23
Macrophage Activation Syndrome in SJIA Alexei Grom, MD Cincinnati Children’s Hospital Medical Center
| Date post: | 28-Jan-2018 |
| Category: |
Science |
| Upload: | systemic-jia-foundation |
| View: | 143 times |
| Download: | 0 times |
Macrophage Activation Syndrome in SJIA
Alexei Grom, MD
Cincinnati Children’s Hospital Medical Center
Macrophage Activation Syndrome
• Caused by excessive activation and multiplication of predominately two types of immune cells
• cytotoxic CD8+ T cells and
• macrophages
• Excessive activation of these cell leads to massive inflammation that might be life-threatening

Normal macrophages
• a type of white blood cells that engulfs and destroys microbes and other foreign substances in a process called phagocytosis

Macrophages in MAS
• Overly activated
• Start phagocytosing and destroying normal blood cells (such as red blood cells, neutrophils and platelets)
• Destruction of these blood cells leads to a sudden drop in their numbers and might be life-threatening
Normal cytotoxic T cells
• A cytotoxic T cell (also known CD8+ T-cell or killer T cell) is a T lymphocyte (another type of white blood cells) that kills cancer cells, and cells that are infected (particularly with viruses)

Annual Reviews
MAS is a cytokine storm
MAS is a cytokine storm
• Immune cells communicate with each other by sending various “chemical signals” called cytokines
• some cytokines cause inflammation
• some cytokines reduce inflammation
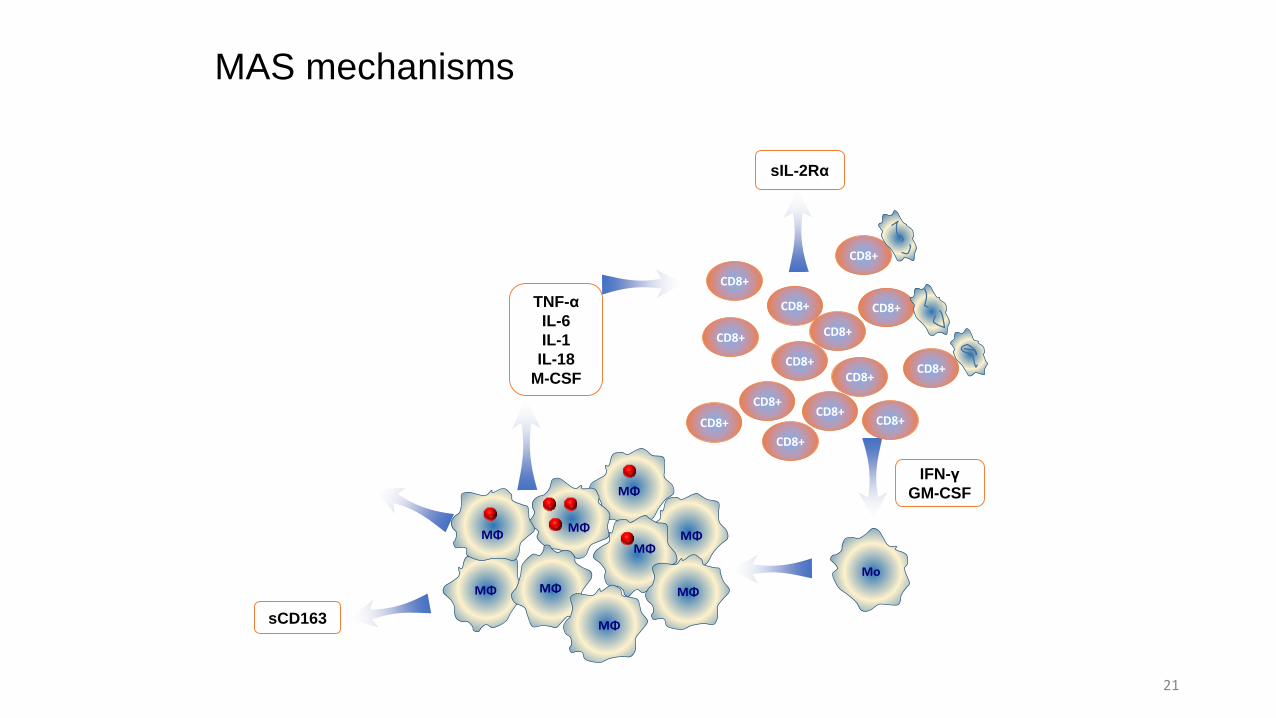
• In MAS, there is excessive activation and multiplication of macrophages and cytotoxic T cells that produce too much cytokines that cause inflammation
MΦ
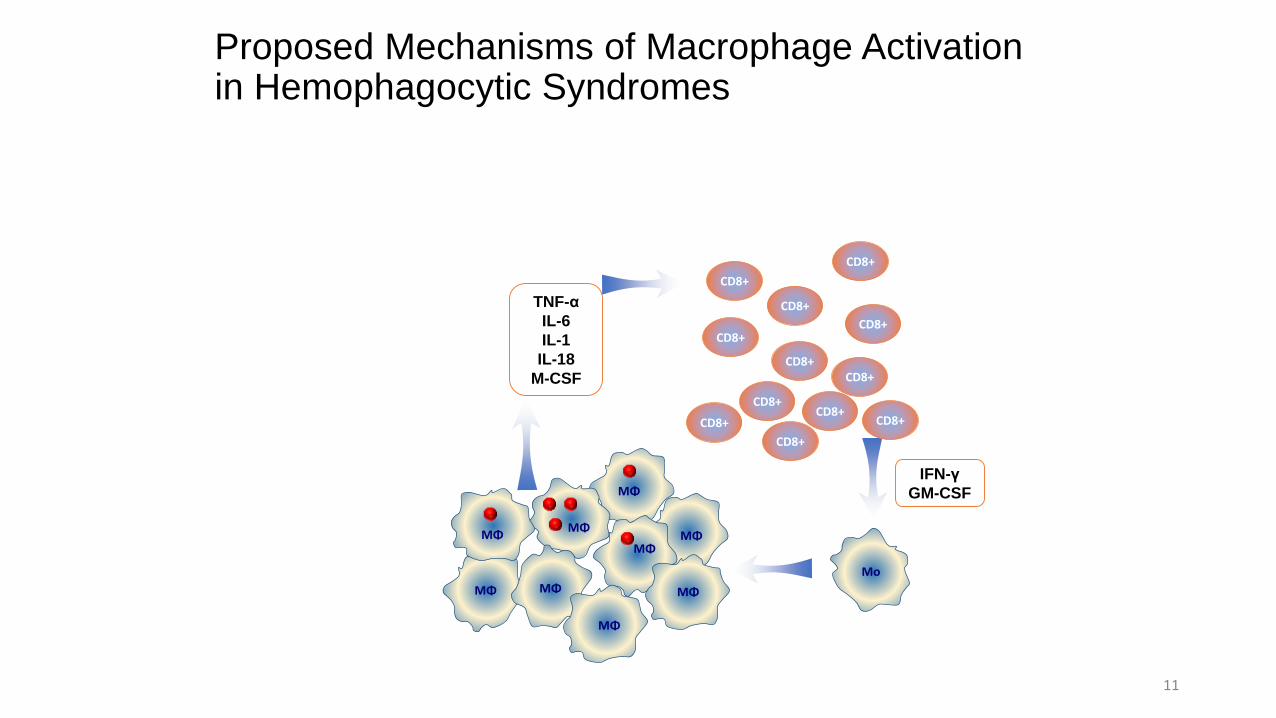
Proposed Mechanisms of Macrophage Activation in Hemophagocytic Syndromes
11
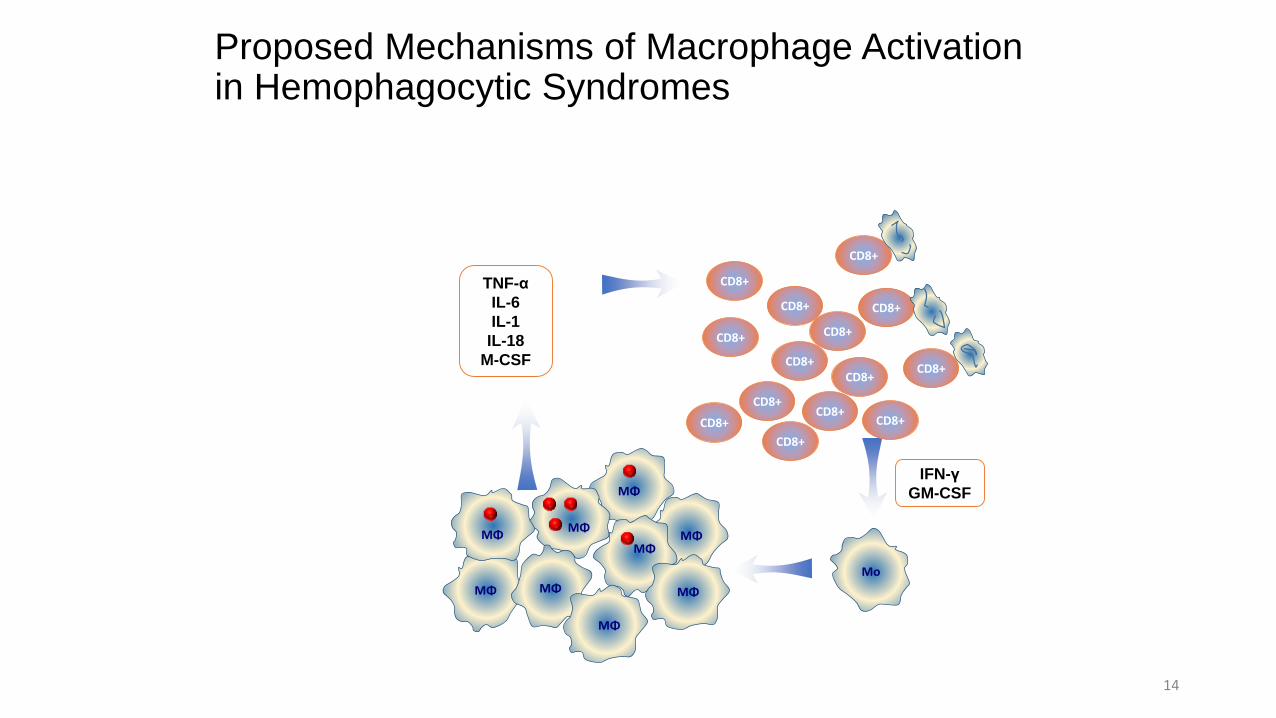
CD8+
IFN-γ
GM-CSF
MΦ
MΦ
MΦMΦ
MΦMΦ
MΦ
Mo
TNF-α
IL-6
IL-1
IL-18
M-CSF
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
MΦ
MAS and Hemophagocytic Lymphohistiocytosis
• striking clinical similarities between MAS and hemophagocytic lymphohistiocytosis
• hemophagocytic lymphohistiocytosis is a genetic disease in which cytotoxic cells have decreased ability to kill cells infected with viruses
• Mouy R, et al. J Pediatr 1996;129:750
Annual Reviews
MΦ
Proposed Mechanisms of Macrophage Activation in Hemophagocytic Syndromes
14
CD8+
IFN-γ
GM-CSF
MΦ
MΦ
MΦMΦ
MΦMΦ
MΦ
Mo
TNF-α
IL-6
IL-1
IL-18
M-CSF
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
MΦ
CD8+
CD8+
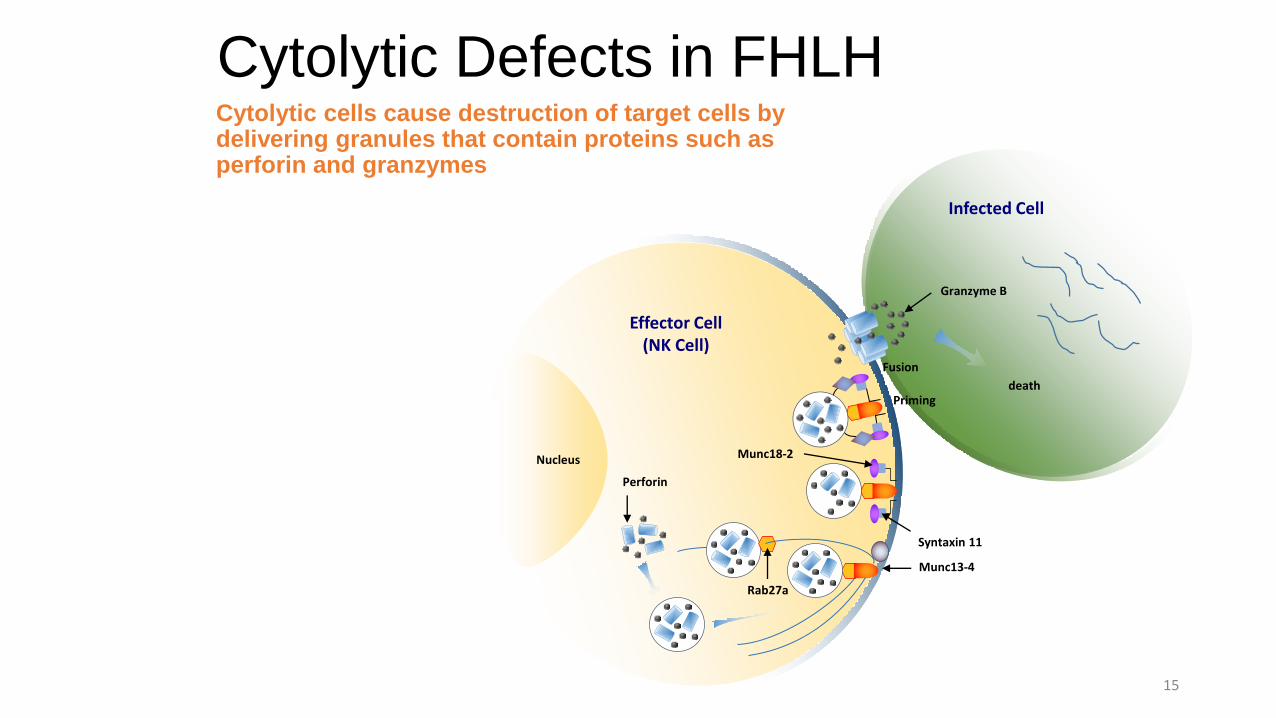
Cytolytic Defects in FHLHCytolytic cells cause destruction of target cells by delivering granules that contain proteins such as perforin and granzymes
15
death
Infected Cell
Effector Cell (NK Cell)
Granzyme B
Fusion
Priming
Munc13-4
Munc18-2
Syntaxin 11
Rab27a
Nucleus
Perforin

Signs and Symptoms Macrophage Activation Syndrome
Macrophage Activation Syndrome
• Patients look very ill, run high fevers
• Laboratory abnormalities:• Sudden drop in hemoglobin, platelet and neutrophil counts
• Very high serum ferritin
• Impaired liver function
• Increased liver enzymes (Ast, Alt)
• Decreased ability to make proteins involved in blood coagulation (such as fibrinogen) leading to bleeding
Silverman ED, et al. J Pediatr 1983;103:872.
Hadchouel M, Prieur AM, and Griscelli C. J Pediatr 1985;106:561.

MAS in Pediatric Rheumatology
• Has been reported in association with almost any rheumatic disease
• By far, most common in systemic JIA• About 80% of reported cases occurred in association with systemic JIA• SLE, Kawasaki disease
• Prevalence of “overt MAS” in systemic JIA is ~10%Sawney, et al. Arch Dis Child 2001;85:4210
• Evidence of subclinical MAS in a subgroup of systemic JIA patients with active systemic disease (~30%)
Bleesing, et al. Arthritis Rheum 2007;56:965Behrens, et al. J Rheumatol 2007:34:1133
Laboratory monitoring for signs of MAS
• Cell blood count
• Ferritin
• Liver enzymes
• Fibrinogen
• Soluble IL2Rα
• Soluble CD163
MΦ
MAS mechanisms
21
CD8+
IFN-γ
GM-CSF
MΦ
MΦ
MΦMΦ
MΦMΦ
MΦ
Mo
TNF-α
IL-6
IL-1
IL-18
M-CSF
sCD163
sIL-2Rα
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
CD8+
MΦ
CD8+
CD8+

Established Treatments of MAS
• High dose corticosteroids
• Cyclosporine A
• Anakinra in some patients
• Etoposide in most difficult cases
Treatments under investigation
• Biologics neutralizing INF-gamma (anti-IFN γ antibodies)
• Biologics neutralizing IL-18 (recombinant IL18BP)
• Jak-Stat inhibitors

















