provider transitions and their value in the marketplace?
• How will MACRA affect physician productivity?
Outstanding questions
Page 52
Summary:MIPSvsAPMMIPS v. APM
• Performance based on quality, resource use, clinical practice improvement activities and meaningful use of EHRs
• Significant reporting burden• 4-9% of total Part B Spending at risk over
time over future FFS rates
• Eligible for 5% bonus on Part B claims (2019-24)• Higher update starting in 2026• No MIPS reporting required
PQRS* MeaningfulUse*
Value-basedModifier*
Merit-BasedIncentivePaymentSystem(MIPS)
QualifyingParticipant(providermeetsthresholdfor“significant”participationinAPM)
PartiallyQualifyingParticipant(providerdoesnot meet“significantparticipation”inAPMthreshold)
• Not eligible for 5% bonus• Lower annual update • MIPS optional, but will receive no payment
adjustment for that year
• Bothoptionscontainsomelevelof“risk”• Bothmodelsrequireafocuson“efficiency”tosucceed• ParticipantsinaneligibleAPMqualifyforbonuseligibility(whichcanhelp
offsetsomerisk)
Page 53
Government- ValueBasedPurchasing- Valuebasedmodifier- PhysicianQualityReportingSystem
(PQRS)- MeaningfulUse- MIPSandAPM- ACOs(MedicareandMedicaid)- HospitalReadmissionsReduction
Program- HospitalAcquiredConditionsProgram- MedicareAdvantage:STARratings- HospiceQualityInitiative- Manyothers
PrivateInsurers:- ACO- Narrownetwork- Highperformingnetworks
Providers- Internalqualitybenchmarkingfor
QIandcompensation- Transparencyofpatients
satisfactionandoutcomes
Many Value Based Initiatives
Paymentmechanismsfocusedonbothcostandquality
Page 54
TheU.S.spendsalotofmoneyonhealthcare,bothinabsolutetermsandrelativetosimilarcountries
TheU.S.derivesquestionablevaluefromitshealthcarespending
Thereisincreasingfocusonenhancingvalueinhealthcare
Howonedefinesvalueisdebatable
Historical Context: Key Points